
Abstract
This concept analysis aims to clarify the definition and key components of nurses’ guilt associated with patient death. Walker and Avant’s methodological approach was employed to identify defining attributes, antecedents, and consequences. A comprehensive literature review was conducted using PubMed, CINAHL, MEDLINE, PsycArticles, Scopus, and the Cochrane Library, focusing on articles published between 2015 and 2025. The literature search and selection process are reported in accordance with PRISMA guidelines. The analysis revealed four defining attributes of nurses’ guilt: (1) Feeling responsible for the patient’s death, (2) Fear of condemnation, (3) Regret, and (4) Self-denial. Antecedents were classified into five domains, namely, the nature of the death, the nurse’s relationship with the patient and family, professional mission and role expectations, ethical dilemmas encountered during care, and concerns regarding one’s involvement in the dying process. The consequences of guilt extended beyond emotional responses, encompassing long-term physical and psychological health effects, self-alienating behaviors, and changes in introspection, meaning-making, and professional identity. These findings suggest that guilt following a patient’s death is a complex, reflective process rooted in nurses’ professional values and moral responsibilities. By clarifying the structure and characteristics of this concept, this analysis provides a shared conceptual framework applicable across diverse cultural and clinical contexts. The findings of this concept analysis suggest that nurses’ guilt related to patient death is not merely an individual psychological reaction but also constitutes a moral injury involving professional judgment and responsibility. The findings highlight the importance of ongoing psychological support for nurses who have experienced the death of a patient. Such support should include educational components that deepen understanding of the guilt experienced by nurses in these situations, as well as opportunities for dialogue and reflection with colleagues who have had similar experiences.
Introduction
For nurses, facing a patient’s death is a critical moment. Nurses may experience deep guilt over such experiences, which is often linked to feelings of self-reproach for their own judgments and actions.1–3 In the narratives of nurses reported by Mast and Gillum (2018), one nurse stated, “If I had spent more time in the room, I might have noticed small changes, contacted the physician earlier, or given other instructions. Thinking that I might have been able to do something to save someone makes me feel deeply sorry.” This illustrates the sense of responsibility that nurses can feel regarding patient deaths. 4 For nurses, a patient’s death is not merely a clinical event but a psychological experience closely intertwined with their professional responsibility and the way they perceive and understand themselves as human beings. Because nurses establish a caring relationship with patients in which they take responsibility for addressing patient needs and resolving health problems, it is not uncommon for them to experience feelings of guilt or internal conflict when a patient dies.
Clarifying the essence of nurses’ guilt and systematically organizing its conceptual structure are critically important for advancing empirical research and laying a foundation for practical interventions to support nurses.
Based on the above, this concept analysis aims to clarify the conceptual characteristics of guilt experienced by nurses following a patient’s death by focusing on the subjective and relational dimensions that cannot be explained solely by the presence or absence of objective negligence or wrongdoing, particularly guilt arising in relation to relationships with patients and their families and the roles expected of nurses.
Background
Nurses routinely encounter patient deaths, leading to psychological burdens such as guilt, 5 intense grief, 6 negative emotions, 7 helplessness, and physical and mental fatigue. 8 Repeated exposure to these emotions can lead to serious mental health problems, including caregiver fatigue (also known as empathy fatigue), chronic work-related fatigue (also known as burnout), and secondary post-traumatic stress disorder, which can result in symptoms similar to those of post-traumatic stress disorder from indirect traumatic experiences.7,9,10
Such conflicts are particularly pronounced in clinical settings such as intensive care units, 11 pediatric and neonatal wards, 7 end-of-life care facilities, 12 and infectious disease wards. 13 Nurses often engage in self-critical reflection on whether a patient’s death resulted from their own mistakes or whether they had provided sufficient care. Furthermore, even when they feel they did their best for the patient or when their care appears sufficient to others, nurses may still experience feelings of guilt.12,14
Some studies have suggested that guilt contributes to psychopathology, whereas others have suggested that guilt may play a protective role. 15 Guilt may lessen over time or through receiving support from colleagues. However, when sufficient support is unavailable or internal conflicts remain unresolved, guilt may persist and subsequently lead to psychological distress. 16
Focusing on the guilt experienced by nurses following a patient’s death is an important aspect of understanding nurses’ grief and stress responses because nurses who continue to feel guilty and blame themselves after a patient’s death may experience prolonged grief. 17 Furthermore, guilt is an emotion that nurses directly internalize. It arises when individuals perceive that they “could not do enough” or “may have hurt another person” through their actions or inaction, and it is experienced in relation to actual or imagined moral violations. 15 Persistent and intense guilt has also been associated with psychological distress and psychopathology. 15
Although guilt has a substantial impact on nurses’ mental health, it also plays an interpersonal role, such as promoting consideration for others, a sense of responsibility, and reparative actions. 15 In addition, guilt may provide an opportunity to deepen understanding and meaning through profound self-reflection.18,19 Furthermore, the experience and interpretation of guilt are thought to vary according to developmental stage and interpersonal context, and guilt has therefore been understood as a social emotion.15,20
In nursing and caregiving contexts, guilt is often experienced even in the absence of actual wrongdoing or a punishable act. For example, nurses who experience a patient’s death may feel that “even though I did my best, it still does not feel like enough,” 5 even when they had in fact done everything possible, or they may feel that “I was somehow involved in that death as well” 4 while participating in physicians’ decisions or treatment processes. Thus, individuals may experience guilt even in the absence of misconduct or negligence. Guilt may also arise when individuals feel that they “could not adequately fulfill their role.” That is, nurses’ guilt following a patient’s death includes both subjective and relational dimensions that cannot be explained solely by the presence or absence of objective responsibility.
In addition to guilt, concepts related to nurses’ experiences following a patient’s death include shame and moral distress. Although these experiences may occur in relation to one another, each concept emphasizes a different aspect. Shame is associated not with a negative evaluation of one’s actions but rather with a negative evaluation of the self, and it is positioned as a self-conscious emotion accompanied by diminished self-worth.21,22 In contrast, bioethicist Andrew Jameton defined moral distress as “the distress that arises when one is unable to carry out what one believes to be the right action because of institutional or situational constraints.” 23 This concept is characterized by its focus on situations in which action is constrained as well as the accompanying sense of powerlessness.
In this concept review, guilt is understood as an internal and distressing self-evaluative emotional response that arises when nurses feel that they could not adequately fulfill their role or involvement in situations related to patient death. This experience may involve regret, self-reflection, and thoughts of reparation, and it is shaped by complex interactions among relationships with patients and their families, perceptions of the dying process, and interpretations of the clinical situation. This definition was adopted to capture nurses’ guilt following a patient’s death as a subjective experience that includes how nurses interpreted their relationships with patients and their families, as well as the meaning they attributed to their own role.
Purpose
This concept analysis aims to elucidate the conceptual components and definition of guilt experienced by nurses in the context of patient deaths.
Methods
Data collection
A literature search was conducted using four electronic databases: PubMed, CINAHL, MEDLINE, PsycArticles, Scopus, and the Cochrane Library. The following search terms were used: “nurse AND (patient death OR patient loss OR death of patient) AND (guilt OR grief OR suffering OR distress).” Because the guilt experienced by nurses in response to a patient’s death is assumed to involve both universal characteristics and context-dependent features influenced by social and temporal factors, the search period was limited to a 10-year span from 2015 to 2025. The initial search yielded 2966 articles. The search results were imported into EndNote 2025. After removing duplicate records and screening the titles and abstracts, 121 articles were selected. Articles were excluded if they (1) did not target nurses, (2) did not include antecedents, attributes, or consequences relevant to the phenomenon, or (3) were published in languages other than English. Following this screening process, a total of 34 articles were included in the final analysis (Figure 1). We followed the PRISMA 2020 reporting guideline
24
when drafting this manuscript, and the PRISMA 2020 reporting checklist
25
when editing (Supplemental A). PRISMA flow diagram for selection process.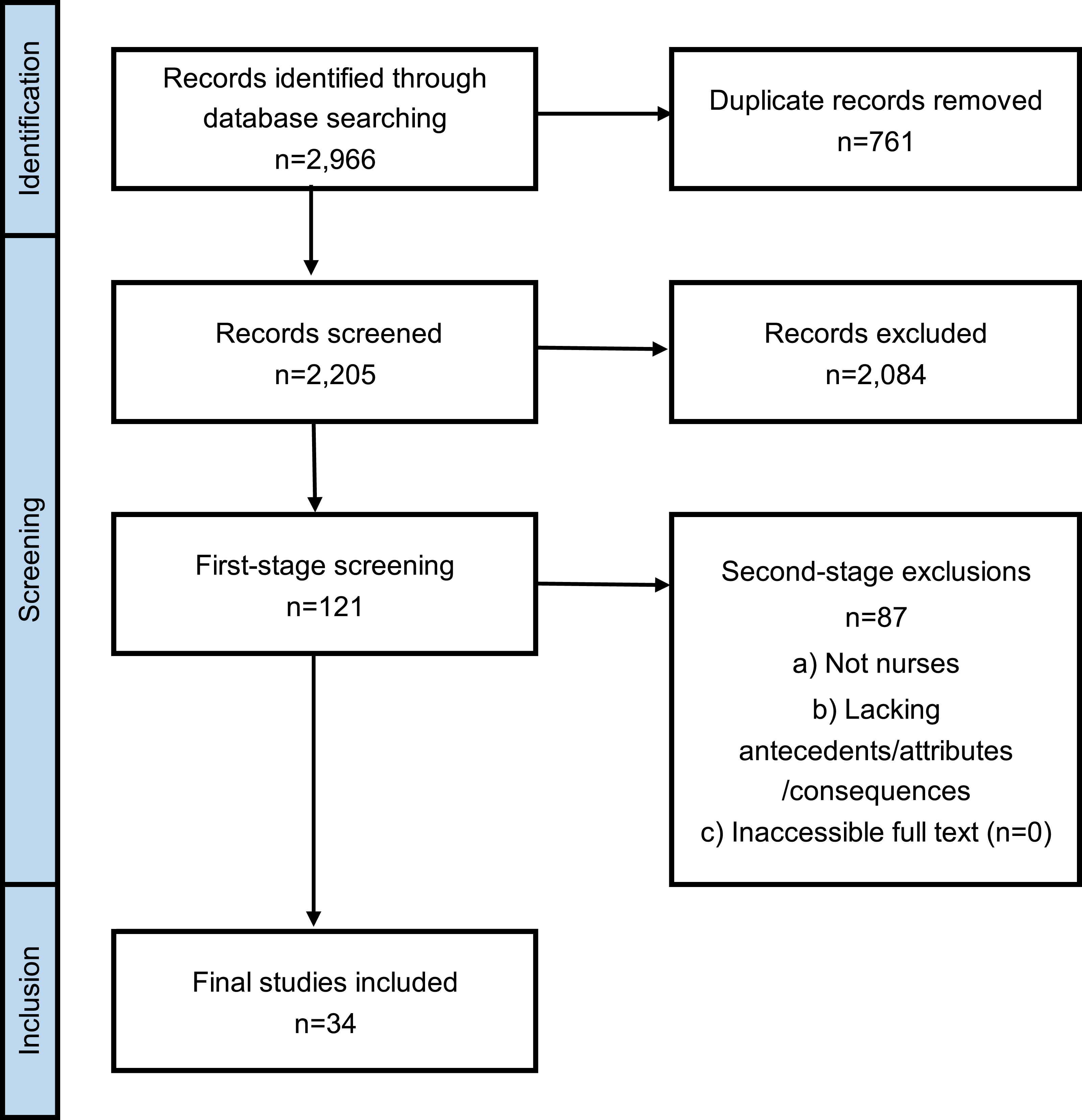
Concept analysis method and procedure
1. Concept Selection: The concept of guilt experienced by nurses when they experience a patient’s death was chosen as the focus of the analysis. 2. Determination of the Analysis’s Objective: The objective was to construct a theoretical framework for guilt. 3. Identification of All Concept Usages: The concept of “guilt” was investigated using the available literature, general dictionaries, psychology dictionaries, and specialized terminology lists such as MeSH (Medical Subject Headings) to explore its usage in as many contexts as possible and to comprehensively cover its full range of meaning. 4. Determination of Definitive Attributes: Three groups of attributes that are most frequently associated with and provide broad insights into the concept of “nurse guilt regarding patient death” were identified as defining characteristics of the concept. 5. Identification of a Model Case: A model case is an example that illustrates all the defining attributes of the concept of “nurse guilt regarding patient death.” This concept review presents a typical scenario illustrating the concept through a fictional case in which a young girl, who had repeatedly been hospitalized and developed close relationships with nurses since childhood, suddenly deteriorated and died in agony. 6. Identifying Borderline and Counterexamples: Borderline examples are cases that satisfy most of the defining attributes of the concept but not all of them. This concept review presents a hypothetical case in which a nurse, while acknowledging that death is a natural process, feels blamed by the family for not being able to provide adequate care to an elderly woman with terminal cancer with whom she had developed a close relationship. This hypothetical case illustrates the boundary between this concept and related concepts. Counterexamples are cases that do not represent the concept. This concept review illustrates a situation where this concept does not apply, using a hypothetical case in which a nurse, who provided daily care while respecting the wishes of an elderly patient, felt deep satisfaction with the end-of-life care she provided. 7. Identifying Antecedents and Consequences: Five antecedents were identified, referring to events or situations preceding the emergence of the concept: Nature of Death, Relationship with Patients and Their Families, Professional Sense of Mission, Ethical Dilemmas, and Regrets in Practice. The following three consequences, which refer to the events and results following the emergence of the concept, were identified: Effects on Mind and Body, Changes in Reflection and Meaning-Making, and Effects on Relationships with Others. 8. Identifying Empirical Reference Points: Observable phenomena demonstrating this concept were organized based on the perceptions and experiences of nurses described in the literature.
Results
Concept selection
Given that nurses who experience patient deaths often face substantial psychological burdens, and that there is no clear and unified definition regarding guilt arising from end-of-life care experiences involving regret or moral conflict, this concept analysis examined the concept of “nurses’ guilt regarding patient death.” Nurses routinely confront patient deaths in their daily practice and may experience guilt stemming from feelings of inadequate care 5 or perceived insufficient effort. 12 Such emotions can become traumatic, leading to prolonged psychological distress. 16 Despite its significance, the essence of this form of guilt remains insufficiently clarified. In particular, guilt associated with a patient’s death may be related to the loss of opportunities to make amends directly to the patient. Although irreversible events other than death also occur in clinical settings, healthcare providers may sometimes be able to compensate for their actions or repair their relationship with living patients through subsequent care and continued involvement. In contrast, after a patient’s death, opportunities to interact directly with or make amends to the patient are lost. 26 As a result, nurses may continue to carry these experiences within themselves, which can cause the guilt related to a patient’s death to persist more strongly and for a longer period of time.
Determination of the aim of the analysis
Analyzing the concept of “nurses’ guilt regarding patient deaths” enables the identification of its defining attributes, antecedents, and consequences specific to nurses. This not only facilitates a shared understanding and terminology that can be applied to future research but also provides a foundation for developing measurement instruments and intervention programs. Furthermore, nurses’ guilt regarding a patient’s death is associated with emotions such as grief and shame as well as feelings of powerlessness, and these emotions can complicate the grieving response. Analyzing this concept is essential for clarifying nurses’ psychological experiences when facing patient deaths as well as for informing appropriate support strategies.
Based on the above, this concept analysis aims to clarify the structure and definition of nurses’ guilt regarding patient deaths.
Uses of the concept of “Guilt”: General, nursing, and psychological perspectives
Guilt has been studied across multiple disciplines, including nursing. Guilt is a complex and multifaceted concept, and its definition and conceptualization vary across fields of study. 15 Previous research has suggested that guilt is associated with psychopathology, while also highlighting its adaptive functions, such as promoting feelings of remorse, responsibility, and reparative behaviors. 15 Furthermore, the definition and measurement of guilt may differ across developmental stages. 15 Nevertheless, a common feature across these various conceptualizations is their focus on an individual’s actions or inaction in relation to real or imagined moral transgressions. 15
In this concept review, guilt is understood as an internal and distressing self-evaluative emotional response that arises when nurses feel that they could not adequately fulfill their role or involvement in situations related to patient death. This conceptualization was adopted to understand nurses’ guilt following a patient’s death, not only in terms of objective responsibility but also in relation to the subjective meanings that nurses attribute to their roles and relationships with patients and their families. The attributes identified through this concept analysis were also associated with perceived responsibility for the patient’s death, relationships with patients and their families, and negative self-evaluations of one’s actions or inaction, thereby supporting the conceptualization adopted in this concept analysis.
The conceptual framework of nurses’ guilt regarding patient death identified in this study provides a foundation for clarifying the structure of guilt, which has previously been understood in an ambiguous manner, and for achieving a deeper understanding of this experience. This framework may also facilitate the identification of factors that intensify nurses’ psychological burden and the aspects of their experiences that require support, thereby contributing to the early recognition of support needs and the development of appropriate psychological and educational interventions. Furthermore, this conceptualization offers a perspective that understands guilt not merely as a negative emotion but also as an experience that may foster reflection and personal growth. The defining attributes, antecedents, and consequences of this concept are illustrated as a conceptual model in Figure 2. Conceptual model: Antecedents, attributes, and consequences.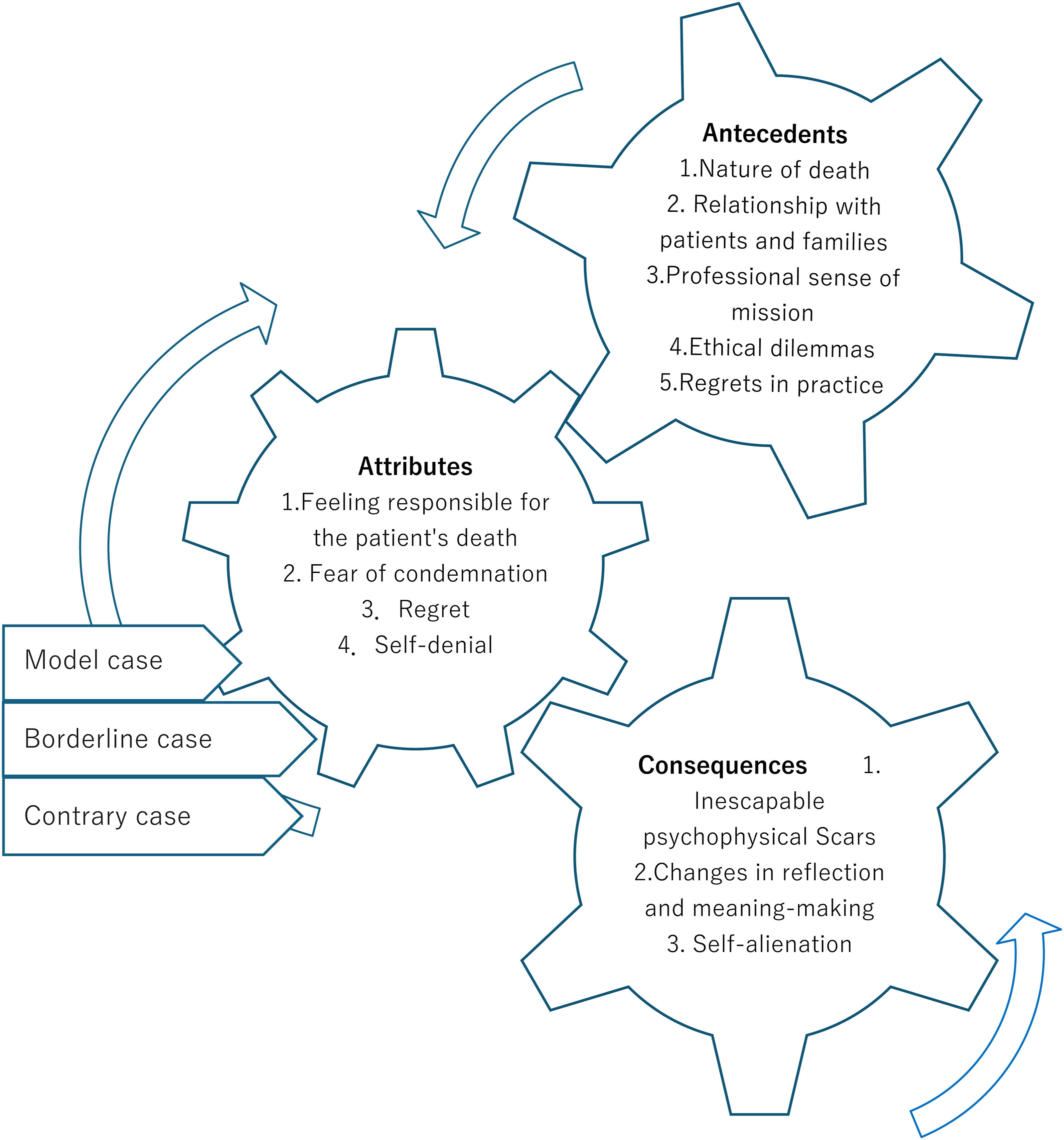
Defining attributes
Analysis of the included literature revealed that the guilt experienced by nurses following a patient’s death comprises four defining attributes that were commonly identified across multiple studies. Guilt experienced by nurses following a patient’s death is an emotional experience characterized by feeling responsible for the patient’s death, fear of condemnation, regret, and self-denial. This emotion is rooted in the perception that one’s actions or judgments may have contributed to the patient’s death and constitutes an internal experience that is common to the four defining attributes identified in this concept analysis.
Feeling responsible for the patient’s death
Feeling responsible for a patient’s death refers to attributing a patient’s death to one’s own actions, inaction, or lack of competence and experiencing a feeling that one may have brought about the patient’s death.14,27,28 This feeling constitutes the foundation of all three subsequent attributes and is regarded as a core component of guilt. In particular, nurses have been reported to experience a strong sense of responsibility when they are involved in resuscitation efforts or in the care provided immediately before a patient’s death, questioning whether their actions may have contributed to the patient’s death or whether they might have overlooked important signs related to the patient’s impending death.4,14 This feeling that one may have brought about a patient’s death becomes deeply rooted regardless of the actual causal relationship and is experienced as a heavy psychological burden that is difficult to dispel even in the absence of objective evidence to the contrary. 14
Fear of condemnation
Fear of being blamed refers to the experience in which nurses confronted with a patient’s death perceive the family members’ anger, distrust, or even the possibility of verbal or physical violence toward healthcare providers as attacks directed at themselves.16,27,29 For example, when a patient who had been recovering and was preparing for discharge dies unexpectedly, the family may express distrust toward the healthcare team or the hospital. 16 In such situations, although nurses recognize the need to face the family, they may experience intense anxiety and fear that the family’s words or behaviors may escalate into personal blame or accusations of responsibility. 16 This fear can lead nurses to interpret the family’s emotional expressions not simply as manifestations of grief or anger but as signs of negative evaluation or a potential attack directed at themselves.16,27,29
Regret
Regret refers to the emotion experienced by nurses when, in reflecting on a patient’s death, they feel a sense of inadequacy and come to regret their own actions or clinical judgments.16,27 This emotion is closely linked to nurses’ strong sense of professional responsibility to protect and care for their patients, and it arises through the process of evaluating both the care they provided as well as their inaction.12,30 As nurses reflect on the patient’s suffering and the events leading to death, they may think, “I should have provided better care,” or “Perhaps I did not fully fulfill my role,” leading them to question the appropriateness of their own judgments and actions.2,16,27 Faced with the irreversible outcome of a patient’s death, nurses experience profound remorse stemming from the belief that they were unable to adequately fulfill the role expected of them. 31 Therefore, regret is not merely a reflection on past actions but emerges as an introspective emotional experience through which nurses re-evaluate the appropriateness of their judgments and the care they provide as healthcare professionals. 12
Self-denial
Self-denial refers to the negative self-evaluation in which nurses interpret a patient’s death as the result of their own flawed judgments or inadequate care, thereby devaluing their worth and significance as nurses.27,32,33 This concept represents a critical threat to nurses’ professional identity. When nurses perceive a patient’s death not as a natural outcome but as the consequence of their own actions, they evaluate the death as a “failure” of their care.28,33 Such perceptions extend beyond judgments about the care provided at that moment and influence their sense of professional worth, prompting thoughts such as “I was not enough” or “I cannot forgive myself,” thereby undermining their perceived value as nurses.16,32 Rather, this sense of failure is not merely about a specific action but is an emotional response that arises when nurses feel that their professional identity has been damaged, reflecting deep distress tied to their values as nursing professionals.
Antecedents and consequences
Antecedents
Nature of death
The nature of death refers to characteristics of death, including sudden death, 5 the death of younger patients, 33 and solitary death, 16 that may trigger guilt in nurses. When a patient’s death is unpredictable or appears to deviate from the natural course of life, as in the case of younger patients, nurses may question whether there were problems or oversights in their care, resulting in feelings of guilt. 34 Additionally, situations in which ideal end-of-life care could not be provided—such as when a child dies without their family present 16 —also contribute to nurses’ guilt.
Relationship with patients and their families
The depth of the relationship with the patient and their family can lead nurses to perceive a patient’s death as a more personal event, thereby becoming a factor associated with feelings of guilt. 7 Such influences are observed not only in close and positive relationships but also in situations involving frequent complaints or a lack of trust toward healthcare professionals on the part of the family members.16,35 Thus, regardless of whether the relationship is positive or negative, the death of a patient whose relationship left a strong impression on the nurse is identified as a factor associated with guilt.
Professional sense of mission
A professional sense of mission can contribute to feelings of guilt. Nurses approach patient care with a sense of professional duty and a commitment to patient recovery, and situations in which recovery is difficult or a patient dies can trigger feelings of guilt.33,35 This reflects an expectation of patient recovery and a strong awareness of their role as nurses. Furthermore, the very circumstances under which recovery is unlikely can cause nurses to feel that they have not fulfilled their professional responsibilities. 36 This suggests that the expectation for patient recovery, combined with the recognition of this responsibility as part of their professional duty, constitutes a key underlying factor in nurses’ guilt.
Ethical dilemmas
Ethical dilemmas may contribute to feelings of guilt. Discrepancies in values regarding treatment approaches or care provision can be a source of conflict for nurses.16,37 When faced with ethical dilemmas, nurses may experience tensions between their own beliefs and the policies or preferences of the patient’s family or the institution regarding patient care or post-mortem decisions, which can lead to feelings of guilt. During the COVID-19 pandemic, significant ethical dilemmas arose between government mandates or other infection control measures and the professional duty to provide humane, patient-centered care. 38 In treatment decision-making, nurses may also be forced to implement care that conflicts with their own values due to disagreements with the patient’s family. 16 Such ethical dilemmas therefore create situations in which nurses may be compelled to act against their personal values, contributing to feelings of guilt.
Regrets in practice
Regrets in practice may contribute to feelings of guilt. Nurses provide care to sustain patients’ lives or, when death is inevitable, to ensure as peaceful a death as possible.34,39 Experiences in which nurses perceive their involvement to be inadequate—such as failing to alleviate patient suffering 34 or being unable to provide a “good death” 39 —contribute to feelings of guilt. Additionally, nurses may empathically identify with the patient or their family, perceiving the patient’s or family’s suffering as if it were their own, thereby amplifying regret and serving as a factor in guilt. 33 This occurs because, through experiences that reveal the limits of their care or perceived insufficiency of involvement, nurses are prone to experiencing guilt and lingering regret.
Consequences
Inescapable psychophysical scars
A patient’s death can lead to inescapable psychophysical scars. When nurses experience a patient’s death, they may exhibit emotional reactions such as irritability 39 and crying. 5 These emotions are not always transient; they can persist as trauma. Narratives such as, “Even while sleeping, the baby’s distressed face would appear before my eyes and continue to appear in my dreams for months” 16 suggest that such experiences threaten nurses’ daily lives both mentally and physically. Furthermore, as reflected in the statement, “Every time a child with trisomy 18 is admitted, I remember that child,” past experiences were strongly recalled in the present and persisted as recurrent and inescapable distress. 16 This consequence also includes negative self-evaluation and the development of adverse beliefs about oneself. 28 This implies that guilt related to a patient’s death may not remain a temporary emotional response but can leave long-lasting psychophysical scars as traumatic memories and negative self-beliefs.
Changes in reflection and meaning-making
Changes in reflection and meaning-making may occur following a patient’s death. After the death of a patient, nurses tend to reflect on the presence or absence of their own responsibility 28 as well as their professional practice. 14 Through this process, they come to accept the limitations of care and the uncontrollable nature of death, 35 perceiving death as a natural part of life. In this way, nurses—through the extreme experience of patient death—deepen their self-reflection and acquire new meaning. As a result, they reach an acceptance of death and experience “growth,” including the reconstruction of their professional mission and the deepening of personal values.
Self-alienation
Self-alienation may occur following a patient’s death. After the death of a patient, nurses may feel guilt or awkwardness toward the patient’s family and consequently avoid interacting with them.7,40 Additionally, due to feelings of guilt, nurses tend to suppress their emotions in order to prevent colleagues or family members from noticing, thereby internalizing their feelings. 7 Furthermore, they may experience a sense of alienation if they feel that colleagues who experienced the same situation do not share or understand their emotions. 16 Thus, the guilt associated with a patient’s death, underpinned by strong self-denial, can cause nurses to distance themselves from the patient’s family, their own family, and their colleagues, resulting in “self-alienation” and potential isolation both at work and at home.
Model case
Olivia was the primary nurse responsible for Emily, a child who had experienced repeated hospitalizations since early childhood. Olivia had developed a long and close relationship with Emily and her family. After the discharge date was set, Olivia would ask Emily almost daily about what she wanted to do and what she was looking forward to after leaving the hospital.
One day, however, Emily’s condition suddenly deteriorated, and she complained of severe pain and difficulty breathing. Olivia promptly performed resuscitation, but Emily’s condition did not improve, and she passed away in distress. Olivia felt a strong sense of responsibility for Emily’s death, believing that she had failed to anticipate and assess the sudden deterioration. She also felt deeply that her care had been insufficient in alleviating Emily’s pain and breathing difficulties, leading to feelings of guilt and remorse.
Olivia feared that Emily’s family was disappointed in her or blamed her, and after Emily’s death, she was unable to face them. Upon returning home, she cried alone and repeatedly questioned herself about her responsibility. Even years later, the memory of that day remains vivid in her mind, occasionally appearing in her dreams.
Clarification of supplementary cases
Borderline cases
In this concept analysis, a borderline case is presented by excluding the attribute considered central to guilt: “feeling responsible for a patient’s death.” This exclusion is necessary because the presence of this attribute would enable one to definitively categorize the emotion as guilt related to a patient’s death. To maintain the nature of a borderline case, this core attribute is deliberately omitted.
Hannah, a nurse, was caring for Sarah, a woman in her seventies diagnosed with terminal cancer. Sarah had undergone treatment for many years, but gradually all medications lost their effectiveness, and the progression of her disease could no longer be halted, leading to hospitalization for palliative care. Sarah had a close relationship with her family, and her husband and grandchildren visited about once a week. One month after admission, Sarah passed away, surrounded by her family.
Hannah perceived Sarah’s death as the inevitable result of disease progression and did not consider her own judgments or actions to have contributed to her death. However, Hannah felt that she had not been able to provide sufficient care and experienced feelings of remorse. Moreover, upon hearing the family’s grieving voices, she felt as though she were being blamed and was unable to face them, and these feelings remained with her for some time. In this case, the nurse experienced feelings of helplessness, regret, and remorse regarding the patient’s death. However, she recognized that the central element of guilt—responsibility for the patient’s death—did not lie with herself but rather with the misfortune of the disease.
Contrary cases
Jessica was the primary nurse caring for John, a 90-year-old patient. John often expressed, “I have enjoyed life enough; now I just want a peaceful end,” and Jessica provided daily care while respecting his wishes. Over the course of several months, John’s condition gradually declined, and he passed away quietly, as if falling asleep, surrounded by his family. After his death, John’s family expressed their gratitude to Jessica, saying, “Thanks to the excellent care you provided, we have no regrets. Thank you.” Jessica felt a deep sense of satisfaction, recognizing that her care had been sufficient for John and had enabled him to experience a peaceful and dignified end in accordance with his wishes.
Empirical referents
The guilt experienced by a nurse associated with a patient’s death is an emotional and subjective experience, making it difficult to capture directly through external observation. However, its presence can be inferred through nurses’ narratives and behaviors. For example, at the time of a patient’s death, nurses may perceive that their own actions or judgments, such as overlooking aspects of care 4 or insufficient observation, 14 contributed to the outcome. Nurses may also experience anxiety about being blamed by patients or their families 29 or interpret the patient’s death as a professional failure. 33 These experiences can serve as indicators that the nurse is experiencing guilt associated with a patient’s death and provide observable phenomena supporting the existence of this concept. At present, there is no specific scale or questionnaire designed to measure guilt in nurses associated with a patient’s death. However, it is expected that these narratives will serve as a foundation for the development of structured items for use in measurement tools.
Definition
Guilt experienced by nurses associated with a patient’s death is defined as an emotion that arises from specific clinical situations—including regrets regarding one’s own involvement, relationships with patients and their families, professional responsibility, ethical dilemmas, and the nature of death—and manifests centrally as regret, moral injury, fear of criticism, and self-recrimination for the patient’s death. This emotion exerts long-term effects on nurses, reflected in psychophysical impact, self-alienation, and changes in meaning-making through reflection.
Discussion
Characteristics of nurses’ guilt related to patient death
This concept analysis clarified the structure and definition of guilt experienced by nurses associated with a patient’s death. Generally, a nurse’s feeling of guilt is understood as an ethical experience arising from the conflict between the values of care and practical constraints, 41 and the findings of the present concept analysis largely align with this characterization. Therefore, the results of this analysis can be considered valid as a conceptual explanation of nurses’ guilt. At the same time, this concept exhibits unique features specific to the context of patient death, including excessive self-blame rooted in the inevitability of death and regret driven by professional responsibility, which act as central elements.
In terms of the conceptual structure, antecedents such as the nature of death, the relationship with the patient and the patient’s family, professional responsibility, ethical dilemmas, and regrets regarding one’s own involvement can increase nurses’ psychological vulnerability and form a cognitive-emotional basis that easily links patient death to self-blame. As a result, nurses tend to excessively reassess their judgment and care, with attributes such as self-blame, regret, moral injury, and fear of criticism mutually reinforcing one another. These attributes can lead to divergent consequences through reflection and meaning-making; for example, when deep reflection enables nurses to reinterpret the inevitability of death and the limits of care, it can contribute to the maturation of their professional perspective. In contrast, when self-denigrating interpretations become entrenched, guilt persists as a traumatic experience, potentially resulting in long-term psychophysical effects and self-alienation.
At the core of this process is excessive self-blame. This refers to a cognitive tendency to attribute events beyond one’s control to oneself, leading to the perception that one is responsible even when the patient’s death was inevitable. 35 Such excessive self-blame corresponds to the psychic structure of the depressive position in Klein’s object relations theory, 42 wherein guilt is experienced after perceiving a sense of insufficiency toward the object one seeks to protect. It also shares the characteristics described in Tellenbach’s concept of the melancholic-affective personality, which is marked by a strong sense of responsibility and duty, orderliness, excessive identification with social roles, and an intolerance of ambiguity, making individuals more likely to interpret outcomes as their own responsibility. 43 Furthermore, a survey of nurses working in general hospitals found that approximately 60% of the respondents exhibited depressive temperaments, 44 suggesting that such psychological predispositions may contribute to the intensification of self-blaming cognitions when confronting the inevitable death of patients.
Against this background, the conceptual distinction between guilt and moral distress warrants careful consideration. The sense of guilt addressed in this review is sometimes described in ways that resemble moral distress. However, when the characteristic features of moral distress identified in the literature are taken into account, it becomes clear that the two should not be treated within the same conceptual frame. Kim and Shelton position moral distress as a distinct type of moral emotion, separate from self-evaluative feelings such as guilt. 45 Furthermore, in Jameton’s original definition, moral distress arises “when one is unable to carry out what one believes to be the right action due to institutional constraints,” 23 thereby placing external circumstances or conditions that impede action at the center of the experience. Although nurses may sometimes use the term “guilt” when describing moral distress,23,46 Wilkinson notes that this reflects a manner of expressing distress rather than an indication that the underlying emotional qualities are the same. In addition, discussions of moral injury treat external conditions—such as moral betrayal by an authority figure and the presence of a highly threatening situation—as definitional requirements, 46 reinforcing that the surrounding environment is central to the experience.
Taken together, the above suggests that moral distress is best understood as distress that arises when external constraints prevent nurses from acting as they believe they should. In contrast, the guilt examined in this review does not necessarily depend on the presence or absence of such external constraints. Rather, it centers on the internal process through which nurses interpret and evaluate their own involvement in the face of a patient’s death. Even in situations where no institutional barriers were present, nurses may still experience thoughts such as “I could have done more” or “My judgment may have been wrong,” which clearly differentiates guilt from moral distress. Thus, although both experiences relate to situations in which nurses feel that they were unable to fully enact the care they considered desirable, moral distress focuses on experiences shaped by external conditions that hinder action, whereas guilt centers on the internal struggle of evaluating one’s own involvement. Recognizing this distinction is essential for understanding nurses’ emotional experiences following a patient’s death and supports the need to treat guilt as an independent concept.
Shame, on the other hand, arises from antecedents such as negative evaluation, the involvement of others, and social or group norms, and involves self-condemnation based on social evaluation or the gaze of others. 22 The present concept shares some aspects of shame, including the fear of blame, but its origin lies not in social evaluation but rather in self-blame stemming from the perceived shortcomings in one’s involvement and professional responsibility. In contrast, whereas shame represents outward-directed self-condemnation based on others or social norms, the present concept is characterized by inward-directed self-blame based on specific clinical situations and one’s own involvement. Nonetheless, both concepts share the potential to induce psychological harm and can, through reflection and meaning-making, lead to personal growth and positive change.
Implications for nursing practice
For nurses, witnessing the death of a patient accompanied by guilt represents an extreme situation in which life-and-death decisions 37 and ethical dilemmas 16 converge. At the same time, it is an unavoidable reality that nurses inevitably face in the pursuit of their professional mission, representing a profoundly significant form of occupational distress. This concept analysis has visualized an emotion that was previously considered ambiguous and difficult to grasp. Such visualization clarifies which aspects of guilt intensify psychological burden and where intervention is needed, thereby contributing to the early identification of support needs and the specification of appropriate intervention points. In turn, it holds substantial value for clinical practice by informing the design of appropriate psychological and educational support and by promoting self-understanding in nurses.
The regret that remains in the minds of nurses confronting a patient’s death, accompanied by guilt, may at first appear as a negative ruminative thought. However, the guilt experienced by nurses can lead to a range of subsequent psychological outcomes, depending on the process of reflection and meaning-making. 35 When adequate support and reflective environments are provided, and nurses are able to reconstruct the meaning of their role, accept their limitations, and come to terms with the uncontrollable reality of death, this can lead to the maturation of their nursing perspective and post-traumatic growth.47,48 However, if negative interpretations become entrenched, guilt can persist as a psyche-eroding trauma 16 or as self-sacrificial thinking, 28 potentially prolonging psychological burden.
Therefore, the guilt that nurses experience after a patient’s death should not be dismissed as a mere stress reaction or a purely personal emotion but rather understood as an experience closely tied to how they reflect on their clinical judgments and involvement. Feelings of “I could have done more” have been noted to influence not only technical skills but also non-technical aspects of practice, such as communication with patients and their families. 27 In light of the possibility that such doubts may affect multiple dimensions of practice, nurses who are prone to experiencing guilt after a patient’s death may benefit not only from psychological support but also from opportunities to articulate and share their experiences as well as educational opportunities that facilitate reflection. 49 Making nurses’ experiences of guilt visible in this way provides a theoretical foundation for considering potential directions for such support and demonstrates the conceptual utility of examining guilt in this context.
Conclusion
This concept analysis clarified the structure and definition of nurses’ guilt associated with a patient’s death. The concept comprises four attributes. The first, “Feeling responsible for the patient’s death,” refers to the perception that one’s actions caused the patient’s death; the second, “Fear of condemnation,” refers to the perception of being criticized by the patient or the patient’s family; the third, “Regret,” encompasses feelings of inadequate care and remorse toward the patient’s family; and the fourth, “Self-denial,” includes perceiving the patient’s death as a professional failure and feeling unable to forgive oneself. Additionally, five antecedents and three consequences were identified.
Previous studies have explained nurses’ guilt as an ethical experience arising from the conflict between values of care and practical constraints. The present concept aligns with this understanding, supporting its theoretical validity. It furthermore highlights the distinct features of guilt in the context of patient death, where excessive self-blame and role-based regret play a central role due to the inevitability of death. At the core lies excessive self-blame, which, when combined with clinical-specific professional mission, relational factors, and ethical dilemmas, forms the basis of guilt.
Although the concept partially overlaps with related concepts such as moral distress and shame, it is distinct in that it primarily represents an inward-directed guilt rooted in clinical care and self-evaluation. By conceptualizing nurses’ guilt in this way, the previously ambiguous and elusive structure of this emotion becomes visible, enabling a clearer understanding of which aspects intensify psychological burden and where intervention is needed. This, in turn, suggests the potential for early identification of support needs in clinical settings, which could inform the design of appropriate psychological and educational support and clarify points for intervention.
The concept demonstrates the potential for guilt to evolve into growth through reflection, underscoring the importance of providing support that enables nurses to achieve positive psychological change following challenging experiences. Overall, this concept provides a foundational framework for understanding nurses’ experiences more deeply and for implementing appropriate supportive interventions.
Study limitations
This concept analysis has several limitations. First, the analysis may be susceptible to selection bias, extraction bias, and analytical bias. Second, Walker and Avant’s concept analysis method does not provide specific criteria for evaluating the quality of the included literature, which might have affected the reliability of the results. Despite these limitations, it is considered that a clinically applicable conceptual model of nurses’ guilt related to patient death was successfully extracted.
Supplemental material
Supplemental material - Nurses’ guilt regarding patient deaths: A concept analysis
Supplemental material for Nurses’ guilt regarding patient deaths: A concept analysis by Kaede Fujimura, Koji Tanaka, Yoko Takeuchi, and Kyoko Nagata in Nursing Ethics
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of AI and AI-assisted technologies in the writing process
The authors used ChatGPT to translate the original draft from Japanese to English and to proofread the translation. The final manuscript was thoroughly reviewed and approved by all authors.
Supplemental material
Supplemental material is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.