
Abstract
The purpose of this study was to investigate the evaluation of end-of-life care from bereaved family of cancer patients who had died in intensive care units in Japan. Cross-sectional anonymous questionnaire surveys were conducted on community dwelling individuals aged 40-79 who were randomly sampled from census tracts. End-of-life care was assessed using the Good Death Inventory and Care Evaluation Scale. The respondents were 4011 bereaved family and response rate was 40%. Of 390 respondents had experienced bereavement in intensive care unit. Of 152 respondents had lost a loved one due to cancer. The result showed that bereaved family of cancer patients evaluated lower than the non-cancer patients for “The doctors dealt promptly with discomforting symptoms of the patients’ (p=0.009), ‘The nurses had adequate knowledge and skills’ (p=0.016), ‘Admission (use) was possible when necessary without waiting' (p=0.008) , Consideration was given to the health of the family (P=0.039) and Physical and psychological comfort (p=0.03). Overall, it can be presumed that the cancer patients' bereaved family evaluated about symptoms management and doctors and nurses skills was low. There is a need to improve for end-of-life care of cancer patients and to conduct further research to explore quality-improvement interventions to bereaved family of cancer in intensive care unit.
Introduction
In Japan, most patients with cancer die in the hospital. The quality of care provided to end-of-life cancer patients in general hospitals is thus important. 1 Some studies evaluating end-of-life care have been conducted in Japan. Hirai et al have conducted qualitative interviews with patients with cancer, their families, physician, and nurses to assess the structure of a “good death.” 2 Miyashita et al have developed measures to evaluate end-of-life cancer from the perspective of bereaved family members. 3 In addition, Miyashita et al have conducted surveys on the quality of hospice and palliative care units (PCUs). 4 Sato et al reported on the quality of end-of-life treatment for patients with cancer by conducting a retrospective medical chart review. 5,6 A growing number of studies are evaluating a “good death” and the quality of end-of-life care. In Japan, however, most studies have been conducted in PCUs and general wards. Few surveys have attempted to evaluate patients in the intensive care unit (ICU). Although many researchers have maintained continuous interest in the evaluation of the bereaved family perspective regarding end-of-life care, little investigation has been described to actually explore those evaluations in Japan. Improving the quality of end-of-life care in the ICU is an important endeavor. Given the severity of the illness, death is common in the ICU setting. 7 However, several studies have reported that many nurses working in ICUs face barriers and difficulties in providing end-of-life care for patients. 8,9 Some data suggest that the quality of end-of-life care in the ICU is often poor. 7,10 In the United States, Curtis et al developed an instrument for assessing the bereaved family members of patients in ICUs, known as the Quality of Dying and Death (QODD) scale. 11 Several studies have used the QODD in the ICU to measure the quality of the dying experience of the patient as perceived by family members, nurses, residents, and physicians, in addition to using the medical record. 12 –15 However, few studies have examined the end-of-life care of patients with cancer in the ICU. According to a large European study, patients with cancer were more often admitted to the ICU for sepsis and respiratory complications than other ICU patients. 16 In Japan, Kawasaki and Abe reported on factors predicting ICU mortality and post-ICU survival among critically ill patients with cancer admitted to the ICU. 17 Some patients with cancer also die in the ICU. Therefore, to advance the goal of improving the quality of care provided to patients with cancer who die in the ICU, understanding the quality of the dying experience is important.
The primary objective of this study was to investigate the evaluation of end-of-life care by bereaved family members in the ICU. The secondary objective was to assess the quality of end-of-life care for dying patients with cancer in the ICU.
Methods
Participants and Procedure
All participants were community-dwelling individuals aged between 40 and 79 years who had experienced bereavement within the past 10 years. A cross-sectional anonymous questionnaire was mailed to a sample of the general Japanese population. We identified 4 target areas (Tokyo, the capital city; Miyagi prefecture, in eastern Japan; Shizuoka prefecture, in central Japan; and Hiroshima, in western Japan) in order to obtain a wide geographic distribution for the nationwide sample. The 4 areas included an urban preference (Tokyo) and mixed urban/rural areas (Miyagi, Shizuoka, and Hiroshima). We initially identified 5000 participants using a stratified 2-stage random sampling of residents from the 4 areas. We randomly selected 50 census tracts in each area and then selected 25 individuals within each census tract, thus identifying 1250 individuals for each area. Questionnaires were mailed to these potential participants and a reminder postcard was mailed 2 weeks later. The survey was conducted twice, in 2009 and 2010. The protocol of the first study was approved by the institutional review board of the University of Tokyo. The second study was approved by the institutional review board of the University of Tohoku.
Measurements
Care Evaluation Scale (CES), short version. 18
The questionnaire was designed so that the respondent evaluated the structure and process of end-of-life care by rating the necessity of improvement for each item on a 6-point Likert-type scale (from 1 = improvement is highly necessary to 6 = improvement is not necessary).
Good Death Inventory (GDI). 3
The questionnaire was designed so that the respondent evaluated the outcome for end-of-life care using a 7-point Likert-type scale (from 1 = absolutely disagree to 7 = absolutely agree).
Participant characteristics
The demographic background of respondents (age and sex) was determined as the time since the most recent bereavement, relationship with the deceased, cause and place of death of the deceased, whether the death was expected or unexpected, and number of days in which the respondent spent time with the deceased during the last week of life.
Analysis
The χ2 test was used to compare a number of demographic characteristics. We made comparisons between the bereaved family members of patients with cancer and those of patients with no cancer for CES and GDI using Mann-Whitney U test. Statistical significance was set at P < .05 level (2-tailed). All analyses were performed using SPSS version 15.0 statistical software (IBM, SPSS).
Results
Participant Characteristics
Of the 10 000 questionnaires sent to a sample of the general population, 4011 were returned (response rate, 40%). Of these, 2321 respondents had experienced bereavement within the previous 10 years. Of those, 1591 respondents had experienced bereavement involving a patient in a general hospital. A total of 390 respondents had experienced bereavement involving a patient in an ICU (including ICU, coronary care unit, and high-care unit). Three respondents were excluded because of missing data regarding the cause of death. Finally, 387 bereaved family members of patients who had died in the ICU were analyzed. Demographic data for the sample are shown in Table 1.
Demographics of Respondents.a
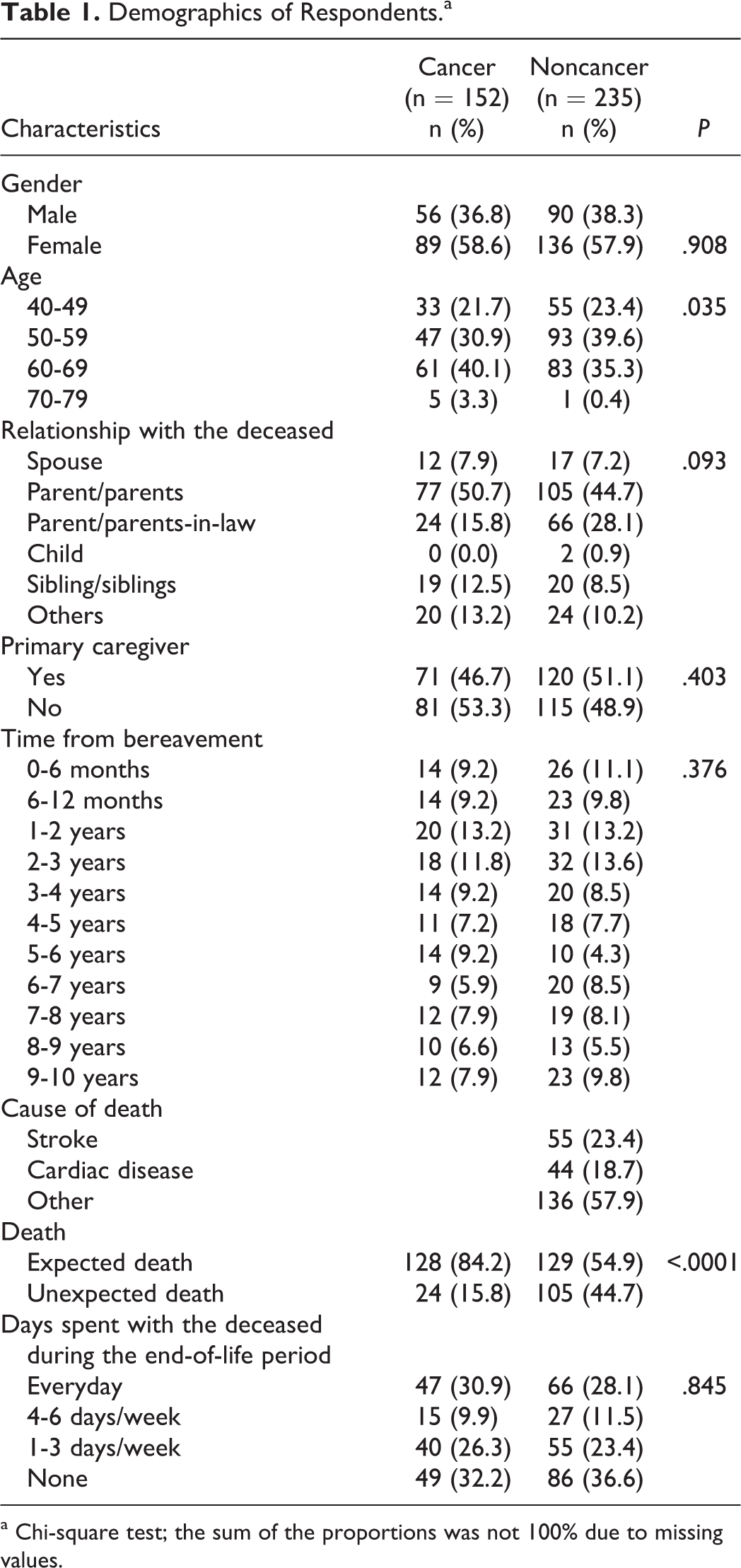
a Chi-square test; the sum of the proportions was not 100% due to missing values.
Using χ2 test, significant differences between bereaved family members of patients who died due to cancer and those of patients without cancer were seen for “whether the death was expected or unexpected” (P < .0001).
Care Evaluation Scale
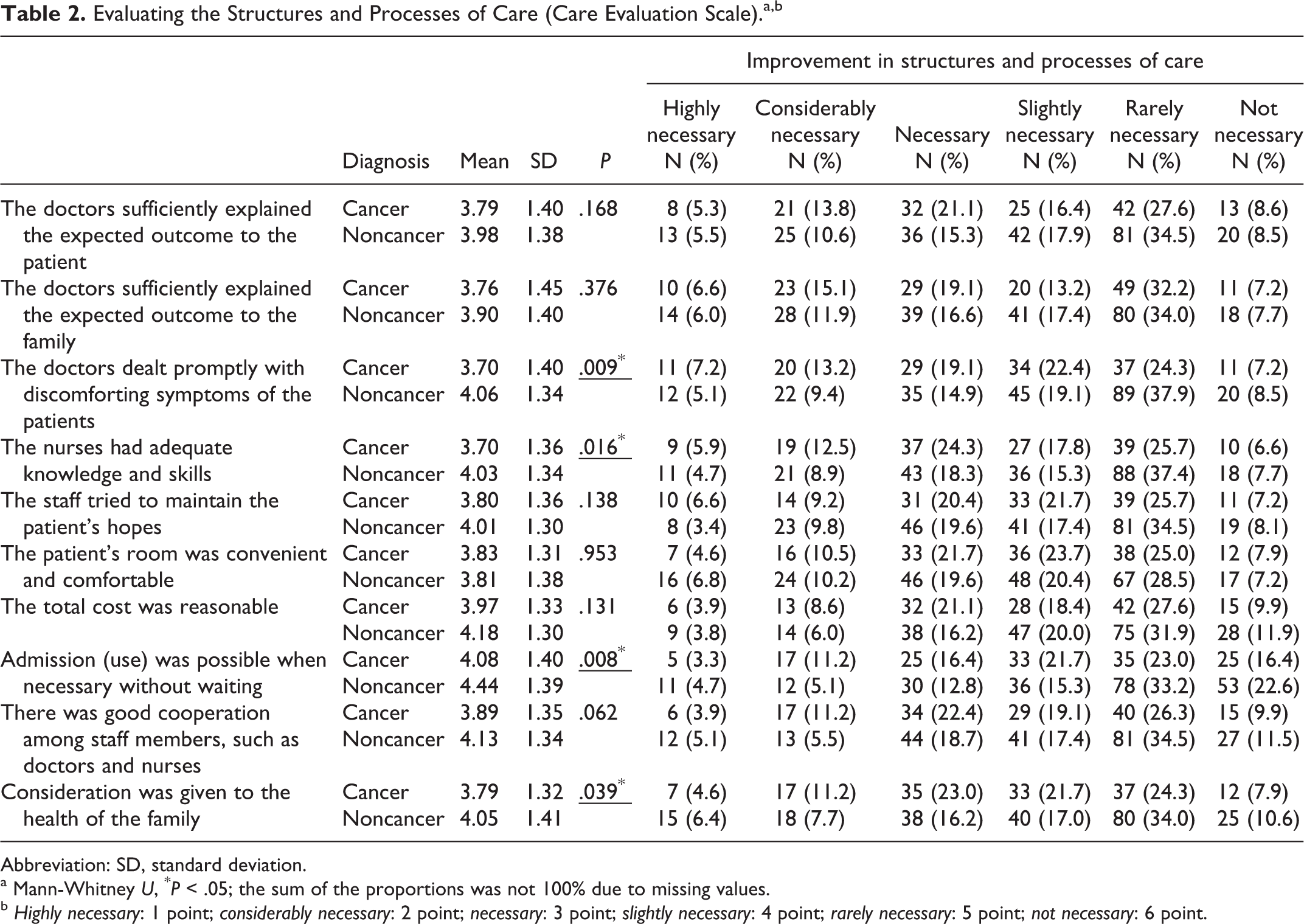
Table 2 shows the mean values and response rates for each item in the CES. Significant differences were found in the scores of 4 items between bereaved family members of patients with cancer and noncancer patients: “Doctors dealt promptly with patient discomfort” (P = .009), “Nurses had adequate knowledge and skills” (P = .016), “Admission (use) was possible when necessary without waiting” (P = .008), and “Consideration was given to the well-being of the family” (P = .039). Bereaved family members of patients with cancer patients perceived the necessity for improvements in some items more than those of non-cancer patients. Moreover, only 32% of bereaved family members of patients with cancer patients rated “Doctors dealt promptly with patient discomfort” or “Nurses had adequate knowledge and skills” as “improvement is rarely necessary” or “improvement is not necessary.”.
Evaluating the Structures and Processes of Care (Care Evaluation Scale).a,b
Abbreviation: SD, standard deviation.
a Mann-Whitney U, * P < .05; the sum of the proportions was not 100% due to missing values.
b Highly necessary: 1 point; considerably necessary: 2 point; necessary: 3 point; slightly necessary: 4 point; rarely necessary: 5 point; not necessary: 6 point.
Good Death Inventory
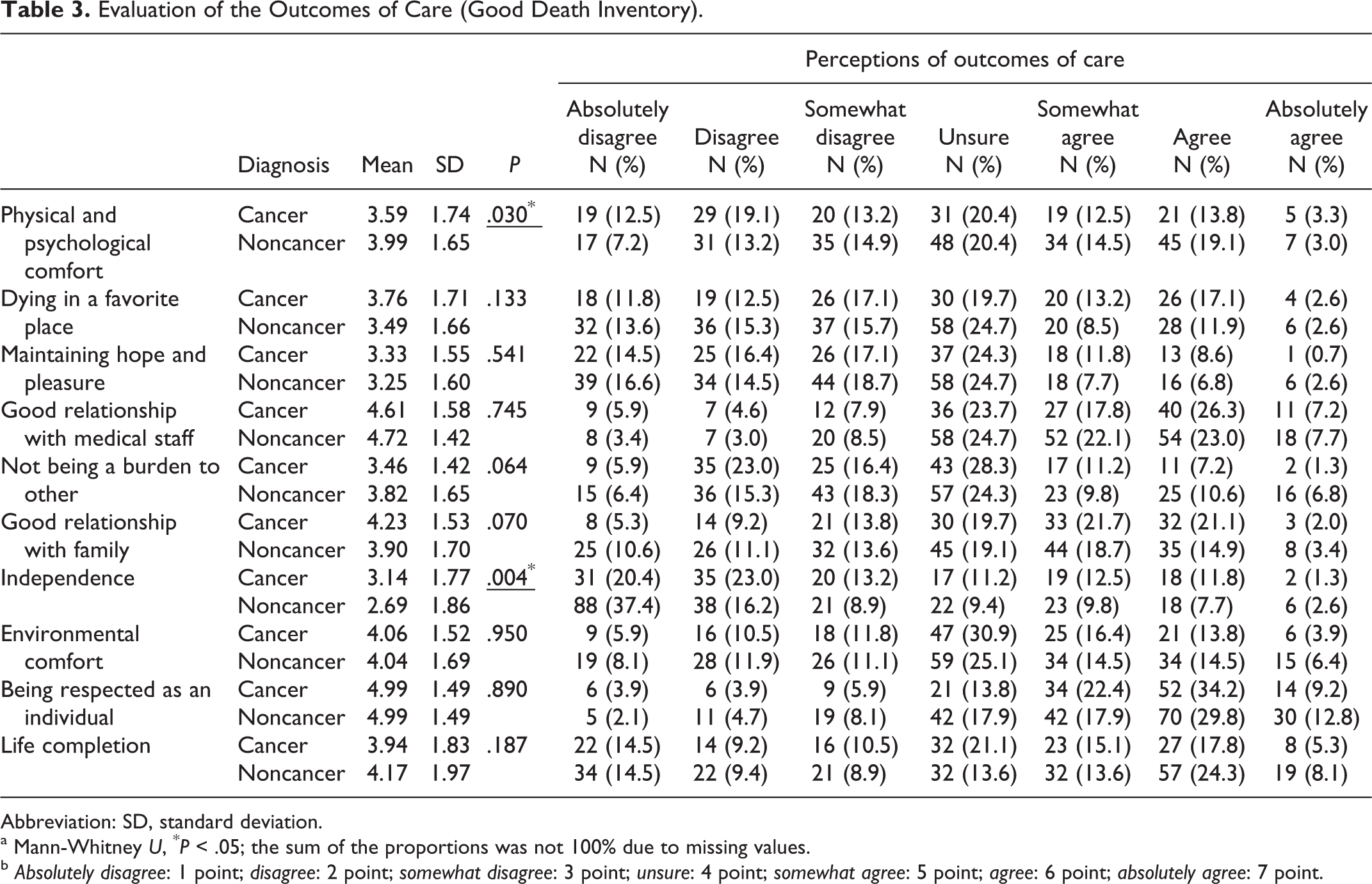
Table 3 shows the mean values and response rates for each item in the GDI. Bereaved family members of patients with cancer provided low evaluations for “physical and psychological comfort” (P = .030) compared with those of noncancer patients. Conversely, bereaved family members of patients with cancer provided high evaluations for “independence” (P = .004). “Being respected as an individual” was rated agree or absolutely agree by 43% of bereaved family members for both cancer and noncancer patients. However, only 10% to 13% of the family members rated agree or absolutely agree for “independence.”
Evaluation of the Outcomes of Care (Good Death Inventory).
Abbreviation: SD, standard deviation.
a Mann-Whitney U, * P < .05; the sum of the proportions was not 100% due to missing values.
b Absolutely disagree: 1 point; disagree: 2 point; somewhat disagree: 3 point; unsure: 4 point; somewhat agree: 5 point; agree: 6 point; absolutely agree: 7 point.
Discussion
Our findings suggest that family members with a loved one dying in the ICU report less positive evaluations of end-of-life care than family members with a loved one dying in the PCU, in Japan. 1 In addition, the present results suggest that bereaved family members of patients with cancer provided lower evaluations of end-of-life care than bereaved family members of noncancer patients. In particular, evaluations by bereaved family members of patients with cancer focused on symptom management and the skill levels of doctors and nurses. Results in the present study are consistent with the findings of relevant studies investigating bereaved family perspectives on end-of-life care. 10,19 Moreover, the results imply that doctors and nurses have insufficient knowledge and skill regarding the care of patients with terminal cancer, as ICUs are designed to maintain life with a primary emphasis on recovery or cure. In other words, patients with terminal cancer, as a rule, are not admitted to ICUs. Another potential explanation for these findings is that bereaved family members of patients with cancer provided high evaluations for “independence” in the GDI compared with those of noncancer patients. Patients with cancer may thus have a higher consciousness level than noncancer patients at the end of life. According to research results from Japan, 20 most patients who die in the ICU are already unconscious. Noncancer patients may thus be likely to show little expression of physical symptoms.
Ringdal et al have reported that satisfaction of bereaved family members with the pain relief and assessment of patient symptoms was significantly higher among the respondents in an intervention group than in the control group after intervention with a comprehensive palliative care program. 21 In the ICU setting, a study from France showed the effects of a proactive communication strategy that comprised an end-of-life family conference conducted according to the specific guidelines and that concluded with the provision of a brochure. This intervention resulted in a decrease in posttraumatic stress disorder–related symptoms and symptoms of anxiety and depression among family members by 3 months after the patient’s death. 22 In the United States, Curtis et al performed a quality-improvement intervention consisting of clinician education, local champions, academic detailing, feedback to clinicians, and implementation of a system support. The results showed no significant improvement in family assessments of the quality of dying or satisfaction with care but significant improvements in nurse-assessed quality of dying and reductions in ICU stay, with an intervention to integrate palliative care in the ICU. 14 In Japan, however, no studies have tried to investigate the effects of quality-improvement interventions in the ICU. Further research is needed to explore the relationship between interventions involving the family and outcomes in Japan.
Our results show that the ratio of patients with cancer was higher than we assumed. In the United States, emergency room (ER) visits or use of the ICU and aggressive treatment in the end-of-life setting was identified as poor quality indicators (QIs). 23,24 In Japan, however, most bereaved family members did not consider ER visits or use of the ICU as poor QIs in end-of-life cancer care. 25 The ability to make use of the ER or ICU is presumably important to family members when a loved one is in a serious condition. It is implied that family members consider that good care is received by patients undergoing aggressive treatment. According to our results, compared with bereaved family members of noncancer patients, many bereaved family members of patients with cancer expected death. The family members of patients with cancer may thus hope for high-quality end-of-life care. However, the ICU is oriented toward saving lives and not toward helping patients die. The ICU nurses may find it difficult to care for dying cancer patients. There is a need to improve end-of-life care for patients with cancer and to conduct further research to explore quality-improving interventions for bereaved family members of cancer patients in the ICU.
Limitations of this study include the small sample size and low response rate, although the rate was considered acceptable for a mail-based survey conducted on the general population. Further studies with larger sample sizes are needed. Second, the reliability of the data was compromised because the questionnaires were totally self-administered by participants. Despite these limitations, the present study represents the first nationwide survey to explore the perceptions of bereaved family members regarding end-of-life care in Japanese ICUs. The resulting data not only contribute to research into end-of-life care in ICUs but also to research into improving care for family members of patients in ICUs in Japan
Conclusion
We investigated the evaluation of end-of-life care by bereaved family members and assessed the quality of end-of-life care for dying cancer patients in ICUs in Japan. The results implied that doctors and nurses have insufficient knowledge and skills for care of terminal cancer patients. Further research is needed to explore the quality-improving interventions for bereaved family members of cancer patients in the ICU.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: supported by the Grant-in-Aid for Cancer Research endowed to MM from the Ministry of Health, Labor and Welfare, Japan (MHLW).