
Abstract
Background
As Korean neonatal nurses frequently experience the deaths of infants, moral distress occurs when they provide end-of-life care to the infants and their families. Although they need to care for the patients’ deaths and consequently experience burnout and turnover due to moral distress from the situation, there is a lack of a support for nurses. Moreover, not much information is available on the moral distress of neonatal nurses. There is a need to better understand Korean neonatal nurses’ moral distress to develop and implement appropriate supports.
Objective
This study aimed to describe nurses’ experience of moral distress when they provide end-of-life care to infants and their families in neonatal intensive care units.
Research design
This is a secondary analysis qualitative study. Content analysis was performed based on Corley’s theory of moral distress to develop a codebook and identify themes regarding moral distress among the nurses.
Participants and research context
Qualitative data were collected from 20 nurses working in two NICUs in Seoul, South Korea.
Ethical considerations
The original study obtained permission from a university’s institutional review board (IRB). This secondary analysis study obtained the exemption from another university’s IRB. Nurses’ participation was voluntary and confidential.
Findings
The nurses’ moral distress was derived when they faced moral constraints and/or moral conflicts. Two distinct categories of moral constraints and four distinct categories of moral conflicts were identified among the neonatal nurses. In addition, impacts of moral distress on patients and nurses were identified.
Conclusions
This study identified occasions neonatal nurses experience moral distress, and thus can guide in developing and implementing effective interventions to decrease their moral distress and improve their resilience in end-of-life care by providing insight into neonatal nurses’ needs for support in end-of-life care.
Introduction
Moral distress is a psychological response to morally challenging situations. 1 Nurses experience moral distress when they feel constraints in terms of decision-making, either when there is an action they want to take or when they feel uncertain about which action to take. 1 While moral constraint occurs due to external, uncontrollable factors,2,3 moral conflict occurs in the presence of conflicting moral values when there is more than one moral factor related to any particular principle or duty at play. 1
Nurses’ moral distress has been a huge global issue for over three decades.4,5 Previous studies have revealed the potential consequences of moral distress among nurses, including high levels of emotional exhaustion, emotional resignation, burnout, and turnover.6–12 In addition, such negative consequences on nurses lead to poor quality of care. 13 As moral distress negatively impacts nurses themselves, patients, and healthcare organizations, 7 the interventions to encourage and support nurses to decrease their moral distress are crucial.
Previous studies revealed that nurses frequently confront morally challenging situations surrounding end-of-life care issues: (a) being unable to reflect their expertise on decision making of the patients’ care due to low recognition of nurses’ authority over the care; (b) witnessing patients’ pain and suffering because family or physician wished the provision of the care that nurse thinks futile; and (c) having an unsupportive healthcare system such as inadequate staffing and resources, and limited policies.14,15 Neonatal intensive care unit (NICU) nurses experience such situations frequently because about half of the pediatric deaths involve infants. 16 In addition, most infant deaths occur in hospitals, especially in the NICU, because it is risky to move an infant in critical condition to a hospice unit or home setting. 17 Nurses who have experienced numerous losses of infant patients can suffer from chronic grief and death anxiety, resulting in barriers to providing compassionate care to patients and their families. 11 A better understanding of NICU nurses’ experience surrounding end-of-life issues is essential to prevent such negative consequences.
In Korea, because hospice care for children is in its early stages, 18 NICU nurses provide end-of-life care for dying infants and their families being untrained, resulting in a work environment where stress related to end-of-life care can arise at any time. Although NICU nurses’ experiences related to end-of-life care have been explored recently, only a few studies have focused on their moral distress or stress related to such care in Korea.19–21 Especially, there are limited studies based on a concrete theoretical basis. In addition, to our knowledge, there is no instrument that measures nurses’ moral distress related to end-of-life care or palliative care despite the care circumstances various ethical issues can arise. Therefore, Korean NICU nurses’ moral distress related to caring for dying infant patients and their families should be thoroughly explored to be adequately examined, resolve the moral distress issue, prevent proven negative consequences, and provide quality end-of-life care in NICU. This study specifically aimed to explore Korean NICU nurses’ experience of moral distress related to end-of-life care and its impacts, guided by Coley’s theory and Fourie’s definition of moral distress.1,7
Methods
Study design, data, and sample
This qualitative descriptive study described Korean NICU nurses’ experience of moral distress when providing end-of-life care to patients and their families. As a secondary analysis of a qualitative study, the previously collected dataset derived from the original study was analyzed. 22 The data contained interviews of 20 NICU nurses at two tertiary hospitals in Seoul, South Korea.
Theoretical framework
The Corley’s model for a theory of moral distress 7 was used to categorize coding and address themes surrounding moral distress among Korean NICU nurses. The theory outlines various concepts and their relationships surrounding nurses’ experience of moral distress—the internal/external contexts, the precedent and consequent moral concepts, and moral comfort. 7 To analyze the qualitative data in this study, the concepts in the theory were utilized as origins of codes of a directed content analysis. 23 In addition, the propositions of the theory guided to develop this study’s conceptual framework that shows the relationships of the extracted themes. The current definition of moral distress 1 was used in this study to reflect the NICU nurses’ experience of moral distress that occurs not only when they do know but also when they do not know what is right in a moral situation. Fourie’s definitions and Corley’s model allowed us to develop our own codebook to analyze the interview data.2,7
Data analysis
Based on the research questions, quotations that contain any expressions of nurses’ emotional distress were selected from the transcribed verbatim. And then, content analyses were carried out to understand Korean NICU nurses’ experiences of moral distress when they provided end-of-life care to infant patients and their families. 23 Two bilingual coders (SH and SK) who independently analyzed all transcripts written in Korean and had both in-person meetings and email or phone communications to compare and match each other’s codes and establish a codebook by following the codebook development process described in study. 24 A full consensus on finalizing the codebook, including themes, definitions, and quotes, was arrived at after continuous discussions. After the consensus given by the two coders, one bilingual peer-reviewer (HM) who worked in a Korean NICU reviewed the codebook to increase rigor. After completing qualitative data analysis and qualitative verification using peer debriefing and the audit trail, all quotes yielded from these analyses and verification methods were translated into English by a professional translator and reviewed by the authors.
Ethical consideration
This secondary analysis study obtained exemption from a university’s institutional review board (IRB). The original study was reviewed and approved by another university’s IRB. The informed consent forms, including the description of the purpose, procedure, risks, and benefits of the study, were received from the study participants during the original study.
Results
Participant characteristics
Characteristics of participated NICU nurses.
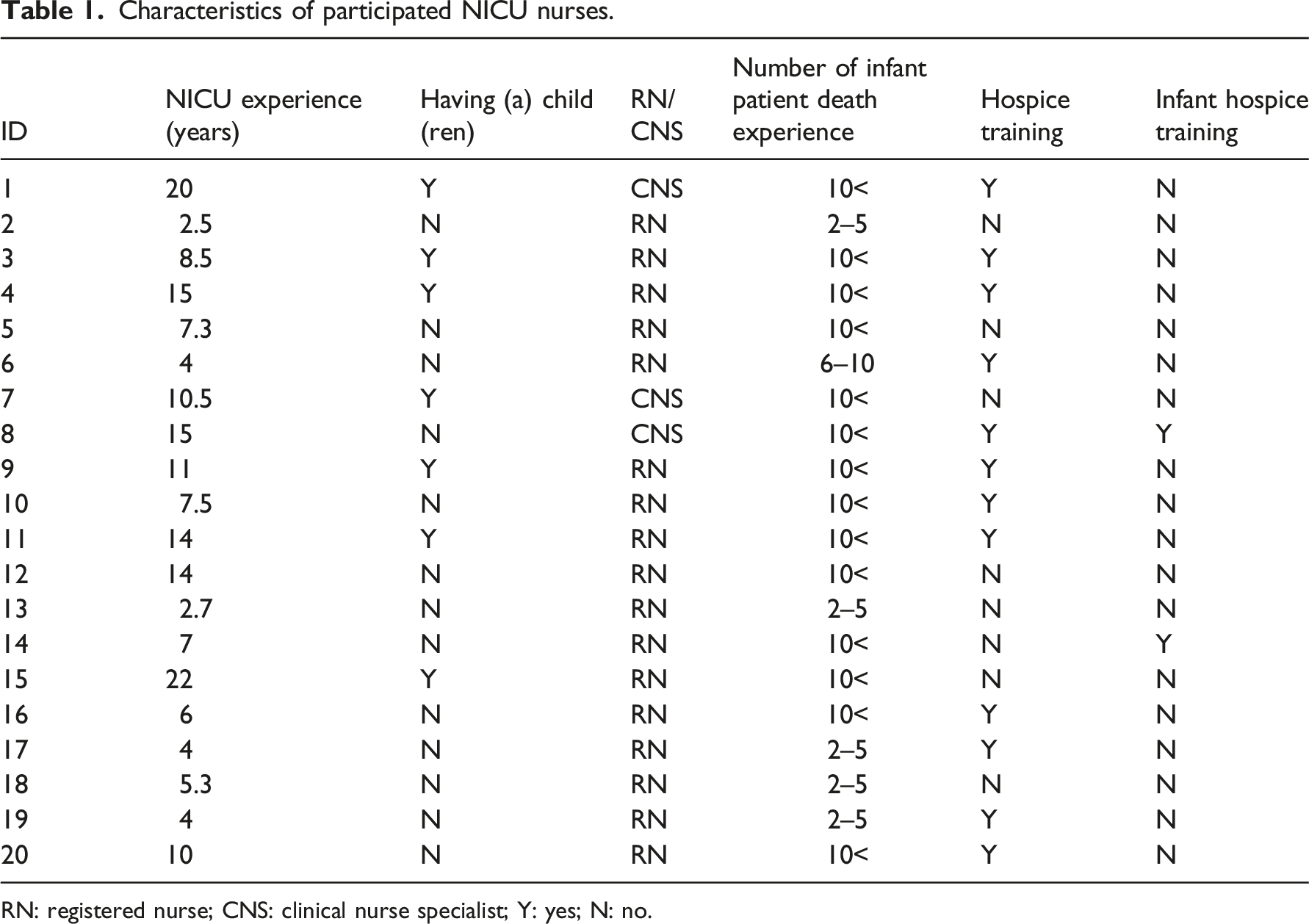
RN: registered nurse; CNS: clinical nurse specialist; Y: yes; N: no.
Korean NICU nurses’ moral distress
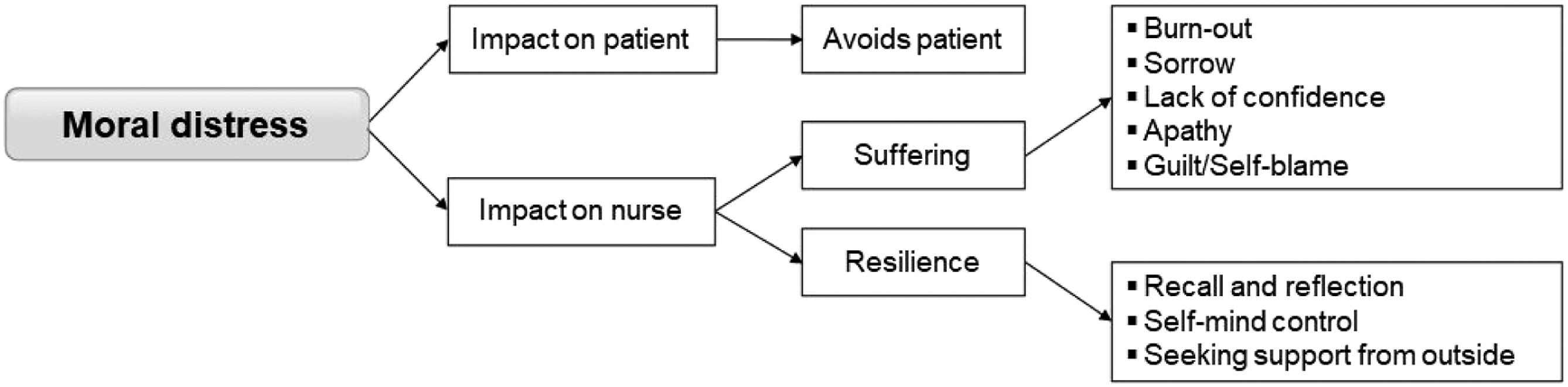
Based on the theory (7) and definition (1), morally distressing situations were coded and categorized as moral constraints or conflict based on the characteristics of the coded situation. Identified themes of moral constraints and conflicts were presented in Figure 1. In addition, impacts of the moral distress were coded and categorized based on the impacted subjects, including nurses, patients, or organizations. Identified themes of impacts of moral distress were presented in Figure 2. Derived themes of moral constraints and moral conflicts among NICU nurses. Derived themes of impacts of moral distress on patients and nurses.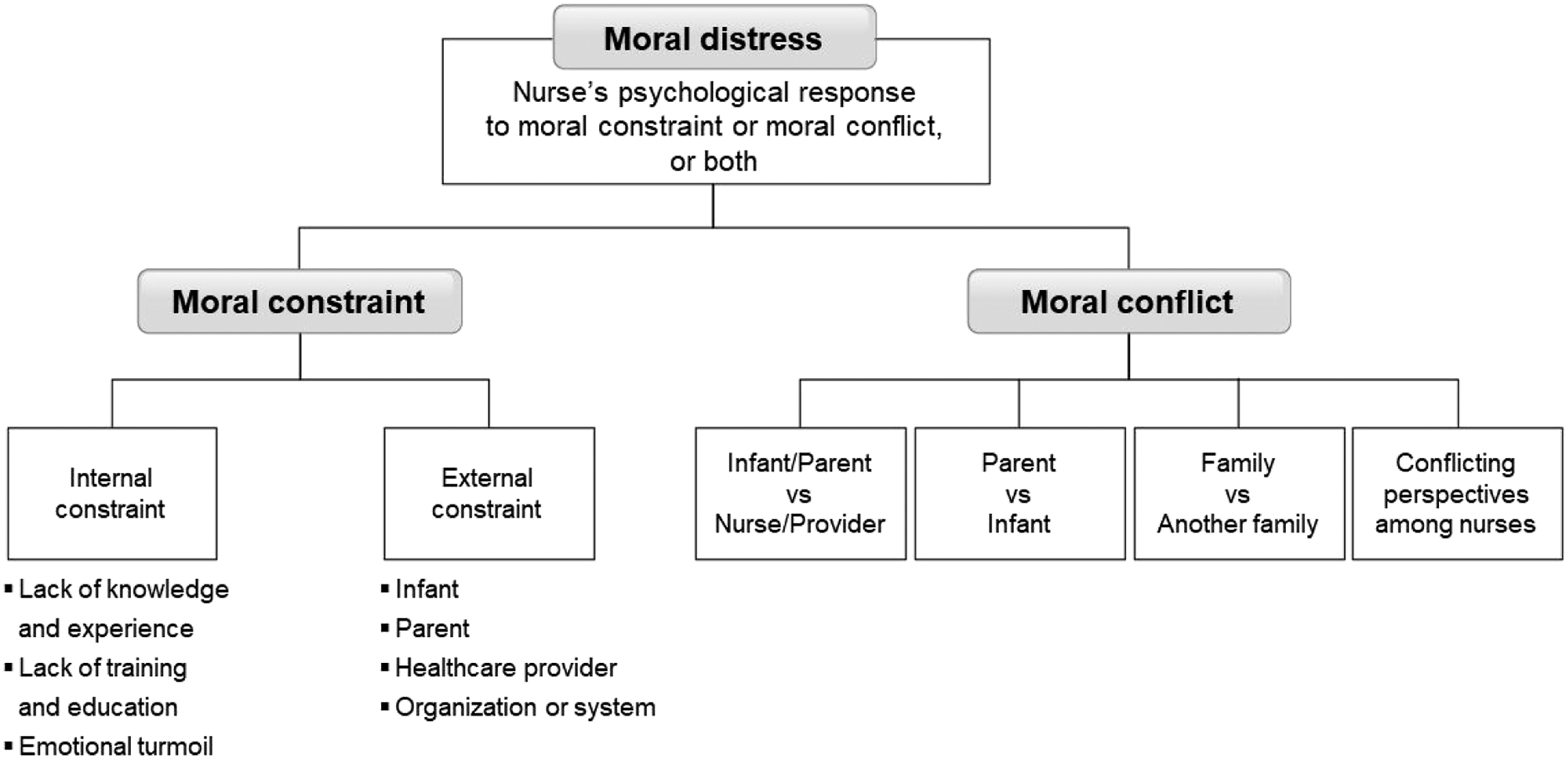
Moral constraint
Themes related to moral constraints were categorized into two main sub-categories—internal and external. These internal and external constraints can lead to moral distress among nurses.
Internal constraint
Nurses experience moral distress due to internal constraints such as lack of knowledge and experience, lack of training and education, and emotional turmoil. Some nurses expressed that they experienced moral distress because of a lack of experience and education. One nurse said, “I’ve rarely encountered death, and have never received any training or education on what to say. Since I don’t have much experience, there are things that I can’t associate with and are careful to do so” (N5). Another nurse identified lack of education as a hindrance to improving their communication skills. “I would like to encourage and comfort mother, and leave a few words for the baby. But I unsure whether I am allowed to interfere at the moment or talk to the baby when I am considered as an outsider (of the family). Even if I wanted to say something, I don’t know if I'm allowed to do so, but when I don’t (do something), it seems as if I’m neglecting the parents of the baby I’ve been caring for. It’s a dilemma.” (N20)
In addition, one nurse shared the status of her emotional turmoil. The nurse stated that since she could not manage her own emotion, she could not interact with parents who were unable to deal with the situation of their critically ill infant. She said, “I was so panicked at that moment [because of a previous bad experience in which I saw parents fall down after seeing suddenly worsened baby]. It was like that regardless of the years of nursing experience. It might be my personality.” (N14)
External constraint
Besides the internal constraints, there are external constraints associated with outside factors that include an infant, a parent, a healthcare provider, and an organization/system. The first external constraint is related to an infant’s condition. Nurses sometimes do not have enough time to prepare for quality end-of-life care. The following two quotes describe nurses’ moral distress related to this external constraint regarding infants’ fatal conditions. “When it all happens so fast, it’s actually hard. There are many cases of death within a few hours shortly after arrival. It’s too short a time for the parents to grasp the situation and to accept it. And so are we…..”(N12) “Among the things I recall, but couldn’t control anyway, was when the baby’s condition suddenly worsened that we had to perform CPR….. It almost felt like I was forcing them to accept the dire situation by showing them the unsettled scene.” (N19)
Specific themes of external constraint that were related to parents included (1) parents’ indifference toward an infant, (2) parents’ different perceptions toward better care, wishes, and goals, and (3) parents’ religious and/or cultural beliefs. Regarding parents’ religious and/or cultural beliefs, nurses shared that Korean culture creates an atmosphere that urges the infant’s mother to forget about the baby as soon as possible than cope. “When a baby dies, although it may be overwhelming to keep, I think keeping one or two items of the baby’s belongings might by fine for parents to reminisce about. But, there are times when the grandparents present at the site of death say, “Why try to remember it all when it only breaks the heart? Just burn it all.” It seems like a Korean thing. Culturally, we mostly tell mothers, ‘You should get over it quickly.’” (N1)
The specific themes of external constraint that are related to healthcare providers included (1) providers’ preference for aggressive care, which may lead to the absence or omission of palliative care, and (2) healthcare providers’ perception that parents are not participants in the end-of-life care process. One nurse said: “I think the healthcare professionals still believe that parents shouldn’t be involved (in the process of treatment). Rather than treating patients with the help of caregivers/parents, parents are more perceived as people who should be watched or those who make us (healthcare professionals) uncomfortable. If we let parents remove the monitor or medical devices when the patient dies, it may give them a better opportunity (to provide end-of-life care by themselves) and may be more helpful for their emotions. But (still), even at that moment, they are usually asked to step out.” (N3)
The specific themes of the last external constraint that are related to organization/system included (1) inappropriate environment such as limited private space, (2) staffing shortage resulting in nurses’ busy schedule due to heavy workload such as taking up various responsibilities of other patients, documenting, clearing the bed where a patient died, preparing for the next admission, returning medications after the death, and repeating information about death certificate to parents who couldn’t pay attention to the same at the time of death, (3) negative effects of rotating shift work for different patients on quality and continuity of care for each patient, (4) visiting policy that limits siblings’ visit, and (5) poor management, lack of educational opportunities, and non-established protocol. As an example of a non-established protocol, one nurse shared: “This was the first case that the ventilator was turned off even though the baby had spontaneous breathing on the ventilator, which was approved by the hospital ethics committee. I, on the other hand, was a bit befuddled because currently there isn’t any protocol that specifies in which circumstances more painkillers or sedatives should be administered to the infant… Because at that time, even after following the attending’s verbal orders, most healthcare providers thought that the baby must’ve suffered a lot. In fact, since there was no precedent for such a case… I’m not saying that our treatment efforts were insufficient, but it felt like we could’ve done much better. So I think it would have been nice if research was conducted.” (N13)
Moral conflict
This concept captures a situation mostly where nurses experience moral dilemmas between two parties who maintain opposing ethical positions. Our analysis revealed four specific themes of the following conflicting pairs—(1) infant/parent versus nurse/provider; (2) parent versus infant; (3) family versus another family; and (4) nurse versus another nurse.
Infant/parent versus nurse/provider
The first theme, infant/parent versus nurse/provider, was primarily identified when nurses feel uncomfortable with following physicians' orders of providing continuous aggressive care for an infant because they do not think it is not an action for the infant. For example, nurses sometimes think that continuously checking blood labs and keeping the infant alive with a life support machine gives only pain and discomfort to the infant despite having no chance of recovery. Additionally, nurses experienced the conflicted feeling when maintaining the convenience and efficiency of their practice while thinking about advocating for the infants and their families. For example, while nurses wanted to help the infant and families have more attachment during end-of-life, they did not want to let parents hold an infant, as it can be risky without supervision. One nurse said, “When the infant is close to death, I think it is fine for the parents to hold them. But typical nurses or mostly show concern by saying, “What if the ventilator detaches from the infant,” “Shouldn’t we stay in front of them?” Since a little movement of the body can cause a change in his/her condition when parents cuddle them, there’s an atmosphere of reluctance.” (N8). Also, when parents do not trust the providers and nurses and want to remain in the NICU with an infant, nurses have a difficult time because parents tend to get involved and interfere with their work. Lastly, nurses cannot be certain if it is right to clean the dead body before inviting parents or if they should invite parents immediately after an infant’s death.
Parent versus infant
The second theme, parent versus infant, is identified when there are conflicts between the best care for the infant and parents’ preference and hope to pursue life-sustaining treatments. In this case, parents pursue continuous aggressive care even though nurses believe that providing comfort care is best for the infant. From the interview transcripts of 20 nurses, seven nurses reported this theme of their moral dilemma between parents and infants. One nurse said, “As I have worked for years, there are times when I often feel that the baby can’t be resuscitated through CPR anymore.… It’d be better if the baby suffered less before death, and for the parents to feel like they did their best. But then, parents tend to ask for us to go the full distance by doing everything we can. Which in turn would cause harm to the infant.” (N10) Another nurse also mentioned a similar situation: “The mother and father couldn’t give up on their baby. I mean, even though there was no chance of recovery, they would relentlessly try everything. It felt as though the baby was being ill-treated, almost to the point of being bothered. As far as I remember, those cases ended up being the worst ones.” (N19) Nevertheless, one nurse addressed the opposite case in which parents decided in favor of comfort care, although more aggressive treatments could have been applied to the infant.
Family versus another family
The third theme, family versus another family, is identified mostly when visits are allowed for extended family members of an infant at the end-of-life stage. Nurses have a responsibility to maintain consistency regarding visiting policies for all families. Most Korean NICUs have provisions for limited visits. Nurses experience moral dilemmas when they cannot allow visitors to go in. Nurses sometimes think family members who are not allowed to visit may think that they cannot do anything for the patient. Nurses think limiting visits can prevent infections, but families lose their moment to be with the infant before the time of death. When nurses create a separate private room to allow extended family members to see the infant at the end-of-life stage, other families with an infant whose time is yet to come complain, asking why they are not allowed to visit. In addition, when family members are grieving loudly, it affects other families in the same room. The adjacent families can feel grief, worry, and even terrified. One nurse said, “They wept loudly in the unit, which made the other caregivers/parents turn sad, alarmed, and scared because we are closely spaced. When a death occurs nearby, other mothers and fathers start to worry if their baby might die too.” (N4) Nurses think such family’s response interrupts them from providing good quality end-of-life care to other families.
Two or more conflicting perspectives among nurses (Nurse versus another nurse)
The fourth theme, nurse versus another nurse, is identified when nurses have different perceptions about delivering bad news. While some nurses think they should tell the truth, including about poor prognoses, other nurses think they should or want to deliver only good news.
Impact on patient
Several nurses tried to keep a distance from infants and their parents for varying reasons. One nurse avoided parents who lost their infant because she did not know how to communicate with them. Other nurses said they avoided them because they had a very difficult time after the death of an infant when they were too emotionally attached to the infant. Another nurse said she did not want to be assigned to one infant because she believed that what she had to do was only damaging the infant’s physical condition.
Impact on nurse
Two primary concepts of impacts on nurses—suffering and resilience, were identified.
Suffering
The concept of suffering is specifically divided into five specific themes—(1) burnout, (2) sorrow, (3) lack of confidence, (4) apathy, and (5) guilt and self-blame. To specifically explain apathy as one of the negative consequences, two nurses said they are becoming more detached and machine-like due to repeated work. One of the two nurses said, “When it repeats and I’m swamped with work, I eventually become a person who needs to get things done quickly, regardless of whether it’s providing end-of-life care or not. So there’s a gap between the ideal type of end-of-life care I think of and what I actually do.” (N10)
Resilience
The concept of resilience is further divided into three specific themes—(1) recall and reflection, (2) self-mind control, and (3) access and utilize outside help and resources such as religion and friends. Based on our analysis, it is not always the case that there are only negative consequences of end-of-life care among nurses. To elaborate on the theme of recall and reflection, nurses sometimes recalled a time from their work experience and questioned what steps they would or could have taken differently if given the same situation. For example, one nurse said she recalls the time when an infant suffered due to insufficient pain control. She could not remember every end-of-life situation, but she could clearly remember the situation when the infant passed away in pain.
Discussion
The results of this study detailed the situations in which Korean NICU nurses experience moral distress, their emotional reactions to this distress, and how they cope with it, based on a theory of moral distress. 7 This study generated extensive information on morally conflicting situations that nurses frequently encountered in critical care settings and their responses to such conflicting situations. Moreover, it provided foundational knowledge for future studies that can focus on developing instrument that measures moral distress surrounding end-of-life care or interventions for decreasing moral distress among nurses who care for dying infants and their families.
This study reported detailed situations where moral distress can occur among NICU nurses. Some situations were similar to those found in previous studies conducted on pediatric nurses.25,26 One study that was conducted in pediatric oncology settings in Sweden used an instrument to measure the level of moral distress and highlighted that nurses experienced morally distressing situations more frequently than medical doctors and nursing assistants. 25 The study identified lack of competence and continuity of care and inadequate staffing of nurses as contributing factors to morally distressing situations. 25 Another study conducted in Canada also identified certain circumstances such as patients’ unmanaged pain and unnecessary suffering that can cause moral distress among NICU nurses leading them to experience negative emotions such as guilt, sadness, hopelessness, and powerlessness. 27 A systematic review was done to capture and categorize pediatric oncology staffs’ stress and revealed two domains of stressor—(a) organizational issues such as workload, limited time, lack of communication with colleagues, and lack of supplies and staffing; and (b) interaction between staffs and patient or families such as communications on care trajectories with conflicted points of view, witnessing pain and patient loss, etc. 26 Although similar results have been seen, this study could report more detailed and variety of situations which pediatric nurses experience as many of the previous studies have used such instruments to examine the nurses’ moral distress level, which have limitations of discovering detailed situations that are not listed in the instruments. As the need for pediatric-appropriate instruments has been reported in previous studies, this study’s results will provide fundamental knowledge to future studies related to instrument development.
Palliation of distressing symptoms decreases patients’ pain and suffering from unnecessary aggressive treatments. Despite the benefits of palliative or hospice care, family members sometimes have different opinions about how much or how long aggressive treatments should be continued on patients and when to stop those treatments and focus on comfort and hospice care. 28 In this study, several nurses described this family situation as moral distress. They sometimes did not have enough time to discuss end-of-life care or were not competent due to a lack of training or education. This implies the importance of palliative care training and education, which may require support from organizational and system levels.
In this study, identified moral constraints were categorized into internal or external constraints. The findings of our study are consistent with the results found in the literature. 29 That qualitative study reported nurses’ moral distress into four themes—(a) institutional barriers and constraints; (b) communication problems; (c) futile actions, malpractice, and medical/care errors; and (d) inappropriate responsibilities, resources, and competencies. In another study, lack of skills and education, shortage in nursing staff, and lack of time were identified by nurses as constraints that cause moral distress. 30 Their study emphasized that the staffing issue affects nurses’ workload, which can influence the quality of care. 30 Another review study also pointed out the nursing shortage issue as one of the causes of moral distress. 12
This study concurred with previous literature emphasizing that NICU nurses who experience moral distress can bring negative consequences to themselves, patients, and families, such as emotional exhaustion and depersonalization toward patients.12,31 Not surprisingly, the participants of our study expressed negative consequences on themselves, including burnout, sorrow, lack of confidence, apathy, and guilt/self-blame as well as for patients, including avoiding tendencies. However, all their responses to moral distress were not negative. In this regard, this study’s findings are essential because our qualitative analysis broadly explored the impacts of moral distress on nurses to capture their positive coping strategies, and resilience and not limiting to identifying contributing factors of moral distress. A few nurses reported their coping styles and resilience. They tried to cope with moral distress to some extent, and further, they reflected on past situations to think about how they would do differently in the future. Understanding how they manage their moral distress can be a worthwhile starting point to support shifting from the negative consequences of moral distress to the development of resilience. As such, there is a need for further studies focusing on the development of interventions to improve resilience among nurses experiencing moral distress.
The limitations of our study warrant consideration. First, this study was conducted using a dataset that was collected from two major hospitals in Seoul, South Korea. This homogeneous sample may not be generalized to other settings, such as hospitals located in rural areas or countries with different environments or cultures. Second, as end-of-life settings are complicated, the sample size can still be relatively small. In addition, when nurses were interviewed, the interview questions were not aimed to cover aspects of coping experience. Therefore, it is difficult to delve into and rely on only the findings of this study for all coping experiences of nurses. Coping styles may differ across individuals. Future studies can support finding other relevant themes of coping strategies for moral distress among diverse nurses.
Conclusions
This study explores various themes of moral distress and their impacts on NICU nurses in Korea. Based on Corley’s theory of moral distress, situations that cause moral constrains and moral conflicts among NICU nurses were identified and categorized. In addition, their impacts on nurses and patients were explored in detail. Continuous investigation and exploration of nurses’ experiences related to moral distress and their coping experience is important to support the moral resilience of nurses. This would help them provide better quality care to patients and their families.
Footnotes
Acknowledgments
The authors are sincerely grateful to interview participants and nursing staff members who supported the recruitment and enrollment process.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors wish to acknowledge the financial support of the Catholic Medical Center Research Foundation made in the program year of 2021 and Summer Faculty Fellowship from Seattle University.