
Abstract
Objective
To compare the performance of five lupus disease-activity indices measured at a single retrospective pregnancy timepoint for discriminating a composite adverse obstetric outcome (AO), and to perform exploratory clinically interpretable categorical and renal-item analyses across indices.
Methods
Retrospective cohort at a tertiary center in Bogotá, Colombia (2012–2024). For each pregnancy, one retrospective assessment with complete clinical and laboratory information required to compute all indices was selected. AO was defined as any of: preterm birth, miscarriage, stillbirth/early fetal death, preeclampsia/eclampsia, premature rupture of membranes, postpartum hemorrhage, thromboembolism, placental abruption, or maternal death. We calculated SLEPDAI, Lupus Activity Index in Pregnancy (LAI-P), modified SLAM (m-SLAM), SLE Disease Activity Score (SLE-DAS), and BILAG2004-P. Because the dataset was retrospective and selected on complete data, we treated categorical and renal-item analyses as exploratory.
Results
Twenty-nine pregnancies (28 women) were included; AO occurred in 18/29 (62.1%). The original continuous-score analyses showed overlapping confidence intervals across indices. Exploratory clinically interpretable analyses showed AO in 15/18 (83.3%) pregnancies with any BILAG2004-P A/B domain, 16/20 (80.0%) with SLEPDAI ≥3, and 13/14 (92.9%) with SLE-DAS >7.64. Exploratory renal analyses showed the clearest signals for BILAG2004-P renal A/B (13/14 vs 5/15; OR 26.0, 95% CI 2.61–259.31), SLEPDAI renal-item score >0 (13/13 vs 5/16; OR 56.45, 95% CI 2.81–1133.97), and the LAI-P renal item >0 (12/13 vs 6/16; OR 20.00, 95% CI 2.05–195.01).
Conclusion
In this small single-center cohort, active lupus was associated with adverse obstetric outcomes across disease-activity instruments. However, the study is underpowered to detect meaningful differences in discrimination between indices. Renal activity remained the most clinically relevant organ-specific signal in exploratory analyses, but these findings should be interpreted cautiously and confirmed in larger longitudinal cohorts.
Keywords
Introduction
Pregnancy in systemic lupus erythematosus (SLE) remains high-risk, with active disease associated with preeclampsia, preterm birth, and fetal loss.1–4 Pregnancy can complicate the attribution of clinical and laboratory abnormalities to lupus activity versus physiological gestational change; therefore, activity items should only be entered into a lupus activity tool when the clinician considers them attributable to lupus activity.5–7 To address pregnancy-specific attribution challenges, pregnancy-adapted indices such as SLEPDAI and LAI-P have been proposed, while SLE-DAS and BILAG2004-P offer alternative global and organ-based approaches.5–11
Evidence directly comparing these instruments within the same pregnancies, especially in Latin-American settings, is limited.7,12 We compared five indices computed at a single timepoint during pregnancy for discrimination of adverse obstetric outcomes (AO) and added exploratory analyses using clinically interpretable activity categories and renal-item information across indices.
Methods
We conducted a retrospective cohort study at Hospital de San José, Bogotá, Colombia, including pregnancies in women with clinician-confirmed SLE seen from January 1, 2012 to February 29, 2024. Pregnancies in women ≥18 years with SLE were eligible. Each pregnancy was analyzed as an independent record. Exclusion criteria were active malignancy or solid-organ transplant in the previous year.
For each pregnancy, one retrospective assessment with complete clinical and laboratory information required to compute all indices was selected. Accordingly, the analysis reflects a single-timepoint comparison rather than longitudinal disease-activity profiling throughout pregnancy.
The primary outcome was any adverse obstetric outcome (AO): preterm birth, miscarriage, stillbirth, preeclampsia/eclampsia, premature rupture of membranes, thromboembolism, postpartum hemorrhage, placental abruption, or maternal death.
We calculated SLEPDAI, LAI-P, m-SLAM, and SLE-DAS using published definitions and formulae.5–11 For BILAG2004-P, we retained domain grades (A-E). For comparability with continuous indices, we derived a numerical summary by mapping A = 12, B = 8, C = 1, and D/E = 0 and summing across domains.
Exploratory categorical analyses used clinically interpretable thresholds where feasible: any BILAG2004-P A/B domain, SLEPDAI ≥3, and SLE-DAS >7.64. Exploratory renal analyses examined the BILAG2004-P renal domain and renal items or renal-item scores from SLEPDAI, LAI-P, m-SLAM, and SLE-DAS.
Continuous variables are summarized as median (IQR) and categorical variables as n (%). Discrimination was assessed with area under the ROC curve (AUC) and bootstrap 95% confidence intervals (2000 resamples). Exploratory binary associations were summarized with odds ratios and Fisher exact tests. Gestational week at the selected assessment was not consistently retrievable for all pregnancies. The study was reported in accordance with the STROBE statement. 13
Results
Cohort characteristics, serology, treatments during pregnancy, and pregnancy outcomes.
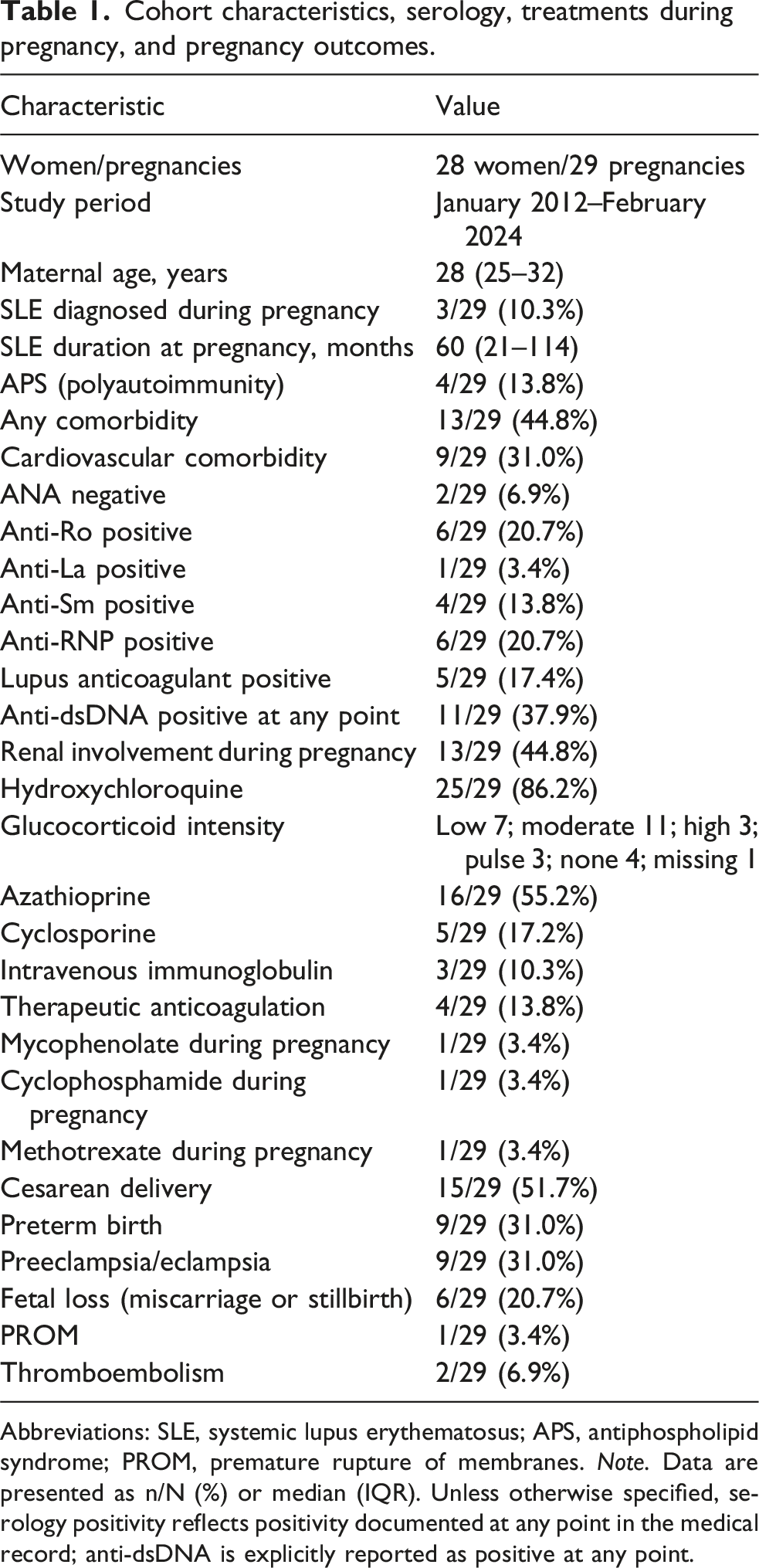
Abbreviations: SLE, systemic lupus erythematosus; APS, antiphospholipid syndrome; PROM, premature rupture of membranes. Note. Data are presented as n/N (%) or median (IQR). Unless otherwise specified, serology positivity reflects positivity documented at any point in the medical record; anti-dsDNA is explicitly reported as positive at any point.
SLE was diagnosed during pregnancy in 3/29 pregnancies (10.3%); the remaining pregnancies occurred in women with established SLE. Median disease duration at pregnancy was 60 months (IQR 21–114). Polyautoimmunity with antiphospholipid syndrome (APS) was documented in 4/29 (13.8%).
Treatment during pregnancy included hydroxychloroquine in 25/29 (86.2%). Available glucocorticoid-intensity data were categorized as low in 7, moderate in 11, high in 3, pulse in 3, none in 4, and missing in 1 pregnancy. Azathioprine was used in 16/29 (55.2%), cyclosporine in 5/29 (17.2%), IVIG in 3/29 (10.3%), and therapeutic anticoagulation in 4/29 (13.8%). Exact daily prednisone dose was not consistently available retrospectively.
Distribution of lupus activity indices at the selected single-timepoint assessment and exploratory clinically interpretable categories for adverse obstetric outcomes.
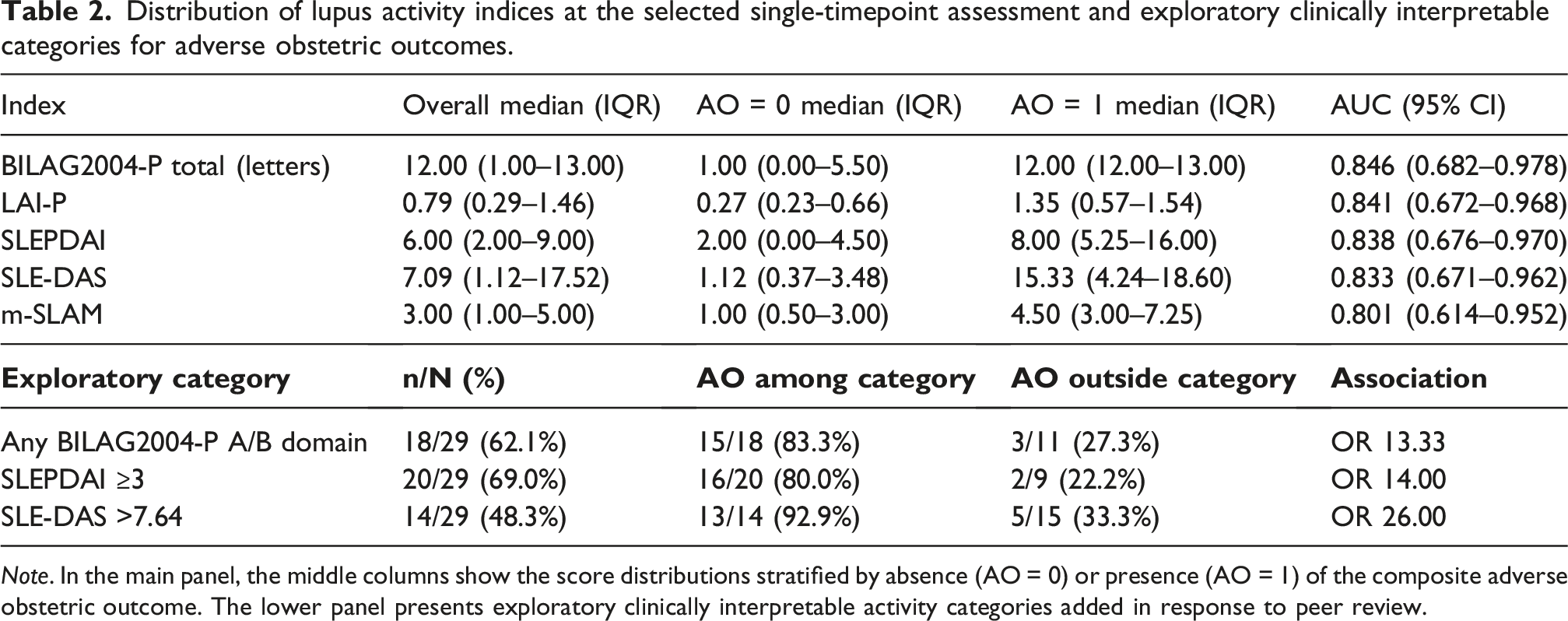
Note. In the main panel, the middle columns show the score distributions stratified by absence (AO = 0) or presence (AO = 1) of the composite adverse obstetric outcome. The lower panel presents exploratory clinically interpretable activity categories added in response to peer review.
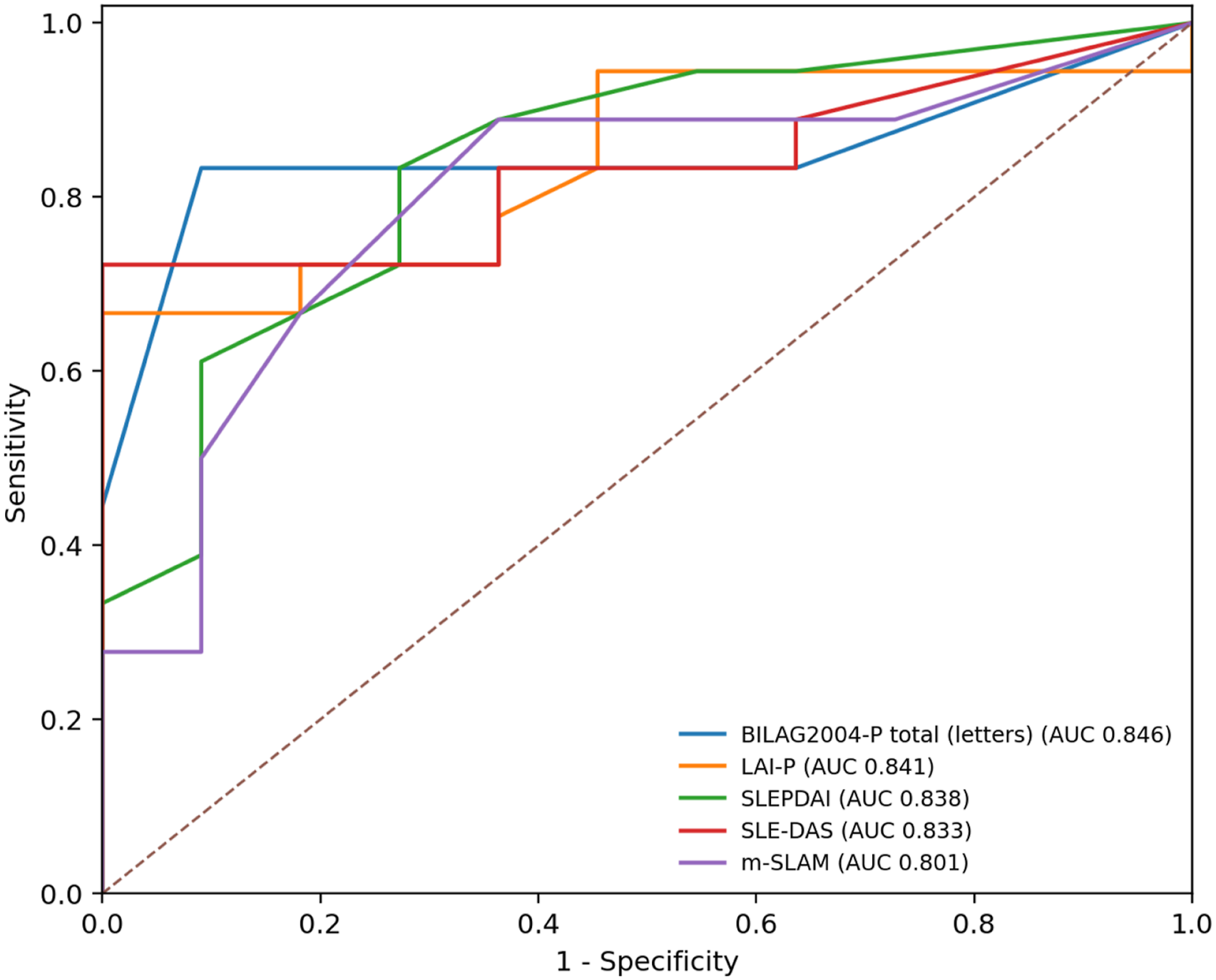
ROC curves comparing discrimination for the composite adverse obstetric outcome across activity indices. The figure is presented for visual comparison only; given the small sample size and overlapping confidence intervals, it should not be interpreted as evidence of superior discriminatory performance of any one index.
To improve clinical interpretability, we added exploratory categorical analyses. AO occurred in 15/18 (83.3%) pregnancies with any BILAG2004-P A/B domain versus 3/11 (27.3%) without active A/B domains; in 16/20 (80.0%) pregnancies with SLEPDAI ≥3 versus 2/9 (22.2%) with lower activity; and in 13/14 (92.9%) pregnancies with SLE-DAS >7.64 versus 5/15 (33.3%) otherwise (Table 2).
BILAG2004-P domain-level findings and exploratory renal activity across indices.
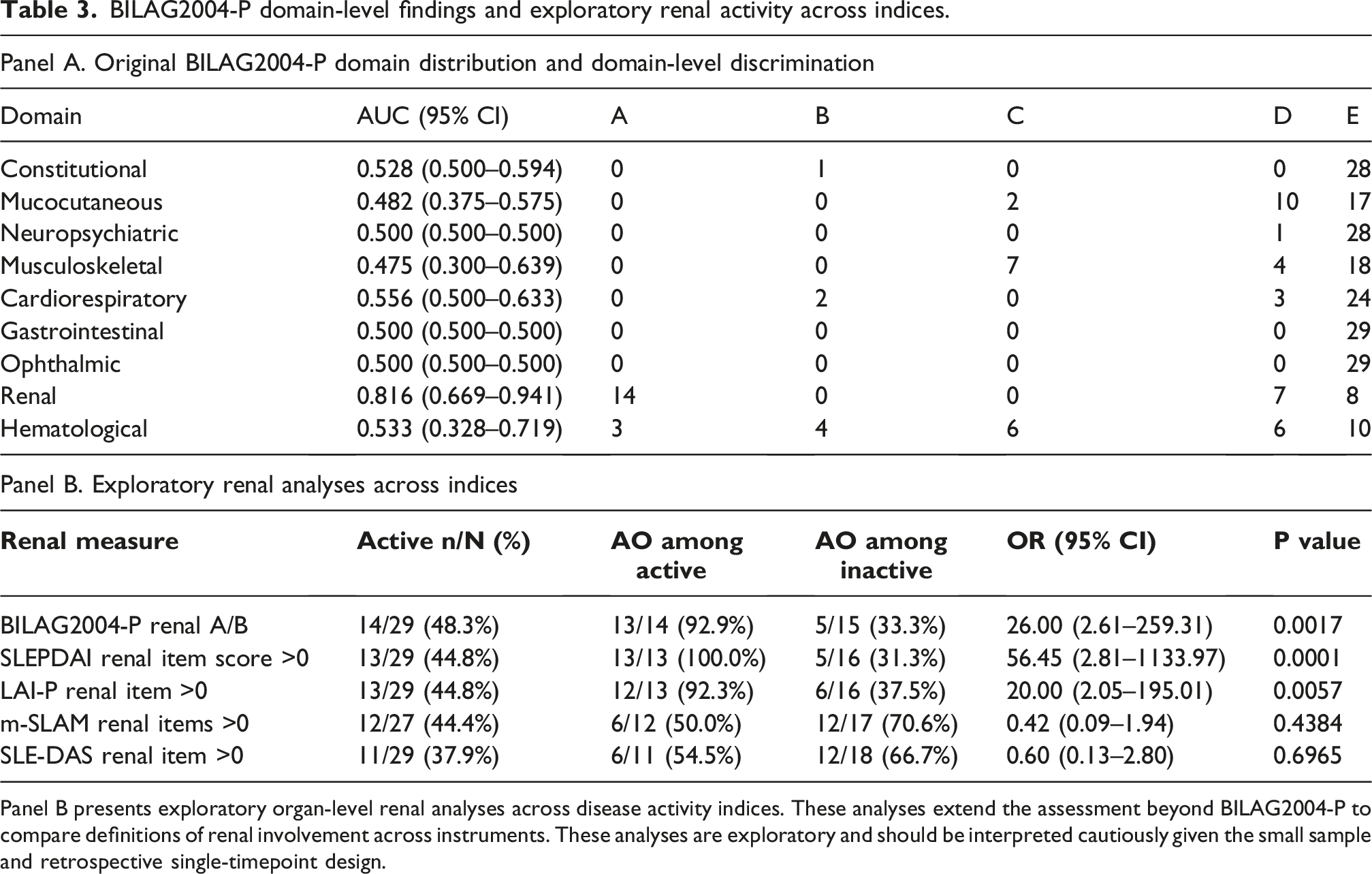
Panel B presents exploratory organ-level renal analyses across disease activity indices. These analyses extend the assessment beyond BILAG2004-P to compare definitions of renal involvement across instruments. These analyses are exploratory and should be interpreted cautiously given the small sample and retrospective single-timepoint design.
Discussion
In this cohort, several lupus disease-activity instruments measured at a single retrospective pregnancy timepoint were associated with adverse obstetric outcomes.1–4 However, the sample is too small to support formal claims that one index discriminates better than another, and overlapping confidence intervals should not be interpreted as evidence of superiority or rank ordering.
The revision also clarifies an important conceptual issue: activity instruments do not themselves misclassify physiological pregnancy changes; rather, pregnancy makes attribution more challenging, and attribution remains the responsibility of the clinician before scoring an instrument.5–7
The exploratory categorical analyses were added to improve bedside interpretability. These analyses should not be over-read as validation of thresholds in pregnancy, but they help contextualize the continuous-score findings in clinically familiar terms.10–12
The exploratory cross-index renal analyses suggest that renal activity remains a key risk signal in this dataset and that this information can also be captured using renal items from SLEPDAI and LAI-P.1–4,14 At the same time, the weaker signals observed for the renal items available in m-SLAM and SLE-DAS illustrate how unstable organ-specific comparisons can be in a very small retrospective sample.
From a practical perspective, this study does not support recommending pregnancy-adapted indices as superior to non-pregnancy-adapted indices. Index selection in routine care should also consider feasibility, continuity of longitudinal follow-up, and the specific clinical question.7–9,12,15,16 Using several instruments at each visit would add administrative burden, and changing instruments across preconception, pregnancy, and postpartum care may hinder longitudinal assessment of flares and improvement.
The rationale for not including DORIS or LLDAS definitions is based on data limitations. Because this retrospective dataset lacked consistently captured PGA and exact daily prednisone dose, these targets could not be operationalized reliably. SLE-DAS-based states may be of interest in future work, but were beyond what could be robustly supported here. 12
This study has several additional limitations. These include the small sample size, single-center design, retrospective scoring of all instruments, possible misclassification of subjective items, selection bias introduced by restricting the analysis to one assessment per pregnancy with complete data, incomplete availability of gestational week for the selected assessment, inability to distinguish persistent activity from short-lived flare, and instability of comparative discrimination estimates with few outcome events. Therefore, the renal and categorical analyses should be interpreted as exploratory and hypothesis-generating.
Conclusions
In this single-timepoint retrospective analysis of pregnancies complicated by SLE, active lupus was consistently associated with adverse obstetric outcomes across disease-activity instruments. The study does not demonstrate superiority of any index, because it is underpowered for formal comparative-performance claims. Exploratory analyses identified renal activity as the most clinically relevant organ-specific signal, particularly when captured by BILAG2004-P, SLEPDAI, and LAI-P renal measures. These findings should be validated in larger multicenter cohorts with repeated assessments across pregnancy.
Footnotes
ORCID iDs
Ethical consideration
The study was approved by the Hospital de San José Human Research Ethics Committee (CEISH), Act 511-2023.
Author contributions
Jairo Cajamarca-Barón: Conceptualization, Methodology, Investigation, Data curation, Formal analysis, Writing - original draft, Writing - review & editing, Project administration. Catalina Sanmiguel-Reyes: Investigation, Data curation, Writing - review & editing. Juan Esteban Bedoya-Loaiza: Investigation, Data curation, Writing - review & editing. Claudia Ibáñez: Methodology, Formal analysis, Validation, Writing - review & editing. Alejandro Escobar: Investigation, Resources, Writing - review & editing. Diana Guavita: Investigation, Resources, Writing - review & editing. Adriana Rojas-Villarraga: Conceptualization, Methodology, Supervision, Validation, Writing - review & editing. All authors reviewed the manuscript critically, approved the final version, and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data underlying this article are not publicly available because they contain potentially identifiable clinical information from a small single-center cohort. De-identified data may be made available from the corresponding author on reasonable request, subject to institutional and ethics approval.
Generative AI statement
During the preparation of this paper, the authors used ChatGPT to improve the readability and language of the manuscript. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.