
Abstract
Objective:
Some complementary and integrative health (CIH) therapies are recommended for the management of chronic musculoskeletal pain, but little research has evaluated how these alternatives affect downstream healthcare utilization, including imaging costs.
Methods:
Using US Department of Veterans Affairs (VA) Veterans Health Administration electronic health record data, we conducted propensity score modeling, allocating 2,215,231 Veterans with chronic pain using the VA from 2018 to 2022 into two therapy exposure groups – acupuncture with and without movement therapies (yoga or Tai Chi/Qigong) – compared with conventional care, or primary care management alone, to examine differences in imaging costs during a 6-month period following indexing. We calculated the probability of treatment in either exposure group based on demographic and clinical characteristics, and applied a nearest neighbor matching algorithm for subsequent estimation of average treatment effects.
Results:
Veterans using acupuncture with or without movement therapies had sizable baseline clinical needs and healthcare utilization. After matching, we found that imaging costs and visits were higher among Veterans using acupuncture with CIH movement therapies (cost difference $140, 95% confidence interval (CI) $97–$183; visit difference 0.37; 95% CI 0.30–0.45) and without CIH movement therapies (cost difference $155, 95% CI $147–$163; visit difference 0.34; 95% CI 0.33–0.35) during the 6-month follow-up period, compared with those using conventional care.
Conclusion:
Veterans using acupuncture with or without CIH movement therapies had greater imaging costs than those using conventional care, possibly reflecting higher usage of healthcare among integrative therapy patients. These results also suggest unobserved patterns of comorbidity, recovery or access and/or radiology inefficiencies leading to an imaging loop effect as potential considerations for future investigation.
Keywords
Introduction
Chronic pain is associated with higher healthcare costs and the treatment of chronic pain is more costly than the treatment of other chronic conditions in the United States. 1 However, costs can vary depending on the stage of pain development, the impact of such pain and the type of treatment or healthcare use in question. 2 In addition, the treatment of pain can lead to overuse of care along the continuum of nonsurgical and surgical medical treatments, including diagnostic tests, nonsteroidal anti-inflammatory drugs, opioids, analgesic injections and unnecessary surgical procedures.3,4 Such overuse can be particularly wasteful when treating normal levels of age and functionally appropriate pain, potentially causing more harm than benefit, as well as squandering valuable healthcare resources. 5
Part of the conundrum of pain management is the effective balancing of the medical treatment of pain with integrative approaches. Mounting evidence suggests that complementary or alternative medicine can be a suitable substitute for or add-on to allopathic treatments, with fewer side effects and potentially lower costs. 6 The literature shows that nonpharmaceutical and nonsurgical treatments (e.g. physical therapy and exercise) can be just as effective as and have a more favorable side-effect profile than surgical treatments and medication.7,8
A growing body of research has demonstrated the effectiveness of nonmedical interventions such as complementary and integrative health (CIH) therapies for pain, which are oftentimes cost-effective in comparison with diagnostic tests, pharmaceutical and invasive treatments, and early-stage or routine conventional care.9 –11 One such intervention is acupuncture, which is effective for some patients in the management of musculoskeletal pain. Acupuncture activates the self-healing capacity of the body through its effects on the nervous system and can be a first choice for pain management before medical treatments, depending on its availability, which differs by healthcare system and setting.12 –15 Movement therapies such as yoga, Tai Chi and Qigong are also effective at pain management and can improve physical functionality through strength training and joint flexibility. 16 Separately, acupuncture, yoga, Tai Chi and Qigong are evidence-based therapies for managing chronic musculoskeletal conditions, particularly low-back, neck and shoulder pain.14,15,17 Although very few studies have examined their shared effectiveness as a single intervention, acupuncture paired with movement therapies, such as yoga, is recommended to not only reduce and manage pain, strengthen muscles and optimize joint mobility, but also to promote an active and engaged lifestyle in support of long-term health.18 –21
However, while studies have evaluated the degree to which non-allopathic interventions generally reduce healthcare utilization and costs among patients with chronic pain, few have rigorously investigated the associated costs of CIH therapies on the most frequently billed specialty care in the US healthcare system: imaging and radiology. 22 As has been noted in the literature, imaging is overused in US healthcare, particularly among patients with pain, and is a contributing factor to overspending in non-integrated and integrated healthcare systems alike, including the US Department of Veterans Affairs (VA).22,23 Ideally, CIH therapy use would be associated with fewer healthcare costs, including imaging expenditures, as a complementary and cost-effective form of pain management. However, the use of specialty care, including CIH therapies, is associated with imaging use before such specialty care referrals, as well as increased use of other forms of healthcare in the aftermath.24,25 In addition, routine imaging is suggested for serious, progressive conditions such as pain, despite its potential side effects, and postponing initial imaging until an intervention or trial has been completed is sometimes recommended for the treatment of pain and other long-term, degenerative conditions. 26 Furthermore, evidence indicating the cost-effectiveness of acupuncture and movement therapies in terms of downstream health service utilization is sparse and presents a mixed set of findings demonstrating both increased and decreased healthcare utilization subsequent to the therapeutic intervention.27 –29
Because CIH therapy use is differentially associated with downstream health service utilization, including imaging use as a potential precursor to and outcome following referral, we examined the effect of acupuncture with or without yoga, Tai Chi and Qigong movement therapies on imaging costs in this non-randomized observational study of a national sample of patients with chronic musculoskeletal pain at the VA. Using propensity score methods, we compared these two Veteran patient exposure groups to a conventional care patient control group using nearest neighbor matching methods, estimating the average treatment effects of total imaging costs between each exposure group and its respective comparison group.
Methods
Study setting and participants
We examined a national cohort of 7,361,398 Veterans receiving care at the VA between 1 October 2017 and 30 November 2022. Among these, we identified, via the VA’s electronic health record (EHR), a cohort of 2,873,610 Veterans with chronic musculoskeletal pain, which we defined as having two or more diagnoses of back, fibromyalgia, headache, limb, chest, neck, ear or other pain occurring within at least 90 days of each other but no more than a year apart. These diagnoses were collected with reference to the last qualifying VA visit in each fiscal year, meaning a member of the cohort had received a chronic musculoskeletal pain diagnosis before the last primary care visit of each fiscal year (1 October to 30 September annually). From the medical records, we then obtained measures of Veterans’ acupuncture, yoga, Tai Chi and Qigong use at the VA and in community care settings paid for by the VA in each fiscal year. We limited the fiscal year 2022 visits to 31 March 2022 to allow for a full 6-month follow-up period after indexing across the entire 5-year timeframe until the end of fiscal year 2022. We excluded duplicate visits and duplicate scrambled patient identifier social security numbers by keeping the first visit by social security number. This study was declared a quality improvement project by the institutional review board (IRB) and was, therefore, exempt from oversight by the IRB.
Main measures and covariates
Total imaging costs and imaging visits
Two separate outcome variables were used, including total outpatient and inpatient radiology costs and visits, using data from the VA’s Managerial Cost Accounting Office as total outpatient and treating specialty inpatient National Data Extracts for a 6-month follow-up period after the index date. 30 Total imaging dollars in 2018 through 2021 were adjusted for inflation relative to 2022.
Exposure groups
We defined movement therapies as receiving any of the three yoga, Tai Chi or Qigong visits between 1 October 2017 and 30 September 2022. We created two exposure groups consisting of patients: (1) receiving acupuncture with CIH movement therapies; and (2) receiving acupuncture without. We indexed acupuncture without movement therapy patients based on the first acupuncture visit that occurred after their earliest chronic musculoskeletal pain diagnosis. Indexing of chronic musculoskeletal pain patients receiving acupuncture in addition to movement therapies was a multistep process. First, among chronic musculoskeletal pain patients, we identified each instance of three yoga, Tai Chi or Qigong visits occurring within 90 days of each other after their earliest diagnosis. We then found the first acupuncture visit after their diagnosis that occurred within 14 days of one of these three instances of yoga, Tai Chi or Qigong visits. Finally, we indexed these CIH movement therapy visits on the first of these four visits, regardless of which of the four CIH therapies it was. We excluded 549,577 patients who died within 6 months of the index date or who experienced paraplegia, quadriplegia, spinal cord injury, ankylosing spondylitis, stroke, meningitis or cancer, or who were pregnant or in long-term care. We also excluded 108,802 Veterans who were considered to have received an insufficient dose of CIH movement therapies (as defined above).
Control groups
We compared the two CIH therapy exposure groups to two corresponding allopathic conventional care control groups. We defined conventional care as the receipt of primary care, including the use of pharmacologic treatments, referrals to physical therapy or lifestyle counseling and, in some cases, referral to specialty care, but no acupuncture or CIH movement therapies (as described above).
Baseline covariates
Covariates included patients’ demographics, health conditions and healthcare utilization, all of which are related to exposure to CIH therapies, for example, comorbidity and pain clinic or physical therapy utilization. 31 These also represent a group of covariates nearing the complete set of confounders that predict exposure, co-vary with imaging costs and can be effectively balanced between the exposure and control groups. 32 These covariates included gender, age, race, ethnicity, marital status, rurality, distance to primary care, smoking status, Elixhauser comorbidities, number of chronic musculoskeletal pain sites, time since first chronic musculoskeletal pain diagnosis, service-connected disability (disability caused by military service), mental health utilization, anxiety, depression, post-traumatic stress disorder (PTSD), pain clinic utilization, physical therapy utilization, opioid use, year of entry into cohort, and months to last VA utilization. The purpose of the last utilization measure was to address the potential for immortal time bias in the conventional care control group, who may have utilized VA healthcare less (or not at all) after entry into the study.
Propensity score matching
Propensity score matched samples for both exposure groups were created through nearest neighbor matching methods given the probability of treatment based on baseline demographic and clinical characteristics with a one to many matching ratio, where each treated observation was matched with the best allopathic conventional care control unit, followed by the second best and onward for an average of five comparison units for each treated individual in the acupuncture without movement therapies exposure group and an average of eight in the acupuncture with movement therapies exposure group, to allow for effective balancing of each the exposure and control group. 32 Ties were calculated through deterministic ordering over each run of one or more matches per treated observation to produce the same results in case of repeated matching algorithms. 33 We fit two propensity score models predicting the likelihood of using acupuncture without movement therapies and the likelihood of using acupuncture with movement therapies. Observable covariates were used to predict exposure in both the acupuncture with and the acupuncture without movement therapies groups. A Consolidated Standards of Reporting Trials (CONSORT) diagram illustrating patient inclusion into and exclusion from the study, progressing from chronic musculoskeletal pain diagnosis to the refinement of the analytical data set after nearest neighbor matching of each exposure and allopathic conventional care control group, is presented in Figure 1.
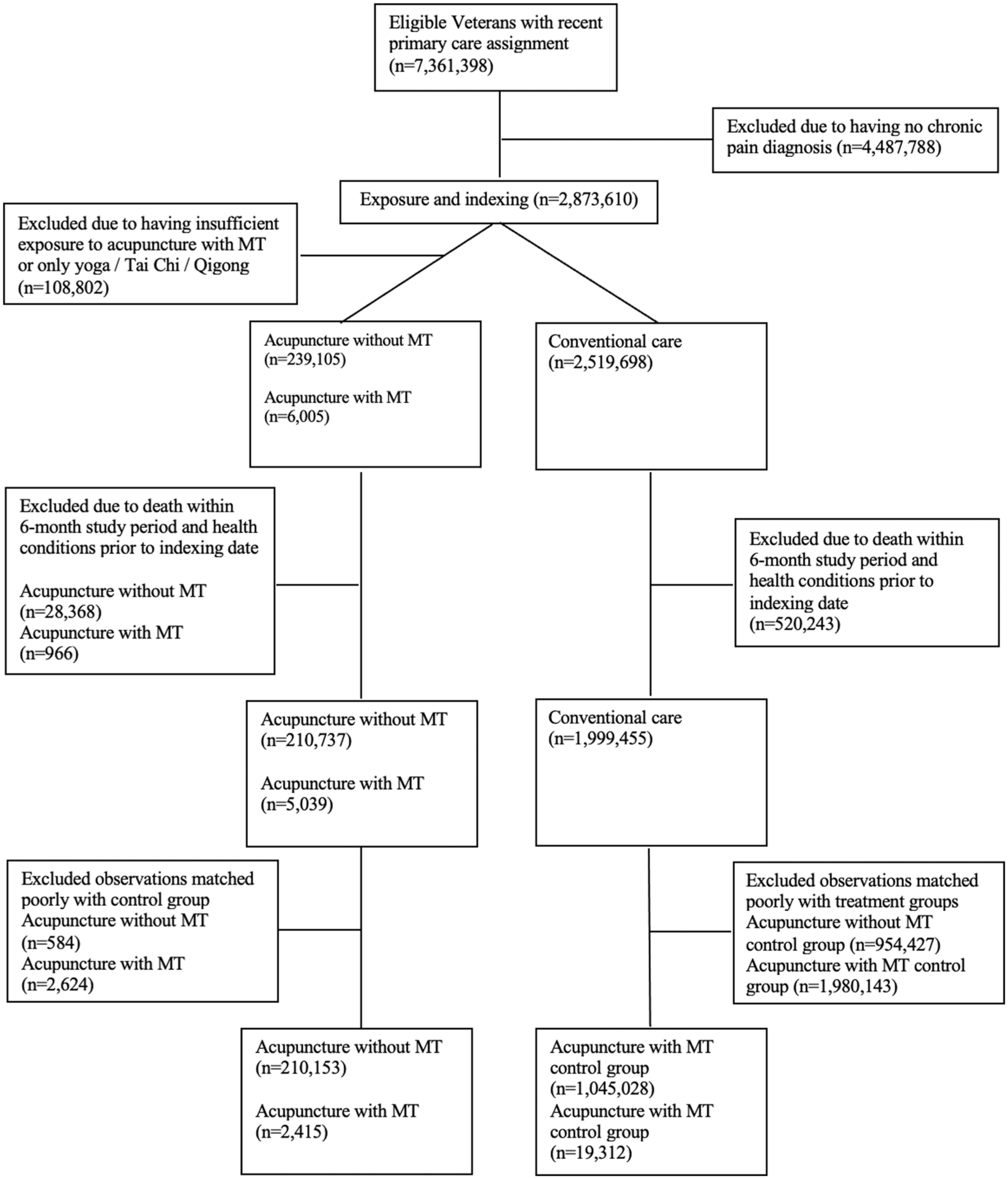
Consolidated Standards of Reporting Trials (CONSORT) diagram of study participant allocation.
Statistical analyses
For baseline characteristics of the exposure and control groups, we generated descriptive statistics, including frequency and proportion (n (%)) for categorical measures, mean ± standard deviation (SD) for continuous measures and median [interquartile range] for non-normally distributed continuous measures. For each continuous measure, we also calculated its standardized mean difference (SMD) – the difference in means between the exposure and control groups divided by the pooled SD – measuring the quality of matches across each covariate between the exposure groups, conventional care control groups and the overall chronic musculoskeletal pain cohort, before and after propensity score matching.
Imaging cost and utilization average treatment effects of those treated were calculated for the matched samples of both exposure groups and their respective control groups, representing a doubly adjusted set of imaging use regression analyses on baseline covariates after achieving a quality treatment and control group match, corresponding to the average effect of exposure relative to no exposure among treated patients. The imaging cost average treatment effects were calculated using a linear estimator for imaging dollars as an outcome, and the imaging utilization average treatment effect analyses were calculated using a negative binomial estimator for overdispersed visit counts. These effects represent the difference between the exposure and control groups, accounting for the counterfactual of the exposure group. More specifically, these outcomes compare average total imaging costs and use among treated patients’ combined and predicted costs to average control patients’ combined and predicted costs and use, mimicking the exposure group without treatment. We tabulated average treatment effect estimates, showing the effect of each exposure, its conventional care control, and the difference or contrast between the two. We also conducted sensitivity analyses, adjusting for baseline imaging costs and utilization to test for confounding of imaging use before acupuncture and movement therapy referral.
Results
Table 1 shows the demographic and clinical characteristics of Veterans in both exposure groups (those using acupuncture with or without movement therapies) and Veterans in the conventional care control group before matching. Veterans using acupuncture with movement therapies had substantial comorbidity (Elixhauser comorbidity index 4.1 ± 1.9), anxiety (59.1%), depression (66.4%) and PTSD (55.4%). A considerable proportion of them had utilized pain clinics or physical therapy in the past 30 days: 23.1% and 56.9%, respectively, with a corresponding number of utilizations over the past year (3.2 ± 7.4 and 8.5 ± 14.2, respectively). In addition, this group had nearly 30 months of utilization from indexing to patients’ last recorded visit across the 5-year timeframe (29.0 ± 14.7). Veterans in the acupuncture without movement therapies exposure group also had sizable comorbidity (Elixhauser Comorbidity Index: 3.5 ± 1.9), anxiety (47.6%), depression (53.4%) and PTSD (46.2%), as well as significant pain clinic and physical therapy use, both recently (9.3% and 17.1%, respectively, in the past 30 days) and over the past year (1.0 ± 3.1 for pain clinic utilization and 2.2 ± 5.0 for PT utilization). In addition, Veterans in this group had a little more than 30 months of utilization across the timeframe (32.0 ± 15.3).
Demographic and clinical characteristics.
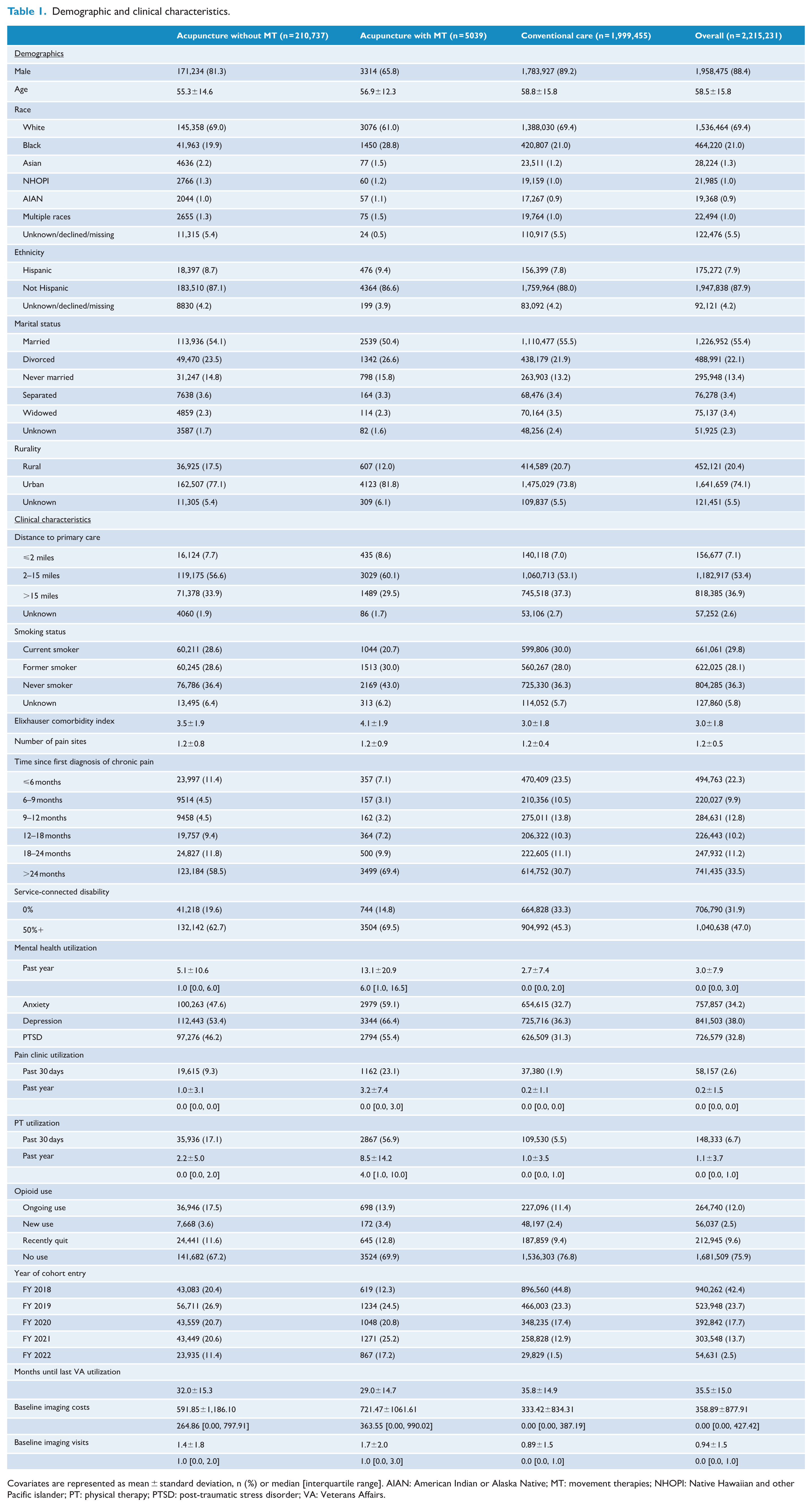
Covariates are represented as mean ± standard deviation, n (%) or median [interquartile range]. AIAN: American Indian or Alaska Native; MT: movement therapies; NHOPI: Native Hawaiian and other Pacific islander; PT: physical therapy; PTSD: post-traumatic stress disorder; VA: Veterans Affairs.
Given these differences, we matched each exposure group with a comparable conventional care control group, with Table 2 showing Veterans’ demographic and clinical characteristics after matching. A total of 210,153 Veterans in the acupuncture without movement therapies exposure group were matched to 1,045,084 Veterans in the conventional care control group to derive a comparison patient pool that was most similar to the acupuncture with movement therapy exposure group. Each of the characteristics had a SMD of <0.1, the accepted criterion of a quality match across covariates, except for months since last VA utilization. In addition, the overall distance score parameter between the matched samples was <0.001, demonstrating a very strong overall match (results not tabulated).
Baseline covariate balance after propensity score matching: acupuncture without MT.
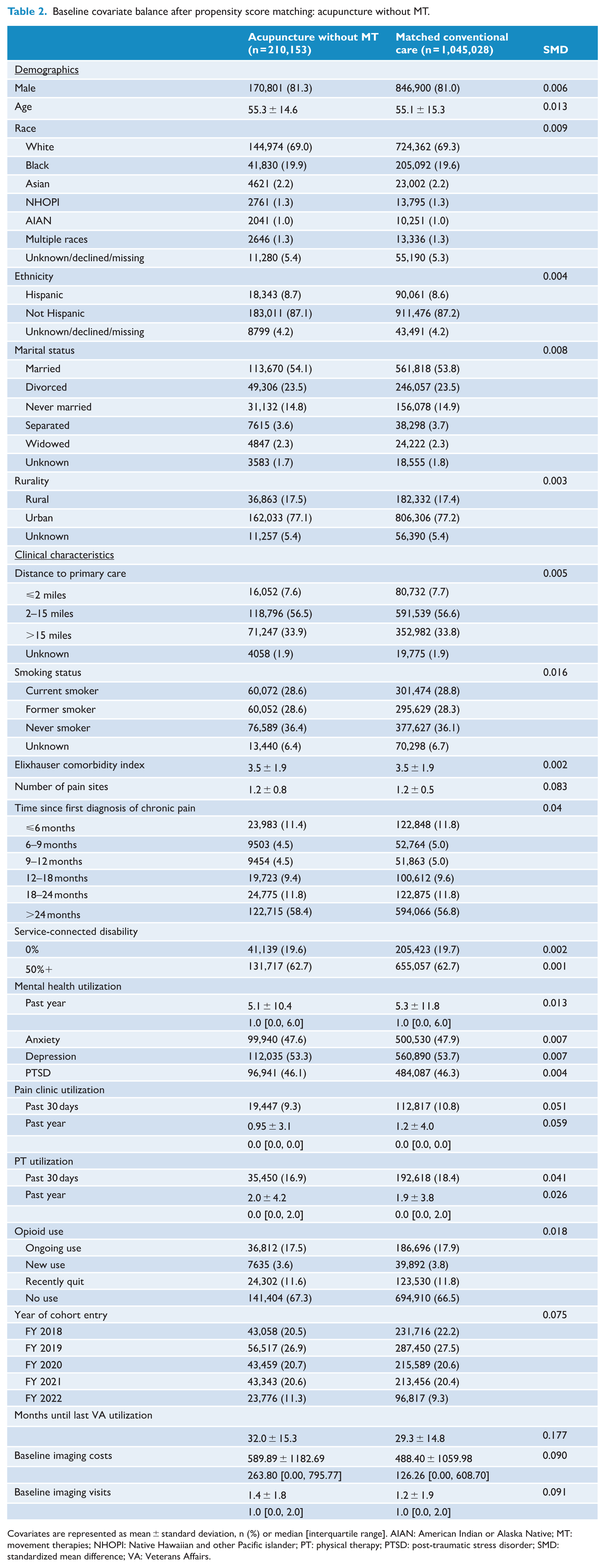
Covariates are represented as mean ± standard deviation, n (%) or median [interquartile range]. AIAN: American Indian or Alaska Native; MT: movement therapies; NHOPI: Native Hawaiian and other Pacific islander; PT: physical therapy; PTSD: post-traumatic stress disorder; SMD: standardized mean difference; VA: Veterans Affairs.
Table 3 shows the same characteristics for matched samples of acupuncture with movement therapies and their respective conventional care control group. Out of 5039 patients exposed to this treatment, 2415 were matched with a comparison group of 19,312 Veterans. Although the overall distance score parameter between the matched exposure and control groups was <0.05 (results not tabulated), two characteristics had SMD values of >0.1, namely year of entry into the cohort and opioid use.
Baseline covariate balance after propensity score matching: acupuncture with MT.
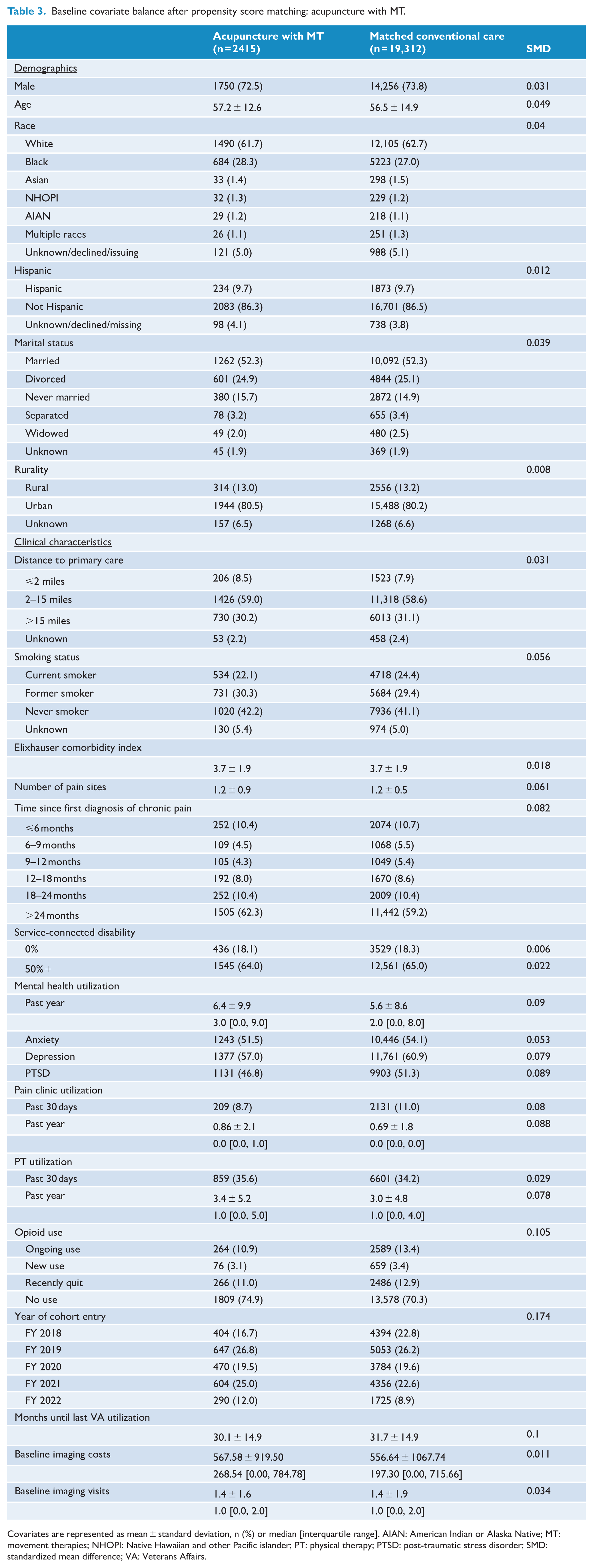
Covariates are represented as mean ± standard deviation, n (%) or median [interquartile range]. AIAN: American Indian or Alaska Native; MT: movement therapies; NHOPI: Native Hawaiian and other Pacific islander; PT: physical therapy; PTSD: post-traumatic stress disorder; SMD: standardized mean difference; VA: Veterans Affairs.
Tables 4 and 5 present total imaging costs and use before and after matching and compare the costs of the two exposure groups with their respective matched conventional care control groups. Before matching, total imaging costs were greatest among acupuncture with movement therapy patients, followed by the acupuncture without movement therapy group and the overall conventional care control group. However, as shown in Table 4, after matching, Veterans using acupuncture without movement therapies had imaging costs $155 greater than Veterans using conventional care, and Veterans using acupuncture with movement therapies had total imaging costs that were $140 greater. As shown in Table 5, Veterans using acupuncture without movement therapies had (on average) 0.34 more imaging visits than Veterans using conventional care, and Veterans using acupuncture with movement therapies had 0.37 more imaging visits, showing a similar treatment effect between the two exposure groups compared with their respective control groups.
Total imaging costs across 6-month period following indexing.
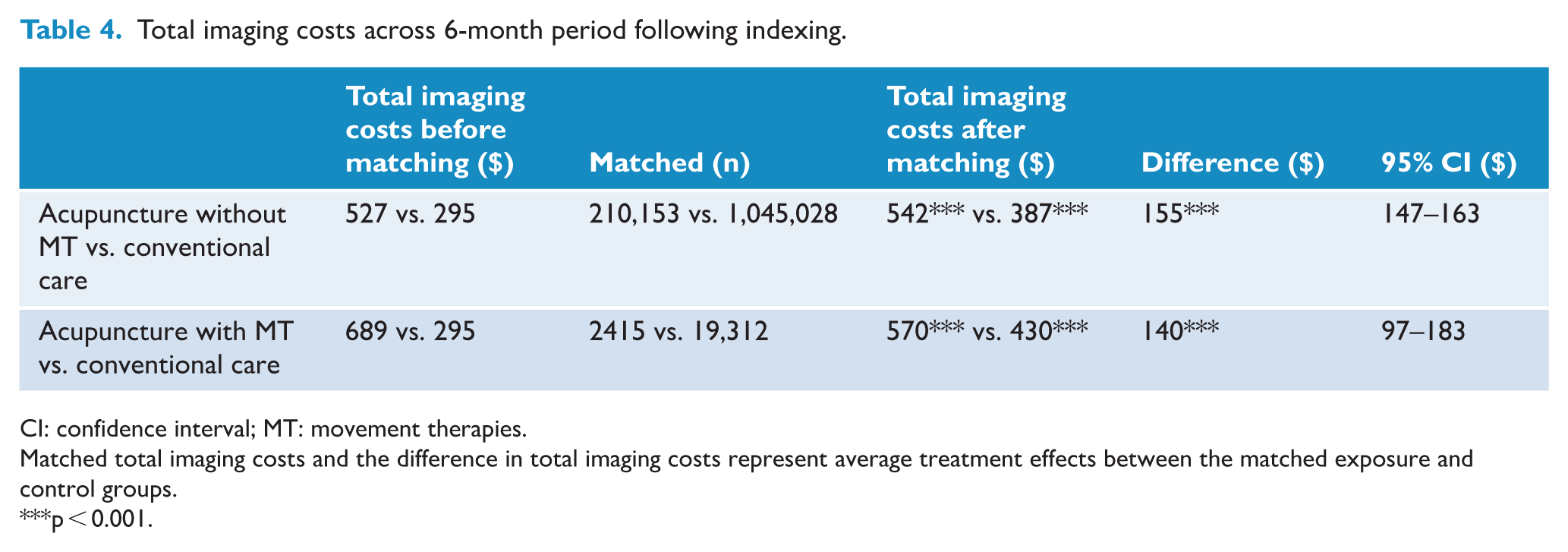
CI: confidence interval; MT: movement therapies.
Matched total imaging costs and the difference in total imaging costs represent average treatment effects between the matched exposure and control groups.
p < 0.001.
Total imaging visits across 6-month period following indexing.
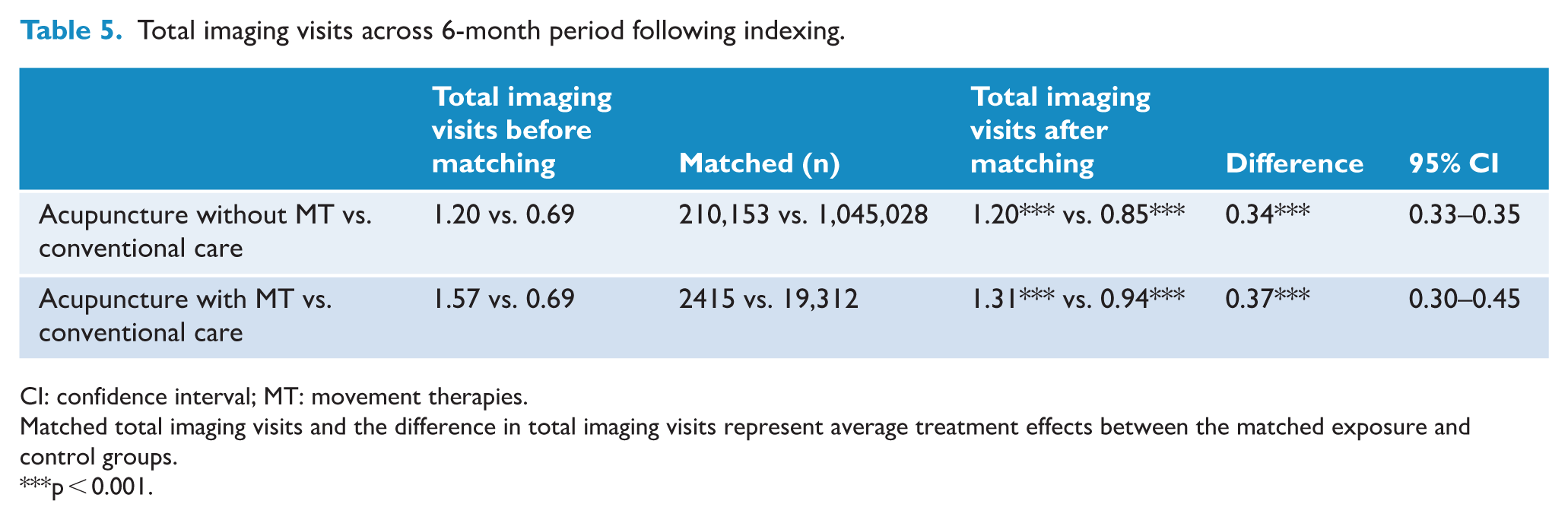
CI: confidence interval; MT: movement therapies.
Matched total imaging visits and the difference in total imaging visits represent average treatment effects between the matched exposure and control groups.
p < 0.001.
Baseline imaging costs and utilization sensitivity analyses
To test for confounding of the treatment effects, given baseline imaging costs, we incorporated the total imaging costs in the 6 months before index date as an additional covariate to be matched to each respective conventional care control group in four separate sensitivity analyses. Overall, the sensitivity analyses indicated a stable comparison between treatment and control groups when adding baseline imaging costs and utilization. After matching, this constituted a doubly adjusted estimation of imaging costs and use following regression for matched covariates in the treatment effect calculations, including well-matched baseline outcome measures. For both the acupuncture with and without movement therapies average treatment effects, the sensitivity analyses were more or less the same. Veterans using acupuncture without movement therapies had $128 greater costs ($526 compared to $398 in the conventional care group) and Veterans using acupuncture with movement therapies had $139 greater imaging costs ($565 compared to $419 in the conventional care group). Veterans using acupuncture without movement therapies had 0.32 more imaging visits (1.26 compared to 0.94 in the conventional care group) and Veterans using acupuncture with movement therapies had 0.42 more imaging visits (1.32 compared to 0.90 in the conventional care group). These sensitivity analyses are presented here as evidence of the robustness of the effects as reported in Tables 4 and 5, although adjustment for baseline imaging costs and visits may indicate some small degree of residual confounding on the part of acupuncture without movement therapies imaging costs and acupuncture with movement therapies imaging visits treatment effects analyses, marginally changing usage and costs, despite the unchanged direction and relative magnitude of each respective effect. Although baseline imaging costs and use were higher or relatively equal in both treatment groups, compared with their respective control groups in each sensitivity analysis, the SMDs measuring the quality of the baseline costs and use match were 0.09 and 0.091, respectively, for the acupuncture without movement therapies analysis, and 0.01 and 0.034, respectively, for the acupuncture with movement therapies robustness check, demonstrating that the former had slightly higher pre-intervention costs (and higher or commensurate pre-intervention use) than the latter, but that neither were different enough from conventional care to absolutely confound the post-intervention effect.
Discussion
In this study, we calculated total imaging cost and the average treatment effects of Veterans using acupuncture with or without CIH movement therapies using propensity score methods. We found that patients using acupuncture had higher imaging costs and utilization compared with a matched comparison group.
Although these findings contrast with a growing literature indicating the cost-effectiveness of CIH therapy use, particularly acupuncture, as an alternative to medical treatments for pain, a number of considerations may help to explain these findings. 10 First, although we made a concerted effort to match both exposure groups with suitable conventional care comparisons, the unadjusted baseline covariates portrayed two treatment groups with markedly different health profiles compared with conventional care patients, despite an attempt to account for these differences through matching. These drastically different baseline characteristics suggest residual confounding of comorbidity and healthcare utilization that characterizes these chronic musculoskeletal pain acupuncture patients as higher users of healthcare, due to greater pain and disability, as evidenced by their unmatched or unadjusted pain and therapy healthcare utilization, especially among acupuncture patients using other complementary components, such as yoga and Tai Chi. 9 Another possible explanation is that the use of acupuncture may be highly correlated or on the pathway to physical recovery and rehabilitation, for example in the aftermath of an injury or as a result of other unmeasured factors that may better explain imaging use beyond normal levels of healthcare utilization as observed among conventional care patients. 34 Third, as the VA continues to expand availability of CIH therapies across the United States, therapies such as acupuncture are still currently limited as nonmedical alternatives for pain management in many locations, which is an inherent drawback based on the organizational behavior and healthcare delivery of acupuncture in select geographies compared with the conventional care that is ubiquitous in the VA. 35
Furthermore, one of the main differences between the exposure group patients in this study and their respective control group patients is a pattern of utilization that may denote some level of enhanced self-advocacy or distress caused by measured and unmeasured comorbidity, leading to utilization beyond that observed among conventional care patients. Prior research points to medical complexity as an explanation for higher utilization but also overutilization driven by consumerism, patient experience, clinician beliefs, and healthcare cultures and systemic structures that promote or incentivize inordinate usage.36,37 Either of these considerations, in addition to usage resulting from physical recovery or geographical availability, may help to explain the observed baseline differences between the treatment and control groups, as well as the excess imaging usage seen in the treatment effects.
Perhaps most importantly, the literature contains numerous evaluations of acupuncture that, beyond a fairly unequivocal portrayal of its effectiveness for pain management, also indicate its cost-effectiveness, but with certain exceptions that seem to support our findings of higher post-intervention healthcare costs. At the VA, acupuncture is a tried-and-true method of managing chronic pain, headache and migraine, as demonstrated across dozens of evaluations, and it is of potential benefit for general pain and pain related to a number of specific health conditions. 38 However, there is limited evidence at the VA and elsewhere as to the cost-effectiveness of acupuncture as an alternative intervention for pain management compared with conventional care, and even sparser evidence related to its associated downstream health service utilization costs, as evaluated in this study. Some research shows a beneficial effect on health outcomes, but a null effect on the cost of acupuncture compared with allopathic care for certain conditions and ailments. 39 Some studies have shown an overall lower cost of acupuncture compared with conventional care, while some have shown higher comparative costs.40 –42 Evaluations of acupuncture as a cost-effective treatment for chronic pain that reduces other forms of healthcare use incurred after intervention are fairly limited and form a mixed collection of findings, some of which support the results of this study. One investigation showed a statistically insignificant decrease in total average hospital charges subsequent to acupuncture use. 27 Others have demonstrated reduced downstream opioid usage, fewer emergency department visits, more surgical treatments, and increased total costs and medication costs following acupuncture. 28 As has been noted intermittently in the literature, observational studies are prey to selection bias, in which a given healthcare population may be fundamentally different (sicker or more disadvantaged, for instance) from the population at large. This is a challenge that is difficult to disentangle both at the VA (with older, poorer and more comorbid patients) and in other safety-net healthcare systems conducting similar investigations.43,44 One interpretation of this study’s findings is that patients with chronic pain treated with acupuncture represent some of the sickest of VA beneficiaries, who get caught up in an inefficient diagnostic feedback loop, beginning with modest levels of imaging, referral to CIH therapies and subsequent specialty care utilization encounters, in an attempt to alleviate pain associated with unobserved and uncontrolled clinical characteristics.
For movement therapy interventions, the existing evidence is equally narrow and in contrast to this study’s findings. One study evaluating a resilience program including yoga, meditation and biofeedback reported fewer emergency department visits, and decreased imaging and total healthcare use during follow-up. 29 While our treatment effect analysis showed higher imaging costs and use following intervention, we evaluated such therapies in tandem with acupuncture, which formed a group of patients characterized by higher comorbidity and healthcare utilization compared with the acupuncture without movement therapies treatment and conventional care control groups. In other words, these users of acupuncture exemplify some of the neediest of patients, as shown not only by the group’s observed health and utilization profiles but also by self-selection into multiple CIH therapies as an intervention, for which finding a suitable comparison group is challenging and most likely influenced by uncontrolled confounding of other healthcare utilization measures.
Accounting carefully for the baseline adjustment of treatment effects in this study subsequent to matching, our sensitivity analyses (which include baseline imaging use) revealed potentially relevant but mainly incremental differences in follow-up costs and use. For patients using acupuncture alone, including baseline costs in the imaging costs treatment effect analysis led to a marginal decrease in follow-up imaging dollars, revealing potential cost confounding from relatively higher baseline spending among exposure group patients. This effect, paired with more or less equal post-intervention use in its accompanying imaging use sensitivity analysis, suggests that imaging before acupuncture referral may reduce more costly and unnecessary imaging after the fact, demonstrating minimal economic efficiency in imaging before and after. The acupuncture with movement therapies sensitivity analysis, including baseline use in the imaging use treatment effect analysis, points to slightly higher use after intervention, which – paired with similar follow-up costs in the companion imaging cost sensitivity analysis – may indicate healthcare efficiency related to the selection and delivery of imaging visits, although only narrowly.
While we strived to conduct a rigorous set of analyses, several limitations exist in this study. Although the overall matches in our two analyses were of high quality, a few individual covariates in both matching algorithms were of slightly less quality, including months until last VA utilization in the acupuncture without movement therapies analysis, and opioid use and year of entry into the cohort in the acupuncture with movement therapies analysis. In each iteration of the acupuncture without movement therapies matching analysis, coercing a quality match on the last utilization compromised the overall match strength of the analysis, with a particular effect on the other utilization variables. Consequently, we settled for an overall match of the highest quality while allowing for a slightly inferior match on last utilization. In the acupuncture with movement therapies matching analysis, due to extreme differences in exposure and comparison group characteristics, roughly half of the exposure group was discarded to address imbalance with respect to the control group, including the timing of entry into the cohort from 2018 to 2022, as the VA continued to expand acupuncture availability. Acupuncture with movement therapy patients entered the chronic musculoskeletal pain cohort in 2018 at the lowest rate and in 2022 at the highest rate by far, demonstrating the expansion of this care combination over the course of the 5-year study period. Executing a quality match on the timing of the provision of these therapies, in addition to all other covariates in the analysis, was a challenging task that resulted in a quality overall match but with certain compromises, such as this one. In addition, in terms of healthcare costs, the VA generally delivers lower-cost care compared with private sector providers, by a magnitude of 20% or greater, depending on the type of care. This suggests that the costs revealed in this study may be lower than those associated with imaging procedures provided outside of the VA; however, this study’s findings are presently neither comparable nor generalizable to the non-VA or general population. 45
Conclusions
Patients utilizing acupuncture with and without movement therapies at the VA had higher total imaging costs and a greater number of visits than conventional care patients before and after propensity score matching, suggesting patterns of comorbidity and utilization, and trajectories leading to acupuncture use unobserved in this study. In other words, patients using these therapies appear to be markedly more complex than conventional care control group patients in terms of contextual, social and clinical characteristics (such as chronic disease, disability and rehabilitation), prompting a slight increase in initial imaging encounters and costs for specialty care referrals such as CIH therapies, as well as subsequent imaging in the presence of persistent pain and medical complexity, potentially leading to an imaging loop of sorts. Furthermore, as the VA continues to expand access to acupuncture across the United States, differences in costs and utilization resulting from organizational or healthcare delivery disparities by geographical location may emerge as additional explanatory factors to be controlled for, as acupuncture and other CIH therapies are currently limited to a select number of flagship sites in the VA.
Because acupuncture and other CIH therapies are effective at pain management with minimal side effects and at lower cost, the VA should continue making them more widely available as an alternative to pain medication, injections and surgery.6,16 In augmenting national non-randomized observational studies on the cost-effectiveness of CIH therapies compared with conventional care, the VA should also investigate site, healthcare system and geographical characteristics (with respect to where CIH therapies are currently provided) to identify potential organizational cost and utilization confounders for future investigations.
Footnotes
Acknowledgements
This material is based upon work supported by the United States Department of Veterans Affairs, Veterans Health Administration, Office of Patient-Centered Care and Cultural Transformation. The views expressed in this presentation are those of the authors and do not necessarily reflect the position or policy of the US Department of Veterans Affairs or the US government.
Ethical considerations
This project was conducted as a quality improvement initiative at the US Department of Veterans Affairs.
Consent to participate
According to institutional guidelines, quality improvement activities that do not involve research aimed at generalizable knowledge are not classified as human subjects research. Therefore, IRB and informed consent were not required.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the United States Department of Veterans Affairs, Veterans Health Administration, Office of Patient-Centered Care and Cultural Transformation and Quality Enhancement Research Initiative (grant no. PEC 16-354). Stephanie L. Taylor was supported by a Veterans Health Administration Health Services Research and Development (HSR&D) Research Career Scientist Award (grant no. RCS 23-082).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.