
Abstract
This paper examines how sustained armed conflict operates as a primary occupational hazard that produces moral injury among nurses. It moves beyond burnout and moral distress frameworks to propose a justice-centered approach to nurse well-being in conflict settings. This discursive paper employs a critical interpretive synthesis (CIS) of peer-reviewed studies and humanitarian reports from 2020 to 2024, comparing documented conditions in Gaza with prevailing nursing well-being models. Sixty-eight sources were analyzed through iterative comparison of situational evidence and conceptual scholarship. Gaza served as a critical case to test the explanatory limits of dominant frameworks. Three systemic hazards shape nursing practice in Gaza: severe resource deprivation, direct violence against healthcare workers and facilities, and the collapse of health and civic infrastructure. Under these conditions, moral injury emerges as the dominant occupational harm. Nurses are compelled by external political and military forces to act in ways that violate core professional duties. Resilience and coping approaches fail where harm originates outside healthcare systems and where internal reform is not possible. In settings where healthcare is systematically targeted, political violence becomes a primary occupational hazard. A justice-centered framework is required, centered on protection of healthcare under international humanitarian law, accountability for violations, and global professional solidarity as core elements of nurse well-being. Occupational health becomes inseparable from protection, accountability, and justice. Models that assume stable healthcare systems cannot explain nurse suffering in conflict zones. Nursing policy and practice must expand occupational health frameworks to address structural and political conditions. Practical responses include protection mechanisms, documentation of violations, and evacuation pathways for healthcare workers under attack.
Introduction
The limits of conventional frameworks
Nurses worldwide report psychological strain linked to workload, staffing shortages, and ethical tension.1,2 In response, the profession has developed robust frameworks to explain and address occupational harm. Burnout theory describes emotional exhaustion, depersonalization, and reduced personal accomplishment arising from chronic workplace stress. 2 Moral distress captures the anguish nurses experience when constrained from acting according to their ethical judgments, typically by institutional hierarchies or resource limitations.3,4 More recently, resilience has emerged as both an explanatory concept and a policy goal, emphasizing individual and collective capacity to adapt to adversity.5,6
Policy and organizational responses informed by these frameworks often focus on resilience training, wellness programs, staffing improvements, and internal reforms.1,7 These approaches share a common assumption: that the healthcare system, although stressed, remains fundamentally functional and that occupational risk can be managed within institutional boundaries through organizational intervention and individual adaptation. This assumption does not hold in settings of sustained armed conflict. In such contexts, political and military actions systematically dismantle the material and ethical foundations required for safe nursing practice.
Hospitals operate without reliable electricity, water, medical supplies, or physical protection. Throughout this manuscript, the term systematic refers to recurrent and patterned conditions affecting healthcare delivery rather than isolated events; targeted denotes actions directed toward healthcare personnel, infrastructure, or functions recognized under international humanitarian law as protected entities; and deliberate refers to actions documented by authoritative sources as intentional or foreseeable despite known humanitarian consequences. Staff work under direct threat of attack, forced displacement, and detention.8–10
Gaza as a critical case
Using Gaza as a critical case, this paper examines the limits of dominant nursing well-being frameworks when applied to settings of systematic healthcare destruction. The aim is not to present Gaza as exceptional or to suggest that nurse suffering there is unique in kind. Rather, Gaza is employed as a strategic methodological site (a critical case in the sense articulated by Flyvbjerg 11 ) where the extremity of conditions allows us to test whether prevailing concepts adequately explain nurse suffering where healthcare systems are systematically degraded by political-military violence. A critical case functions as a theoretical probe. If dominant models of burnout, moral distress, and resilience fail to adequately explain nurse suffering in Gaza’s extreme conditions, their claimed universal applicability is called into question, revealing the need for new conceptual tools. Conversely, if these frameworks prove sufficient even in Gaza, their theoretical robustness is strengthened. This methodological logic moves the analysis beyond a descriptive case study toward a discursive engagement with nursing theory itself.
Importantly, Gaza is not isolated in experiencing healthcare system collapse under conflict. Similar patterns have been documented in Syria, Yemen, Sudan, and Ukraine, where healthcare has been systematically targeted through attacks on facilities, detention of providers, and deliberate resource deprivation. 12 These conflicts share three common features: sustained military operations in civilian areas, direct targeting of healthcare infrastructure, and breakdown of governance structures that protect medical neutrality. Gaza therefore serves not as an anomaly but as a particularly visible and well-documented example of a broader phenomenon observable across contemporary armed conflicts, contexts where healthcare ceases to function as a protected space and becomes instead a site of danger, deprivation, and ethical impossibility.
Purpose and structure
Through a discursive analysis of competing frameworks against documented realities in Gaza, this paper argues that a fundamental reconceptualization is required. We contend that in these conditions, political violence constitutes a primary occupational hazard and that the resulting dominant harm is best understood as moral injury, a concept that, unlike burnout or moral distress, centers the role of external transgression in producing nurse suffering. The paper proceeds as follows: ‘Methodological approach: Critical interpretive synthesis' section outlines the methodological approach, explaining the principles of critical interpretive synthesis and the strategic use of Gaza as a critical case. ‘The conflict workplace: Three systemic hazards in Gaza' section presents three systemic hazards that reshape the nursing workplace in Gaza. ‘Testing dominant frameworks: Burnout, moral distress, and resilience' section examines how dominant frameworks of burnout, moral distress, and resilience explain (or fail to explain) nurse suffering under these conditions. ‘Moral injury: A reframing' section introduces moral injury as an alternative conceptual framework, including a comparative framework to distinguish it from moral distress. ‘Toward a justice-centered framework' section proposes a justice-centered approach to nurse well-being in conflict settings. ‘Discussion' section offers concluding reflections on the implications for nursing theory, practice, and policy. This reframes occupational health as inseparable from questions of protection, accountability, and justice in conflict settings, not as peripheral political concerns, but as central professional imperatives.
Methodological approach: Critical interpretive synthesis
What is critical interpretive synthesis?
This paper employs a critical interpretive synthesis (CIS), a form of integrative review designed to develop conceptual models through the interpretive analysis of diverse literature. 13 This approach aligns with a qualitative research design philosophy that prioritizes deep engagement with complex, contextualized phenomena to generate new understanding. 14 Unlike systematic reviews that aggregate findings from methodologically similar studies, CIS is suited to interdisciplinary questions where empirical data is embedded in complex, real-world contexts and where the goal is theoretical critique and development rather than empirical generalization. CIS involves three key processes: (1) reciprocal translation, where concepts and findings from different sources are compared and integrated; (2) refutational synthesis, where contradictions and gaps between frameworks are identified; and (3) lines-of-argument synthesis, where a new interpretive framework emerges from critical engagement with these comparisons. 13 This approach is particularly valuable when examining phenomena that cross disciplinary boundaries, such as the intersection of political violence, occupational health, and nursing ethics, and when established frameworks may prove inadequate to explain empirical realities. The method acknowledges that theory and evidence exist in dynamic relationship: empirical observations can challenge theoretical assumptions, while theoretical frameworks shape what counts as relevant evidence. In this synthesis, humanitarian reports documenting conditions in Gaza provide empirical grounding, while scholarly literature on burnout, moral distress, resilience, and moral injury provides competing conceptual lenses. The discursive task is to bring these into productive tension.
Search and selection process
Sources were identified through systematic searches of academic databases (PubMed, CINAHL, PsycINFO) and grey literature repositories of key humanitarian organizations (UN OCHA, WHO, ICRC, MSF, Amnesty International, Human Rights Watch) covering the period from January 2020 to April 2024. No language restrictions were applied during the search; however, only English-language sources were ultimately included due to translation resource limitations. This timeframe captures both pre-existing structural constraints on Gaza’s health system and the intensification of conditions following October 2023. Search terms included: nursing in conflict, healthcare workers AND armed conflict, moral injury, moral distress AND nurses, burnout AND nurses, resilience AND nursing, healthcare under siege, Gaza AND health, attacks on healthcare, occupational hazard AND conflict, structural violence AND health, international humanitarian law AND healthcare. Boolean operators and truncation were used to capture variations.
Figure 1 presents a flow diagram of the search, screening, and selection process. The initial search yielded 200 items. Titles and abstracts were screened for relevance before full-text review. Inclusion criteria prioritized: (1) Humanitarian reports (2020–2024): Recent documentation from major humanitarian organizations (UN agencies, ICRC, MSF) providing situational evidence of conditions in Gaza, with particular attention to reports describing healthcare infrastructure, resource availability, attacks on facilities, and constraints on medical practice. (2) Peer-reviewed conceptual articles: Scholarly literature conceptually addressing moral injury, structural violence, nursing ethics in extreme settings, and frameworks of burnout, moral distress, and resilience. Priority was given to recent reviews and foundational texts that have shaped nursing policy. (3) Foundational texts: Seminal works defining key concepts (e.g., Jameton’s original formulation of moral distress, Litz et al.’s conceptualization of moral injury, Maslach’s burnout inventory, Farmer’s structural violence framework). PRISMA-style flow diagram illustrating the identification, screening, and inclusion of sources for the critical interpretive synthesis. Initial search yielded 200 items; 112 excluded after title and abstract screening; 20 excluded after full-text review; 68 sources included in final synthesis (29 peer-reviewed academic sources and 39 humanitarian or international health agency reports).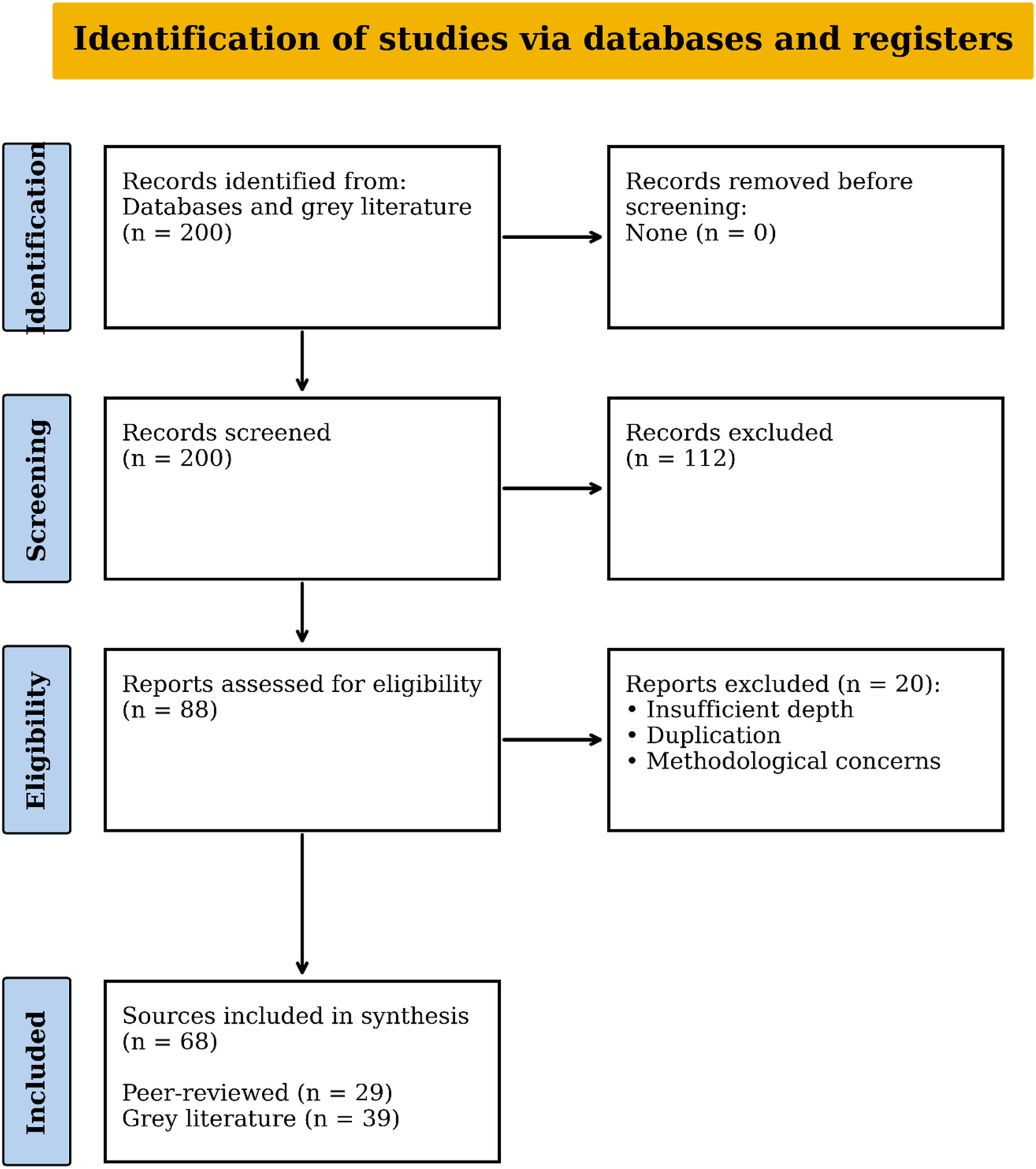
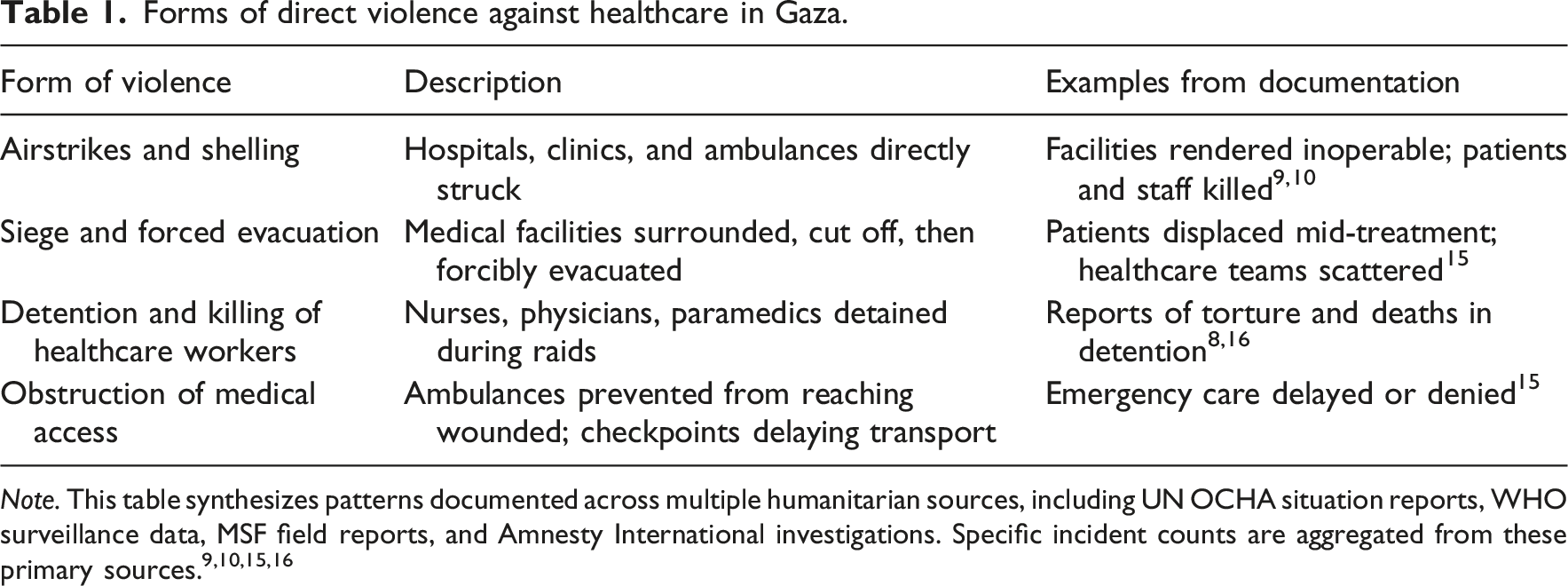
Forms of direct violence against healthcare in Gaza.
Analytic process: Iterative comparison and interpretive critique
The synthesis followed an iterative process of reciprocal translation and interpretive critique, as described by Dixon-Woods et al. 13 The analysis proceeded in three phases. Phase 1: Coding of Humanitarian Reports. Reports from UN agencies, ICRC, MSF, and human rights organizations were systematically coded for recurring descriptions of: constraints on clinical care (medication shortages, equipment failures, inability to perform standard procedures); threats to physical safety (attacks on facilities, injuries to staff, detention); ethical dilemmas (triage under scarcity, inability to provide standard of care); and descriptions of working conditions (infrastructure damage, displacement, psychological impacts reported by healthcare workers). This coding generated a detailed empirical picture of the conditions under which nursing is practiced in Gaza. Phase 2: Coding of Conceptual Literature. Scholarly nursing and occupational health literature was coded for how harm to nurses is conceptualized. This included: definitions of key concepts (burnout, moral distress, resilience, moral injury); identified sources of occupational stress; proposed mechanisms linking workplace conditions to psychological outcomes; and recommended interventions or policy responses. This coding illuminated the assumptions embedded in each framework about the nature of the workplace, the sources of harm, and the locus of intervention. Phase 3: Systematic Comparison and Interpretive Synthesis. The two bodies of evidence were systematically compared. For each documented condition in Gaza (e.g., repeated displacement of nurses from destroyed hospitals, inability to provide pain relief due to blockade-induced medication shortages, forced triage decisions with mass casualties), the following questions were asked: How would this situation be explained within a burnout framework? How would moral distress theory interpret this? What response would a resilience-focused approach recommend? Where do these frameworks converge or diverge? What aspects of the situation remain unexplained or inadequately addressed? Points of convergence and divergence were identified, and particular attention was given to situations described in reports that could not be adequately explained using existing concepts. Through this process, three recurring systemic hazards and the centrality of moral injury emerged as key interpretive themes. These findings were iteratively refined through repeated engagement with both bodies of literature, comparing theoretical predictions with empirical observations and refining interpretations.
Critical case justification and transferability
Gaza was selected as a critical case, 11 a strategic research site where theoretical limits can be rigorously tested. The logic of a critical case is not statistical generalizability but theoretical probing: if a theory fails to explain phenomena in a case specifically selected to challenge its assumptions, the theory’s claimed scope must be revised. Conversely, if the theory holds even in an extreme case, confidence in its robustness increases. Gaza meets the criteria for a critical case because: (1) Extremity: The intensity and duration of resource deprivation, infrastructural collapse, and direct violence against healthcare are among the most severe documented in contemporary conflict settings, making it a “most likely” case for theoretical breakdown. (2) Documentation: Despite access restrictions, the presence of long-standing humanitarian operations means Gaza’s healthcare conditions are among the best-documented conflict zones, reducing speculation and increasing empirical grounding. (3) Theoretical challenge: If frameworks designed to explain nurse suffering in resource-limited or ethically constrained settings cannot explain suffering in Gaza, this reveals conceptual limits rather than empirical peculiarity.
While Gaza functions here as a critical case, the analytical insights are not confined to this single setting. Similar patterns, combinations of resource deprivation, infrastructural destruction, and direct violence against healthcare, have been documented in Syria, Yemen, Sudan, and Ukraine.8,10,12 Comparative analysis reveals common features: civilian areas as theaters of sustained military operations, healthcare facilities explicitly targeted or rendered inoperable, governance collapse that erodes medical neutrality protections, and mass casualty events that overwhelm clinical capacity. These conflicts differ in their specific political contexts, geopolitical dynamics, and the nature of armed actors involved, but they share structural similarities in how violence reshapes healthcare into a site of danger and ethical impossibility. Thus, while Gaza serves as the primary empirical reference point, the conceptual argument has broader transferability. The proposed shift from individualized resilience frameworks to justice-centered models of occupational health is relevant in settings where healthcare workers face systematic, externally imposed political-military conditions that destroy the capacity for internal mitigation and render ethical practice structurally impossible. These conditions include sustained siege or blockade, repeated attacks on healthcare infrastructure, collapse of governance protections for medical neutrality, and the absence of meaningful institutional agency within healthcare systems themselves. The analysis therefore moves beyond case description to theoretical intervention with implications for nursing scholarship and policy across conflict-affected settings.
Reflexivity and positionality
This synthesis was conducted in the context of restricted access to Gaza and relies primarily on secondary documentation produced by international humanitarian organizations, UN agencies, and peer-reviewed scholarship. While these sources are widely recognized as authoritative in conflict health research, they inevitably represent mediated accounts rather than direct testimony from nurses currently practicing in Gaza.
In acknowledging the epistemic limits imposed by ongoing conflict, access restrictions, and risks to healthcare workers, we adopt a reflexive stance that makes our positionality as researchers explicit, a practice essential for rigor in qualitative and critical inquiry. 17 The authorship team brings disciplinary backgrounds in nursing ethics, health policy, occupational health, and international humanitarian law. This interdisciplinary composition shapes our interpretive lens, foregrounding attention to structural determinants of occupational harm and the legal frameworks governing healthcare in conflict. Our analysis is informed by prior engagement with nursing scholarship on moral distress and resilience, as well as familiarity with humanitarian documentation practices. This analysis therefore does not claim to represent the full diversity of nurses’ lived experiences but rather to engage critically with how dominant nursing frameworks align (or fail to align) with the best available documented evidence.
The interpretive stance adopted here is explicitly normative, grounded in nursing ethics and international humanitarian law. The analysis proceeds from the position that systematic violations of healthcare protection constitute not only humanitarian crises but professional and occupational safety failures requiring conceptual and policy response.
The conflict workplace: Three systemic hazards in Gaza
This section presents three interconnected systemic hazards that have transformed healthcare settings in Gaza from therapeutic spaces into sites of danger and ethical impossibility. These are not transient crisis conditions but sustained structural features of the environment in which nurses practice. Understanding these hazards is essential for assessing the adequacy of existing occupational health frameworks and for conceptualizing appropriate professional responses.
Resource deprivation: Scarcity as a weapon
Resource deprivation in Gaza extends beyond the shortages familiar in under-resourced health systems. It represents a deliberate, sustained restriction of medical supplies, electricity, water, and fuel imposed through military blockade and systematically intensified during armed conflict.9,10,15,18 Since 2007, Gaza has been under comprehensive land, sea, and air blockade, restricting the entry of medical equipment, medications, and essential supplies. 18 This baseline deprivation creates chronic scarcity: hospitals operate with expired medications, broken medical devices that cannot be repaired due to lack of spare parts, and supply chains so fragile that routine surgeries must be postponed. 10 Even before escalations of armed conflict, Gaza’s health system operated in a state of permanent shortage.
During intensified military operations, this chronic scarcity transforms into acute crisis. Humanitarian reports document sustained periods when hospitals function without electricity, relying on generators that fail when fuel supplies are blocked.9,15 Surgical units operate in darkness. Incubators for premature infants shut down. Refrigeration for medications and blood products fails. Water supplies become contaminated or inaccessible, creating infection risks in operating theaters and intensive care units. 10 Critically, scarcity is not random but targeted. Restrictions on “dual-use” items, materials claimed to have potential military application, have blocked medical imaging equipment, laboratory reagents, and even basic construction materials needed to repair damaged facilities.10,18 The cumulative effect is a healthcare system structurally prevented from meeting basic clinical standards.
The clinical consequences for nurses practicing under these conditions are profound and involve impossible decisions daily. Triage occurs not based on clinical need alone but on resource availability: pain medication is rationed even for trauma patients; antibiotics are withheld to preserve limited stocks; advanced procedures are denied not due to clinical contraindication but material impossibility. 9 These are not discretionary clinical judgments but forced choices imposed by blockade-induced scarcity. Humanitarian reports describe nurses manually ventilating patients when electricity fails, performing wound care without adequate supplies, and watching patients deteriorate from preventable complications because essential medications are unavailable.9,10 This is not the stress of heavy workload or time pressure familiar in under-resourced settings elsewhere. This is the experience of being systematically prevented from providing care that clinicians know how to deliver and ethically must deliver, a distinct form of occupational harm. The mechanism producing this deprivation is not healthcare system failure but political-military control over resource flows. Blockade policies determine what enters Gaza; military operations determine what reaches hospitals; administrative procedures determine processing times for humanitarian convoys. 15 Nurses experience scarcity not as an unfortunate circumstance but as an externally imposed constraint, a critical distinction for understanding the source of occupational harm.
Direct violence: Healthcare as target
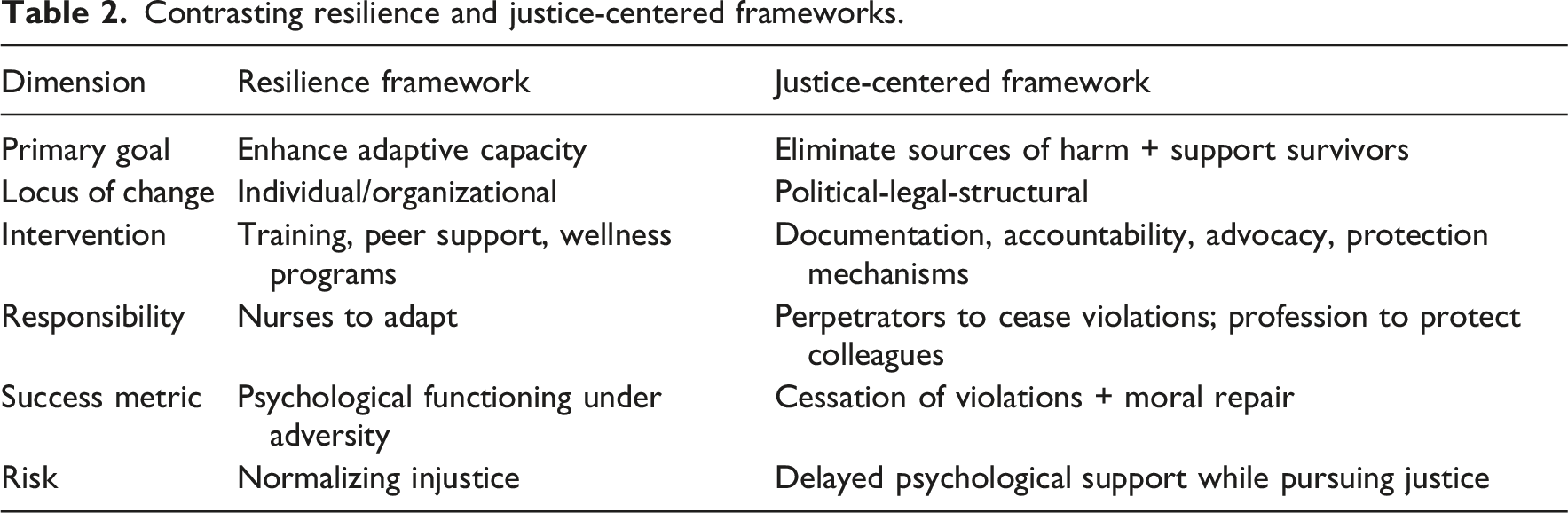
Contrasting resilience and justice-centered frameworks.
For nurses, direct violence transforms the workplace from a therapeutic environment into a combat zone. Humanitarian reports document nurses treating patients while under fire, evacuating intensive care units under military order with no safe destination, and witnessing colleagues killed while providing care. 9 The fundamental assumption of nursing practice, that the clinical environment is a protected space dedicated to healing, is systematically violated. The psychological impact extends beyond fear for personal safety, though that is significant. It includes the trauma of witnessing patients harmed in hospitals meant to protect them, the moral weight of continuing to work in facilities known to be targets, and the grief of losing colleagues killed while performing professional duties. 19 This is distinct from the occupational stress described in burnout literature; it is traumatic exposure to violence specifically targeting the healthcare role itself. These attacks constitute violations of core principles of IHL, including distinction (differentiating between combatants and civilians/protected persons), proportionality (limiting incidental harm), and precaution (taking measures to minimize civilian harm). 12 Under IHL, medical facilities lose their protected status only under specific conditions (active use for acts harmful to the enemy, after warning and reasonable time limit), none of which justify the systematic patterns documented in Gaza. 12 The significance for nursing is that direct violence against healthcare represents a collapse of international legal protections meant to enable medical practice in conflict. Nurses are not experiencing an unfortunate side effect of warfare but a fundamental breakdown in the legal and normative structures designed to protect medical neutrality. This is an occupational hazard created by political-military decisions to disregard international law.
Infrastructural collapse: The disintegration of the care environment
The third hazard is infrastructural collapse: the systematic destruction and deterioration of the physical, organizational, and social systems that make healthcare possible. This extends beyond individual facility damage to encompass collapse of water systems, sanitation, electricity grids, communication networks, supply chains, and governance structures.10,15 Repeated military operations have destroyed or severely damaged a majority of Gaza’s hospitals and clinics. 10 Even facilities not directly struck suffer cumulative damage from nearby explosions, loss of windows and roofs, structural instability, and equipment destruction from power surges when electricity is restored after outages. Water and sanitation systems fail, creating infectious disease risks within clinical settings. Roads are impassable, isolating facilities and preventing patient transport. 15
Healthcare depends on organizational systems: patient records, staff scheduling, supply chain management, referral networks, and quality assurance mechanisms. In Gaza, these systems have disintegrated. Repeated displacement scatters healthcare teams; patient records are lost when facilities are evacuated; continuity of care becomes impossible when patients are displaced to unknown locations; coordination between facilities breaks down when communication systems fail.9,15 The social fabric supporting healthcare also collapses. Families are separated, making patient follow-up impossible. Community health workers cannot access populations. Mental health services, already inadequate, become unreachable precisely when psychological trauma is most acute.10,20 Social determinants of health deteriorate catastrophically: malnutrition, homelessness, trauma, infectious disease, all increasing care needs while simultaneously making care delivery impossible.
Infrastructural collapse creates a situation where nursing practice becomes increasingly improvised, disconnected from standard protocols, and unsupported by the organizational structures that ordinarily guide clinical decision-making. Nurses work in makeshift facilities, without access to patient histories, unable to refer patients for specialized care that no longer exists, and unable to provide discharge planning because there is nowhere safe to discharge patients to. 9 This is distinct from the resource constraints familiar in low-income settings, where limited resources are managed within functioning systems. Here, the system itself has disintegrated. The organizational scaffolding that supports professional judgment, ensures accountability, enables continuity of care, and distributes responsibility across teams is absent. Nurses bear impossible burdens of decision-making in isolation, without the institutional supports that ordinarily make nursing practice possible.
Interconnection of hazards: A systemic pattern
These three hazards do not operate independently but interact and amplify each other. Resource deprivation intensifies when infrastructure is destroyed, preventing supply distribution even when humanitarian aid enters Gaza. Direct attacks cause infrastructural damage, which persists because repair is impossible under ongoing blockade. Infrastructural collapse increases vulnerability to further attacks by forcing healthcare to operate in exposed, makeshift settings. The cumulative effect is a healthcare environment characterized by sustained danger, material impossibility, and ethical compromise, conditions that constitute a distinct occupational context requiring conceptual frameworks adequate to this reality. The question, examined in the following section, is whether prevailing nursing frameworks of burnout, moral distress, and resilience adequately explain nurse suffering under these conditions.
Testing dominant frameworks: Burnout, moral distress, and resilience
Having established the empirical reality of the nursing workplace in Gaza, we now examine how dominant conceptual frameworks within nursing scholarship would explain nurse suffering under these conditions. This section applies each framework, burnout, moral distress, and resilience—to the documented hazards, identifying points where these theories provide explanatory power and where significant gaps emerge.
Burnout: Explaining chronic workplace stress
Burnout, as conceptualized by Maslach and colleagues, is a syndrome of emotional exhaustion, depersonalization, and reduced personal accomplishment resulting from chronic interpersonal stressors at work. 2 The framework identifies six sources of burnout: workload, control, reward, community, fairness, and values. 2 Interventions target organizational factors (improving staffing ratios, reducing time pressure) and individual factors (stress management, self-care, professional development). Burnout theory readily explains aspects of nurse suffering in Gaza. Humanitarian reports document extreme workload, nurses managing mass casualties far exceeding standard patient ratios, working extended shifts without relief, and experiencing physical and emotional exhaustion. 9 Loss of control is evident: nurses cannot influence resource availability, cannot ensure patient safety, and cannot control when their workplace will be attacked or evacuated. The community dimension is disrupted by displacement and loss of colleagues. Reward structures collapse when professional achievements (patient recovery, quality care) become unattainable. Burnout theory predicts that such conditions produce emotional exhaustion and depersonalization, and indeed, humanitarian accounts describe nurses reporting numbness, detachment, and overwhelming fatigue. 19 From this perspective, burnout provides a partial explanation for nurse suffering in Gaza.
However, significant aspects of the Gaza situation exceed burnout’s explanatory scope. First, burnout theory locates stress within the employment relationship and organizational environment. It assumes that occupational stressors originate from workplace management, staffing decisions, and organizational culture. In Gaza, primary stressors originate entirely outside the healthcare organization, from military operations, blockade policies, and political decisions. The hospital administration is not causing the harm; it is equally subject to external constraints. Burnout theory lacks concepts to address occupational harm imposed by external political-military actors. Second, burnout theory assumes healthcare organizations have agency to modify working conditions. Recommended interventions (improving staffing, reducing time pressure, and enhancing control) assume organizational capacity to implement change. In Gaza, no internal organizational reform can address blocked medical supplies, electricity failures caused by fuel restrictions, or attacks on facilities. The capacity for internal mitigation that burnout theory assumes is systematically destroyed. Third, burnout describes a gradual erosion of energy and engagement. The harm documented in Gaza includes acute trauma (witnessing colleagues killed, treating patients injured in attacks on the hospital itself, and evacuating under military threat). Burnout’s chronic stress model does not capture traumatic exposure to violence directed at the healthcare role. Fourth, burnout interventions target individual coping (stress management) and organizational reform (staffing, scheduling). Neither addresses blockade policies, military attacks, or infrastructural collapse. Recommending “self-care” or “organizational improvement” to nurses in Gaza risks absurdity, implying that suffering stems from inadequate stress management rather than systemic violence. Burnout theory illuminates aspects of nurse suffering in Gaza but fundamentally misidentifies the primary source and nature of harm. Its value lies in recognizing chronic stress and workload as harmful; its limitation lies in assuming stress originates within healthcare organizations and can be mitigated through internal reform. When the workplace is under siege, burnout’s conceptual assumptions break down.
Moral distress: Constraint and ethical compromise
Moral distress, originally defined by Jameton, 3 occurs when a healthcare provider knows the ethically correct action but is constrained from taking it by institutional obstacles. Subsequent scholarship has refined this definition, 21 with a comprehensive narrative synthesis highlighting its core components: the psychological distress arising from internal conflict between ethical knowledge and imposed action; constraints typically from hierarchical authority or resource limitations; and the cumulative, corrosive effects over time (moral residue). 4 Moral distress theory emerged from observations of nurses constrained by physician orders they deemed harmful, institutional policies prioritizing efficiency over patient welfare, and resource limitations forcing triage decisions. 3 Interventions derived from this framework include ethics consultation, shared governance structures empowering nurses, and advocacy for institutional policy change. 7
Moral distress theory powerfully explains aspects of nurse suffering in Gaza. Reports document nurses forced to ration pain medication, deny life-saving treatment due to supply shortages, and discharge patients they know are returning to unsafe conditions, all situations where nurses know the right action but cannot take it. 9 The internal conflict Jameton described (“I know what I should do, but I cannot do it”) is vividly present. The concept of moral residue is particularly relevant. Epstein and Hamric 21 describe how unresolved moral distress accumulates, leaving a residue that lowers the threshold for future distress. In Gaza, nurses face repeated, unresolvable ethical compromises: rationing care daily, witnessing preventable deaths repeatedly, losing patients to bombardment after saving them in surgery. Each instance leaves moral residue; the cumulative effect is profound. Moreover, moral distress captures the betrayal nurses experience when institutional protections fail. The hospital, meant to be a therapeutic sanctuary, becomes a target. Colleagues, meant to be protected under IHL, are detained or killed. The profession’s ethical codes (promising beneficence, non-maleficence, and patient advocacy) become impossible to fulfill. This gap between professional values and enforced actions aligns precisely with moral distress theory.
Despite this explanatory power, moral distress theory faces significant limitations when applied to Gaza. First, moral distress theory assumes constraints originate from within the healthcare institution: physician authority, administrative policies, resource allocation decisions made by the organization. Jameton’s 3 original examples involved nurses overruled by physicians or constrained by hospital policies. In Gaza, constraints originate entirely outside the institution, from military blockade, attacks on healthcare, political decisions about resource flows. The hospital administration is not constraining nurses; it is equally constrained by external forces. Moral distress theory lacks conceptual tools to address constraints imposed by actors external to healthcare. Second, moral distress assumes the correct ethical action exists and is known; the problem is an inability to perform it. This framework implicitly references the possibility of moral courage, the commitment to act on one’s ethical knowledge despite fear or risk. 22 In Gaza, however, situations arise where no ethically acceptable action exists, not because nurses lack courage, but because all available options violate ethical principles. The systematic destruction of agency makes the exercise of moral courage structurally impossible, revealing a limitation of the moral distress framework. Choosing which patient receives the last dose of medication violates justice; choosing which critically ill patient to evacuate first violates non-abandonment; continuing to work in a facility known to be a military target may endanger patients. These are not situations where the right action is blocked but where structural conditions render all actions ethically compromised. Moral distress theory does not account for contexts where ethical practice is structurally impossible. Third, moral distress interventions assume institutional capacity to change: ethics committees can review policies, nursing leadership can advocate for different resource allocation, shared governance can shift power dynamics. These interventions assume healthcare organizations have agency to modify constraints. In Gaza, the institution has no capacity to end the blockade, stop attacks, or restore infrastructure. Recommending “institutional advocacy” or “ethics consultation” as responses to blockade-induced scarcity mistakes the source of harm. Fourth, moral distress is typically framed as an individual nurse’s experience, even when recognizing it is widely shared. It focuses on the individual’s internal conflict and psychological response. In Gaza, the harm is not merely individually experienced but collectively imposed, an entire healthcare workforce systematically prevented from ethical practice by political-military actions. Moral distress theory’s individualized focus misses the collective, political nature of the violation. Moral distress theory captures the internal ethical conflict nurses experience in Gaza but misidentifies the source of constraint as internal to healthcare rather than external political violence. Its strength lies in recognizing the psychological harm of being unable to act ethically; its limitation lies in assuming constraints originate from healthcare institutions and can be addressed through institutional reform. When ethical practice is made impossible by military siege, moral distress theory’s conceptual scope is exceeded.
Resilience: Individual and collective adaptation
Resilience in nursing scholarship refers to the capacity to adapt to adversity, maintain well-being despite stress, and recover from difficulties.5,6 It is conceptualized both as an individual trait (psychological resilience) and a collective capacity (organizational or community resilience). Resilience discourse emphasizes positive adaptation, resourcefulness, and post-traumatic growth. Resilience interventions include mindfulness training, peer support programs, leadership development, and fostering organizational cultures that support staff.5,7 Such interventions, exemplified by work-based educational programs designed to build personal resilience, 23 operate on the underlying assumption that by strengthening nurses’ adaptive capacities, they can better withstand occupational stress and maintain professional effectiveness even in challenging conditions.
Resilience theory might observe that Gaza’s nurses continue to provide care despite overwhelming adversity, and indeed, humanitarian reports document extraordinary dedication, improvisation, and mutual support among healthcare teams. 9 Nurses develop makeshift protocols, share limited resources, support one another emotionally, and persist in caring for patients despite impossible conditions. From a resilience perspective, this demonstrates adaptive capacity and professional commitment. Resilience theory could recommend interventions: establishing peer support networks, providing trauma-informed supervision, creating safe spaces for emotional processing, building team cohesion, and offering psychological first aid. 19 These interventions aim to strengthen nurses’ capacity to endure and adapt.
However, applying resilience frameworks to Gaza raises profound theoretical and ethical problems. First, resilience discourse risks shifting responsibility for managing harm from those who cause it to those who suffer it. When nurses are framed as needing greater resilience to withstand siege, blockade, and attacks on healthcare, the ethical burden shifts from perpetrators of violence to victims of violence. This misidentifies where accountability belongs. Nurses should not need to be more resilient to bombardment; bombardment of hospitals should cease. Framing the problem as a resilience deficit rather than a justice violation is ethically and analytically flawed. Second, resilience interventions, including structured, work-based educational programs, 23 target individual and organizational capacity to adapt. This approach is appropriate when stressors are inevitable (natural disasters, disease outbreaks) or when systemic change is underway but incomplete. It is profoundly inappropriate, however, when harm is avoidable, externally imposed, and sustained by political choice, as it mistakes a political-military assault for a manageable workplace stressor. Recommending resilience training to nurses under siege individualizes a structural and political problem, treating symptoms while ignoring causes. Third, Traynor 24 argues that resilience discourse in nursing can perpetuate workplace exploitation by normalizing adversity and repositioning suffering as an opportunity for personal growth. Applied to Gaza, this reaches a grotesque extreme: framing survival under siege as “resilience” normalizes conditions that violate international law and obscures the political violence causing harm. Resilience discourse risks making unbearable conditions bearable, not by addressing their sources but by shifting the adaptive burden onto nurses. Fourth, resilience implies that adaptation is possible and desirable. But what does “adapting” to working in a hospital under bombardment mean? What does “resilience” look like when treating patients without anesthesia, or evacuating an intensive care unit under military order with nowhere safe to go? In such contexts, resilience rhetoric can pathologize normal responses to abnormal conditions, suggesting that distress indicates resilience failure rather than recognition of atrocity. This imposes impossible standards: expecting nurses to remain psychologically intact while witnessing systematic violations of everything they were trained to protect. Fifth, resilience interventions consume resources and attention that could be directed toward addressing root causes. Time spent on mindfulness training is time not spent documenting violations, advocating for IHL compliance, or mobilizing international solidarity. This is not to say psychological support is unimportant (it is necessary) but framing it as the primary response obscures the need for justice-oriented action. Resilience theory fundamentally misframes nurse suffering in Gaza by treating it as an adaptive challenge rather than a justice violation. Its ethical failure is profound: it risks normalizing atrocity by suggesting nurses should develop greater capacity to endure it. While psychological support for trauma is necessary, resilience discourse as a primary framework is both analytically inadequate and ethically unacceptable when applied to contexts of systematic political violence against healthcare. Resilience may be a necessary harm-reduction strategy in the absence of justice, but it cannot substitute for justice.
Summary: Where frameworks fall short
This analysis reveals a consistent pattern: burnout, moral distress, and resilience theories each provide partial insights into nurse suffering in Gaza but fundamentally misidentify the source of harm and, consequently, the appropriate response. All three frameworks assume healthcare organizations retain agency to modify working conditions and that occupational harm originates within healthcare systems, from staffing decisions, hierarchical constraints, or organizational culture. None adequately conceptualizes harm imposed by external political-military actors. All three assume internal reform, individual adaptation, or institutional advocacy can meaningfully address suffering. None accounts for situations where the capacity for internal mitigation is systematically destroyed by forces outside healthcare. Most critically, none of these frameworks captures the distinctive ethical violation at the core of nurse suffering in Gaza: being forced by external political violence to participate in practices that transgress deeply held moral commitments. This gap points toward a different concept (moral injury) which centers external transgression rather than internal constraint as the source of harm.
Moral injury: A reframing
Historical-conceptual background
Moral injury was first articulated in the context of combat trauma, describing psychological and spiritual harm experienced by military personnel who participate in, witness, or fail to prevent acts that violate deeply held moral beliefs.25,26 Unlike post-traumatic stress disorder (PTSD), which focuses on fear-based responses to life-threatening experiences, moral injury centers on betrayal and transgression. Clinical work with Vietnam veterans revealed a subset of psychological suffering not explained by PTSD. Veterans described enduring guilt, shame, and moral anguish from actions they were ordered to take, witnessed colleagues commit, or failed to prevent, actions they understood as violations of moral codes. 26 This included killing non-combatants, following unjust orders, or being betrayed by leaders who sent them into situations violating rules of engagement. These veterans did not describe fear as the primary issue but rather a shattering of moral identity: “I did something I believed was wrong, and I can never undo it.” 25 Shay 26 distinguished between trauma as a physiological threat response and moral injury as a social and moral phenomenon requiring different healing processes. While PTSD could be treated through exposure therapy and anxiety reduction, moral injury required processes of acknowledgment, accountability, and moral repair, recognition that something morally wrong occurred, that the wrong mattered, and that responsibility was properly assigned.
Moral injury concepts have been extended to healthcare, 27 describing clinicians forced to provide care they know is inadequate, participate in practices they believe are harmful, or be complicit in unjust allocation of resources. The COVID-19 pandemic accelerated this discussion, with clinicians reporting moral injury from rationing ventilators, denying families access to dying patients, and being unable to protect colleagues from inadequate personal protective equipment. 19 Dean et al. 27 argue that framing clinician distress as “burnout” when it arises from systemic betrayals (healthcare systems prioritizing profit over care, administrators demanding impossible productivity, and regulatory structures penalizing clinical judgment) obscures the source of harm and shifts responsibility inappropriately. They advocate for “moral injury” as a more accurate description, centering systemic betrayal rather than individual exhaustion.
Defining features of moral injury
Moral injury is distinguished by several defining features.25,26 First, it involves a transgressive action or inaction: The individual commits, witnesses, or fails to prevent an action that violates deeply held moral beliefs. Critically, this action is not freely chosen but externally compelled, by orders, circumstances, or systemic constraints. Second, it typically involves betrayal by legitimate authority: Moral injury often involves betrayal by figures or institutions in positions of legitimate authority, commanding officers who give unjust orders, healthcare administrators who prioritize profit over patient safety, or governments that violate laws they claim to uphold. The betrayal is more psychologically devastating when it comes from sources the individual trusted and granted moral legitimacy. Third, it creates internal moral conflict: The individual experiences profound internal conflict, recognizing the action as morally wrong while feeling unable to refuse or prevent it. This differs from moral distress (where the individual cannot act) in that the individual often does act but is forced to act wrongly. Fourth, it produces a lasting psychological and spiritual impact: Moral injury produces enduring guilt, shame, loss of meaning, difficulties with trust, and a sense of moral taintedness. Unlike acute stress reactions, these symptoms do not resolve with time or distance from the event. They represent a fundamental disruption of moral identity. Fifth, while individually experienced, it has systemic sources: The individual feels culpable for actions forced upon them by systems they could not control.
Moral injury in Gaza’s nursing context
Applying the moral injury framework to Gaza reveals its explanatory power. Nurses in Gaza are forced to commit acts they recognize as violations of professional ethics: denying treatment due to supply shortages imposed by blockade; triaging patients based on resource scarcity rather than clinical need; evacuating critically ill patients without medical justification because the facility is under military threat; treating patients without informed consent when communication is impossible; and working in facilities they know are military targets, potentially endangering patients. 9 These are not free choices but forced selections among impossible options. A nurse who rations the last dose of antibiotics knows she is denying life-saving treatment to one patient to potentially save another, an act that violates the principle of non-maleficence. She does it not because she chooses to but because no alternative exists. This is transgression under compulsion, the core of moral injury.
Multiple betrayals compound the injury. The international community and the UN system exist to protect healthcare in conflict. When these systems fail to prevent attacks on hospitals or enforce accountability for violations, nurses experience betrayal by institutions granted global moral authority to protect them. 12 State authorities imposing blockades and conducting military operations in civilian areas violate their obligations under IHL. For Palestinian nurses, this includes their own governing authorities’ inability to protect them and the occupying power’s systematic violations of protection duties. Professional organizations may also betray nurses when international nursing bodies fail to forcefully advocate for protection of healthcare or frame the situation primarily in resilience terms rather than justice terms, representing a form of professional abandonment. The betrayal is particularly devastating because it comes from institutions explicitly created to prevent such harms, IHL, the UN system, professional codes of ethics. The dissonance between stated protections and lived reality constitutes a profound moral betrayal.
Nurses in Gaza live in constant moral conflict. Every shift involves ethical compromises: which patient to treat first when all are critical, whether to continue working when the facility is under threat (abandoning patients vs endangering them by one’s presence), how to maintain professional standards when basic supplies are absent. This is not occasional ethical dilemma but sustained, unresolvable moral conflict embedded in the structure of practice. While comprehensive psychological studies of Gaza’s healthcare workers face methodological barriers due to ongoing conflict, available evidence suggests enduring psychological harm consistent with moral injury, including pervasive guilt, shame, erosion of professional identity, loss of trust in institutional protections, and loss of meaning in professional work.19,20
Importantly, moral injury frequently co-occurs with trauma-related responses, including fear-based symptoms characteristic of post-traumatic stress disorder (PTSD), particularly in contexts of direct violence and life-threatening exposure. However, the two are conceptually distinct. PTSD centers on dysregulated fear responses to threat, whereas moral injury centers on transgression, betrayal, and violation of deeply held moral commitments.25,26,28
This paper analytically foregrounds moral injury not to deny the presence of trauma, but to highlight a dimension of nurse suffering that is insufficiently explained by fear-based models alone and that directly implicates external political-military actors as the source of harm.
These are not symptoms that resolve when the individual shifts or rests; they are fundamental disruptions to moral selfhood requiring processes of moral repair. Critically, moral injury in Gaza originates entirely from systems external to healthcare: blockade policies determined by state authorities, military operations targeting civilian infrastructure, international failure to enforce IHL protections. Nurses bear the psychological burden of actions forced upon them by political-military decisions over which they have no control. This is systemic violence manifesting as individual moral suffering.
Moral injury versus moral distress: A critical distinction
The distinction between moral distress and moral injury is analytically important. To orient the reader, Box 1 presents a comparative framework distinguishing these concepts across key dimensions.
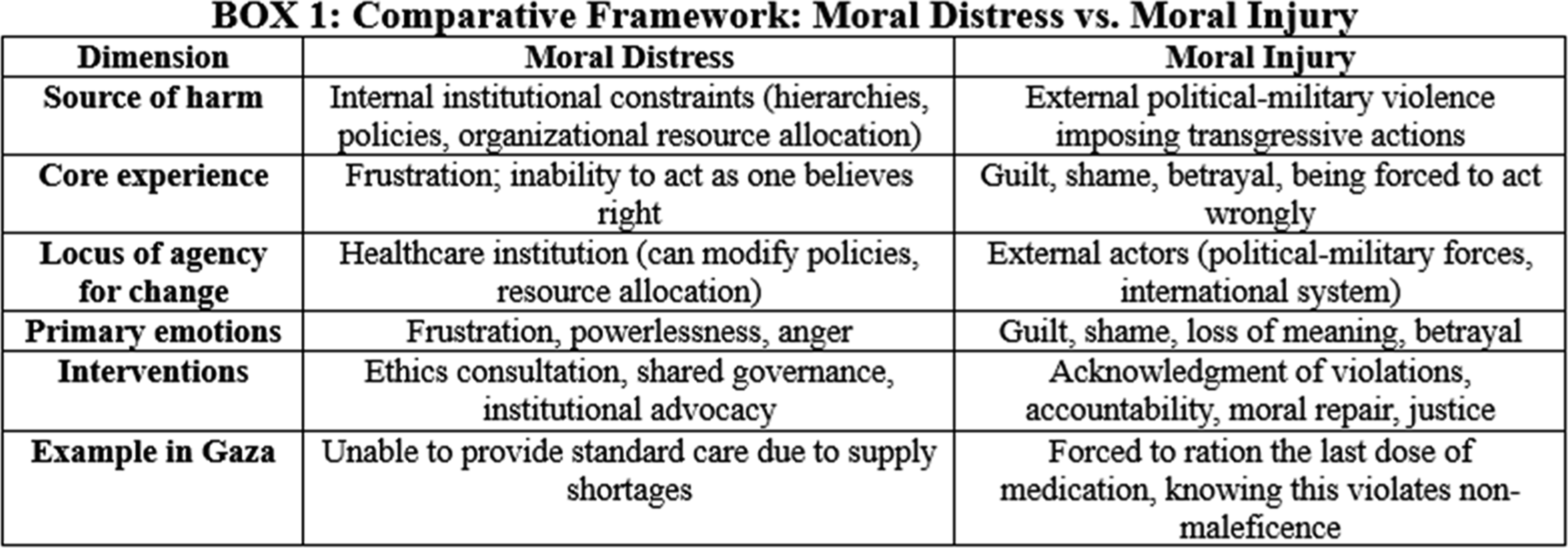
Moral distress originates from internal institutional constraints (administrative hierarchy, policies, resource allocation), where the nurse is unable to act as one believes right, leading to frustration, ethical compromise, and internal conflict. The locus of agency for change lies with the healthcare institution, and interventions include ethics consultation, shared governance, and institutional advocacy.3,4 In contrast, moral injury originates from external political-military violence forcing transgressive action, where the nurse is forced to act in ways one believes wrong, leading to guilt, shame, betrayal, and loss of moral identity. The locus of agency lies outside the healthcare institution, which has no capacity to change external forces, and interventions require acknowledgment of violation, accountability for perpetrators, moral repair, and justice.25,26
In Gaza, nurses experience both moral distress (constrained by limited resources within healthcare) and moral injury (forced to transgress ethical commitments by external political violence). The critical distinction is that moral distress points toward internal healthcare reform, while moral injury points toward external accountability and justice. Collapsing moral injury into moral distress obscures the need for political and legal responses to systematic violations.
Implications for conceptualizing nurse suffering
Recognizing moral injury as the dominant harm in Gaza has several implications. First, it reframes the problem: Nurse suffering is not primarily about exhaustion (burnout), institutional constraint (moral distress), or adaptation failure (resilience deficit). It is about being forced by political violence to violate core professional and moral commitments. This reframing shifts analysis from healthcare system dysfunction to political violence as an occupational hazard. Second, it identifies the source correctly: Moral injury locates the source of harm in external political-military actors who impose conditions making ethical practice impossible. This enables appropriate accountability: perpetrators of violations, not healthcare institutions or individual nurses, bear responsibility for harm. Third, it validates experience: Moral injury validates nurses’ suffering as a rational response to moral violation rather than pathologizing it as stress intolerance or resilience failure. Guilt and shame, rather than being irrational symptoms requiring cognitive restructuring, are recognized as moral responses to being forced into moral transgressions. This validation is ethically and therapeutically important. Fourth, it directs intervention appropriately: Moral injury requires interventions addressing structural sources and seeking moral repair: documentation of violations, accountability for perpetrators, acknowledgment by authorities and professional bodies that wrongs occurred, restoration of protections, and processes of witnessing and moral reckoning. While individual psychological support remains necessary, it is insufficient without justice-oriented structural change. The next section develops these implications into a justice-centered framework for nurse well-being in conflict settings.
Toward a justice-centered framework
Having established that moral injury, arising from externally imposed political violence, constitutes the dominant occupational harm in Gaza, this section proposes a justice-centered framework for understanding and addressing nurse well-being in conflict settings. This framework repositions protection, accountability, and solidarity as central professional imperatives rather than peripheral political concerns.
Principles of a justice-centered approach
A justice-centered framework rests on four foundational principles, extending the core imperatives of global health ethics, which emphasize equity, solidarity, and the duty to address structural determinants of health, 29 to the specific occupational reality of nurses in conflict. First, political violence as occupational hazard: In conflict settings where healthcare is systematically targeted, political-military violence constitutes a primary occupational hazard, not an external context separate from occupational health but a direct threat to worker safety requiring explicit professional response. Just as industrial nursing recognizes chemical exposure or equipment failure as occupational hazards requiring regulatory intervention, nursing in conflict must recognize blockade, bombardment, and detention of healthcare workers as occupational safety violations requiring international legal accountability. Second, structural sources require structural responses: When harm originates from external political structures rather than internal healthcare management, responses must target those external structures. Individual resilience-building and institutional reform, while potentially supportive, cannot address blockade-induced scarcity, military attacks, or infrastructural collapse. Appropriate responses must engage political, legal, and advocacy mechanisms to address root causes. Third, justice as a precondition for well-being: In contexts of systematic moral injury, psychological well-being cannot be sustainably restored without justice. Moral repair requires acknowledgment that violations occurred, attribution of responsibility to perpetrators, and meaningful accountability. Well-being interventions that bypass justice risk becoming mechanisms of adaptation to injustice, making unbearable conditions psychologically bearable without changing the conditions. Fourth, professional solidarity as ethical imperative: Protection of colleagues targeted for providing care is not charity but professional obligation. If healthcare is a global profession with universal ethical commitments, then protecting nurses working under siege, advocating for IHL compliance, and facilitating safe evacuation when necessary are core expressions of professional identity, not peripheral political activism but central professional solidarity.
Components of the framework
The justice-centered framework comprises four interconnected components.
Documentation and legal accountability
Systematic documentation of attacks on healthcare, violations of IHL, and impacts on clinical practice must be recognized as a core professional activity, not an optional advocacy add-on. This requires the development of standardized incident reporting protocols for healthcare workers to safely document attacks on facilities, detention of colleagues, and blockade-induced supply failures, integrated into occupational health reporting systems rather than treated as separate advocacy work. Violations should be tracked alongside traditional occupational health metrics (injury rates, exposure incidents), making visible the occupational burden of political violence. Documentation should feed into international mechanisms (UN Commission of Inquiry, Special Rapporteurs, International Criminal Court investigations), ensuring healthcare worker testimony contributes to legal accountability.
Professional nursing organizations must reframe advocacy for IHL compliance as occupational safety advocacy. When the International Council of Nurses calls for protection of healthcare workers under IHL, this is not a political statement but an occupational safety demand, equivalent to demanding safe patient handling equipment or infection control measures. This requires explicit position statements classifying attacks on healthcare as occupational safety violations, integration of IHL compliance advocacy into occupational health policy, and partnerships with legal organizations pursuing accountability for healthcare violations.
Global professional solidarity mechanisms
Professional solidarity must include material dimensions, not just statements of support but tangible assistance. This includes establishing supply chains coordinated by nursing organizations to ensure medical supplies reach blockaded settings, including advocacy with governments controlling borders and coordination with humanitarian agencies. Financial support through professional funds can support salaries for nurses in conflict zones when healthcare systems collapse, enabling continued provision of care. Technical assistance via remote consultation and telemedicine support connects isolated healthcare teams with specialists globally.
While psychological support alone is insufficient, it remains necessary. Trauma-informed peer support networks facilitated by professional organizations can connect nurses in conflict zones with peers who have worked in similar contexts, providing validation and practical coping strategies. Culturally grounded mental health services should be provided in partnership with local mental health professionals, avoiding Western pathologization of normal responses to atrocity. Moral repair processes involving structured opportunities for healthcare workers to testify about ethical violations they were forced to commit can facilitate collective acknowledgment and reduce isolation in moral injury.
Protection under international humanitarian law
The framework demands renewed commitment to IHL enforcement. This involves advocacy for state accountability to fulfill obligations to protect healthcare in occupied territories and during armed conflict, with specific mechanisms to monitor compliance and impose consequences for violations. Professional association advocacy with national governments for IHL compliance and for prioritizing healthcare protection in diplomatic and military policy is essential. Support for international legal mechanisms like ICC investigations and UN inquiry commissions examining healthcare violations, including provision of healthcare worker testimony and expert analysis, is also crucial.
Renewed emphasis on protective emblems and identification is needed: healthcare facilities and vehicles clearly marked with protective emblems, healthcare workers visibly identified as protected persons under IHL, and international observation and documentation when these protections are violated. While emblems alone cannot prevent attacks when belligerents disregard IHL, their systematic use creates evidentiary records of violations and reinforces normative expectations of protection.
Evacuation and safe passage rights
Just as occupational safety in industrial settings requires emergency exits, occupational safety in conflict zones requires viable evacuation mechanisms for healthcare workers. This represents a fundamental but currently underdeveloped component of professional protection. The principle is that healthcare workers should not be required to remain in combat zones until injured or killed. When a facility becomes a target, safe evacuation is a right, not abandonment of duty. Evacuation should be internationally facilitated, ensuring safe passage regardless of which parties control territory. Professional organizations should establish protocols for when evacuation is ethically permissible and practically necessary, removing the moral burden from individual nurses to decide whether staying constitutes dedication or recklessness.
Implementation requires international coordination: UN agencies, ICRC, and professional nursing organizations should establish standing mechanisms to facilitate healthcare worker evacuation from active conflict zones, including negotiation of safe passage, logistical support, and reception in destination countries. Protection of evacuees is essential, with evacuated healthcare workers granted temporary protection status in receiving countries, supported by professional organizations with licensure transfer and employment. Professional codes should explicitly affirm non-punishment for evacuation, countering narratives that frame evacuation as abandonment.
Evacuation raises complex ethical questions: if all healthcare workers evacuate, who remains to care for patients? This tension has no perfect resolution. However, framing evacuation as a legitimate safety right rather than professional failure creates space for ethical deliberation rather than forcing individuals to choose between professional duty and survival. It also increases pressure on international actors to establish protections that make evacuation unnecessary, because healthcare should not require evacuation; it should be protected.
Implementation challenges and responses
This framework faces significant implementation challenges, particularly in contexts where political will to enforce international humanitarian law is weak or actively obstructed. The justice-centered approach articulated here is therefore not presented as an immediately realizable policy blueprint but as a normative professional standard, analogous to occupational safety frameworks that historically preceded enforcement, regulation, and accountability mechanisms. Challenge 1: Access and Documentation Safety. Healthcare workers in conflict zones face risks documenting violations. Security protocols must be developed to enable safe documentation, including encrypted communication, secure data storage, anonymous reporting options, and protection for witnesses who come forward after evacuation. Challenge 2: Political Will. The framework requires political will to enforce IHL, pursue accountability, and prioritize healthcare protection, often absent in contemporary conflicts. Professional organizations must engage in sustained advocacy to create this will, recognizing that immediate success is unlikely but that consistent principled advocacy shapes long-term norms. Challenge 3: Resource Constraints. Implementing solidarity mechanisms requires resources, funding for material support, staff time for coordination, political capital for advocacy. Professional organizations must commit resources to this work, recognizing that protecting colleagues in conflict zones is a core professional investment, not an optional charitable activity. Challenge 4: Balancing Support with Justice. There is inherent tension between providing psychological support to enable survival under unjust conditions (which risks normalizing injustice) and refusing to provide support until justice is achieved (which abandons people in immediate need). The framework attempts to hold both: provide necessary support while simultaneously advocating for structural change, always making clear that support is harm reduction, not solution, and that justice remains the goal.
Contrasting with resilience approaches
The critical difference is that resilience asks, “How can nurses endure this?” while the justice framework asks, “Why should nurses be required to endure this, and how do we change the conditions?” Both questions have merit, but the justice framework refuses to accept political violence as an inevitable context requiring only adaptive response.
Application beyond Gaza
While this framework emerged from analysis of Gaza, its principles apply wherever healthcare is systematically targeted in conflict: Syria’s barrel-bombed hospitals, Yemen’s blockaded healthcare system, Ukraine’s targeted medical infrastructure, Sudan’s healthcare collapse amid civil war. The framework is not specific to Palestinian nurses or Gaza but to a structural condition: healthcare under political-military siege. Wherever nurses are forced to practice in conditions of systematic resource deprivation, direct violence, and infrastructural collapse imposed by external political actors, this framework applies. Moral injury, not burnout or moral distress, is the dominant harm; justice, not resilience, is the prerequisite for well-being; professional solidarity includes material protection, not just statements of concern; occupational health includes political advocacy for IHL compliance. The universality of the framework rests on the universality of IHL and nursing ethics: healthcare should be protected in all conflicts; nurses should not be forced to violate professional commitments. When these universals are systematically violated, the professional response must be equally universal.
Discussion
This synthesis reveals a fundamental mismatch between how nursing scholarship explains occupational harm and the conditions documented in contemporary conflict settings. The analysis proceeded through three stages. First, humanitarian evidence from Gaza documented three systemic hazards: resource deprivation imposed through military blockade, direct violence against healthcare infrastructure and personnel, and infrastructural collapse rendering healthcare improvised and unsupported. These hazards interact and amplify each other, transforming healthcare settings from therapeutic spaces into sites of danger and ethical compromise. Second, dominant nursing frameworks (burnout, moral distress, and resilience) were systematically applied to these conditions. Each framework provided partial insights but ultimately proved inadequate. Burnout recognizes chronic stress but locates its source within healthcare organizations rather than external political violence. Moral distress captures ethical conflict but assumes constraints originate from internal institutional hierarchy rather than external military siege. Resilience emphasizes adaptive capacity but inappropriately shifts responsibility for managing harm from perpetrators to victims, risking normalization of atrocity. All three frameworks assume healthcare organizations retain agency to modify working conditions and that occupational harm can be addressed through internal reform, individual adaptation, or institutional advocacy. None adequately conceptualizes harm imposed by external political-military actors or accounts for situations where the capacity for internal mitigation is systematically destroyed. Third, moral injury was introduced as an alternative framework. Originating in combat trauma studies, moral injury describes psychological harm arising when individuals are forced by external actors to commit, witness, or fail to prevent acts violating deeply held moral beliefs. Applied to Gaza, moral injury captures the core dynamic of nurse suffering: being compelled by blockade, bombardment, and infrastructural collapse to act in ways that transgress professional ethical commitments. Unlike burnout or moral distress, moral injury correctly identifies the source of harm (external political violence), the nature of harm (forced transgression producing guilt and betrayal), and the appropriate response (justice, accountability, and structural change rather than individual adaptation).
Theoretical implications
This analysis has significant implications for nursing theory. The findings challenge the assumed universality of occupational health frameworks developed in peacetime, institutional settings, thereby engaging directly with the core project of theoretical nursing: to critically examine, develop, and refine the conceptual structures that guide the profession. 30 Burnout, moral distress, and resilience theories rest on implicit assumptions about the nature of the workplace, that it is governed by internal management, subject to organizational reform, and located within a functioning legal and normative order. When these assumptions do not hold, the frameworks lose explanatory power. This suggests the need for distinct theoretical frameworks for nursing in conflict, or at minimum, explicit acknowledgment of the scope conditions under which mainstream theories apply, a necessary step in the theoretical progress of the discipline. 30
The analysis reveals that occupational health is irreducibly political in conflict settings. Worker safety cannot be separated from questions of state accountability, international law compliance, and military conduct. This finding underscores that nurse well-being in Gaza is a complex phenomenon, arising from dynamic interactions between political, military, legal, and ethical systems, a reality that demands analytical frameworks capable of engaging with such complexity. 31 This directly challenges tendencies within nursing to marginalize politics, a critique aligned with scholarship that problematizes depoliticized social justice discourses in the profession. 32 In conflict, there is no apolitical nursing, only nursing that acknowledges political sources of harm or nursing that obscures them. Therefore, occupational health frameworks must incorporate political analysis and advocacy as core, integrated components, not peripheral additions.
Dominant frameworks individualize suffering; burnout as personal exhaustion, moral distress as individual internal conflict, resilience as personal adaptive capacity. Moral injury, while individually experienced, centers collective and systemic sources. This shift from individual to systemic analysis has methodological and ethical implications: it demands research methods capturing collective experiences (participatory research, testimonial projects), and it repositions intervention from individual treatment to collective advocacy and structural change.
The analysis suggests that in contexts of systematic violence, psychological well-being cannot be sustainably restored without justice. Moral repair requires acknowledgment of violations, attribution of responsibility, and meaningful accountability. This challenges health frameworks that treat well-being as achievable through psychological intervention alone, independent of addressing structural injustice. It suggests the need for integrative frameworks linking occupational health with human rights, international law, and social justice scholarship.
Implications for practice
For nursing practice in conflict settings, the analysis suggests several implications. Recognizing moral injury validates healthcare workers’ suffering as a rational response to moral violation rather than pathologizing it as stress intolerance or professional inadequacy. This has therapeutic importance: nurses should understand their guilt, grief, and moral anguish as appropriate responses to being forced into ethical compromise, not as signs of personal failure. Well-being interventions should begin with this validation.
The framework affirms evacuation as a legitimate ethical choice when personal safety is at risk or when continued presence may endanger patients. Professional discourse should support these deliberations rather than imposing impossible standards of self-sacrifice. This requires nuanced ethical frameworks acknowledging that dedication to patients does not require martyrdom and that collective professional capacity is preserved by protecting individual members.
Healthcare workers should be supported to document violations as part of professional practice. This requires training in safe documentation methods, provision of secure reporting systems, and organizational cultures affirming documentation as valuable professional work rather than political activism.
Practice settings should provide access to moral repair processes, structured opportunities for healthcare workers to testify about violations they were forced to commit, facilitating acknowledgment and reducing isolation. This goes beyond conventional critical incident debriefing to include ethical reflection, collective witnessing, and connection to accountability processes.
These implications are supported by emerging evidence from Palestinian nursing contexts. Recent research has documented the relationship between stress, resilience, and psychological outcomes among nurses and nursing students experiencing political violence.33–35 Studies examining professional quality of life and work environment among nurses in intensive care and neonatal units highlight the intersection of occupational demands and psychological well-being in high-stress clinical environments.36,37 Research on workplace violence against healthcare workers reinforces the importance of occupational safety frameworks that explicitly address external threats to nursing practice. 38 These studies collectively underscore the need for conceptual models that move beyond individual resilience to address structural and systemic sources of occupational harm.39,40
Implications for policy
For nursing organizations and policymakers, the analysis demands several shifts. International and national nursing organizations must reposition advocacy for IHL compliance and healthcare protection as occupational safety advocacy, not optional political engagement but core professional responsibility. Position statements should explicitly classify attacks on healthcare, blockades creating supply shortages, and detention of healthcare workers as occupational safety violations requiring the same institutional response as chemical exposure or equipment failure in other settings.
Professional organizations should develop concrete mechanisms for protecting colleagues in conflict zones: coordination of humanitarian supply delivery, financial support for salaries when systems collapse, facilitation of evacuation when necessary, and provision of legal support for healthcare workers facing detention or prosecution for providing care. These mechanisms should be standing capacities, not ad hoc responses to each new crisis.
Resources should be committed to supporting healthcare workers to safely document violations and to ensuring this documentation feeds into international legal accountability mechanisms. This includes funding for secure communication technologies, legal expertise to support testimony in inquiry commissions and courts, and sustained engagement with UN mechanisms and the International Criminal Court.
Research funding should prioritize participatory and testimonial methods that center healthcare workers’ lived experience in conflict zones. This research should be conducted in equitable partnership with local scholars and professional associations, ensuring knowledge production serves the interests of those most affected.
Methodological reflections and limitations
This synthesis employed critical interpretive synthesis (CIS) to engage discursively with competing theoretical frameworks and integrate diverse forms of evidence. Unlike conventional systematic reviews, CIS enabled the inclusion of both humanitarian reports and conceptual scholarship, facilitating theoretical development rather than empirical aggregation. This approach was particularly appropriate in a context where direct access for primary research is constrained by insecurity and restricted entry. Furthermore, the use of Gaza as a critical case enhanced methodological rigor by moving beyond descriptive case analysis to theoretically probe the adequacy of existing frameworks for understanding nurses’ experiences in extreme settings.
Several limitations should be acknowledged. First, the synthesis relied primarily on secondary sources, including humanitarian reports rather than direct testimony from nurses working in Gaza. Although reports from authoritative agencies such as the United Nations, World Health Organization, International Committee of the Red Cross, and Médecins Sans Frontières are widely regarded as credible, they represent mediated accounts rather than firsthand narratives. Future research should prioritize direct engagement with nurses through participatory, qualitative, and testimonial approaches when access and safety permit.
Second, the focus on Gaza as a single critical case enabled analytical depth but necessarily limits the breadth and transferability of findings. Comparative analyses across multiple conflict settings, including Syria, Yemen, Sudan, and Ukraine, would strengthen understanding of both shared and context-specific patterns affecting healthcare workers and should constitute an important direction for future scholarship.
Third, this synthesis examined the conceptual adequacy of theoretical frameworks but did not empirically evaluate psychological outcomes or the effectiveness of proposed interventions. Empirical studies measuring moral injury, moral distress, burnout, resilience, and related outcomes among conflict-affected healthcare workers are needed to complement conceptual analyses and assess the impact of justice-oriented interventions in practice.
Finally, although no language restrictions were applied during the search process, only English-language sources were ultimately included because of resource and translation constraints. Consequently, relevant scholarship published in Arabic or other languages may have been overlooked. Future reviews would benefit from multilingual search strategies and greater translation capacity to ensure a more comprehensive and inclusive evidence base.
Future research directions
The analysis suggests several research priorities. Research projects employing participatory methods to document lived experiences of moral injury among nurses in Gaza and other conflict settings, conducted in partnership with Palestinian nursing scholars and professional associations, are needed. This should include testimonial projects creating permanent records of violations and their impacts. Systematic comparison of healthcare working conditions and nurse well-being across multiple conflicts (Syria, Yemen, Sudan, Ukraine, Gaza), examining how different patterns of violence (siege, bombardment, displacement, detention) produce distinct or similar forms of moral injury and how local professional responses vary, is essential. Development and evaluation of interventions based on moral injury and justice frameworks, documentation protocols, moral repair processes, professional solidarity mechanisms, and accountability advocacy strategies, should be undertaken. Research should examine both immediate psychological impacts and longer-term effects on professional identity and practice. Continued theoretical work integrating moral injury concepts with nursing ethics, international humanitarian law, and social justice frameworks to develop comprehensive models of nursing in conflict that can guide education, practice, and policy is also required.
Conclusion
This synthesis reveals that dominant frameworks within nursing scholarship (burnout, moral distress, and resilience) fail to adequately explain nurse suffering in conflict settings where healthcare is systematically targeted. These frameworks assume functional healthcare systems capable of internal reform and locate occupational harm within institutional boundaries. In Gaza, and in similar conflict settings globally, these assumptions do not hold. The analysis demonstrates that in contexts of sustained armed conflict, political violence constitutes a primary occupational hazard, and the resulting harm is best understood as moral injury: psychological, moral, and existential suffering arising when nurses are forced by external political-military actors to transgress core professional ethical commitments. This is not a problem of individual burnout, institutional moral distress, or inadequate resilience. It is a problem of systematic violations of international humanitarian law producing morally injurious working conditions.
This reframing demands a fundamental shift in how the nursing profession responds to colleague suffering in conflict. Individual resilience-building and institutional reform, while potentially supportive, cannot address harm imposed by military siege and systematic attacks on healthcare. This analysis does not seek to replace trauma-informed care but to situate it within a justice-oriented professional response that acknowledges externally imposed moral harm and collective responsibility. Appropriate responses must engage political, legal, and advocacy mechanisms to address root causes: documentation of violations, pursuit of accountability under international law, material protection and solidarity with colleagues under attack, and, when necessary, facilitation of safe evacuation. The justice-centered framework proposed here repositions protection, accountability, and solidarity as core professional imperatives. In conflict settings, occupational health is inseparable from international humanitarian law compliance, human rights advocacy, and collective professional action to protect healthcare. These are not peripheral political concerns but central requirements for maintaining the ethical foundations of nursing practice.
Gaza served in this analysis as a critical case, a methodological site where theoretical limits could be tested. The findings suggest that when healthcare is systematically destroyed by political violence, new conceptual tools are required. However, Gaza is not unique: similar patterns have been documented across contemporary conflicts. The conceptual shift proposed, from internal, individualized models of harm to recognition of externally imposed, politically-generated moral injury, is therefore relevant beyond a single setting. For nursing scholarship, this demands expanding occupational health frameworks to explicitly address political sources of harm and integrating justice-oriented responses as core components of professional practice. For nursing organizations, this demands material solidarity with colleagues in conflict zones and sustained advocacy for international humanitarian law compliance as occupational safety advocacy. For individual nurses, this demands recognition that suffering under systematic violence is a moral response to moral violation, not professional inadequacy.
Ultimately, this analysis argues that nurse well-being in conflict cannot be secured through individual adaptation to unjust conditions but requires collective action to transform those conditions. Justice is not a political preference but a practical prerequisite for ethical nursing practice. When nurses are compelled by political violence to violate professional commitments, the profession’s response must prioritize accountability, protection, and solidarity in recognition that political violence itself has become a primary occupational hazard.
Future empirical research should prioritize direct engagement with nurses working in conflict-affected settings through participatory, testimonial, and mixed-method approaches. Such studies are needed to examine the lived experience of moral injury, evaluate justice-oriented interventions, and translate conceptual advances into evidence that can inform nursing education, practice, policy, and humanitarian preparedness.
Footnotes
Acknowledgments
The author acknowledges Nablus University for Vocational and Technical Education for its academic support and the librarians who assisted with resource access. This paper relies on the essential documentation provided by humanitarian and health organizations, including the World Health Organization, Médecins Sans Frontières, and the United Nations. Above all, it is written in solidarity with and profound respect for the nurses of Gaza, whose courage and dedication under extreme duress embody the highest ideals of the nursing profession.
Ethical considerations
Not applicable. This is a discursive analysis based on publicly available literature and reports. No human or animal subjects were involved.
Author contributions
Ibrahim Aqtam: Conceptualization, methodology, formal analysis, investigation, writing—original draft, writing—review and editing, project administration, and data curation. Nihad Bsharat: Writing—review and editing, validation, resources, supervision, and funding acquisition. Mustafa Shouli: Writing—review and editing, validation, investigation, data curation, and visualization. Hamdallah H. Khaled: Writing—review and editing, validation, supervision, project administration, and funding acquisition. Ehab Tumeh: Writing—review and editing, validation, investigation, resources, and data curation. Issam Iyrot: Writing—review and editing, validation, methodology, resources, and supervision. Saqer Al-Koroum and Ibrahim Khraiwesh: Writing—review and editing, validation, investigation, resources, and visualization.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The full bibliographic dataset compiled and analyzed during this study is available from the corresponding author on reasonable request.