
Abstract
Objective
The objective of this study was to evaluate the potential impact of irreversible damage accrual in women with systemic lupus erythematosus (SLE) and adverse maternal and/or fetal/neonatal outcomes.
Methods
Retrospective cohort study with SLE pregnant patients was carried out from January 2011 to January 2020 at the Hospital University Pedro Ernesto (HUPE) of the State University of Rio de Janeiro, Brazil. Irreversible damage was defined according to SLICC/ACR damage index (SDI). The association of SDI on pregnancy outcomes was established by univariate and multivariate regression models and included demographic and clinical variables.
Results
This study included data from 260 patients in their first pregnancies after SLE diagnosis, with a quarter of them (67/260) scoring one or more points on SDI at the beginning of prenatal care. These patients presented more frequently adverse maternal events, namely, disease activity during pregnancy (p = 0.004) and puerperium (p = 0.001), active lupus nephritis (p = 0.04), and hospitalizations (p = 0.004), than those with no SDI score. Similarly, the risks of adverse fetal and neonatal outcomes were also higher among the patients with SDI ≥ 1 (59.7% vs 38.3% p = 0.001) even after controlling data for disease activity (SLEPDAI > 4). Patients with SDI ≥ 1 presented more frequently preterm deliveries (46.3% vs 31.6%; p = 0.01), small for gestational age infants (28.3% vs 18.1%; p = 0.04), and neonatal intensive care unit admission (26.9% vs 1.5%; p < 0.001). The multivariate analyses showed that SDI ≥ 1 is an independent risk factor for hospitalization due to obstetric complications (p = 0.0008) and preterm delivery (p = 0.009).
Conclusion
Pregnant SLE patients who present irreversible damage accrual may have higher risk of maternal and fetal adverse outcomes, independently of disease activity. These results should be validated in further prospective studies.
Keywords
Introduction
Systemic lupus erythematosus (SLE) mainly affects women in reproductive age and pregnancy is common in this population. Over the past decades, the proportion of successful pregnancies increased considerably among these patients, 1 with decreasing rates of fetal loss 2 and adverse pregnancy outcomes. 3 However, ominous events related to lupus activity during pregnancy remain a major challenge. While evaluating pregnant patients with SLE, some disease aspects should be considered as predictors of adverse pregnancies outcomes, such as active or the history of lupus nephritis,4–6 moderate or high disease activity, pulmonary hypertension, presence of antiphospholipid syndrome (APS) or antiphospholipid antibodies (aPL), chronic kidney disease, and chronic arterial hypertension.
Among SLE patients, irreversible organ damage is assessed using the Systemic Lupus International Collaborating Clinics (SLICCs)/American College of Rheumatology (ACR) Damage Index (SDI), which has been extensively validated. The presence of permanent damage accrual, measured by the SDI, is associated with increased risk of further damage, reduced health-related quality of life and higher socio-economic burden, and early mortality, 7 especially when there is early damage and renal or cardiovascular impairment. 8
Although there have been, in the last decades, many studies that searched for predictors of adverse gestational results in women with SLE, to our knowledge, there is no published data that analyzed the impact of damage (SDI) at the beginning of prenatal care, on pregnancy outcomes. The aim of the present study is to evaluate this potential association in a cohort of SLE pregnant patients.
Material and Methods
This is an observational single center cohort study, approved by the Institutional Ethics Committee. The studied population was selected among the two hundred and eighty three women with SLE followed at the high-risk prenatal care clinic for autoimmune diseases and thrombophilia (PrAT) at Hospital Universitário Pedro Ernesto in Rio de Janeiro, Brazil, during a 9-year period between 2011 and 2020. Data were obtained retrospectively by medical charts’ review and personal interviews when necessary.
All pregnant patients that fulfilled ACR 1997 classification criteria for SLE 9 were included. For this study, all data referred exclusively to the first pregnancy of each patient after the SLE diagnosis in order to avoid duplication of SDI count and its potential bias for patients with more than one pregnancy. Cases with congenital malformations or aneuploidies, miscarriages, twin pregnancies, second or more pregnancies, and lack of adequate data for analysis were excluded.
Definitions
Definition of maternal variables
SLE activity was defined as Systemic Lupus Erythematosus Pregnancy Disease Activity Index (SLEPDAI) ≥ 4 during pregnancy 10 and/or a rheumatologist and obstetrician consensual judgment with a need for increasing steroid and/or azathioprine doses. Irreversible organ damage was assessed in the first visit using the SDI.8,11–13 Patients with SDI score of 1 or more were grouped and compared to pregnant women with score of zero.
Lupus nephritis was classified according to ISN/RPS histological criteria, 14 while patients with nephritis without renal biopsy were classified by clinical inference according to previously published criteria. 15 Pre-eclampsia was diagnosed according to the criteria proposed by the American College of Obstetricians and Gynecologists. 16
For this study, maternal adverse pregnancy outcomes (APOs) were defined as lupus disease activity (SLEPDAI ≥ 4), hypertensive disorders related to pregnancy (gestational hypertension, pre-eclampsia, eclampsia, HELLP syndrome, and placental abruption), need for hospitalizations due to SLE or obstetric complications not directly related to lupus, obstetric complications during puerperium (infections, hemorrhage, blood transfusion, and surgical complications), and Cesarean section.
Definition of fetal and neonatal variables
Adverse fetal and neonatal variables were defined as small for gestational age (SGA) at delivery, preterm birth, stillbirth, admission to neonatal intensive care unit (NICU), neonatal death, and neonatal lupus. SGA newborns were classified as birthweight below the 10th percentile according to the INTERGROWTH-21st (between 24 and 42 weeks and 6 days) and Fenton (between 22 and 24 weeks) curves.17,18
Statistical analysis
The descriptive analysis will be presented in the form of tables, the data observed will be expressed by measures of central tendency and dispersion (mean, standard deviation, median, and interquartile range) for numerical data, and frequency and percentage (n and %) for categorical data.
In order to assess the individual influence and the association of demographic, clinical variables, laboratory markers, treatment and comorbidities relationship between adverse pregnancy outcome (APO) and chronic damage (SLICC/ACR-DI), univariate analysis was used.
Once identified, in the univariate analysis, the variables with significant association and p value of up to 0.20 were adjusted to the logistic regression models for the multivariate analysis. In this, initially, all predictors were evaluated individually and later they were selected by the stepwise forward selection method and then choose the multiple statistical model with only the significant variables (p value < 0.05). Thus, the final logistic regression estimated the relative risks and their corresponding 95% confidence intervals.
The comparison of childbirth and newborn characteristics between subgroups with and without SDI was assessed by Student’s t test for independent samples or Mann–Whitney (nonparametric), and for categorical data, the Χ2 test or Fisher’s exact test was applied. The chi-square test was used for categorical data and Fisher’s exact test was used as an alternative to the chi-square when at least one of the variables was <5. A nonparametric method was applied, as some numerical variables that did not have a normal distribution (Gaussian), due to the rejection of the hypothesis of normality according to the Shapiro–Wilk test. The database was implemented in a Microsoft Excel 2007 spreadsheet. The statistical analyses were processed using free program R version 3.3.2 (www.r-project.org).
Results
The first pregnancies of 283 SLE patients that occurred from January 2011 to January 2020 were reviewed. Twenty-three patients were excluded, the reasons were malformed or aneuploid fetuses (5 patients), twin pregnancies (2 patients), miscarriage (12 patients), and pregnant SLE patients for whom adequate data were not available (4 patients). Therefore, 260 patients in their first pregnancies after SLE diagnosis were included. At the beginning of the prenatal care follow-up, a quarter of the patients (67/260) had a SDI score ≥1 with the following results: 50/67 (74.6%) scoring 1; nine (13.4%) patients with score of 2; three (4.5%) with score 3 and five patients (7.5%) scoring 4. The most commonly affected systems were neurological (24.7%), peripheral vascular (21%), renal (19.4%) cardiovascular (10.4%), pulmonary (6%), and infarction or resection of bowel (below duodenum), spleen, liver, or gallbladder (6%). These patients with SDI ≥1 constituted the Group 1.
Demographics and clinical variables of pregnant in SLE with and without SLICC/ACR-SDI.
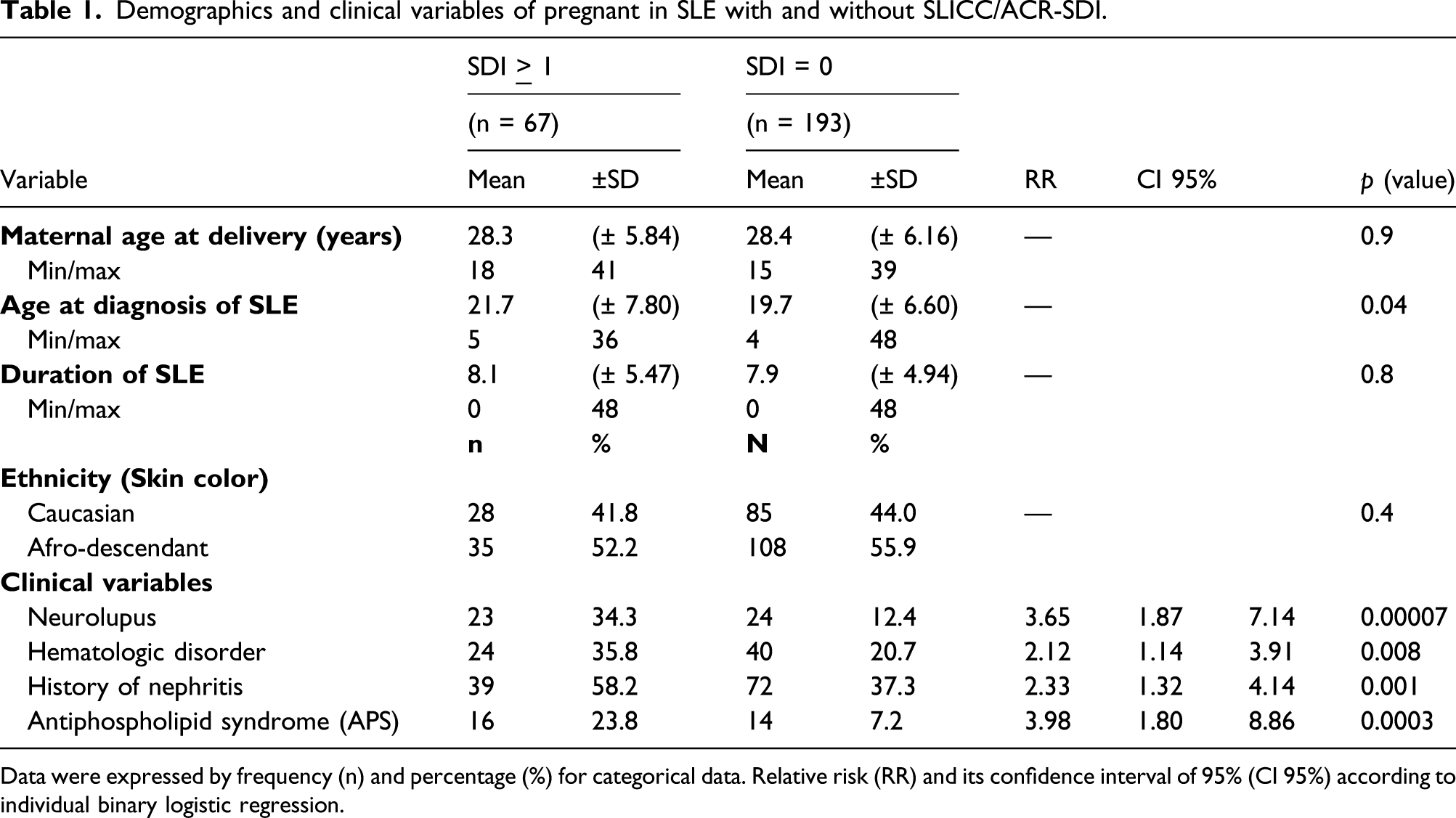
Data were expressed by frequency (n) and percentage (%) for categorical data. Relative risk (RR) and its confidence interval of 95% (CI 95%) according to individual binary logistic regression.
Maternal outcomes of pregnant in SLE with and without SDI.
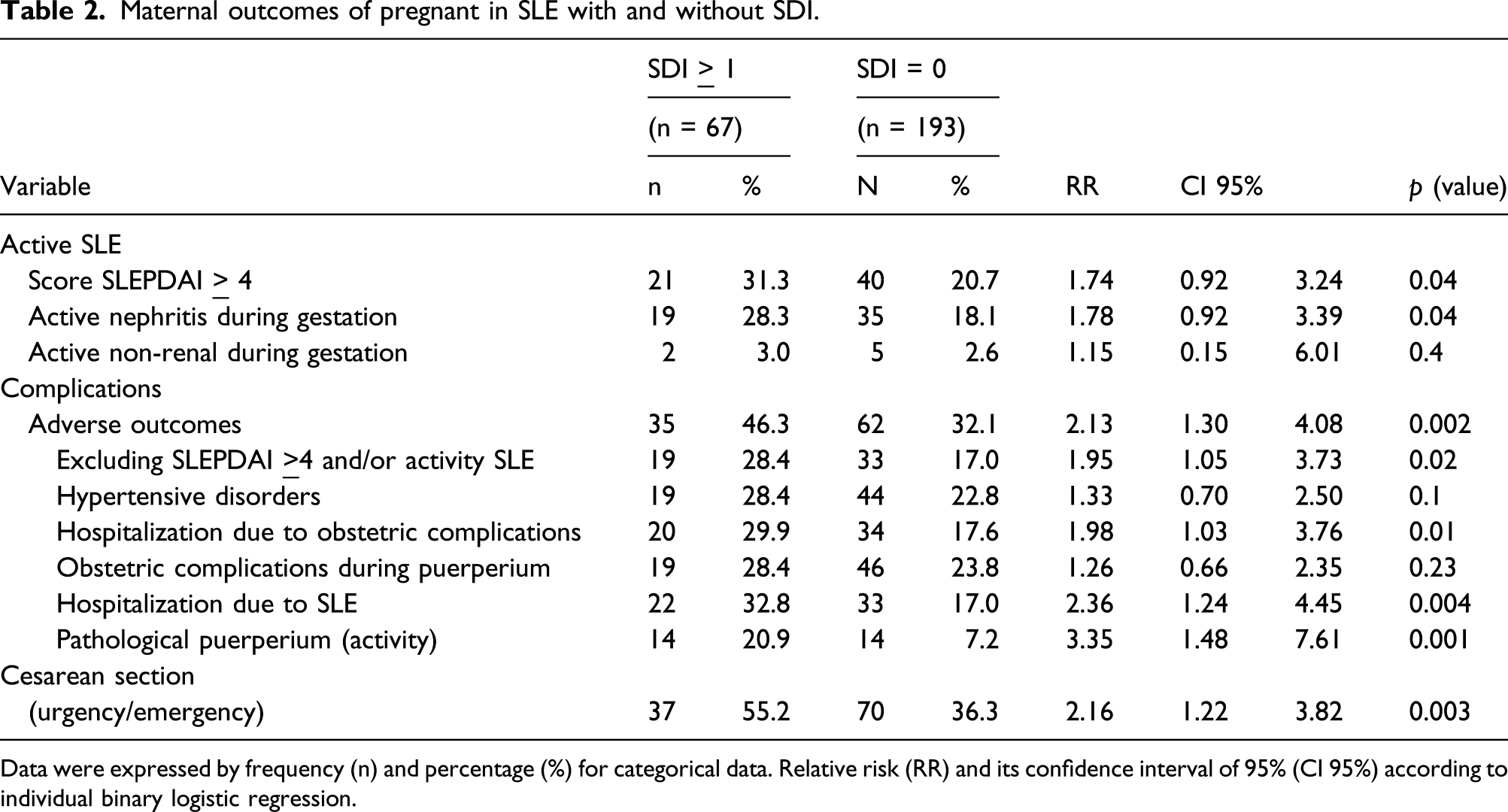
Data were expressed by frequency (n) and percentage (%) for categorical data. Relative risk (RR) and its confidence interval of 95% (CI 95%) according to individual binary logistic regression.
Adverse fetal/neonatal outcomes in pregnant with SLE, with and without SDI.
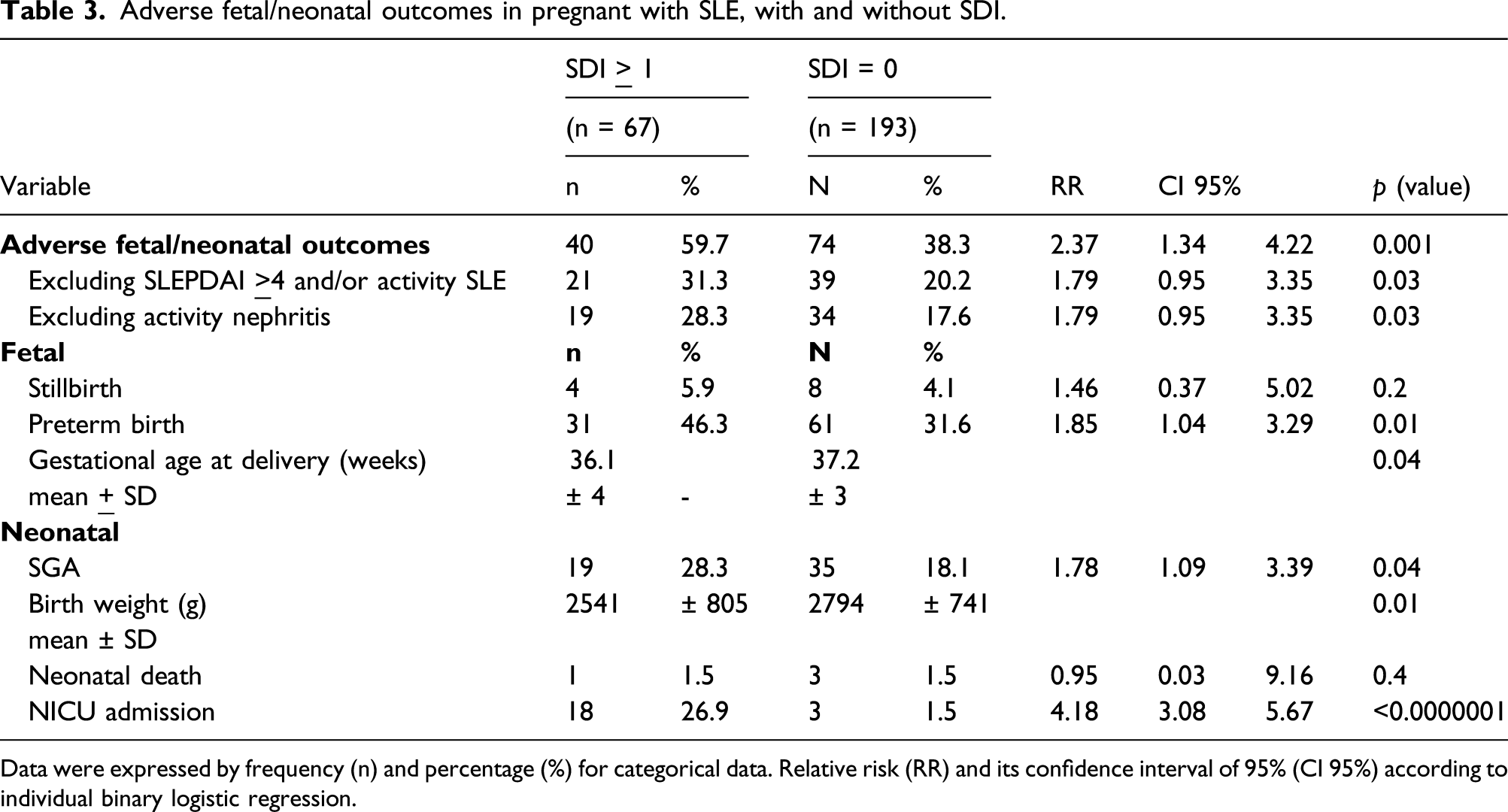
Data were expressed by frequency (n) and percentage (%) for categorical data. Relative risk (RR) and its confidence interval of 95% (CI 95%) according to individual binary logistic regression.
Considering fetal and neonatal outcomes, only 4/40 patients had permanent damage that was not related to these systems (cataract, scaring chronic alopecia, and deforming arthritis). Likewise, only 5/35 patients with adverse maternal outcomes had ocular and skin SDI. This suggests that cardiovascular and neurological permanent damage are more related to adverse events.
On multivariate analysis, SDI ≥1 was an independent risk factor for hospitalization due to obstetric complication during pregnancy non-related to SLE (RR 4.42; CI 1.75-11.47, p = 0.0008) and preterm birth (RR 3.76; CI 1.39-10.69, p = 0.009).
Discussion
The present study that analyzed a single center obstetric cohort of women with SLE and included 260 pregnancies unveiled that organ damage accrual according to SDI may be potently interpreted as a risk factor for adverse maternal and fetal outcomes. Scoring one or more on SDI at the beginning of pregnancy was associated with adverse maternal and fetal outcomes. Due to the typical disease activity and chronic hypertension impact on both maternal and fetal adverse outcomes, we have controlled these variables and the association between damage accrual and adverse outcomes was still observed, suggesting that it was not a random finding. Adverse obstetric events related to SDI may be partially attributed to cardiovascular and renal function impairments, well-known factors for pregnancy complications. 19
A number of studies have demonstrated an increased frequency of maternal and fetal complications even during disease remission, but, to the best of our knowledge, there is no data directly correlating the SDI score with gestational outcomes. Few studies analyzed if pregnancy in SLE had any impact in damage accrual.13,20 In the Lumina cohort study, 13 the authors described that pregnancy was not associated with an increase in damage accrual and they could not find any interactions between maternal and/or fetal outcomes and SDI score prior to pregnancy. They also reported 76.2% of fetal and/or neonatal adverse outcomes, a considerably higher percentage, and this cohort evaluated 63 pregnancies and was limited to the outcomes of miscarriage, premature birth, and stillbirth, not reporting other fetal and maternal adverse outcomes.
In the same context, a nested case–control analysis 20 that included 104 patients, but evaluated only 13 pregnancies after the diagnosis of SLE, did not find any impact of pregnancy on the development of new damage accrual. 20
Previous publications have associated damage accrual in patients with age at disease onset, disease duration, serositis, neurological disorder, hypertension, cumulative dose of glucocorticoids and/or immunosuppressants, uncontrolled disease activity, and the presence of antiphospholipid antibodies. 21 In our cohort, there were no significant associations between SDI and maternal age, chronic hypertension prior to pregnancy, and the use of specific medications. This may be due to the young age of the patients studied (mean 28 years old). However, and in agreement with other studies, we also found a correlation between SDI >1 and higher age at diagnosis, higher disease activity, mostly nephritis, and/or positive aPL.22–26
The presence of any permanent damage measured by the SDI in non-pregnant patients has been shown to predict new damage accrual and complications like hospitalizations, disease activity, organ failure, and even death.21,27–32 Although part of these events is infrequent during pregnancy, such as mortality, some of the other mentioned complications related to damage accrual for non-pregnant SLE patients were also identified in this pregnant population, which corroborates the findings of the study.
This study has some clear limitations. It is a retrospective analysis and the presented results need to be validated in subsequent prospective studies. It also may hinder extrapolation of results, considering data come from a single center, and it was not possible to assess modifiable risk factors such as smoking, since most of patients discontinue or reduce their use during pregnancy. Stratification within the SDI ≥1 group was not possible as almost 75% of patients had a score of 1, limiting comparison with patients with higher scores. Also, evaluation of SDI occurred at beginning of prenatal care and its modification during pregnancy was not analyzed, despite the short period of pregnancy course as this was not the purpose of this study.
On the other hand, to the best of our knowledge, this is the first study to point out a possible correlation between SDI ≥1 and adverse gestational outcomes. The SDI is straight forward to calculate in the routine clinical settings and identifies SLE patients with or without damage accrual. When the damage is present at the beginning of the prenatal care follow-up, it may be interpreted as a risk factor for adverse obstetric outcomes in patients with SLE.
Conclusion
In this single center cohort study that compares adverse maternal, fetal, and neonatal outcomes of pregnant women with SLE, damage at the beginning of prenatal care, as measured by the SDI, can be a predictor of future adverse obstetrics outcomes. These complications were still more frequent in patients with damage accrual even when patients with active disease were removed from analysis as a potential bias. Further studies, with prospective design and larger populations, are required to validate these results and to allow risk stratification inside the SDI scoring group and types of organ involved.
We recognize that larger and prospective studies are needed to confirm our hypothesis; however, this does not invalidate the presented data. Despite these limitations, our study is quite relevant as it demonstrates for the first time that SDI can influence adverse pregnancy outcomes and, in addition, it helps understand pregnancy in SLE women in developing countries like Brazil, with low rate of family planning, low adherence to contraceptive methods, and a significant number of patients with severe and active lupus since conception.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Roger Abramino Levy is a former professor of Rheumatology at State University of Rio de Janeiro, currently working as global medical expert for GSK in Upper Providence, PA, USA. The other authors declare that there is no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.