
Abstract
Background:
Little is known about case managers’ ethical issues and professional values.
Objectives:
This article presents an overview of ethical issues in case managers’ current practice. Findings are examined in the light of nursing ethics, social work ethics and principle-based biomedical ethics.
Research design:
A systematic literature review was performed to identify and analyse empirical studies concerning ethical issues in case management programmes. It was completed by systematic content analysis of case managers’ national codes of ethics.
Findings:
Only nine empirical studies were identified, eight of them from North America. The main dilemmas were how to balance system goals against the client’s interest and client protection against autonomy. Professional codes of ethics shared important similarities, but offered different responses to these two dilemmas.
Discussion:
We discuss the respective roles of professional and organizational ethics. Further lines of research are suggested.
Keywords
Introduction
Case management can be defined as a ‘targeted, community-based and pro-active approach to care that involves case-finding, assessment, care planning, and care co-ordination’. 1 It appears in the United States in the 1970s. First introduced in social work in the United States in the 1970s, it then developed in healthcare, in part because of the need for cost containment. 2 Role functions of case managers include conducting a comprehensive assessment, establishing a care plan, coordinating the members of the healthcare team and educating and empowering the client. 3 The precise missions of a case manager may vary according to his or her employer (hospital or long-term care agency, private insurance, etc) and his or her professional background. They may include a gatekeeping role. So case managers have to make ethically challenging decisions concerning, for example, clients’ right to live at risk, resource allocation or balance between clients’ and caregivers’ interests. 4 Given the ageing population and the growing focus on care coordination, case management is now well established in North America and is developing fast in Europe, 1,2,5 Asia, 6,7 Africa 8 and South America. 9 However, the identity of the case manager is still under construction, 10 challenged by a recurrent question: Is case management just a professional practice or a new profession? The Case Management Society of America (CMSA) 3 clearly replies that it is a professional practice that could be exercised after a graduate degree in health or social work, whereas the Case Management Society of the United Kingdom (CMSUK) 11 introduces its code of ethics by naming case management ‘a young profession’. In this debate, the question of professional ethics is important, as it is a primary component of a professional identity: Davis 12 considers that the attempt to set special standards, including education, skills and ethical conduct, characterizes a ‘would-be’ profession. But case managers are often already part of an established profession, usually nurses or social workers. Those two professions have strong values, embodied in updated codes of ethics (see for the American context 13,14 ). So is there really a need for a new ethical approach, shaped specifically for case managers?
The aim of this article is to present a comprehensive overview of case management professional ethics, based on empirical studies of case management ethical issues and values, and on the professional values of case managers as stated in codes of ethics. We systematically reviewed the literature on studies of case managers’ ethical issues and values, and analysed case management national codes of ethics. To clarify the content analysis of the retrieved studies, we first present ethical concepts commonly used in case management ethics.
Origins of case management ethics
Principle-based ethics, especially the approach advocated by Beauchamp and Childress, 15 is often used in the case management literature. 16,17 However, this approach shouldn’t overshadow the rich traditions of social work and nursing science’s ethical thinking. Both have inspired case management ethics. We are unable here to present all possible ethical approaches used by nurses or social workers. Instead, we will just present some values and theories useful for the comprehension of the following review.
Principles of biomedical ethics
Among principle-based theories, 18 the pluralist principlist approach, as described by Beauchamp and Childress, has achieved great popularity, especially in North America, as it can be used by all healthcare professionals and is applicable to large range of situations. The authors defined in 1979 four principles as an analytical framework that expresses the general values underlying rules in common morality. These four principles are respect for autonomy, beneficence, non-maleficence and justice. Prima facie they are of equal importance. They can, however, conflict with each other and hence have to be balanced against each other according to the context. 15 Although reference to such principlism does not generate uncontroversial solutions, it does provide a framework for moral deliberation and decision-making. Unlike the following approaches, so-called ‘principlism’ has not been developed by practitioners but by ‘experts’. Despite numerous criticisms, 19,20 this approach is nowadays widely used in medical and healthcare ethics.
Social work ethics
Social work ethics has been developed over the last 100 years, mainly by professionals, based on their daily practice. Despite a long-lasting quest for unity, 21 it has never been unified in a single theoretical framework. Theories have succeeded each other and have sometimes been at odds. Important values that deeply shaped first social work practice and then case management practice can, however, be identified. 22
As stressed in the preamble of the United States National Association of Social Worker (NASW)
23
standards for social work case management: Case management […] has its origins in the earliest history of social work practice and the social work profession. Social work case management is clearly linked to social case work […]. It is based on the recognition that a trusting and empowering direct relationship between the social worker and the client is essential.
Another important concept arising from social work is empowerment. According to the preamble of the NASW Code of Ethics, empowerment of vulnerable people is one of the primary goals of social workers. The ‘empowerment approach’ appeared in social work in the 1960s. It first involved community-oriented work, seeking the liberation of oppressed groups. 26,27 It was seen as a process of gaining power, mainly led by the group, with the help of social workers. It implied a commitment to social justice and a struggle against discrimination. This concept clearly evolved when it was ‘enthusiastically accepted’ by nurses in the 1990s. 28 It shifted to a helping process in which nurses ‘give power’ to patients by mutual decision-making. Nurses use their own power, based on their knowledge and skills, to maximize the patient’s independence. This second definition, oriented towards individual progress, seems to us closer to the case manager’s understanding of the concept.
Finally, a classic dilemma for social workers is the balance between clients and system interests, and between individual and community interests. 14 The social worker’s role especially may include legal obligations to report certain facts. Thus, their primary commitment is clearly, in the NASW code, 14 to the client. So this commitment may conflict with their legal obligation, for example, if a client asks them not to report that he has been abused. Their intervention ‘occurs at both the client and the system level’, the system level intervention aiming at advocating the client’s rights. Social workers may have to struggle for adequate resources and fair allocation procedures, for example. Case managers have to serve both the client and the system, as ‘improving quality of care and maintaining cost effectiveness’ 3 is one of their functions. In case management literature, this dilemma is conventionally described as the difficulty of serving two masters. 29
Nursing ethics
As ‘caring professions’, social work and nursing share common values. 30 The American Nurses Association 13 Codes of Ethics seems close to that of the NASW. It includes respect for the uniqueness of the person and sensitivity to his or her environment, as well as a commitment to social justice. The word ‘empowerment’ is not used directly, but it is stated that ‘Nursing care aims to maximize the values that the patient has treasured’. The main difference with social worker ethics lies in the use of the term ‘patient’, which primarily refers to ‘one who suffers’, instead of ‘client’. A stress is placed on compassion, with patients as well as colleagues or students. Emotions and relationships are central in ‘care ethics’, which we will now define in order to see whether it can be relevant for case managers.
Care ethics has been constructed in opposition to principlism, as a concrete feminine approach opposed to an abstract masculine one. Principle ethics has been criticized by nurses because it emphasizes abstract reflection instead of contextual sensitivity and emotion: In an ethics of care, moral reasoning and behaviour involves empathy, compassion, and connectedness; consideration of abstract ethical principles is secondary concern. Contextual factors and interpersonal relationships are key elements to understanding and resolving ethical dilemmas that occur in practice.
31
However, one form of caring 33 has been fully adopted by case managers, with the concept of advocacy. 34 Advocacy in the nursing literature reflects diverse usages, from ‘paternalistic advocacy’ to ‘consumer advocacy’ and ‘existential advocacy’. 27 Whereas ‘paternalistic advocacy’ places the nurse in the position to make an expert judgement and to defend it, ‘consumer advocacy’ emphasizes patients’ information and defence of their right to services. ‘Existential advocacy’ is somehow different, as it can be defined as ‘the effort to help patients become clear about what they want in a situation, to assist them in discerning and clarifying their values and examining available options in light of those values’. 35 So it involves the development of the nurse–patient relationship as the medium for expression of the patient’s values. 33
Methods
As case management is somehow different from both nursing and social work, it seemed to us necessary to compare these concepts and theories with case managers’ actual discourse. This comparison, through studies of empirical ethics, can lead to theoretical enhancement as well as critical assessment of current practices. 36 That is why we performed a systematic literature review 37 of studies on case management ethics. In addition to these empirical data, we analysed case management national codes of ethics. These codes, written by professional organizations, formalize case management values as case manager leaders understand them.
We searched the literature in March 2015 in the Scopus database, by combining the words ‘case management’ and ‘ethics’ in the title, abstract or keywords. Scopus was chosen for its large coverage (18,500 peer-reviewed journals indexed), especially for human science and non-English journals (http://www.info.sciverse.com/scopus/scopus-in-detail/facts). Title and abstract were read to identify articles related to case management ethics. We then identified in these articles those based on empirical research, and excluded articles solely based on experts’ opinions of this systematic analyse. Full-text articles were retrieved when necessary, to check their relevance. As there is no consensual method to check the internal validity of such studies, 38 we considered all studies based on qualitative data, as long as the data collection methods were clearly reported. We added to the retrieved articles our own study, 4 which was published online but not yet indexed in Scopus in December 2012. Selected studies were analysed to identify the context of case manager practice (year, place, care setting), the underlying theoretical framework as stated by the authors and the methods used; and to summarize the main results.
We then conducted a systematic Internet search using Google® to identify national codes of ethics addressed to case managers available online and written in English. The search algorithm combined ‘code of ethics’ and ‘case manager’ with the name of the 20 country members of the G20 group. All documents dealing with values or principles were retained, whatever their name. We did not consider codes addressed only to a certain category of case managers, such as nurse case managers or social worker case managers, as those codes do not allow us to identify values specifically linked with case management. A comprehensive comparative thematic analysis 38 was then performed to seek the four principles of biomedical ethics, the primacy of the client’s interest, the case manager’s attitude towards regulations, the concepts of advocacy and empowerment and respect for privacy.
Results
Review of published literature on empirical ethics
Our bibliographic search retrieved 252 references. After reading the titles and abstracts, it appeared that 61 articles directly concerned ethical questions linked to case management. They were published between 1988 and 2013 in case management professional reviews, or in journals of nursing science, public health or social science. In all, 51 articles were expert opinions, and the 10 others were retrieved for further analysis. One was excluded after full-text reading 29 because of a clearly insufficient internal validity: it was based on case reports without any methodological description. We analysed the nine other articles, eight from North America, in addition to our own study, from France. Notably, we retrieved no quantitative study. The results are summarized in Table 1. In these nine articles, the analysis is based on principles of biomedical ethics in two, 4 three mainly focus on the classic social work dilemma of the case manager’s role in the system, 39,40,43 two are based on nursing ethics concepts and theories (advocacy 34 or relational ethics 32 ) and the last two do not discuss any theoretical framework.
Approach, methods, setting and results of empirical ethics studies.
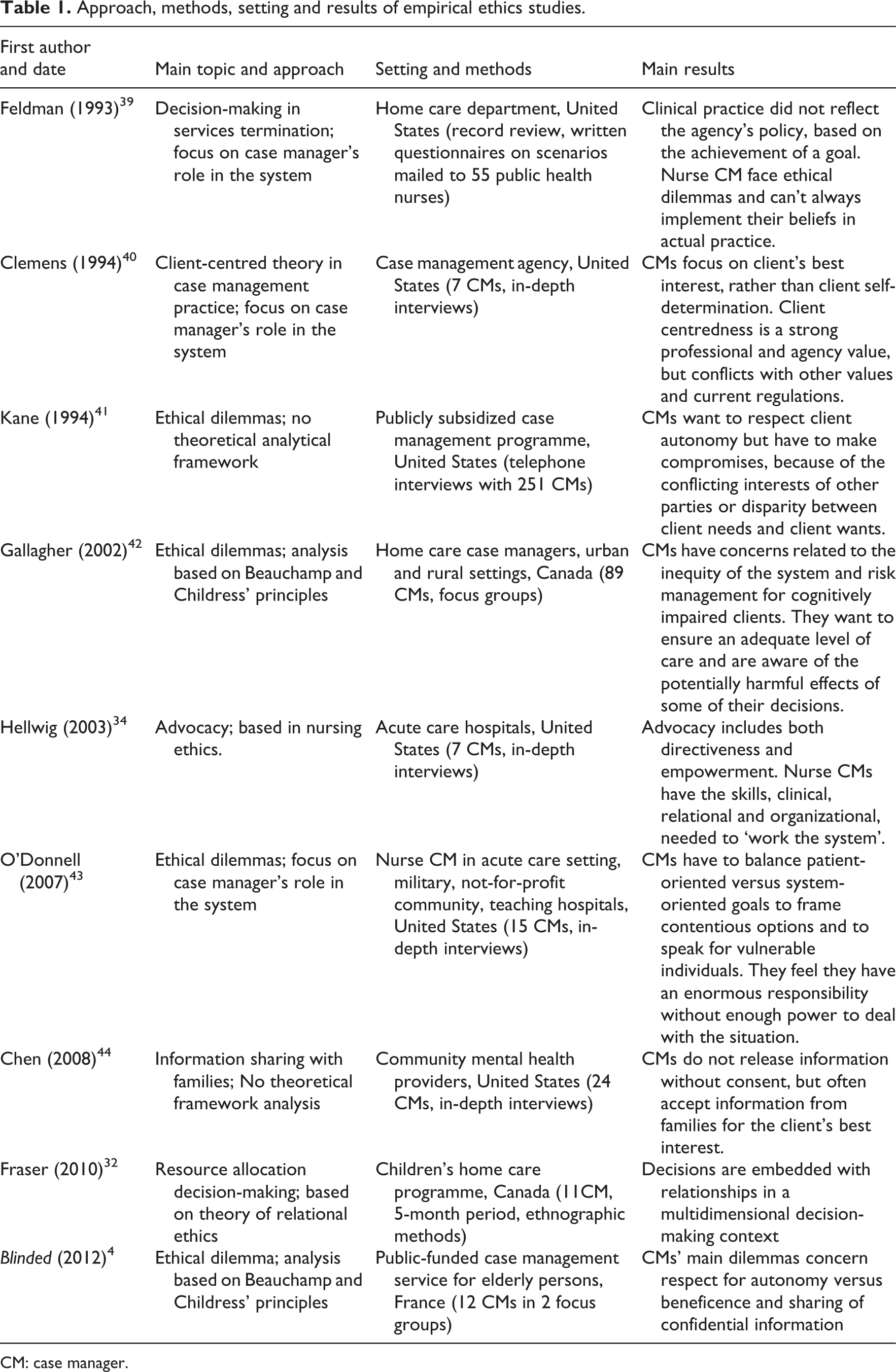
CM: case manager.
The four articles focussed on identifying ethical dilemmas all stress their frequency and diversity. The two articles focussed on ethical decision-making both stress the complexity of that process and the importance of relationships.
Three main dilemmas appear in case managers’ discourse. The first dilemma, considered in seven studies, concerns balancing client-centred goals versus system-centred goals, especially cost-containment. Five studies present this balancing task as burdensome. They estimate that case managers’ lack of power 40,43 jeopardizes their ability to protect clients’ best interests and can lead to frustration for case managers who cannot implement their own values in actual care. 39,40 Conversely, two studies conclude that case managers have enough skills and power to make adequate resource allocation decisions 32 and to advocate efficiently 34 for the client. These two studies are the only ones based on the nursing ethics concepts of advocacy and relational ethics.
The second dilemma, identified in four studies, 4,37,41,44 concerns balancing client respect for autonomy versus beneficence, especially for persons living at risk and/or mentally ill. It appears that case managers often have to make an ‘uneasy compromise’ with the principle of respect for autonomy, in order to protect their clients. The third and last dilemma, considered in only three studies, 4,41,44 concerns maintaining confidentiality when dealing with families and stakeholders. It appears that case managers do not always strictly respect the client’s decision regarding confidentiality. None of these articles states that case managers directly refer to a professional code.
Professional codes analysis
Our online search identified five relevant documents. Two are addressed to American case managers (the Standards of Practice of the CMSA, 3 and the Code of Professional Conduct for Certified Case Managers 45 ), one is addressed to Canadian case managers (the Standards of Practice of the National Case Management Network of Canada 46 ) and one is addressed to United Kingdom case managers (we analysed together the Code of Ethics 11 and Standards of Practices for case managers, both published by the CMSUK). We also analysed ethical principles published by the Case Management Society of Australia. 47 Standards of practices published by this society were not considered, as no online access was available. No ethical guidelines were found on the website of the Case Manager Association of South Africa.
Our comparative thematic analysis found important convergence in these documents: all define case management functions quite the same way, as a ‘collaborative process’ that includes assessment, planning, facilitation, care coordination and evaluation to meet the individual’s comprehensive health needs. All emphasize an individualized client-centred approach and stress respect of the client’s autonomy. Discrimination is condemned and cultural sensitivity promoted. Despite these important similarities, some differences are apparent.
The CMSA, Canadian, British and Australian codes consider that the primary obligation of case managers is to their clients. Yet, we can see some shades: whereas the CMSUK code states that ‘decisions should be made irrespective of how the service is resourced’, the CMSA Standards of Practice refuse to oppose the individual’s interest against the payer’s interest, arguing that ‘when an individual reaches the optimum level of wellness and functional capability, everyone benefits’. The Commission for Case Manager Certification (CCMC) code has a somewhat different approach, since the first principle focus is on public interest, which certified case managers have to place above their own. The client’s rights only appear in the second principle.
Another difference concerns the attitude the case managers should adopt towards laws, regulations and local policies. For the CCMC code, case managers just have to respect them. For the four other codes, case managers also have to identify gaps in those regulations and to report them to the authorities, to enhance the fairness of the system. The CMSA code even argues for a more critical attitude, recognizing that ‘regulations are sometimes in conflict with ethical principles’.
Respect for privacy is present in all codes, but only the CMSUK code really considers it as a value, under the outline ‘respect’. In other documents, it appears mainly as a legal requirement.
For the guiding principles, the two US codes explicitly refer to the four principles of Beauchamp and Childress, CMSA adding fidelity as a fifth one. The UK standards of practice first stress the therapeutic relationship, described in terms of power, trust, respect and empathy. The concept of advocacy has an explicit and important place in the two US codes and in the Australian code. Its usage refers mainly to ‘consumer advocacy’ in the CMSA and Canadian standards of practice, whereas it also seems to include a more paternalistic and relational approach in the CCMC code. The empowerment concept is explicit in the two US codes and implicit but clearly present in the United Kingdom and Canadian codes. The UK code refers to ‘an active duty to respect client autonomy, including their right to live with risk’. The Canadian code states a ‘right to self-determination’, and a duty to explore the ‘client’s needs, concerns, values and choices’. The Australian code is far more ambiguous on that subject, by assuming ‘the right to live at risk so long as there is no harm’, in other words as long as there is no ‘real’ risk. It adds that case managers should consider the ‘best interest of the client as paramount at all times’.
Altogether, we can conclude that despite strong common ethical values, there are variations between the codes, especially concerning the case manager’s stance towards regulations, the balance between client and system interests and the attitude towards clients living at risk. The CCMC code is the more legalistic, whereas the British one is virtue-based, and more critical.
Discussion
Strengths and limitations
The identification and selection of articles are important challenges in a systematic review of empirical ethics. 37 ‘Ethics’ as well as ‘case management’ are broad concepts and can have different meanings. In order to seek coherence, we limited this review to articles that explicitly address ethical questions in case management. That is why we chose a simple search algorithm, selecting only articles directly focussed on our subject. By so doing, we did not consider articles focussed on decision-making or on organizational processes without explicit ethical discussion, or articles on global ethical evaluation of healthcare systems. We may have missed ethical discussions based on specific case management systems, as a large range of terms can be used to describe quite similar interventions. But we believe that our approach helped us to select a coherent range of articles, allowing a comparative analysis.
Another controversial question in empirical study analysis is quality assessment. 38 We chose to consider all studies based on empirical data with a clear report of data collection, whatever the methodology. Because of the scarcity of the studies, we believe it was important to take all of them into account. It seemed to us important to consider the underlying theoretical framework with the results, as it could have influenced them. This framework was not clearly stated in all studies, and different levels of abstraction were observed, from decision-making theory to professional values, which can appear confusing. However, the fact that the two articles based on nursing ethics were the only ones to conclude that case managers are able to serve the interest of the client within the constraints of the system, whereas other articles were more sceptical, seems to us a valuable result. It may indicate that nursing ethics theories are not critical enough to evaluate the system, even if they can be very useful in helping case managers to make decisions. 32
A monocentric qualitative study can only draw conclusions about its own setting. Yet, since we haven’t identified important differences according to the different settings, their conclusion may be used in similar context. In other terms, some external validity (or ‘transferability’) may arise from the addition of all the studies. 38 However, as eight out of nine studies were done in North America, the conclusions of this review should not be applied without caution to other cultural contexts or healthcare organizations.
Concerning our analysis of case management codes of ethics, we cannot claim exhaustiveness because we limited our search to the English language and because of the limitations of search engines such as Google. But it seemed to us relevant to explore case managers’ values as defined by professional organizations. Whereas qualitative studies are based on individual discourse, such codes reflect how case managers define themselves as a professional group. Writing such codes, they assert their identity and state the way they want to act, which can be different from the way they do act. Our analysis demonstrates high homogeneity between these codes. However, identified differences can enhance reflection, especially as these differences match case managers’ actual dilemmas.
Study results versus expert opinion
According to our literature review, the main case managers’ dilemma is to fulfil both a client-centred role and a system-centred role, in other words to serve two masters. 29 Our analysis of codes also shows how this point is debated. Interestingly, our results differ from the opinion mainly expressed by ‘experts’. Experts, at least those writing in professional case management journals, often argue that these two roles are coherent, as both improve public interest by implementing an efficient care plan. 48 –50 They mainly base their recommendations on Beauchamp and Childress’ principles, 16,17,29,51,52 sometimes adding other principles such as fidelity 51 and veracity. 51,52 They usually do not refer to nursing or social work ethical traditions. An important exception here is Padgett, 53 who argues, on the basis of feminist and critical theory perspectives, that nurse case managers may not have enough power to face a ‘capitalist and sexist’ system. If case managers don’t have enough power, working as agents of a broader system, to make their own choices, so Padgett claims, then this system, and not individual case managers, should in fact be accountable for an ethical practice of case management.
Organizational ethics versus relational ethics
Our results show that professional ethical guidelines as well as research studies are based on the idea that case managers are professionals, who can make autonomous choices and assume their own responsibilities. The three ethical approaches presented above as roots of case management ethics focus on the individual as a moral agent. However, this approach, which is usual in bioethics, can be questioned concerning case management. Wolff 54 prefers a systemic, organizational approach, as it doesn’t ‘base an ethics for case management on a requirement of heroism’. She argues that the need for an advocate for the client should be recognized by the organization, so the case manager should be asked to play this role, and only this one, without any gatekeeping mission. Thus, case managers could act according to their agency rules, without having to resist their employer because of their own standards of care.
Wolff is not the only one to stress the importance of organizational ethics for case managers, and Cesta
55
wrote about ‘case management ethics, also known as organizational ethics’. Organizational ethics can be defined as the organization’s efforts to define its core values and mission, identify areas in which important values come into conflict, seek the best possible resolution of these conflicts, and manage its own performance to ensure that it acts in accord with espoused values.
56
although many healthcare professional codes of ethics have been updated or revised reflecting the increasing awareness of ethical issues in healthcare, professionals say they are practicing in situations with a lack of congruency between individual patients’ needs and the demands of the organization.
57
But is organizational ethics enough? While an organization should ensure that its procedures respect clients’ rights, only professionals can give clients more than just rights, compassion for example. Hugman 30 notes that ‘risk management make particular sense in the neo-liberal commodification of the work of the caring professions as a product to be consumed’, but ‘does not easily accommodate the idea of discretion contested moral norms or a plurality of value’ (p. 151).
Organizational ethics can provide rules or standards to guide professionals, but can’t deal with the complexity of each real situation in a pluralist world. Attention to the context, stress on relationships, emotional engagement, those concepts that Hugman 30 calls ‘new approaches in ethics’, although they have deep roots in nursing and social work ethics, are necessary to discern not only ‘what to do’ in difficult situations but also ‘how to do’. When case managers face an ethical dilemma opposing two important principles, beneficence and respect for autonomy, for example, their question may not be ‘Which of these principles is the most important?’ but ‘How can I keep these two principles in dealing with that situation?’ So they won’t consider balancing or specifying principles, but try to find a concrete way to deal with a difficult situation. Their answer will depend on codes and regulations, but also on their own professional and personal values, on the client’s values and on their relationship with the client.
To understand this process, Fraser et al. 32 stresses the relevance of Gadow’s relational ethics theory for case managers. This approach is based on care ethics and enhances her definition of ‘existential advocacy’. Gadow 61 describes three layers in ethical approaches. The first one, ‘subjective immersion’, matches communitarian ethics. In a society where everybody agrees on what is good and what is wrong, intuition is enough to guide professionals. The second one, ‘objective detachment’, corresponds to rational ethics, replacing tradition with universal principles, and matches principlism. Gadow calls the last layer ‘relational narrative’. It includes intersubjective engagement: ‘At times of vulnerability, personal narratives can fail, just as ethical certainties can fail in face of radical contingency. In those moments, a new narrative is needed, and help may be needed to compose it’. Case managers may therefore have to engage in relationships in order to help clients to construct new narratives, and to make meaningful choices. ‘The move from universalism to engagement is the turn from rational to relational ethics, replacing detached reason with engagement between particular selves’. Relational narrative corresponds to our post-modern world, where no certainty can be achieved, but a form of shelter can be ‘constructed by the patient and the nurse as a way of making their situation inhabitable’. According to Gadow, these three layers co-exist in professional practice, according to the situation, each based on the others, like a coral reef.
As our systematic review of empirical ethics studies stresses the complexity of the decisions case managers have to make and the importance of individualized decisions based on relationships, Gadow’s theory seems to us relevant to case management ethics. This theory doesn’t contrast abstract thinking based on principles with a contextual, emotionally engaged decision process. It stresses that if principles are necessary, they sometimes lead to impossible choices. In these situations where no acceptable solution appears, intersubjective engagement may be a way to make a choice meaningful both for the client and the case manager. Thus, whereas organizational ethics, with its rules based on principles, is necessary to manage the ethical risk of case management, it does not replace the case manager’s ethical reflection and personal engagement in relationships. This relational approach may provide case managers with motivation to act ethically and to participate in the construction of their professional identity.
Lines of future research
Our systematic review has revealed two main gaps in research on case management ethics. First, all empirical studies but one have been conducted in North America. As the cultural and organizational context may differ in other continents, further research in other countries would enhance understanding of case management ethics. Second, no comparative study has examined the professional background of case managers, or the organizational context in which they work. So no conclusion can be drawn regarding the potential specificity of case management ethics, compared with social work or nursing ethics. Third, all studies focus on individual, professional approaches, with little consideration for interactions between professionals and organizational ethics.
Conclusion
The published data have identified case managers’ main dilemmas, but so far are insufficient to define a specific professional ethic for case managers. It seems to us more interesting to consider the specific ethical dilemmas they face in the broader context of ‘caring profession ethics’, 30 which includes both nursing and social work ethical traditions. Organizational and professional ethics have to be dovetailed in order to provide a coherent framework that takes into account both institutional risk management and case managers’ personal and professional values. Standardized processes should leave room for relational engagement and individualized care.
Footnotes
Acknowledgement
The authors thank Dr Minou Friele for her useful comments on the manuscript that helped them to make significant improvement, and Pr Armelle Gentric for her help in final revisions.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This work has been partially supported by a doctoral grant from the Fondation Mederic Alzheimer.