
Abstract
Introduction
Medication nonadherence is common in systemic lupus erythematosus (SLE) and associated with morbidity and mortality. We explored the reliability of pharmacy data within the electronic medical record (EMR) to examine factors associated with nonadherence to SLE medications.
Methods
We included patients with SLE who were prescribed ≥1 SLE medication for ≥90 days. We compared two datasets of pharmacy fill data, one within the EMR and another from the vendor who obtained this information from pharmacies and prescription benefit managers. Adherence was defined by medication possession ratio (MPR) ≥80%. In addition to MPR for each SLE medication, we evaluated the weighted-average MPR and the proportion of patients adherent to ≥1 SLE medication and to all SLE medications. We used logistic regression to examine factors associated with adherence.
Results
Among 181 patients (median age 36, 96% female, 58% Black), 98% were prescribed hydroxychloroquine, 34% azathioprine, 33% mycophenolate, 18% methotrexate, and 7% belimumab. Among 1276 pharmacy records, 74% overlapped between linked EMR-pharmacy data and data obtained directly from the vendor. Only 9% were available from the vendor but not through linked EMR-pharmacy data. The weighted-average MPR was 57%; 45% were adherent to hydroxychloroquine, 46% to ≥1 SLE medication, and 32% to all SLE medications. Older age was associated with adherence in univariable and multivariable analyses.
Discussion
Our study showed that obtaining linked EMR-pharmacy data is feasible with minimal missing data and can be leveraged in future adherence research. Younger patients were more likely to be nonadherent and may benefit from targeted intervention.
Introduction
Medication adherence among patients with systemic lupus erythematosus (SLE) is low,1,2 and nonadherence is associated with increased morbidity and mortality.3–5 Reasons for nonadherence can be broadly categorized into difficulty acquiring medications (e.g., cost, insurance), barriers to taking medications on a regular basis (e.g., busyness/forgetting, side effects), and lack of motivation (e.g., knowledge, beliefs). 6 For complex reasons that are often outside of patients’ control, medication nonadherence is more common among Black patients with SLE and likely exacerbates known racial outcome disparities such as higher rates of end stage renal disease among Black patients. 7
An important prerequisite for research to improve medication adherence is the ability to measure adherence easily and reliably. Current methods for measuring adherence broadly include patient surveys, pharmacy refill data, therapeutic drug monitoring, and electronic Medication Event Monitoring System (eMEMS), or a device that records when medications are taken. 8 The heterogeneity in these methods, in part, contributes to large variations in medication adherence rates reported in the literature, ranging from 20 to 57% among patients with SLE. 1 Each method of ascertaining adherence has its advantages and drawbacks. 9 For example, while patient surveys are easy to obtain, they are prone to overestimate adherence due to social desirability effect. Therapeutic drug levels and eMEMS, on the other hand, provide more granular and objective measures of adherence but are more costly to implement on a large scale.
Pharmacy refill data are considered one of the most effective and objective approaches to estimating adherence on a population level. These data are conventionally obtained from insurance claims data, which are limited to certain populations like beneficiaries of a given insurance provider or closed health systems that include a pharmacy, such as the Veteran’s Health Administration. With the prevalent use of electronic medical record (EMR) systems and e-prescribing of medications, there is a growing opportunity to harvest linked EMR-pharmacy data that are updated in real time when a medication is filled. These data could be useful both for studying medication adherence at a population level as well as addressing nonadherence at the point of care. 10 Linked EMR-pharmacy data has been shown to be reliable and more complete than insurance claims data when estimating adherence to medications for hypertension. 11 In this study, we explored the reliability of linked EMR-pharmacy data for patients with SLE and used these data to examine refill adherence and factors associated with nonadherence for lupus medications.
Methods
Patient population
This is a retrospective cohort study of patients with SLE seen at the Duke Rheumatology Clinic. The Duke University Medical Center uses a single EMR system (Epic, Epic Systems).
To ensure that patients we include in the study have SLE and to maximize the number of patients with SLE included in the analysis, we identified patients who were part of either the Duke Lupus Registry (DLR), the Duke Autoimmune in Pregnancy (DAP) Registry, or the Maternal Autoimmune Disease Research Alliance Registry (MADRA). The DLR is a prospective cohort of patients with SLE followed at the Duke Lupus Clinic; the DAP (2007-2017) and MADRA (2018-ongoing) registries are prospective cohorts that collect pregnancy and postpartum data on women with any rheumatic diseases. We included unique patients diagnosed with SLE in these registries who were ≥18 years old, fluent in English, had no cognitive or other physical barriers to provide informed consent. All patient met SLE classification criteria (either American College of Rheumatology 1997 and/or SLE International Collaborating Clinics 2012 SLE classification criteria).12,13 All enrolled registry subjects provided signed informed consent to participate in research and were followed regularly as clinically indicated. These registries have been approved by the institutional review board (IRB) at Duke University (IRB study # Pro00008875 for DLR, Pro00000756 for DAP, and Pro00084014 for MADRA).
Additional inclusion criteria for this analysis were having at least one active prescription for commonly prescribed SLE-specific medications including hydroxychloroquine, methotrexate, azathioprine, mycophenolate, or belimumab, and having at least 90 days of linked EMR-pharmacy refill data available. Patients were excluded if their only prescribed SLE medication was corticosteroids. The current study was approved by the Duke University IRB (study #Pro00094645).
Data sources
We obtained pharmacy refill data in two ways: (1) directly from the vendor (Surescripts, LLC), 14 and (2) through linked EMR-pharmacy data in Epic EMR. The vendor Surescripts facilitates electronic transmission of prescriptions from EMRs to pharmacies and also links EMRs with medication fill information from pharmacies and pharmacy benefit managers through both insurance claims and pharmacy sales. 14 Linked EMR-pharmacy data is received from Surescripts in Duke’s Epic EMR and is cleaned using a structured query language script to remove duplicate records, match fields with Epic records, and combine records when necessary. The linked EMR-pharmacy data is updated in Epic for each patient whenever they have an active encounter in the health system, such as having an outpatient clinic visit or hospitalization.
We limited our scope to specifically examined refill data of hydroxychloroquine, methotrexate, azathioprine, mycophenolate mofetil and belimumab during the year 2018, when this study was conducted and EMR-linked pharmacy refill data was available. We obtained patients’ sociodemographic information from the patient registries that include age, gender, race, ethnicity, education level, annual household income, insurance status, marital status, and social support.
Data cleaning and validation
All pharmacy refill data were reviewed for medication strength and days of supply, and to remove duplicates by a statistician (DW) and a rheumatologist (AS). We determined the reliability of linked EMR-pharmacy data by comparing them to data provided directly by Surescripts based on medication names and dispense dates for missing data and overlap. After establishing their reliability, we used linked EMR-pharmacy data for the rest of the adherence analyses.
Medication adherence calculation and definitions
We calculated the medication possession ratio (MPR) as the ratio of the number of days with medication available by the number of days a patient is expected to be on medication, based on medication pick-up and order dates. We used a MPR cutoff of ≥80% to define adherence; this cutoff has been consistently applied in prior studies examining SLE medication adherence using pharmacy refill data.4,2,15
We examined 4 different definitions of medication adherence in this analysis: (1) MPR ≥80% for at least one SLE medication, (2) MPR ≥80% for all SLE medications prescribed, (3) MPR ≥80% for hydroxychloroquine, and (4) weighted-average MPR ≥80%, calculated by weighing the average MPR by expected days on each medication prescribed.
Statistical analysis
Categorical variables were described with frequencies and percentages, and continuous variables were summarized with either mean (standard deviation) or median (interquartile range (IQR)), depending upon distribution.
To compare the two sources of pharmacy refill data, we classified records as available only directly from Surescripts, available only through linked EMR-pharmacy data, and available from both sources.
We examined associations between socio-demographic characteristics and each of the definitions of adherence first in univariable analysis, then using multivariable logistic regression. For multivariable logistic regressions, variables were selected using a backward selection method with significance level to stay in the model set to 0.05. Candidate variables were selected based on their clinical relevance and included gender, age, ethnicity, race (white/non-white), education, type of insurance, registry membership, marital status, type of social support, and number of concomitant medications.
All statistical analyses were performed with SAS System 9,4 (TS1M7) at the Duke Clinical Research Institute.
Results
Patient population
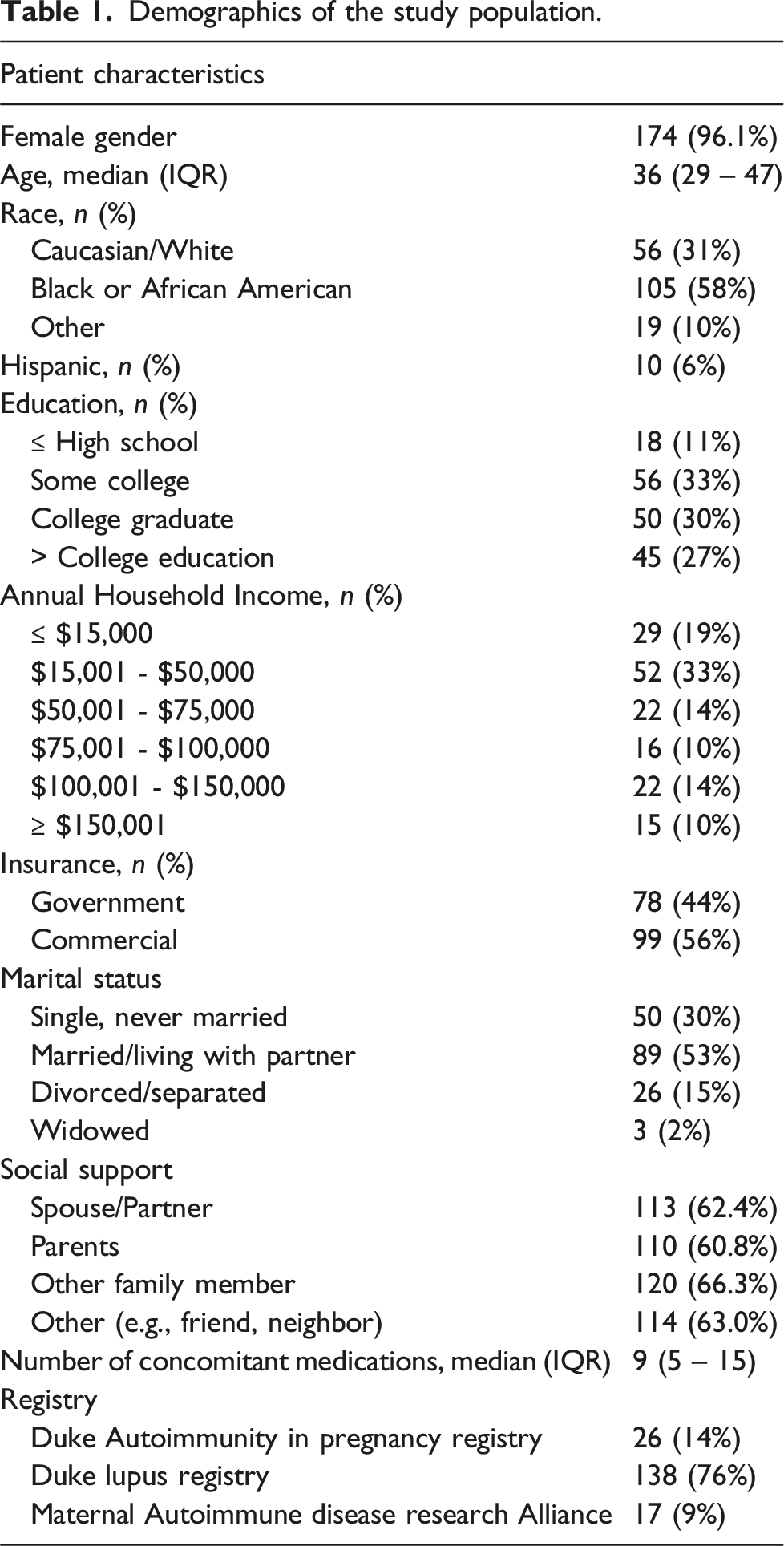
We identified 181 patients with SLE from DLR (n = 138), DAP (n = 26), and MADRA (n = 17) registries with at least 1 SLE medication prescribed during 2018, when this study was conducted (Figure 1). The median age was 36 (IQR 29-47), 174 (96%) were female, and 105 (58%) were Black. Among these patients, 18 (10%) had high school or less education, 89 (49%) were married or living with a partner, 81 (45%) had annual household income ≤$50,000, and 78 (43%) had Medicaid or Medicare insurance (Table 1). Study population flow chart. Demographics of the study population.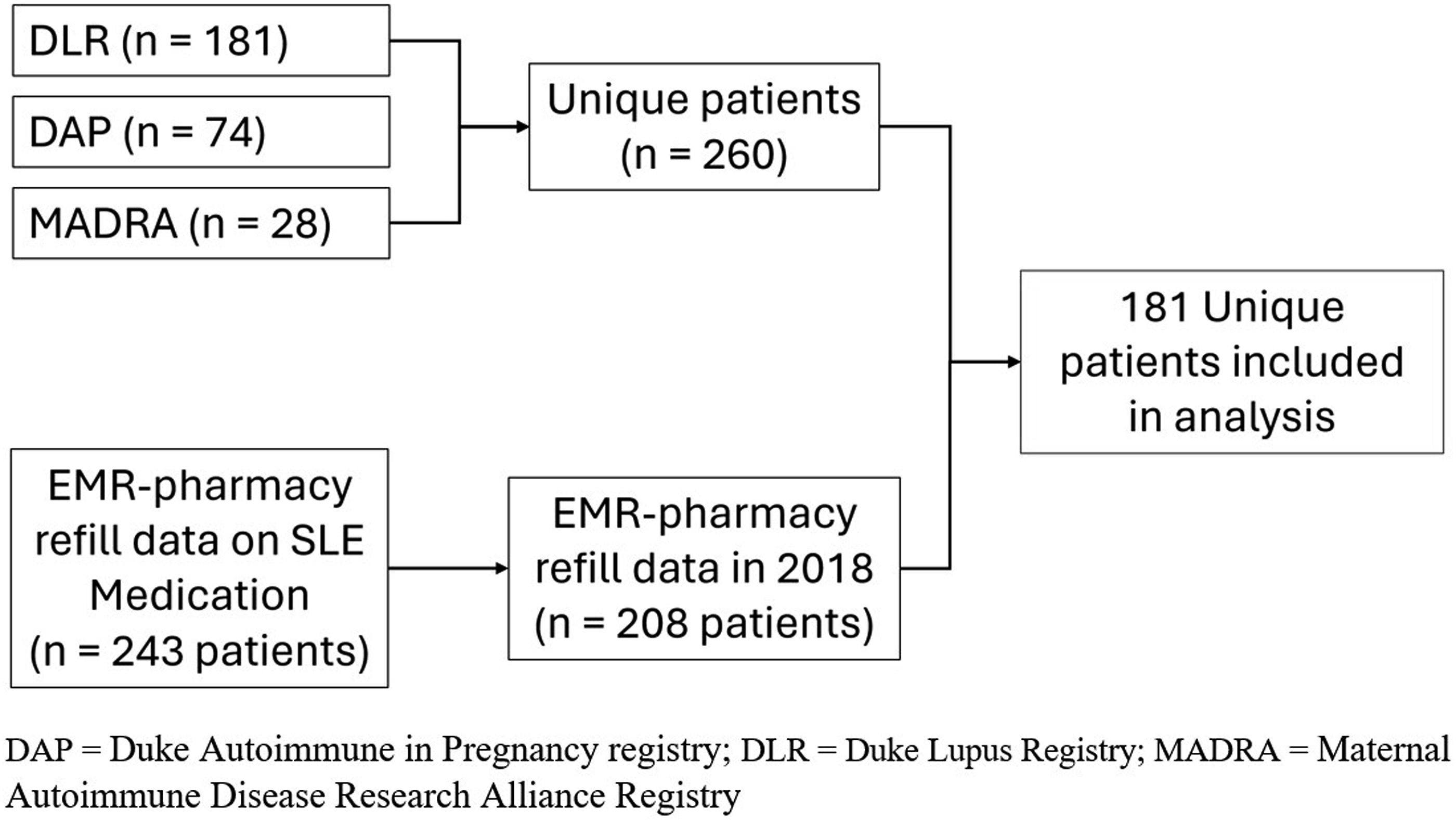
Data validation
Comparing pharmacy refill data obtained directly from the vendor Surescripts to those linked through Epic EMR, we found that among 1276 pharmacy records, 74% overlapped between the two sources, 9% were only available directly from Surescripts, and 17% were only available through linked Epic EMR-pharmacy data. Overlap between the two sources was the lowest for belimumab (49%) and did not differ by commercial (75%) or government (73%) insurance.
Medications
The majority of patients (177 or 98%) were prescribed hydroxychloroquine, 62 (34%) were prescribed azathioprine, 59 (33%) mycophenolate, 32 (18%) methotrexate, and 12 (7%) belimumab. Most patients (65%) were prescribed 2 or more SLE medications, and patients on average took a total of 9 concomitant medications (IQR 5-15).
Medication adherence
Medication adherence rates as measured by MPR ≥80% were 45% for hydroxychloroquine, 34% for methotrexate, 28% for azathioprine, 19% for mycophenolate, and 25% for belimumab. In this cohort, 84 (46%) were adherent to at least one SLE medication, 58 (32%) were adherent to all prescribed SLE medications, and 62 (34.3%) were adherent based on the weighted-average MPR. Figure 2 shows the distribution of MPR for each SLE medication. Distributions of Medication Possession Ratios for each SLE medication.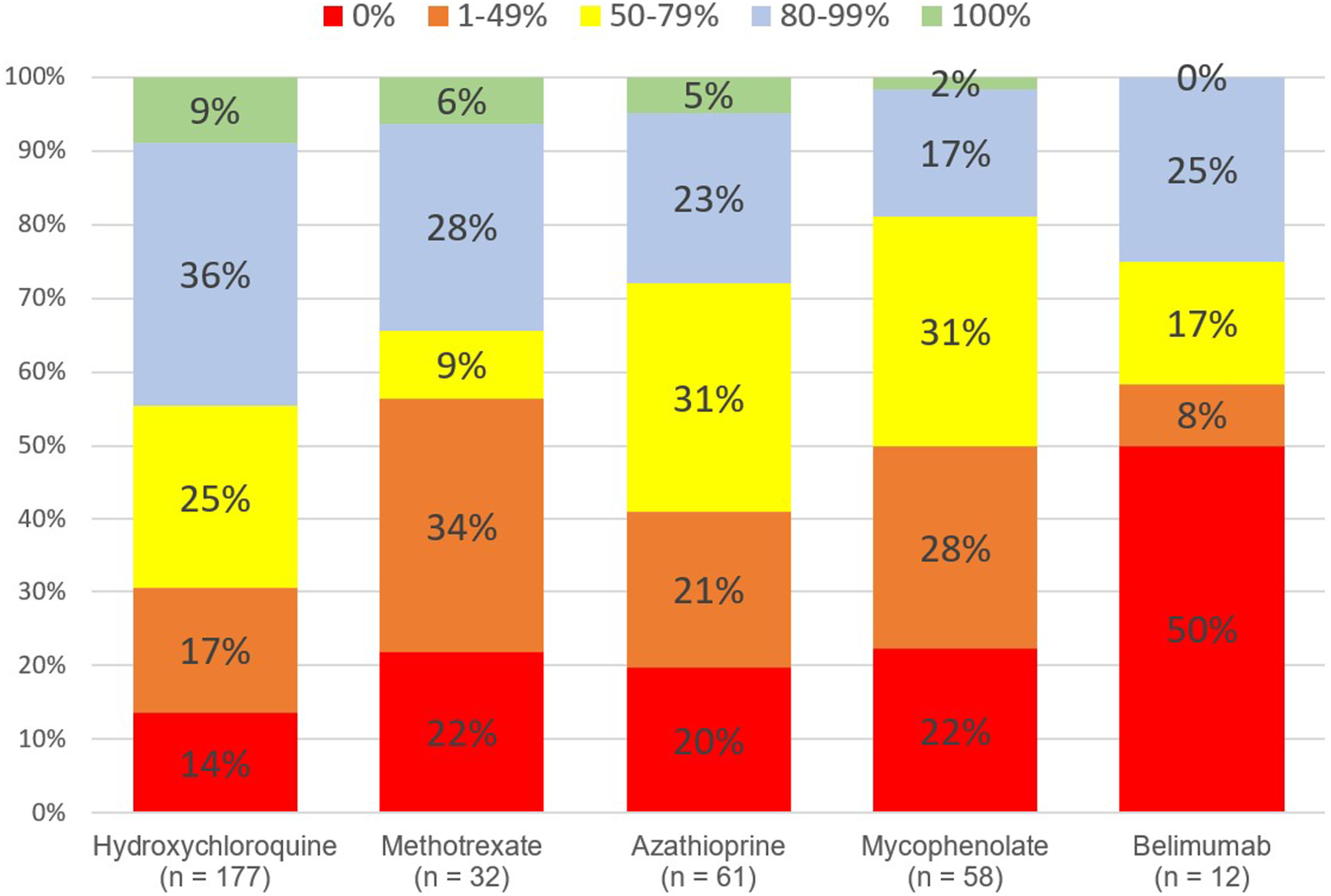
Factors associated with adherence
In univariable analysis, we found that older age was significantly associated with all 4 definitions of adherence (p = .001-.002). Additionally, White race was associated with adherence to all SLE medications (OR 2.22, 95% CI 1.15 - 4.30, p = .02) and had a trend for association with adherence based on the weighted-average MPR (OR 1.90, CI 0.99-3.64, p = .05). Gender, ethnicity, level of education, income, social support, insurance type, marital status, number of concomitant medications, and registry membership were not significantly associated with any definitions of adherence (Supplementary Table).
Multivariable logistic regression showed that older age was the only factor significantly associated with all definitions of adherence after adjusting for other sociodemographic factors.
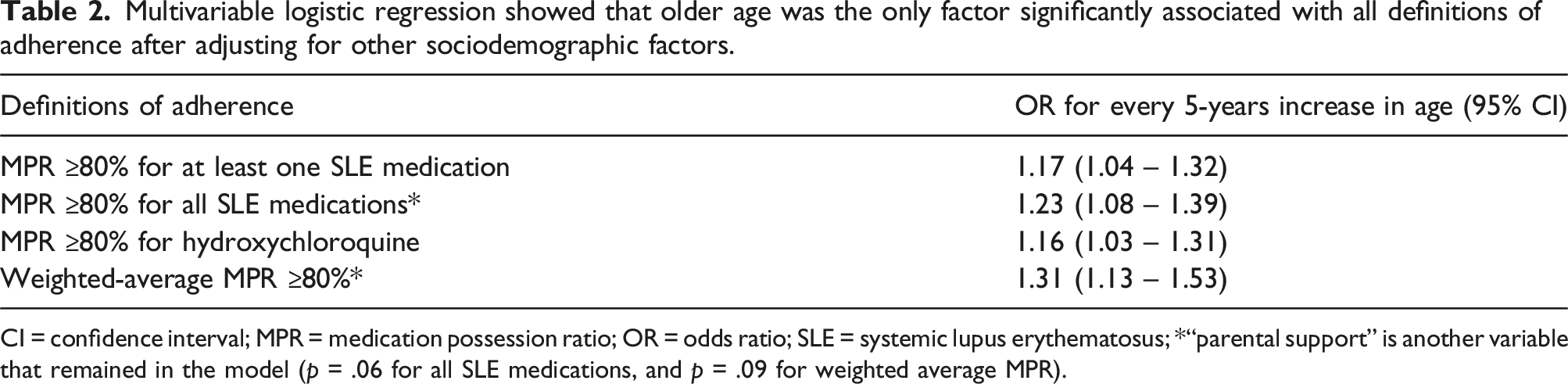
CI = confidence interval; MPR = medication possession ratio; OR = odds ratio; SLE = systemic lupus erythematosus; *“parental support” is another variable that remained in the model (p = .06 for all SLE medications, and p = .09 for weighted average MPR).
Discussion
This is one of the first studies using linked EMR-pharmacy data to examine medication adherence among patients with SLE on a population level. Our study demonstrates that obtaining this data through the Epic EMR is feasible with minimal missing data. Having access to this data, particularly in combination with registry data, can be a powerful tool for adherence research. The overall rates of nonadherence found in this study is similar to a separate study conducted in the Duke Lupus Clinic around the same time period in which adherence was assessed through calling pharmacies, 7 suggesting that the EMR-linked pharmacy data is reliable when compared to phone calls to pharmacies. Additionally, in an analysis by Blecker et al 11 of anti-hypertensive medications, EMR-pharmacy data were also found to be reliable compared to insurance claims data, with 88% of patients having pharmacy data available, and only 9% of data being missing.
Establishing the feasibility and reliability of using linked EMR-pharmacy data to assess adherence is important for several reasons. On a population level, the volume of data can be leveraged to examine changes in adherence over time within or across health systems, particularly with implementing certain policies, programs, or adherence interventions. The ability to extract pharmacy data along with data on health utilization can facilitate cost-effective analyses. On a clinical and individual level, this data can be used at the point of care, alerting clinicians to initiate conversations about SLE medication adherence. 10 Having this data readily available can increase clinician awareness of nonadherence and help standardize adherence discussions to reduce implicit bias about adherence. In fact, we have successfully used this data in clinical practice for an adherence intervention. 10 The application of linked EMR-pharmacy data extends beyond SLE to other rheumatic and chronic diseases that require long term pharmacologic treatment, highlighting the scope of its impact when used appropriately.
As reported in prior studies, we found that medication adherence was low to all SLE medications, with younger age and non-White race associated with lower adherence.7,16,1,17 Patients belonging to these groups may benefit from more targeted intervention to improve adherence. Although other factors like marital status, education, income, insurance status, and polypharmacy have been described in the literature to be associated with adherence,18–20 that was not the case in our cohort. This may be partially due to the relatively small sample size and unmeasured residual confounding.
Limitations of our study includes small sample size limiting power of our analyses. The cross-sectional nature of the study precludes drawing causal conclusions. Although the registry provides rich sociodemographic information, we have not captured drug out-of-pocket cost, other social determinants of health like food and transportation insecurity, or personal characteristics such as depression or resilience, which may also affect adherence.6,21,22 Although we compared linked EMR-pharmacy data to data obtained directly from the vendor Surescripts, we were not able to verify it against other sources. However, our prior study suggests that this data compared to refill data from calling pharmacy had minimal missing and inaccurate data. 10
Lastly, pharmacy refill is an imperfect surrogate for medication taking behavior, and refill data may not be a reliable indicator for adherence. This may be a problem particularly for medications with complicated dosing (e.g., prednisone), medications filled through specialty pharmacies (e.g., belimumab) that are not reliably connected to Surescripts reporting, or in cases of patients taking medication left over from a previous period of nonadherence. This limitation likely explains in part the low adherence observed for belimumab in our study, although linking with specialty pharmacies may have improved over time. Future work should refine methods of tracking adherence of medications like corticosteroids and biologics for which Surescripts reporting may be less reliable. Also, factors associated with refilling medications may be different from those associated with taking medications because these are different adherence behaviors. A major strength of the study is that we were able to enrich the EMR-pharmacy database with registry data, which ensured that all patients included met criteria for SLE and allowed us to examine an array of sociodemographic factors. We also examined several different definitions of adherence to ensure the robustness of our analyses.
In conclusion, we were able to leverage linked EMR-pharmacy data and registry data to analyze medication adherence among a cohort of patients with SLE. We believe that using this method is important for future adherence research both on a population level and at the point of care. Particular attention should be paid to younger, non-White patients who are at higher risk of not refilling medications regularly.
Supplemental Material
Supplemental Material - Using linked electronic medical record-pharmacy data to examine lupus medication adherence: A retrospective cohort study
Supplemental Material for Using linked electronic medical record-pharmacy data to examine lupus medication adherence: A retrospective cohort study by Kai Sun, Daniel Wojdyla, Ankoor Shah, Amanda M Eudy and Megan EB Clowse in Lupus.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research supported by pilot funding from Duke Forge. Research reported in this publication was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health (NIH 1KL2TR002554) and the American Heart Association COVID-19 Fund to Retain Clinical Scientists Award 923717. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Dr Clowse receives grant support from Pfizer, GSK, Exagen, and Immunovant and is a consultant GSK and UCB.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.