
Abstract
This study was conducted to determine the practices, antecedents and outcomes of defensive medicine practices. For this purpose, this study was designed as a phenomenological research study using qualitative research methods. In-depth interviews were conducted with physicians who were practitioners and, thus, the experiencers of defensive medicine. The target population of the research consisted of 1,153 physicians working in the Sakarya city centre. The in-depth interviews were conducted with 21 physicians who agreed to participate. The resulting data were encoded and analysed using the NVIVO 12 software. As a result of this research, definitions of defensive medicine practices, positive defensive medicine and negative defensive medicine have been constructed using the expressions used by physicians. Besides, we obtained results indicating the practices of defensive medicine, the antecedents of defensive medicine and the outcomes of defensive medicine. The results of this study contribute to the literature in terms of providing comprehensive knowledge of defensive medicine.
Keywords
Introduction
Defensive medicine practices are commonly described as the requesting the more medical test by physicians to protect themselves from malpractice and lawsuits, including following unnecessary procedures during a relationship with the patient, hospitalising patients without medical necessity or, conversely, avoiding risky patients and risky methods of diagnosis and treatment (Catino, 2009; Montanera, 2016; OTA, 1993; Paik et al., 2017; Sulmasy & Weinberger, 2014). Defensive medicine, according to this definition, is not for the patient’s benefit. It consists of practices executed by the physician to protect himself/herself from legal responsibility or to strengthen his/her defence in possible cases brought against him/her (Simon, 1992). In other words, physicians perform medically unapproved practices to reduce the likelihood of malpractice (Project, 1971). Accordingly, defensive medicine occurs when physicians create diagnostic and treatment strategies that are not according to scientific evidence to avoid possible risky cases (Toraldo et al., 2015).
In general, two types of defensive medicine practice are mentioned, namely positive defensive medicine practices and negative defensive medicine practices (Summerton, 1995; Yan et al., 2017). Positive defensive medicine practices include extra practices that have no marginal or medical value to prevent the patients from complaining of malpractice, reducing the risk of failed medical attempts or convincing the legal control mechanisms that the standards of care have been met (Hiyama et al., 2006; Studdert et al., 2005). These implementations include additional services such as requesting extra testing, hospitalising the patient even if it is unnecessary, and requesting a non-medical consultation (Bean, 2016; Hoffman & Herring, 2015). Negative defensive medicine practices are described as physicians avoiding risky procedures, cases and patients due to a fear of being sued (Bean, 2016; Yan et al., 2016).
The reasons for using defensive medicine practised by physicians have been sorted in the study by Jackson Healthcare Company (2012) and Catino (2011) as follows: a desire to be protected from possible cases or individual compensation; the physician or a colleague’s involvement in a case of malpractice; the fear of missing something or the desire not to do wrong, their received medical education encouraging the practice of defensive medicine; turning defensive medicine into a standard of care; the desire to increase, protect and not risk the reputation of the physician; the fear that he/she will seem ‘inadequate’ if he/she does not perform the medical practices of other doctors; the physician’s personality traits such as a fear of a disciplinary penalty; the idea that any bad outcome belongs to the physician and pressures such as the patient’s desire for physicians to comply with the perfect physician definition and for them to do everything possible. Besides, evolving technology (Papanikitas & Jani, 2018) and a fear of violence (Akdur, 2013; Yeşiltaş & Erdem, 2018) are other causes of defensive medicine.
There are many positive and negative outcomes of defensive medicine. It is claimed in some research that benefits arise for patients as a result of defensive medicine practices (Passmore & Leung, 2002; Reuveni et al., 2017; Sclar & Housman, 2003; Studdert et al., 2005; Summerton, 1995). However, some studies note the negative consequences of defensive medicine (Antoci et al., 2016; Sclar & Housman, 2003). Although not mentioned much in the literature, it is understood that defensive medicine has some benefits for patients. It may have positive results such as more uniform patient records applied in the scope of defensive medicine (Catino & Cellotti, 2009), more frequent patient follow-ups (Reuveni et al., 2017) and increased technical quality (Perry, 2013) of practices such as communicating more positively with patients (Aynacı, 2008) and the early diagnosis of certain diseases (Studdert et al., 2005).
There is a great deal of research on the harms of defensive medicine, reporting that especially positive defensive medicine practices lead to unnecessary use of resources and increased costs (Kessler & McClellan, 1996; Sethi et al., 2012). In addition to the monetary costs of defensive medicine, there are indirect costs such as personal stress, loss of time, loss of reputation of physicians, and a tendency to avoid treatment of high-risk patients (Kessler, 2011). In addition, research stated that defensive medicine would prevent patients’ access to the service (Studdert et al., 2005; Tancredi & Barondess, 1978) and the patients will be exposed to the side effects (Fronczak, 2016; Yan et al., 2016).
Although there are empirical findings in the literature on defensive medicine and its implementation, we have yet to encounter any comprehensive studies examining the antecedent and outcomes of defensive medicine implementations. To fully understand the subject, inductive reasoning and the antecedent and outcomes of defensive medicine need to be explored. It is very important to determine the experiences and opinions of physicians who are practitioners of defensive medicine regarding the concept of defensive medicine. Therefore, this study aims to determine physicians’ perceptions regarding defensive medicine practices, antecedents and outcomes. To this end, the research’s main question is, ‘What are the experiences of physicians regarding the practice, antecedents and consequences of defensive medicine?’ The sub-questions created to reach this main question are as follows:
What is defensive medicine? [What is positive defensive medicine (Guarantor medicine)? What is negative defensive medicine (avoider medicine)?] What are the defensive medicine practices? What are the antecedents of defensive medicine practices? What are the consequences of defensive medicine practices?
Method
In this study, 1,153 physicians considered to have experience with defensive medicine practices and who worked in public health organisations in Sakarya province were the target population of this study. The phenomenological research method was chosen because it is necessary to work with people who have experienced a particular phenomenon. Phenomenology samples are often selected from within the group with a particularly characteristic feature. It is stated that 5–25 participants who have experienced the phenomenon in all aspects are a suitable sample size in phenomenological studies (Polkinghorne, 1989). However, an important principle of sample size in qualitative research is to obtain the maximum level of information. In this study, the research continued for as long as different information was obtained in the interviews. Since the information began to be repeated, it was decided to limit the sample after interviewing 21 physicians. In the final sample, nine physicians from the surgical specialisation, nine physicians from the internal specialisation, two physicians from the emergency medicine and one physician is anesthesiology and the reanimation specialisation.
Data Collection Tool
The data were collected using semi-structured interviews. In creating a qualitative data collection tool, the questions were determined by examining the literature. The questionnaire was formed according to feedback from two academicians with expertise in the field. Besides, a pilot study was conducted with two physicians. As a result of the pilot study, the questionnaire was finalised. The questionnaire consisted of seven questions (three introductions and four research questions).
Data Collection Method and Process
The interview method was preferred as a data collection technique. We used a semi-structured interview form (questionnaire) during interviews.
Within the scope of this research, the interaction period, participant confirmation and expert review strategies were monitored in order to increase the credibility of research. First of all, in the in-depth interviews, it was considered important to provide a sufficient interview time (average 45 ± 5 minutes) to the participants. Before the interview, the physicians were shown the research permits obtained from the provincial health directorate and the Sakarya University ethics committee. The second strategy followed in this dimension was participant confirmation. In this strategy, the researchers transcribed the audio recordings on paper and showed the participants the interview documents for them to confirm. The last strategy was an expert review. In this strategy, the researchers asked two people with a general knowledge of defensive medicine who specialised in qualitative research methods to review the research.
The researcher preferred to conduct the triangulation of this research for reliability. Considering the recommendations of Moustakas (1994), the textural depiction of an individual’s experiences (i.e., what they experience) was followed by a structural depiction (i.e., how they experience it in terms of condition, state and content). Thus, an effort was made to achieve the essence. During the coding process, the researcher and assistant researcher made the encodings independently. The encodings were compared. The compliance between the compared codes was found to be 90%. Non-conforming codes were discussed among the researchers and transformed into common codes. After the coding phase, the analysis of the qualitative data was carried out.
Results
Definition of Defensive Medicine
The physicians were asked to describe defensive medicine. The definitions made by physicians were analysed using the NVIVO 12 software.
The words that stand out in the definitions of defensive medicine made by physicians are to protect, risky, unnecessary, malpractice, violence, not to do, inspection, lawsuit and surgery. The word protection was used in the interviews as follows: protecting himself/herself, protecting themselves, protecting the physician, protecting the physicians from legal responsibilities [and] protecting the patient. The word risky was mentioned as not taking risks, avoiding risky patients, not being done because it is overly risky, very risky [and] directing risky cases. Physicians referred to the words unnecessary, examination and consultation as unnecessary examination, unnecessary consultation and unnecessary cases. Physicians who used the word malpractice used in phrases such as avoiding malpractice lawsuits; there are so many malpractice lawsuits. Physicians have expressed the word violence in phrases such as attitudes close to violence, applying violence to me and burdening up to violence. Physicians talking about the phrase not to do used it in a phrase such as not to do what I can do, not to do work and not to do to avoid risks. Physicians used the word sue as in he is suing and to prevent him from suing when expressing their concerns.
By taking into account the definitions of defensive medicine that the physicians put forward, it can be given as follows:
It is attitudes and behaviours such as the fear of missing important findings by physicians, the desire to be error-free, the desire to prevent possible complaints from patients and/or their families, the fear of violence and the fear of involvement in malpractice cases, requesting extra tests and examinations, following unnecessary procedures, requesting extra consultations with the fear of violence and fear of involving in the malpractice case, hospitalising the patient more than necessary or avoiding risky patients and risky diagnosis/treatment methods.
Positive defensive medicine (guarantor behaviour): Within the scope of this study, the physicians were asked what the concept of positive defensive medicine meant to them.
The words most frequently used to explain the concept of positive defensive medicine by the physicians were extra/addition/extremely, detailed, extreme, inspection/test, consultation, consent, signature, record, defensive, missing, hospitalisation, for their benefit/advantage. The most mentioned practices within the scope of positive defensive medicine practices are examination/analysis, consultation, consent, signing, record-keeping and hospitalisation. Physicians used the words extra/additional paired with defensive medicine practices such as consultation, examinations, additional tests, and everything else requested. Similarly, they used the word excessive to request an excessive examination. The participants pronounced the word detailed as in detailed consent and detailed review while pronouncing the word benefit/advantage as the benefit of the doctor/patient. Some physicians used the word defensive as a substitute for positive defensive medicine.
Considering the definitions and words used by the physicians, the definition of positive defensive medicine can be constructed as follows: ‘The practices such as the requirement of extra examination and consultation by the physician to legally strengthen his/her defence, hospitalisation of the patient, and receiving signed approvals from the patient to strengthen physician’s legal defence taking into account the benefit of physician and patient’.
Negative defensive medicine (avoidance behaviour): The participants were asked to identify negative defensive medicine.
The practices that the physicians talked about most in the context of negative defensive medicine were avoiding, not doing and directing. All related practices involve caring for the patient as little as possible and not taking responsibility under legal limits rather than interfering with the patient. However, physicians used the risk word quite often, so it is possible to say that the basis of negative defensive medicine practices is based on risk perception.
Taking into account the definitions put forward by the physicians and the words that they often use in said definitions, negative defensive medicine can be defined as ‘an effort by the physician to avoid possible legal and medical risks by taking less initiative of medical intervention and/or referring the patient.’
Defensive Medicine Practices
The study asked the physicians: ‘What practices do physicians perform within the scope of defensive medicine?’ In line with the physicians’ answers and the information in the literature, two main themes—positive and negative defensive medicine practices—have emerged. A total of 12 codes were drawn up under these themes.
Within the scope of positive defensive medicine, the participants’ practices are coded as imaging, hospitalisation, invasive procedures, consultations, examinations, more open communication with the patient and obtaining consent, patient registration, personal registration, and prescribing medication. Because physicians do medical actions more than are legally required, they are evaluated within the scope of defensive medicine.
As seen in Table 1, the most common practice of positive defensive medicine expressed by physicians was asking for extra examination. The implementation of extra examinations was followed by requesting extra imaging and consultations.
Defensive Medicine Practices.
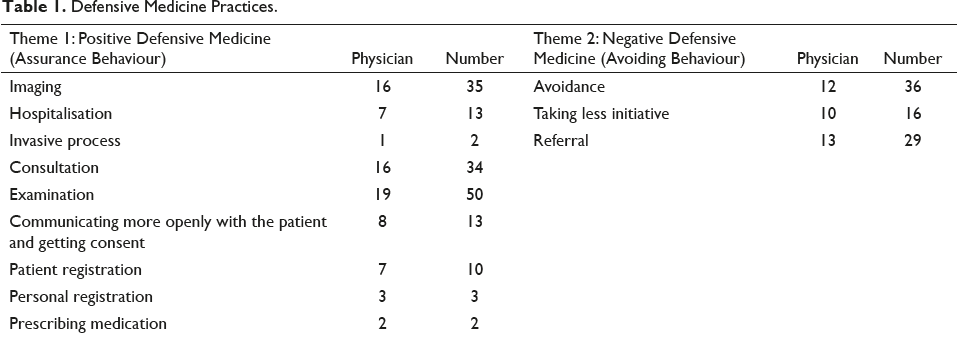
The practice of negative defensive medicine consists of three codes. These codes include avoiding, taking less initiative and referring a patient. When the number of physicians referring to the codes and the frequency of referring were examined, it was observed that physicians talk about mostly the application of referring patients within the scope of negative defensive medicine. This practice is followed by avoiding the patient and taking less initiative.
The Antecedent of Defensive Medicine
The answer to the question ‘Why do physicians need defensive medicine?’ was sought under this heading. With this question posed to the physicians involved, the factors leading to the practice of defensive medicine were sought (Table 2). The factors were divided into three themes, namely patient-related, physician-related and health sector-related factors, as a result of this study. There were 14 codes under these themes.
As detailed in Table 2, the antecedent related to the physicians consists of the personality of the physician, fear of violence, medical education, the willingness to protect the reputation of the physicians, the willingness to meet patient expectations, the changing standards of care, reasons related to their colleagues and the changing relationship between the patient and physician. When the aforementioned causes mentioned by the physicians were examined, it was observed that the most commonly mentioned antecedent was fear of violence. Fear of violence was followed by the antecedent of the physician’s personality.
The Antecedents of Defensive Medicine Practices.
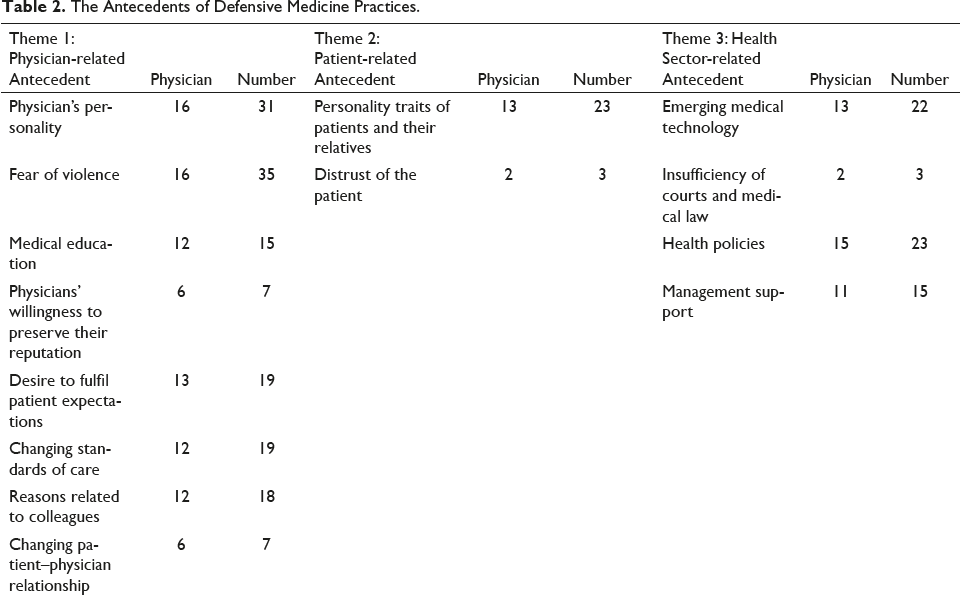
The patient-related antecedent theme includes the risks that the physician perceives regarding the patient. Physicians can use defensive medicine to eliminate possible negative consequences due to these perceived risks. The sources of the perceived risks related to the patient consist of the personality characteristics of the patient, the patient’s relatives and the patient’s distrust of the physician. Among the patient-related antecedent, the one that was the most commonly mentioned by physicians was the antecedent of the personality traits of the patient and the patient’s relatives.
The theme of health sector-related antecedent states that defensive medicine is affected by changes, developments, irregularities and deficiencies in the health sector. The codes under this theme are the evolving medical technology, the inadequacy of the courts and medical law and the support of health policies and management. Among the antecedent related to the health sector, physicians are most concerned with health policies. This antecedent is followed by ‘evolving medical technology’ and ‘not feeling the support of management’.
Outcomes of Defensive Medicine Practices
The findings regarding the answers to the question ‘What are the outcomes of defensive medicine?’ can be seen in Table 3. The physicians’ responses were distributed across three themes the outcomes for the physician, the outcomes for the patient and the outcomes for the health system. There are a total of 16 codes under these themes.
Outcomes of Defensive Medicine.
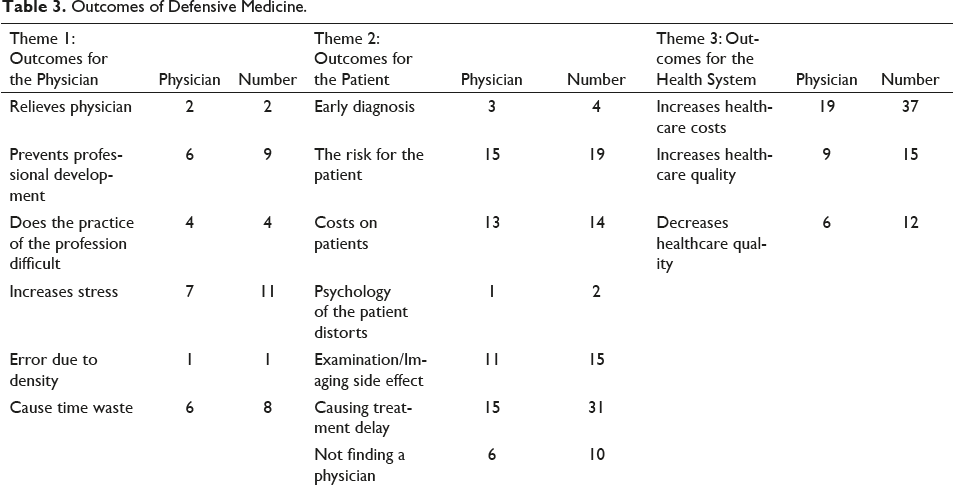
The outcomes of defensive medicine are composed of the codes as it relaxes the physician, prevents the professional development of the physician, makes it difficult for the physician to perform his/her profession, causes stress in physicians and causes errors due to intensity and time loss. When we look at the frequency of the codes mentioned by physicians, it can be seen that physicians mention the code for causing stress the most. These outcomes are followed by the outcomes ‘defensive medicine prevents the professional development of the physician’ and ‘causes loss of time for physicians’.
The outcomes of defensive medicine for the patient include the following codes: ‘it provides early diagnosis, creates risk for the patient, imposes costs on the patients, deteriorates the psychology of the patient, causes side effects of examination/imaging for the patient, causes a delay of treatment and causes the patient to be unable to find a physician’. It can be observed that as an outcome of defensive medicine from the patient’s point of view, physicians refer mostly to the code that causes a delay in treatment, followed by the codes that it creates risk for the patient and impose an extra cost for the patients.
In the theme describing the outcomes of defensive medicine in the health system, codes state that it increases the cost of health services, improves the quality of health services and decreases the quality of health services. When these results were examined, it was found that physicians are very concerned about the outcome, whereas defensive medicine increases the cost of health services. The positive or negative effect of defensive medicine on the quality of health services differs from situation to situation, which is another outcome of defensive medicine regarding the health system.
Discussion
Defensive medicine has similar and different aspects when the definitions in the literature are considered. The definitions made in this study consist of the words used in the definitions made by physicians who have experienced defensive medicine directly. Based on the results obtained from the interviews, the practice of defensive medicine was described as
the fear of missing important findings by physicians, the desire to be error-free, the desire to prevent possible complaints from patients and/or their families, the fear of violence and the fear of involvement in malpractice cases, requesting extra tests and examinations, following unnecessary procedures, requesting extra consultations with the fear of violence and fear of interfering with the malpractice case, hospitalizing the patient more than necessary or avoiding risky patients and risky diagnosis/treatment methods.
Considering the definitions made by the physicians, the definition of positive defensive medicine is as follows: ‘Considering the physician’s benefit and patient benefit, these are the practices that include excessive service provision such as requesting extra examination and extra consultation, hospitalizing the patient, obtaining a signed consent from the patient to strengthen his defence.’ Negative defensive medicine practices are defined as ‘an effort by the physician to avoid potential legal and medical risks by taking less initiative and/or referring the patient.’
According to the physician-related antecedent obtained as a result of this qualitative research, it was concluded that the most important antecedent was the fear of malpractice cases. This antecedent was the most mentioned in the literature due to its effect on defensive medicine (Catino, 2011; Toraldo et al., 2015). Another antecedent similar to the fear of being sued is the fear of being complained about and the patient’s complaint being made through a phone call. This antecedent is suggested by many of the studies we have examined (Toraman & Çarıkçı, 2019; Yeşiltaş & Erdem, 2018). In line with the definitions in the literature, this study also shows that the most important antecedents of defensive medicine are fear of lawsuits and complaints. Besides, the fear of having to pay compensation as a result of the processes of the lawsuit or complaint was found to be another reason why physicians act defensively. It is stated in the literature that possible cases cause serious financial burdens and that the physician applies defensive medicine to avoid this form of financial burden (Sclar & Housman, 2003). Another antecedent that may be referred to as an aftershock of this antecedent is a foregoing complaint/lawsuit process that a physician has experienced. According to this antecedent, physicians who have been through the difficult process of either a complaint or a lawsuit before are more defensive to avoid experiencing a similar process (Asher et al., 2012).
One of the antecedents related to physicians derived from this study that bears a similarity to the literature is the willingness of physicians to protect their reputations (Catino, 2011; Jackson Healthcare Company, 2012). Other antecedents, which are thought to be related to the antecedent of the physician’s willingness to protect their reputation, include the desire to meet patient expectations, the desire to act in the best interests of the patient, anxiety related to the competence of the physician, their fear of making a mistake and missing something, and the desire to avoid bad outcomes and risk. When all of these antecedents are evaluated together, the physician wants to act for the benefit of the patient but he/she is concerned about their competence and about making mistakes; therefore, the desire to avoid the potential risk is seen of as an important reason for the physician to behave defensively. All of these antecedents are in line with the literature and support each other (Akdur, 2013; Jackson Healthcare Company, 2012; Sánchez-González et al., 2005). Another one of the antecedents related to the physician is their anxiety about being exposed to violence. The phenomenon of widespread violence, one of the most important problems in today’s health sector, was found both in the national literature (Toraman & Çarıkçı, 2019; Yeşiltaş & Erdem, 2018) and this study as an important antecedent of the practice of defensive medicine. Accordingly, physicians practise defensive medicine to avoid confronting the patient in a lawsuit, not having an argument with the patient, and not being subjected to physical, verbal or psychological violence.
Reasons related to their colleagues are among the reasons for the practice of defensive medicine. Accordingly, physicians need to engage in defensive medicine practices for reasons such as anxiety about their colleagues criticising them, the instinct to perform in their colleagues’ antecedent, colleague orientation and the complaint processes experienced by their colleagues. Although the literature contains the finding that physicians practise defensive medicine with the influence of their colleagues (Akdur, 2013; Hossein & Mina, 2018; Jackson Healthcare Company, 2012), no direct information or findings regarding the antecedent obtained in this study were found in the literature.
In the title of the antecedent of defensive medicine related to the health sector, there are antecedents such as developing medical technology, inferior courts in terms of medical law, health policies, strict performance criteria, an insufficient health workforce, and not feeling the support of management. Although no direct findings have been found in the literature based on this antecedent, Yeşiltaş and Erdem (2018) stated that the constantly renewed health system and health policies encourage physicians to act more guardedly. Similarly, Toraman and Çarıkçı (2019) stated that rapidly changing health policies are an important antecedent in the practice of defensive medicine. In line with this information, it can be said that the results obtained from the study are similar to the results found in the literature.
The outcomes of defensive medicine and its application for physicians can be divided into positive and negative outcomes. According to the results of this study, the only positive outcome of defensive medicine for physicians is that physicians can relax in both the medical and legal sense. Accordingly, physicians who practice defensive medicine feel more confident. This is a positive result. Similar to this finding, Akdur (2013) stated that defensive medicine protects the physician from legal responsibilities. This information and the results of this study support each other. When we look at the negative results of defensive medicine in terms of physicians, it is stated that legalities make it difficult for physicians to perform their profession. This negatively affects the professional development of the physician, causes stress, increases the intensity of their work, causes errors due to aid increased intensity and results in a time deficit. It is clear from these results that physicians who apply defensive medicine practices to protect themselves may legally face more risks as a result. However, these practices make it difficult to perform the profession of medicine, thus causing physicians to experience rustiness and stress. Yeşiltaş and Erdem (2018) found that defensive medicine practices cause burnout in physicians. This supports this view.
When the results of the defensive medicine applications were examined, two types of outcomes emerged, namely positive outcomes for patients and negative outcomes for patients. According to the physicians’ opinions, although rare, the early diagnosis of some diseases is seen as a positive result for the patients after extra examinations are applied within the scope of defensive medicine. Many studies in the literature support these results (Passmore & Leung, 2002; Studdert et al., 2005; Tancredi & Barondess, 1978). In contrast, physicians have stated that defensive medicine results in more harm than good for patients. Some of the physicians stated that defensive medicine poses a risk to the patient, can cause the psychology of the patient to deteriorate, can cause side effects due to the examinations, can cause a delay in treatment, can cause the patient to not find a physician and impose extra costs on the patients. Studies in the literature suggest that defensive medicine involves several risks for patients (Fronczak, 2016; Tancredi & Barondess, 1978) and imposes extra costs on patients (De Ville, 1998). In this respect, the findings of the qualitative research carried out within the scope of this study are in parallel with the literature.
Another result of this study is that defensive medicine has positive and negative consequences for the health system. The result that defensive medicine will increase the quality of health services constitutes a positive outcome due to defensive medicine. Tancredi and Barondess (1978) and Passmore and Leung (2002) argue that positive defensive medicine practices will positively impact the quality of the healthcare that the patient receives, depending on the situation. Accordingly, providing extra health services within the scope of defensive medicine provides marginal benefits. Practices such as explaining the patient’s condition in more detail or keeping detailed records improve the quality of health services (Studdert et al., 2005; Summerton, 1995). Some physicians stated that defensive medicine increases the quality of health services as well as physicians who stated that it might have the opposite effect. It is stated in the literature that the failure to provide services that should be provided due to the practice of negative defensive medicine may result in a substandard level of healthcare provision (Tancredi & Barondess, 1978). In this case, the quality of the offered service will inevitably decrease. The physicians expressed that unnecessary practices within the scope of defensive medicine increase the health system’s overall cost. The most commonly cited outcome of defensive medicine in the literature is that it increases the cost of healthcare. For example, Kessler and McClellan (1996) stated that 5%–9% of health expenditure in the United States consists of practices tied to defensive medicine. Sethi et al. (2012) stated that defensive medicine practices applied in orthopaedics due to legal liability concerns cost an average of $2 billion annually. The studies in the literature and the results obtained from our research support each other.
One of the results obtained in this study was determining what actions are undertaken within the scope of defensive medicine. Accordingly, the actions that physicians refer to within the scope of defensive medicine include requesting medically unnecessary imaging, communicating with the patient more clearly, obtaining specific consent, unnecessary hospitalising, unnecessary invasive procedures, unnecessary consultations, requesting extra examinations and tests, keeping detailed patient records, avoiding risky patients and cases, taking the initiative less, referring the patient to another health professional and prescribing extra medication. These actions align with the literature (Brateanu et al., 2014; Göcen et al., 2018; Ortashi et al., 2013; Osti & Styrer, 2015; Reisch et al., 2015). Some authors consider the practice of prescribing medicine to be negative defensive medicine (Summerton, 1995), and others perceive it as positive defensive medicine (Toraman & Çarıkçı, 2019). In this study, prescribing extra medicine was evaluated within the scope of positive defensive medicine due to the statements of the physicians and the provision of extra services being tied into positive defensive medicine practices, as mentioned earlier.
Conclusion and Recommendation
This study has concluded that the anxiety related to the risk of complaints and lawsuits, the pressure of phone lines specifically for patient complaints, the anxiety of being exposed to violence, and the lack of support from management and the media are very important considerations related to defensive medicine. Accordingly, studies need to be done to eliminate these intense concerns. This may lead to a decrease in defensive medicine practices, thus positively affecting the health system.
Researchers who plan to conduct qualitative research on defensive medicine are advised to conduct in-depth interviews on preventing defensive medicine practices.
Footnotes
Acknowledgements
This study was developed by Özgün Ünal’s PhD thesis and fully supported by the Scientific Research Projects Unit [2018-2-9-212] from Sakarya University.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical approval of the study was obtained from Sakarya University Ethics Committee with a letter dated 31.01.2018 and numbered E.5438. This study does not contain any clinical studies with human participants or animals performed by any of the authors.
Funding
This study is supported by the Scientific Research Projects Unit [2018-2-9-212] from Sakarya University.