
Abstract
Background
Systemic Lupus Erythematosus (SLE) patients tend to have accelerated atherosclerosis. It mayhave a role in the impairment of cognitive function related to a decrease in cerebrovascular blood flow.
Methods
Sixty SLE patients and 61 healthy subjects as participants underwent: history taking, physicalexamination, blood examination, medication, carotid Doppler ultrasound test, and cognitive function test.We compared Carotid Intima-media Thickness (CIMT) and Montreal Cognitive Assessment IndonesianVersion (MoCA-Ina) scores of the two groups.
Result
The comparison of the total MoCA-Ina scores between the two groups was not statistically significant (p = .332). However, the orientation domain in the SLE group was statistically lower than the HS group (5.83 ± 0.41 vs 6 ± 0.00, p = .002). The SLE group was found to have a thicker anterior and posterior IMT of right carotid artery (p < .001, p = .031) and a thicker anterior IMT of left carotid artery (p < .001). There was a significant inverse correlation between the total MoCA-Ina score and the posterior IMT of the left carotid artery (r = −0.272, p = .035) of SLE patients. Atherosclerosis plaque of the right carotid artery was not associated with total MoCA-Ina score; however, there was a significant association with the attention domain (p = .023) and the visuospatial domain of MoCA-Ina (p = .018).
Conclusion
SLE patients have lower orientation domain of MoCA-Ina and thicker CIMT than healthy subjects. Atherosclerosis plaque of the carotid artery was associated with attention and visuospatial domains of MoCA-Ina.
Introduction
Systemic lupus erythematosus (SLE) is a chronic autoimmune disease characterized by multisystemic involvement with a broad spectrum of clinical manifestations. Neurologic or psychiatric manifestations, or both during SLE, occur in up to two-thirds of patients. 1 The American College of Rheumatology (ACR) Nomenclature for neuropsychiatric syndromes in SLE provided case definitions for 19 neuropsychiatric syndromes in SLE, including the presence of cognitive impairment (CI) as a separate syndrome.1,2 Cognitive impairment is one of the most common neuropsychiatric symptoms in SLE patients. The prevalence of cognitive impairment in SLE patients ranges from 23% to 60%; a selective impairment was observed in attention, verbal fluency, visuographic skills, immediate and delayed verbal and nonverbal memory, and cognitive flexibility.3,4 This Cognitive impairment has a negative impact on the quality of life and the ability to work in patients with SLE. 5
Cognitive impairment in SLE may be caused by atherosclerosis, which can impair blood flow to the brain. 6 The atherosclerotic process is accelerated in patients with SLE compared to healthy individuals due to a combination of chronic inflammatory and immune mechanisms characterized by altered lipoprotein metabolism leading to the formation of pro-inflammatory and prooxidative lipids and immune responses. Contributory factors include increased levels of oxidized lipids (such as oxidized low-density lipoprotein [LDL] and proinflammatory high-density lipoprotein [HDL]), upregulation of adhesion molecules, and upregulation of cytokines such as monocyte chemoattractant protein-1 (MCP1), tumor necrosis factor- A (TNF-A), interferon-Y (IFN-Y), interleukin-1 (IL-1), and IL-12. Auto-antibodies to oxidized lipids and immune complexes may also play a role in developing atherosclerosis in SLE. 7
Chronic inflammation and immune disorders that occur in SLE patients, such as immune complex deposition, production of various proinflammatory cytokines, complement activation, autoantibodies, and disruption of the blood-brain barrier, can also cause microvascular dysfunction in the brain. 8
Microvascular dysfunction is likely initiated by endothelium dysfunction followed by increases in vascular tone and blood-brain barrier permeability, inward vascular remodeling, vascular hypertrophy and rarefaction, leading to decreased perfusion, thrombosis, disruption of the integrity of the blood-brain barrier, and even microhemorrhage. These changes can also lead to loss of adaptive vascular responses, so it is predisposed to greater injury in the face of ischemia or other forms of brain injury. The reduction in perfusion to white matter in the brain causes cellular injury and leads to cognitive dysfunction.8,9
The atherosclerotic process can be measured using Doppler ultrasonography; This tool was used to measure CIMT and carotid plaque burden as a surrogate marker of subclinical atherosclerosis. Some studies revealed that carotid plaques were increased more than twofold in patients with SLE compared with individuals without SLE, independent of known risk factors for CVD, and progressed rapidly. 10
This study aims to compare the Carotid Intima-media Thickness (CIMT), carotid plaque, and Montreal Cognitive Assessment Indonesian Version (MoCA-Ina) Scores of SLE patients versus healthy subjects and to determine the correlation between CIMT and cognitive impairment in SLE patients.
Subjects and methods
Study design
This study is a cross-sectional study, evaluating precisely 60 SLE female patients and 61 healthy female subjects as controls. The age and education level of the two groups were matched. This study was done from September 2019 to March 2020.
Study population
The subjects of this study were SLE patients who underwent routine follow-up at the outpatient clinic of the rheumatology division or were currently being treated as inpatients at the Internal Medicine Department of Dr Hasan Sadikin General Hospital and registered in our lupus registry.
The subjects underwent history taking, physical examination, laboratory examination, medication, carotid doppler (Ultrasonography to assess blood vessel structure and function), and cognitive function test using the Montreal Cognitive Assessment Indonesia Version (MoCA-Ina). Data were obtained using a consecutive sampling technique, and the sample was not randomized. Laboratory examination, MoCA-Ina test, and carotid Doppler were done at Dr Hasan Sadikin General Hospital, Bandung. The healthy control women without SLE were recruited from the general population of Bandung Regency. The healthy control that met the inclusion criteria and did not meet the exclusion criteria was matched to patients with SLE by age and gender.
The inclusion criteria of this study were females aged 18-65, who agreed to participate in the research, filled out the informed consent form, could read and write, and finished elementary school. Exclusion criteria in this study were smoking history, poor echo window, history of significant coronary heart disease symptoms, history of angina, a history of acute myocardial infarction (AMI), symptoms of heart failure obtained from the results of physical examination, electrocardiographic results showed myocardial infarction or ischemia, SLE patient diagnosed with Type II diabetes mellitus, Systemic Lupus International Collaborating Clinics (SLICC) Damage Index score >0 with cardiovascular involvement, Glasgow Coma Scale (GCS) score <15, history of head trauma within 2 years with decreased consciousness, history of stroke (based on clinical manifestations or CT scan results), history of moderate or higher anxiety disorder based on Beck Anxiety Inventory (BAI) score, 11 a history of moderate or higher depression based on the Beck Depression Inventory (BDI) score. 12
Assessment of cognitive function
Cognitive functions were assessed using the MoCA-Ina. MoCA-Ina is a Montreal cognitive assessment (MoCA) translated into Indonesian language, which has been validated by Husein et al. they concluded from their research that Indonesian version of MoCA Test (MoCA-Ina) is a valid test instrument based on transcultural and reliable validation principles. MoCA-Ina is applicable and can be used to assess cognitive dysfunction on patients in Indonesia. 13 The time to complete the test is around 10 minutes with a total score of 30 points; 26 points or above is considered normal, and below 26 is considered a cognitive impairment. The assessment based on MoCA-Ina consists of eight domains: visuospatial ability/executive (dimensions and shapes understanding), naming (naming animals’ images), memory (memory measurement), attention (replaying the numerical rows), language (ability in using the language within sentences), abstraction (ability in using abstract), assessing the similarities of nouns, delayed recall (the ability in memorizing words with- out guidance), and orientation (the ability of orientation in understanding the years, months, days, dates, places, and cities). The total score and each cognitive domain of MoCA-Ina were scored separately. 14
Assessment of carotid IMT
A certified sonographer performed Carotid ultrasonography using a method based on the Mannheim consensus.15,16 We examined the thickness of the tunica intima-media of the carotid artery using a Vivid 7 or T8 echocardiography machine with a flat linear array transducer. The patient was examined in a supine position with the neck extended and the head turned in the opposite direction from the side of the neck to be examined. The transducer was placed laterally until the carotid bulb was visualized. The tunica intima of the carotid artery appeared as two lines on the Common Carotid Artery (CCA). The thickness of the tunica intima-media of the carotid artery was measured on the posterior wall of the CCA, approximately 5 mm from the border of the carotid bulb in a plaque-free area. Measurement of the thickness of the tunica intima-media of the carotid artery using an automatic detection program on a Doppler device. One cardiovascular specialist validated Doppler results. According to sonographic criteria, normal CIMT ≤ 0.9 mm, and we considered it thickened if CIMT > 0.9 mm, and if CIMT > 1.3 mm indicative of atherosclerotic plaque. 17
Statistical methods
Patient demographic data, laboratory values, MoCA-Ina scores, and CIMT were described as mean, SD, and percentages. Carotid plaque was a dichotomous variable (present/abnormal vs absent/normal). The Mann-Whitney test was used to compare age, education in years, lipid components, CIMT, total MoCA-Ina score, and MoCA-Ina domains between the SLE and HS groups. Carotid plaque was compared using the Chi-squared test.
We correlated the total MoCA-Ina score and its domains with CIMT by using the Spearman rank test, and we compared the total MoCA-Ina score and its domains with the Carotid plaque by using the Mann-Whitney test.
This study protocol has been approved by Hasan Sadikin General Hospital Ethics and Research Committee. All data analyses were performed using IBM SPSS version 25.0 for Windows software.
Results
Sixty SLE patients and 61 control individuals were included. We had conducted an analysis on age and length of education in both groups with insignificant p-value results (p > .05), so it can be concluded that both groups have similar age and length of education. Age (35.78 ± 10.83 vs 35.56 ± 11.69 years, p = .728), education in years (12.03 ± 2.55 vs 12.13 ± 3.36 years, p = .769), and all patients included in this study were female.
Demographic characteristics of Systemic Lupus Erythematosus patients versus controls.
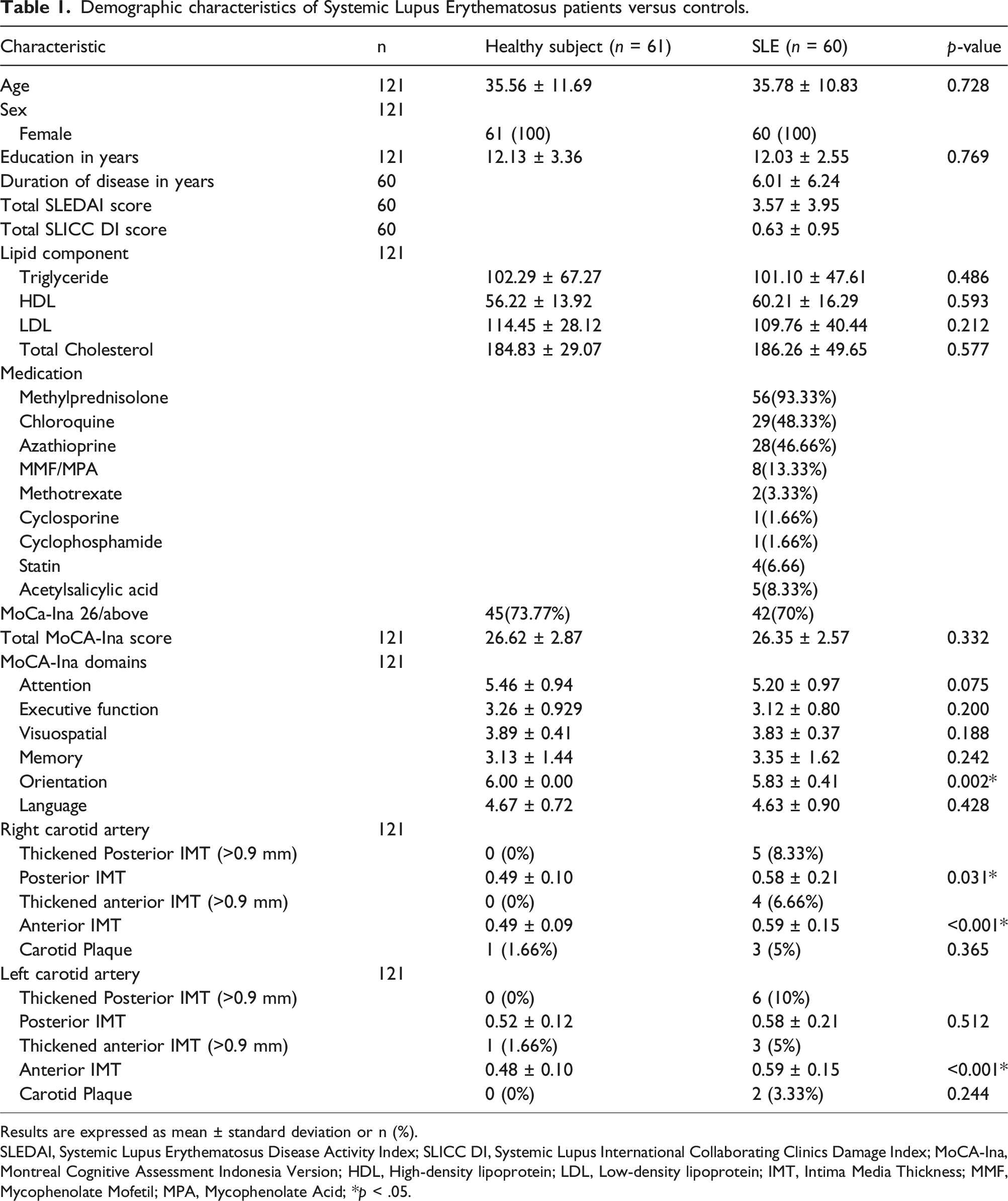
Results are expressed as mean ± standard deviation or n (%).
SLEDAI, Systemic Lupus Erythematosus Disease Activity Index; SLICC DI, Systemic Lupus International Collaborating Clinics Damage Index; MoCA-Ina, Montreal Cognitive Assessment Indonesia Version; HDL, High-density lipoprotein; LDL, Low-density lipoprotein; IMT, Intima Media Thickness; MMF, Mycophenolate Mofetil; MPA, Mycophenolate Acid; *p < .05.
Seventy percent of SLE patients had normal MoCA-Ina test (scores of 26 or above), and 30% of the patients had cognitive impairment (scores below 26). The comparison of the total MoCA-Ina scores between the two groups was not statistically significant (26.62 ± 2.87 vs 26.35 ± 2.57, p = .332); however, in the orientation domain, the SLE group was statistically lower than the HS group (5.83 ± 0.41 vs 6 ± 0.00, p = .002).
On ultrasonography examination of the right carotid artery, we found that five patients (8.33%) in the SLE group had thickened posterior IMT and four patients (6.66%) had thickened anterior IMT, and the SLE group was found to have thicker mean anterior and posterior vessel walls compared to the HS group (p = .031 and p < .001). Meanwhile, on the left carotid artery, we found that in the SLE group, six patients (10%) had thickened posterior IMT and three patients (5%) had thickened anterior IMT, and the anterior IMT was significantly thicker than that of the HS group (p < .001). The SLE group also had thicker carotid plaques than the HS group.
Correlation between MoCA-Ina score and Carotid Intima-Media Thickness (CIMT) in SLE group.
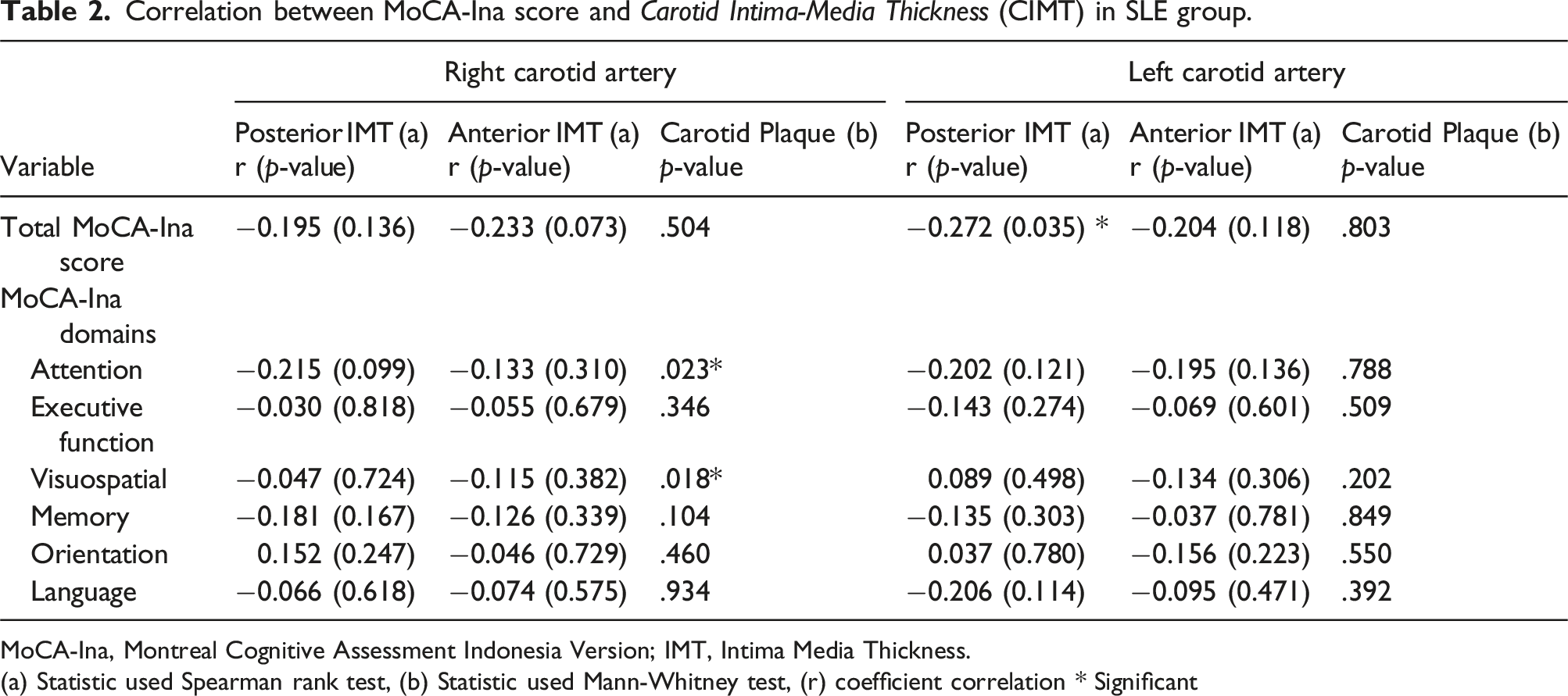
MoCA-Ina, Montreal Cognitive Assessment Indonesia Version; IMT, Intima Media Thickness.
(a) Statistic used Spearman rank test, (b) Statistic used Mann-Whitney test, (r) coefficient correlation * Significant
Carotid plaque of the right carotid artery was associated with the attention domain of MoCA-Ina (p = .023) and the visuospatial domain of MoCA-Ina (p = .018).
Discussion
This study was performed to determine the comparison between CIMT, carotid plaque, and cognitive impairment in SLE patients compared to healthy subjects, and to correlate the CIMT and cognitive impairment in SLE patients. This study showed that the CIMT of SLE patients differed significantly from healthy subjects, but total cognitive impairment did not differ significantly. However, there was a significant difference in the orientation domain, with healthy subjects having a higher score than SLE. Also, there was an inverse correlation between the total MoCA-Ina score and the posterior IMT of the left carotid artery.
Several studies have compared the CIMT of SLE and HS. This study is consistent with the existing meta-analysis by Henrot et al. on the subject that SLE patients have a significant mean difference compared to healthy subjects. Overall, the mean difference in CIMT of both carotid arteries in this study was 0.09 (95% CI [0.06 to 1.1], p < 10−5). 18 However, our study did not reveal a significant elevation in the carotid plaque frequency in the SLE patients versus healthy subjects, despite a tendency to favor SLE patients.
In this study, SLE patients with cognitive impairment (MoCA-Ina scores below 26) was 30%, whereas, in Butt et al. and Kim et al. study, it was reported that as high as 65.1% and 47.3% respectively.19,20 Kanapathy et al. study also showed that the prevalence of mild cognitive impairment was over one-third of patients with SLE. 21
This study also showed that there was no significant difference in total MoCA-Ina scores between the SLE patients and HS, and this was in contrast with the Ainiala et al. study, which showed that the prevalence of cognitive impairment among patients with SLE was twice that of the general population. 22 Various studies showed that the types of cognitive impairment associated with SLE were attention, memory, executive function, and visuospatial processing. 23 However, this study found that the orientation domain was impaired.
To the best of our knowledge, no single study correlates carotid intima-media thickness with cognitive impairments in SLE patients. Some studies have explored the relationship between CIMT and cognitive impairment in elderly patients such as a meta-analysis by David et al. found that CIMT was higher in subjects with cognitive impairment than in cognitively healthy subjects, and a study by Manabesh et al. also revealed that elevated CIMT poses a potential risk for mild cognitive impairment. This study is consistent with the results of both studies.24,25
This study showed that carotid plaque was not associated with the total score but was associated only with attention and visuospatial domains of MoCA-Ina, in which the SLE group had a lower score. In contrast, the Three-city studies, a longitudinal study including 6.025 subjects, reported that carotid plaque, but not mean CIMT, predicted subsequent dementia. 26 A postmortem study also reported that carotid stenosis was associated with increased odds of dementia, while CIMT showed no such association. 27
Cognitive impairment is one of the neuropsychiatric disorders in SLE patients. Various cognitive domains can be disrupted in this state. Pathological processes such as dysfunction of immunological factors involving immune cells, cytokines, chemokines, and antibodies will damage neuroanatomical structures. It is suggested that anti-N-methyl-D-aspartate receptor (NMDAR) and anti-ribosomal-P antibodies contribute to cognitive dysfunction in SLE patients. These antibodies recognize antigens on neuron surfaces scattered in brain areas that play a role in memory, cognition, and emotional processes. These anti-ribosomal-P antibodies will play a role in the pathogenic process by causing microvascular thrombosis and causing cognitive dysfunction. There are also Matrix metalloproteinases (MMP) secreted by neutrophils that will degrade the basal lamina and destroy the blood-brain barrier (BBB). This disruption will cause anti-NMDAR antibodies to cross the BBB and impair cognitive function. 23
Patients with SLE have white matter lesions and smaller white matter volumes in the superior longitudinal fasciculus, cingulate gyrus, and inferior fronto-occipital fasciculus than the average population. Damage to this superior white matter pathway will cause impaired executive function in SLE patients. 28 SLE patients also experience a decrease in the volume of gray matter, which plays a role in impaired visuospatial memory. 29
The carotid intima-media thickness (CIMT) is often used to predict the risk of atherosclerosis and is associated with cerebrovascular disease. This examination is a rapid and non-invasive test for atherosclerosis that is usually performed to assess the risk of stroke, whether small or large vessel disease. Many factors are associated with CIMT, including age, high lipoprotein levels, hypertension, obesity, smoking, and poor lifestyle. From a study by Su-Angka et al., carotid intima-media thickness of pediatric SLE patients was thicker in both active and inactive disease states when compared to the controls. 30
This thickening process is significant for assessing vascular damage in SLE patients. Vascular changes are caused by multifactorial factors such as inflammation, vitamin D deficiency, long-term steroid use, and autoantibodies. All those factors are essential in addition to traditional factors. 31 Medeiros et al mentioned subclinical atherosclerosis in adolescent-onset SLE patients, especially in patients with moderate to severe disease activity with predisposing risk factors, including dyslipidemia, obesity, to poor diet. 32 This is slightly different from the characteristics of this study, where the two groups have a lipid component that was not too high, and the difference in levels of the lipid component of the two groups was not statistically significant.
The thickening of carotid intima-media also affects cognitive function. A study by Zheng et al. 2020 showed that carotid intima-media thickening was an independent factor in the global decline in cognitive, memory, and executive function. 33 The same thing was also stated by Wang et al. and Sander et al., where the thickness of the carotid intima-media will increase in line with the aging process and is directly related to a decrease in cognitive function.34,35
This study showed that the thickening of the carotid intima-media had an inverse correlation with the total score of MoCA-Ina. This contrasts with the study by Komulainen et al., which found that thickening of carotid intima-media was associated with memory ability but not cognitive function in general. 36 Several pathomechanisms were suggested to determine the association between the atherosclerosis process and decreased cognitive function. The ongoing process of atherosclerosis can lead to hypoperfusion and ischemic damage to the frontostriatal area that plays a role in executive function. Although focal ischemia impairing the subcortical prefrontal pathway is generally accepted due to the atherosclerotic process, the distinction between focal, diffuse, or generalized ischemic lesions is still poorly understood in the non- dementia group. Regardless of location, focal ischemic lesions can disrupt the frontal lobes by decreasing metabolic activity and impairing brain connectivity.36,37 Atherosclerosis can disrupt cerebral blood flow and metabolism, eventually leading to neuronal dysfunction and cell death. Atherosclerosis increases the risk of stroke and white matter lesions that play a role in impaired cognitive function. 38 The process of atherosclerosis can cause a decrease in blood flow to the brain. The thickening of the carotid intima-media will make the carotid arteries more rigid, resulting in a decrease in the ability of brain autoregulation. 39
A limitation of the present study is that other risk factors for the formation of atherosclerosis, such as hypertension, diabetes, obesity, steroid usage duration, and their cumulative effects, were not included. We have no data regarding autoantibodies such as APL antibodies in our patients, which could be related to microvascular brain disease leading to cognitive dysfunction.
Further research is needed regarding the long-term increase in carotid artery intima-media thickness and its relationship to cognitive impairment.
Conclusions
There is a significant difference between the CIMT values, but not in the total MoCA-Ina Score in patients with SLE compared to healthy subjects. the only difference was orientation domain of MoCA-Ina, with the HS group scoring higher than the SLE group. We have further analyzed the data in the SLE group, and found an inverse correlation between the total MoCA-Ina score and posterior IMT of the left carotid artery, and an association between right carotid artery plaques and attention and visuospatial domains of MoCA-Ina.
Footnotes
Acknowledgments
We appreciate and thank the Rector of Universitas Padjadjaran for the Internal Research Fund of Universitas Padjadjaran that supported our work. We also want to thank Rheumatology Outpatient Clinic staff at Hasan Sadikin Hospital, Bandung.
Author contributions
UG, LH: study conception, design, writing and editing the manuscript; SH, PAO, CC, MRS: supervision of data collection and analysis, editing manuscript; HA: writing and editing manuscript; II, MA, VA, SC, KK: data collection and editing manuscript. All authors have approved the final manuscript.
Declaration of conflicting interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The authors disclosed receipt the financial support from Internal Research Funding of Universitas Padjadjaran, Bandung, Indonesia for this research.
Ethical statement
Informed consent
Written consent was obtained from all of patients involved in this study.
ORCID iDs
Data Availability Statement
Deidentified participant data are available upon reasonable request to corresponding author