
Abstract
Objective
To assess whether the care model (comprehensive vs regular) has any impact on the clinical outcomes of systemic lupus erythematosus patients.
Methods
Between August 2019 and January 2020, we evaluated SLE patients being cared for at two Peruvian hospitals to define the impact of care model on disease activity state and health-related quality of life (HRQoL). Disease activity was ascertained with the SLEDAI-2K and the Physician Global Assessment (PGA) which allows to define Lupus Low Disease Activity State (LLDAS) and Remission. HRQoL was measured with the LupusQoL. The association between care model and disease activity (Remission and LLDAS) state was examined using a binary logistic regression model. The association with HRQoL was examined with a linear regression model. All multivariable analyses were adjusted for possible confounders.
Results
266 SLE patients were included, 227 from the comprehensive care model and 39 from the regular care model. The regular care model was associated with a lower probability of achieving remission (OR 0.381; CI: 95% 0.163–0.887) and LLDAS (OR 0.363; CI: 95% 0.157–0.835). Regular care was associated with a better HRQoL in two domains (pain and emotional health). We found no association between the care model and the other HRQoL domains.
Conclusion
A comprehensive care model was associated with the probability of achieving remission and LLDAS but had no apparent impact on the patients’ HRQoL.
Keywords
Introduction
Systemic lupus erythematosus (SLE) is a multisystemic, chronic, autoimmune inflammatory disease, in which significant variability in disease activity occurs between and within patients. Patients with SLE experience significant physical, social, and psychological effects, evidenced by the accrual of damage, the deterioration of health-related QoL (HRQoL), 1 and an increased mortality. 2 For these reasons, it is imperative to identify modifiable factors associated with better disease‐related health outcomes. One of these factors could be the model of care. The care of patients with SLE is complicated by the great diversity of clinical manifestations in terms of both, the variety of organ and systems involved, and the different expression of the disease among patients. Providing quality care for patients with SLE is challenging, because many of these patients require ongoing multidisciplinary care. 3
Recently, in a Colombian study, Santos-Moreno et al. 4 showed that the model of care can affect clinical outcomes in patients with rheumatic diseases, specifically rheumatoid arthritis (RA). They showed that a higher proportion of patients under a Usual RA Care model had high disease activity while a lower proportion of them had low disease activity state compared to patients cared at the Specialized RA Center. In contrast, patients cared for at this center exhibited lower levels of disease activity, a high proportion of them were classified as being in remission while a low proportion exhibited high disease activity. 4
In Chicago, Arora et al. 3 compared the care received by SLE patients in two settings—a Lupus Clinic (LC) and a General Rheumatology Clinic (GRC) within the same academic institution. They showed that care provided at the LC or who were seen by rheumatologists with a high volume of SLE patients provided a better quality of care (including sunscreen and drug counseling, vaccination, use of steroid-sparing agents, cardiovascular disease risk assessment, among others) than the one provided at the GRC. Higher quality of care in these SLE patients was associated with better clinical outcomes such as disease activity and damage accrual. 3
These results suggest that to improve clinical outcomes in rheumatic diseases like SLE, a specific care model should be considered. “Care model” is defined as to how the health services are delivered. It refers to the health care practices and services received by patients as they progress through the stages of a condition, injury, or event 5 . The impact of care model in the course and outcome of lupus has not been formally assessed. Therefore, we carried out this study with the aim of comparing the results in disease activity status and HRQoL in SLE patients according to the model of care received, regular care (RC) model and comprehensive care (CC) model, in two Peruvian hospitals.
Methods
Patients
We conducted a cross-sectional study of SLE patients from two hospitals to define the care model associated with better disease‐related health outcomes; these patients had been evaluated between August 2019 and January 2020. We enrolled 227 patients who received CC at Hospital Guillermo Almenara Irigoyen in Lima, the capital city of Perú, and who were participants of the Almenara Lupus Cohort, and 39 patients receiving RC at Hospital III Essalud in Iquitos, the major city in the Peruvian Loreto region located in the Amazon jungle. For the sample size calculation, we assumed an effect size of 0.1, power level 90%, alpha 0.05, and number of predictors 10; the minimum required sample size was 215, and we have included 266 patients. Both hospitals belong to the Peruvian Social Security Administration system. Patients were included if they were at least 18 years of age, were willing to participate voluntarily, and had met the 1997 revised American College of Rheumatology (ACR) criteria for SLE. 6 On the other hand, patients with overlap systemic autoimmune diseases except for secondary Sjögren’s syndrome and antiphospholipid syndrome were excluded; likewise, pregnant women at the time of the study were excluded. Patients were recruited in conjunction with their scheduled outpatient visits; at that time, an interview, a clinical examination, and a review of their medical history were performed. Using a standard protocol, demographic (age at diagnosis, gender, socioeconomic status, and ethnicity), clinical, and treatment features were incorporated in our database.
Variables
Care model. At Hospital Guillermo Almenara Irigoyen, located in Peruvian’s capital city (Lima), the Rheumatology Department has a specific program for the monitoring and treatment of SLE patients; this CC program includes educational activities and regular evaluations, using standardized scales and instruments to assess disease activity and damage accrual. In addition, the medical staff of this clinic is constituted by 11 rheumatologists who all follow a similar model of care. In contrast, at Hospital III Essalud, Iquitos, a reference center of the Loreto Network which counts with an SLE registry of 47 patients, there are only three rheumatologists, who are not dedicated solely to the care of SLE patients. At this hospital, measurement scales and instruments are not applied systematically to all SLE patients, but according to the physician’s criteria as they deemed it necessary.
Disease activity was ascertained with two scales, the Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) and the Physician Global Assessment (PGA).
Remission was defined using 2021 Definition of Remission in SLE (DORIS) definition. 7 Lupus Low Disease Activity State (LLDAS) was defined using Asia Pacific Lupus Consortium (APLC) definition. 8 HRQoL was ascertained with the LupusQoL, that allows obtaining a score by domains that ranges from 0 (worst HRQoL) to 100 (best HRQoL).
Statistical analyses
Categorical variables are reported as numbers and percentages while continuous variables as medians and interquartile range (IQR). The probability of achieving or not remission and LLDAS according to the care model received was determined using a binary logistic regression model. Adjustment confounders were gender, age at diagnosis, disease duration, socioeconomic status, and the use of antimalarials. In the case of remission, the analyses compared remission versus not on remission, and in the case of LLDAS, the analyses compared LLDAS versus active.
The association between HRQoL and the model of care was examined using a linear regression model adjusted for possible confounders such as age at diagnosis, gender, disease duration, socioeconomic status, SLEDAI-2K score, use of antimalarials, prednisone dose, and immunosuppressive drugs use. For the linear regression model, the B value reflects the number of units the HRQoL is higher when the predictive variable is present. The 95% CI would be ±2 times the standard error from the regression line.
All analyses were performed using the statistical package SPSS 26.0 (IBM, Chicago, IL).
Ethics
This research project received approval by the School of Medicine, Faculty of Health Sciences, of the Universidad Científica del Sur, Lima, Perú, as well as by each hospital’s institutional review board. Only patients who signed the informed consent were included.
Results
Characteristics of SLE patients.
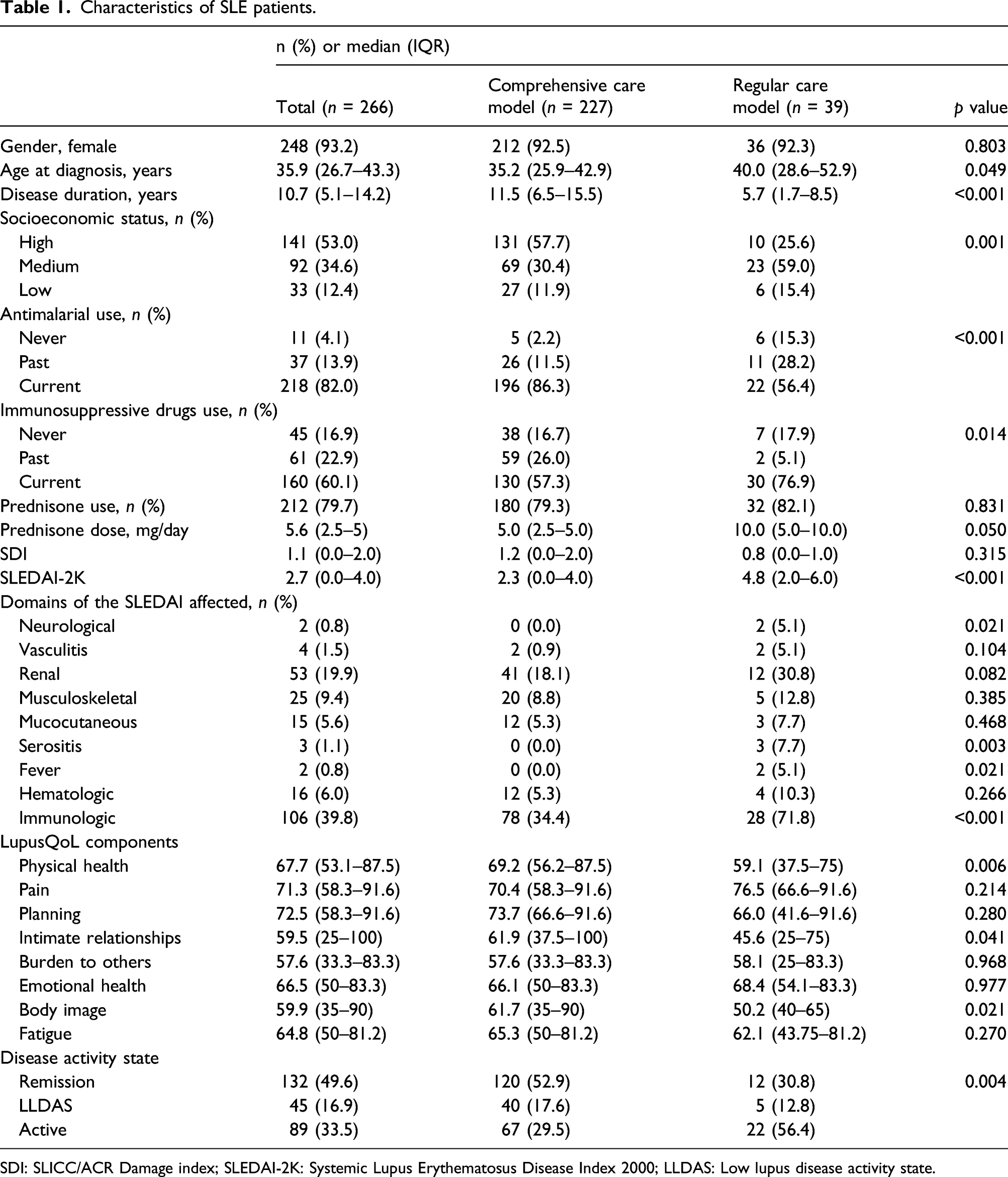
SDI: SLICC/ACR Damage index; SLEDAI-2K: Systemic Lupus Erythematosus Disease Index 2000; LLDAS: Low lupus disease activity state.
Association between disease-related outcomes and care model.
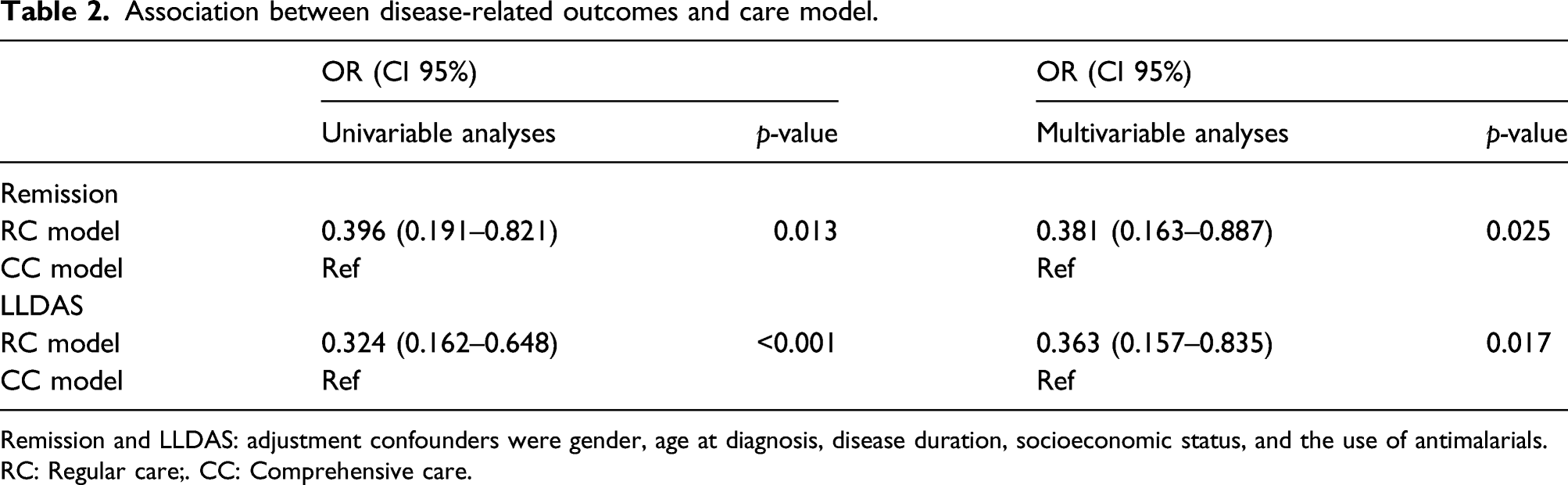
Remission and LLDAS: adjustment confounders were gender, age at diagnosis, disease duration, socioeconomic status, and the use of antimalarials.
RC: Regular care;. CC: Comprehensive care.
Regarding HRQoL, the most affected HRQoL’s domains were burden to others, body image, and intimate relationships, their medians being 57.6 (33.3–83.3), 61.7 (35.0–90.0), and 61.9 (37.5–100.0), respectively, in the CC model, while in RC model they were intimate relationships 45.6 (25.0–75.0), burden to others 58.1 (25.0–83.3), and physical health 59.1 (37.5–75.0). On the multivariable analyses, the RC model was positively associated with pain (B = 13.239; CI 95%: p = 0.003) and emotional health (B = 9.390; CI 95%: p = 0.046). Univariable and multivariable models are depicted in Supplementary Tables 3 and 4.
Discussion
The main objective of our study was to determine the impact of the care model on clinical outcomes in SLE patients. In fact, we found the care model to be associated with the probability of achieving remission and LLDAS, but not with HRQoL.
Regarding disease activity status, RC model is associated with lower odds of being in remission in comparison to the CC model. These results can be explained by the difference in patient management between both models. In the CC model, following the EULAR recommendations for monitoring SLE patients in routine clinical practice and observational studies,9,10 the level of disease activity is assessed and recorded using a standardized scale at each visit, unlike the RC model where it is evaluated when the physician deems it appropriate. The use of validated indices broadens and improves the collection of data and, consequently, allows an earlier identification of changes in level of disease activity and a quicker intervention when increases are detected. Another practice that could explain the association found is the conduct of educational activities, carried out in the CC model but not in the RC model. These could impact on treatment adherence and, as a consequence, on prognosis. These results are consistent with the report of the LuLA (Lupus-Langzeitbeobachtung, Lupus Erythematosus Long-Term Study) cohort from Germany which showed quality indicators were predictive of low disease activity, lower damage, and better HRQoL. 11 The relevance of having found the care model related to the level of disease activity is the achievement of remission and LLDAS—especially prolonged— which in turn are associated with less damage accrual, better HRQoL, and lower mortality.2,12–14
Concerning HRQoL, a better HRQoL in pain and emotional health domains was associated with RC. This could be due to the fact that HRQoL is a multidimensional concept that represents the patient’s individual general perception of the impact of the disease and/or treatment on their health. 15 Therefore, it can be influenced not only by the clinical features and the care received but also by sociodemographic, cultural, psychological, and behavioral factors and by the goals, expectations, standards, and personal concerns of each person. It should be also noted that there are differences, external to the health system, between both locations, such as climatic differences and the idiosyncrasies of the cities in which these centers are located, one in the major coastal capital city of Peru and the other in a medium size city in the Amazon region.
Our study has some limitations. First, as this was a cross-sectional study, the temporal relationship between the variables examined cannot be determined, and we cannot rule out the effect of other variables that could affect the course of the disease between diagnosis and the evaluation. Second, for the same reason, an immortal bias accounting for the differences observed between the two models cannot be rule-out. Third, as the study has been carried out in hospitals from only one Peruvian Health System, the Social Security Administration, the results cannot be extrapolated to other public and private health systems. Fourth, the relatively small sample size of the RC group precluded us from drawing stronger conclusions. Despite these limitations, by including populations from two different realities, the capital city of Perú and a regional center, these preliminary results should encourage the conduct of longitudinal studies to evaluate the true impact of potential interventions in the care model which may lead to improved clinical outcomes in SLE patients.
The main strength of this study is that it is the first to evaluate the impact of care model on disease‐related health outcomes in lupus patients in Latin America. In conclusion, the CC model was associated with a higher probability of attaining remission and LLDAS than the RC. Achieving such targets has significant impact on the prognosis of patients especially in terms of their quality of life and damage accrual over time.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Almenara Lupus Cohort was partially supported by institutional grants from EsSalud (1483-GCGP-ESSALUD-2013, 1733-GCGP-ESSALUD-2014, and the 2015 Kaelin Prize 04-IETSI-ESALUD-2016), from the Pan American League of Associations for Rheumatology (PANLAR) (2015 PANLAR Prize and the 2018 H. Ralph Schumacher MD/JCR/PANLAR Prize), and from the Fundación Instituto Hipólito Unanue and an irrestricted grant from Janssen.
Contributorship
All authors were involved in drafting or revising this article critically for important intellectual content, and all authors approved the final version to be published. Dr Manuel F. Ugarte-Gil has full access to all of the data from the study and takes responsibility for their integrity and the accuracy of the analyses performed.