
Abstract
Although the association of discoid lupus erythematosus (DLE) with squamous cell carcinoma has been described in the literature, coexistence with a basal cell carcinoma is very rare. The indolent and non-pruritic nature of the lesion cause it often to be diagnosed at the late stage of the disease. Long-standing photosensitivity and chronic inflammation later lead to scarring and hypopigmentation, which are considered as the risk factors for the malignant changes over DLE. Incisional biopsy is often performed from the erythematosus lesion which does not respond to medical treatment. Here we have reported a rare case of basal cell carcinoma of the skin developing in the background of long-standing DLE, which was successfully managed with cold knife local excision.
Introduction
Although the association of discoid lupus erythematosus (DLE) with squamous cell carcinoma (SCC) has been described in the literature, coexistence with basal cell carcinoma (BCC) is very rare. 1 The indolent and non-pruritic nature of the lesion cause it often to be diagnosed at the late stage of the disease. Long-standing photosensitivity and chronic inflammation later leading to scarring and hypopigmentation are considered as the risk factors for the malignant changes over DLE. 2 Here we have reported a rare case of BCC of the skin developing in the background of long-standing DLE, which was successfully managed with cold knife local excision.
Case report
A 75-year-old male patient presented to the outpatient department of ENT with an irregular erythematous lesion approximately 4 cm × 2 cm over the left cheek existing for 10 years (Figure 1(a)). The lesion, extending inferiorly towards the submandibular area, was found to be ulcerated. There was no significant cervical lymphadenopathy. The lesion was shallow with a pigmented margin all around. The general physical examination and ear, nose and throat examination were found normal. Routine investigations including haematological tests, chest X-ray and electrocardiogram were found to be within normal limits. Antinuclear antibody was absent. After being diagnosed clinically as DLE by the dermatologist, the patient was referred to the Department of ENT for evaluation of the ulcerative lesion. After the dermatological consultation, the patient was subjected to medical treatment with a topical steroid (clobetasone butyrate 0.1% ointment), local application of sunscreen, and systemic hydroxychloroquine 250 mg daily for 3 months.
(a) Photograph showing an erythematous skin lesion approximately 4 cm × 2 cm over the left side of cheek at the first visit. (b) Intraoperative marking for wide local excision of the lesion under local anaesthesia taking a 5 mm healthy margin, and (c) Postoperative figure showing the healed wound over the left cheek at the end of 6 months.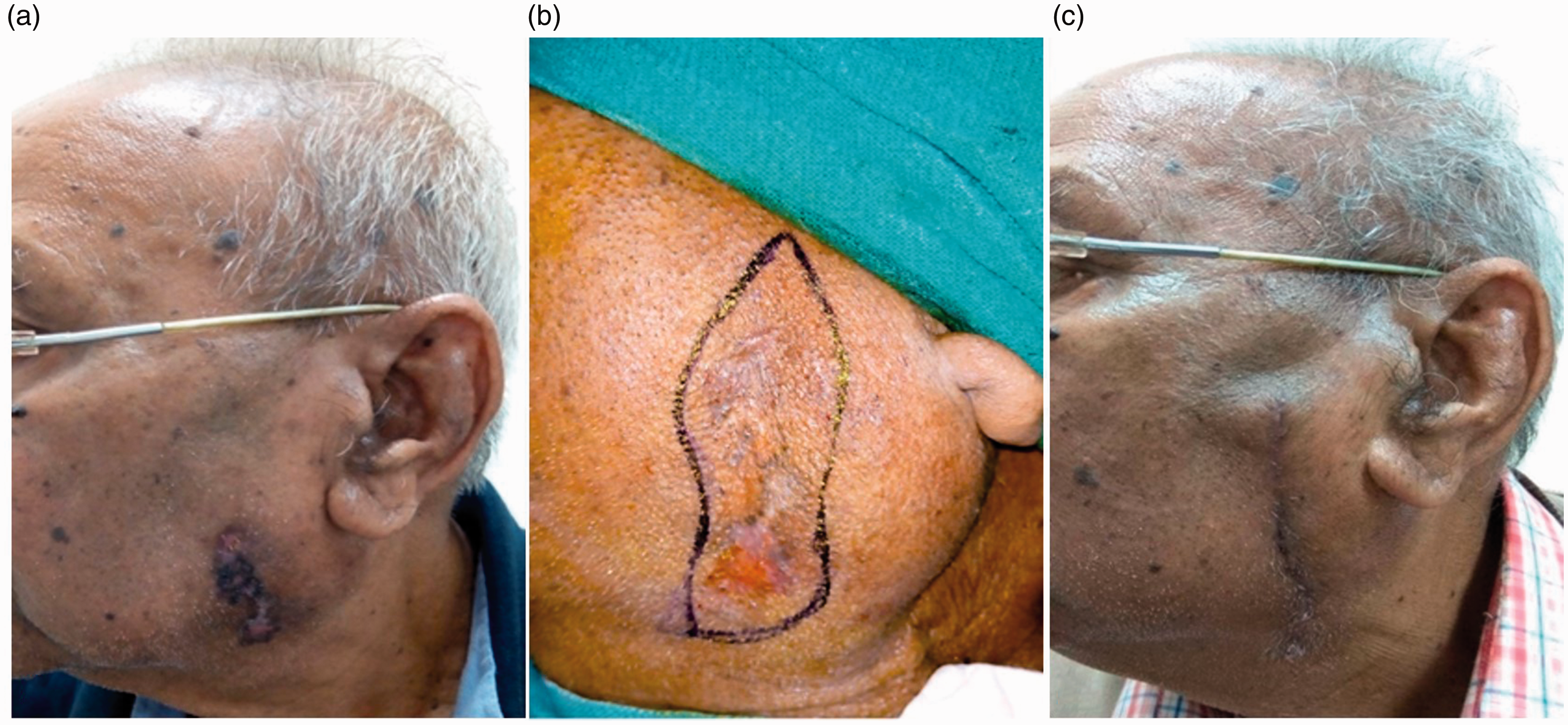
After 3 months of medical treatment, although adequate control of the erythematosus lesion could have been achieved, the ulcerative lesion was found to be increased in size. Suspecting a different underlying pathology, the patient was scheduled for incisional biopsy of the ulcerative lesion. The histopathology revealed thinned out epidermis with nests of basaloid cells in the dermis and dense chronic inflammatory cell infiltration in the superficial and deep layer of the dermis, with destruction of the adenexal structures and occasional follicular plugging noted, suggestive of the dual morphology of both DLE and BCC (Figure 2(a) and (b)).
(a) and (b) Micro section shows thinned out epidermis with nests of basaloid cells in the dermis and dense chronic inflammatory cell infiltration in the superficial and deep layer of the dermis, with destruction of the adenexal structures and occasional follicular plugging (H&E; (a): 40×, (b): 100×).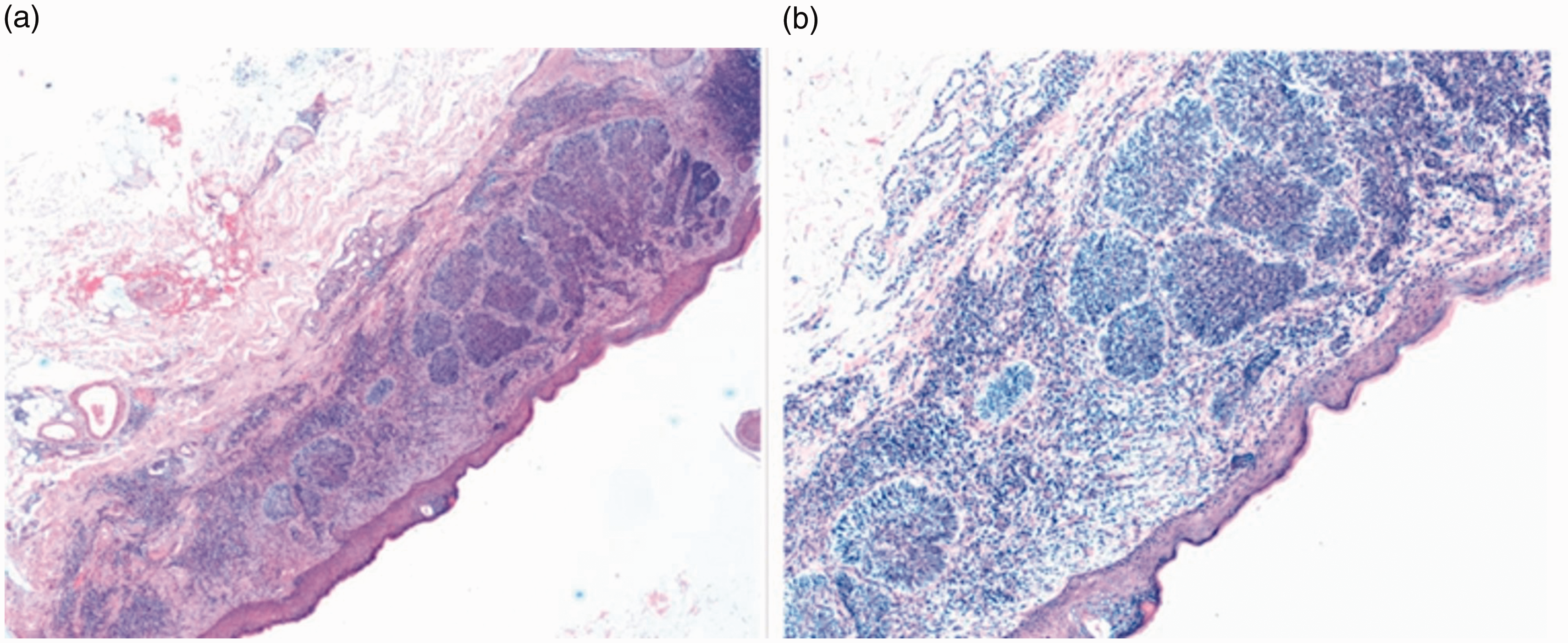
After informed written consent, the patient was scheduled for local excision of the lesion under local anaesthesia. A 5 mm healthy margin was taken along with the excised specimen (Figure 1(b)). Primary closure of the surgical wound was achieved due to the lax skin over the cheek and no skin grafting was required. The final histopathology revealed tumour free margins (anterior, posterior, superior, inferior and deep) of the excised specimen. The patient has been on regular follow-up for the last 6 months, with healed skin (left cheek) without any evidence of local recurrence of the disease (Figure 1(c)).
Discussion
DLE is a benign cutaneous lesion of the head and neck region and development of the malignancy (SCC/BCC) over pre-existing DLE rarely occurs. Both SCC and BCC are feared complications associated with DLE and the occurrence of BCC is very rarely described in the literature. 3 Elderly patients are most often affected by the disease. Diagnosis of the DLE is done mostly by clinical examination, which shows erythematous and scaly patches with features of healing associated with the surrounding pigmentary changes. But due to the indolent course of the disease with a non-painful skin lesion, the diagnosis is often delayed. Patients with high-risk factors, such as elderly patients (>50 years) with exposure to ultraviolet light, can undergo the malignant transformation over the parental DLE. Hence the most common sites affected are the sun-exposed areas of the face, scalp and the forearm and the lip. 1 Medical management (topical and systemic medications) is considered to be effective in controlling the progression of the disease and its further complications. Prompt medical treatment can control the progression of the lesion within 3 months, preventing the chronic inflammation and scarring which is thought to be an important precipitating factor for the development of malignancy.
The biopsy is always warranted in refractory cases and in suspicious lesions in DLE whenever it is associated with a coexisting ulcerative or nodular lesion.4–6 It is routine practice to exclude systemic lupus erythematosus from the parental DLE lesion by clinical (American Rheumatism Association criteria), haematological and radiological investigations. There is a significant variation in the latent period for malignancy in the DLE lesion; Donzis and co-workers reported an average delay of 2 years before the correct diagnosis of DLE. 7 This is mostly due to the indolent nature of the lesion, which delays medical attention. Again, a high index of suspicion of the lesion is always needed to diagnose the primary lesion and the underlying malignancy. 8 There is always a delay in the diagnosis of the BCC over the DLE because of the rarity of the lesion and the variable time interval for its malignant transformation. Incisional biopsy is often required in the patient with DLE with high predisposing factors not responding to medical treatment. DLE affecting the head and neck region should be thoroughly evaluated by the clinicians and histopathological examination is mandatory to rule out any underlying malignancy for early intervention and a better outcome.
Conclusion
An association of BCC is very rare over a long-standing DLE and malignancy should always be excluded in suspicious ulcerative lesions which do not respond to conservative treatment. Patients need a close follow-up in both dermatology and otorhinolaryngology departments and incisional biopsy is often warranted to confirm the diagnosis. Cold knife excision with an adequate margin can provide a complete cure in the management of a coexisting BCC associated with DLE.