
Abstract
In the most general sense, defensive medicine practices are the answer to the concerns that physicians have. Defensive medicine practices can affect physicians, patients and the health system and, as a result, the whole of society, positively or negatively. Therefore, it is important to conduct detailed studies on defensive medicine practices. This study was carried out to conduct a systematic review of the pre-existing studies on defensive medicine practices. Information on the definition of defensive medicine practices, the antecedents of defensive medicine practices and the results of defensive medicine practices was sought. This also constituted the inclusion criteria. The study was carried out following the PRISMA systematic review protocol. In the study, Google Scholar was used as a scanning engine to scan all literature. Articles written in either Turkish or English were included in this study. Relevant information was compiled from the articles included in the study. The information obtained was coded into the NVivo programme, and content analysis was done. As a result, information on the definition of defensive medicine practices, the antecedents of defensive medicine practices and the results of defensive medicine practices was compiled and presented comprehensively. It is thought that this study will compile a new body of literature on defensive medicine practices and integrate the information related to defensive medicine practices, in addition to its precursors and results, to see how the information differs across the studies and contributes to the literature.
Keywords
Introduction
Nowadays, some of the factors that apply pressure to healthcare workers can be observed in the health sector such as the general policies of the government, health policies, media, social media, patients, patients’ relatives and the healthcare professionals themselves. There are many individual and professional reactions that physicians may have to the pressure they are feeling. One of the responses is defensive medicine practices. In the literature, the most commonly used definition of defensive medicine is ‘Definitions of defensive medicine differ, but most include the practice of ordering extra tests and procedures primarily in response to a perceived threat of a future medical malpractice claim’ (OTA, 1993, p. 6). Based on this definition, which is frequently used in the literature, some conclusions can be drawn. The most important of these conclusions imply that physicians feel some anxiety and resort to unnecessary medical practices to face these concerns. These practices may have either positive or negative effects on the patients, physicians and the health system as a whole. It is important to evaluate the effects of these results, and more detailed information about defensive medicine practices is important in the present study. In the literature, there are several studies on defensive medicine practices. When these studies were evaluated, similar situations are expressed in different ways. Besides, there is no consensus in terms of the information on the reasons for the physicians’ use of defensive medicine practices. Diverse results have been obtained from different studies. Similarly, the results of defensive medicine practices have not been investigated in detail yet. Following the evaluation of the results obtained from the studies, inferences about ‘what kind of results defensive medicine practices may produce’ can be accomplished. It is thought that the information about the antecedents and results of defensive medicine practices in the literature should be examined in depth. Therefore, it is aimed to make a systematic review of the studies in the literature on defensive medicine practices in the present study.
Method/Protocol
The study was carried out based on the criteria set out using the PRISMA protocol (Shamseer et al., 2015). According to PRISMA, the following steps have been followed.
Research Questions
In this research, the answers to the following questions are sought:
How are defensive medicine practices defined? What are positive and negative defensive medicine practices? What are the antecedents of defensive medicine? What are the results of defensive medicine?
Information Sources and Search Strategy
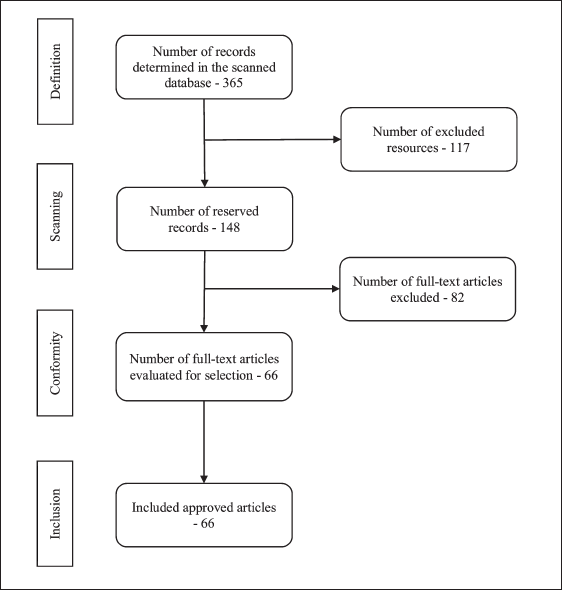
The first studies on defensive medicine practices date back to the 1970s. The research, which was essential for the development of the literature, was carried out between 1970 and 2020. However, the number of studies on defensive medicine practices is very limited. For this reason, the resources used in this study are not limited to any one database. We used resources obtained from Google Scholar, which could scan all databases. In the process of determining the resources found in Google Scholar, the original form of the terms ‘defensive medicine’ and ‘defensive practices’ were used synonymously as keywords. The resources of the study were searched in both English and Turkish. The document selection process for the systematic review is shown in Figure 1.
Flow Diagram of the Systematic Compilation Process.
Eligibility Criteria
The resources used in this research had the following criteria:
Inclusion criteria
The concepts of ‘defensive medicine’ and ‘defensive practices’ in the database are contained in the title of the studies. Open access to both Turkish and English studies. In the study, the information should be on defensive medicine ‘positive defensive medicine and negative defensive medicine’, what the positive and negative defensive medicine practices are, what the antecedents of defensive medicine practices are and what the results of defensive medicine practices are.
Selection Process
The researchers of the included studies should meet the above criteria, and they were compiled independently from each other. Possible mistakes were prevented, and the researchers were checked. Besides, the studies were recorded with titles to avoid possible repetition. In this way, it was possible to compare the studies compiled by the researchers independently from each other and a consensus was reached.
Data Collection Process
The first researcher examined the studies that were planned to be included in the research and the following was compiled from the studies: Title Author(s) Year Method Definition of defensive medicine Definition of positive defensive medicine Definition of negative defensive medicine Defensive medicine practices Positive defensive medicine practices Negative defensive medicine practices Antecedents of defensive medicine Results of defensive medicine
The second researcher checked for any missing or incorrect information by examining the relevant studies and the information compiled by the first researcher.
Data Management and Analyses
Special software was not used to save the articles. Instead, the information compiled from the related articles in line with the criteria created by the researchers was tabled in Microsoft Excel. As a result of the analysis, the defensive medicine practices, positive defensive medicine practices and negative defensive medicine practices definitions, the defensive medicine practices with their antecedents and results were revealed. The obtained information was transferred to the NVivo 12 programme and content analysis was conducted using the codes given below.
Country
Year
Method
Defensive medicine
Positive defensive medicine
Negative defensive medicine
Positive defensive medicine practices
Negative defensive medicine practices
Antecedents
Results of defensive medicine
Results
As a result of the systematic review, the obtained information and content analysis results have been included in this study. The results were evaluated in four main ways: (a) The definition of defensive medicine, the definition of positive defensive medicine and the definition of negative defensive medicine; (b) defensive medicine practices (positive and negative); (c) antecedents of defensive medicine and (d) the results of defensive medicine.
Definition of Defensive Medicine
The studies in the literature were carried out between 1972 and 2020. Defensive medicine practices have been defined in 40 studies. When these definitions were evaluated (Appendix A), the definitions are similar while also having different aspects. Generally, the declared meanings were commonly observed in this study. Defensive physicians offer extra procedures to their patients or they avoid the patient out of fear. When these definitions were evaluated, defensive medicine practices are generally applied due to the anxiety of malpractice and the fear of patient avoidance. Due to concerns about the physician’s feelings, it can be seen that they either offer extra procedures to the patients (extra imaging, testing, hospitalisation, medication, documentation, visits, etc.) or they avoid serving the patient (not accepting the patient, providing a referral, etc.). As an important conclusion observed from the definitions, physicians can apply these procedures to protect themselves.
As a result of the analysis of the definitions, the most frequently used words in the definitions were ordering, procedures, test, malpractice, avoid, lawsuits, litigation, protect and unnecessary. All of the words and definitions define the attitudes and behaviours of the physicians as malpractice anxiety. This can manifest as requesting extra tests, examinations and consultations (no marginal benefit for the patient) and avoiding risky patients and risky diagnostic treatment methods to avoid possible cases and criticism.
Positive defensive medicine practices have been described in 23 studies in the literature (Appendix A). A word cloud of definitions was created. According to the word cloud, the words ordering, additional, test, diagnostic, liability, malpractice, marginal and lawsuit were determined to be the most common in the definitions. These words indicate that physicians resort to these practices with concerns such as legal or malpractice anxiety, including the practice of extra service provision. Word cloud results show that these applications have low potential to benefit.
The definition of positive defensive medicine practices that can be made by considering the definitions in the literature and the most used words in the definitions: Positive defensive medicine practices include physicians applying extra diagnostic methods (requesting extra testing and imaging, following invasive procedures) and providing services with very low marginal benefits (hospitalisation, prescribing drugs, etc.) in order to fulfil legal responsibilities and malpractice anxiety.
In the literature, negative defensive medicine practices were defined in 23 different studies (Appendix A). When these definitions were evaluated, physicians apply negative defensive medicine practices to remove themselves from risk. It was also stated that physicians do not accept risky patients and avoid risky diagnoses and treatment methods. When the word cloud of definitions in the literature was evaluated, it was seen that some of the most used words in the definitions are avoidance, high-risk, procedures, treatments, refuse, withdrawal, fear and malpractice.
Considering the word cloud results obtained from the definitions from the studies, negative defensive medicine practices can be defined as the physicians’ refusal to apply treatments that may be beneficial for the patient due to the fear of malpractice anxiety and to avoid risky patients and cases.
Positive and Negative Defensive Medicine Practices
In addition to the definitions of defensive medicine practices, defensive medicine practices have been discussed in many studies. However, the studies do not show a precise consensus of positive and negative defensive medicine practices. For this reason, compiling the positive and negative defensive medicine practices information from the literature will contribute to the literature.
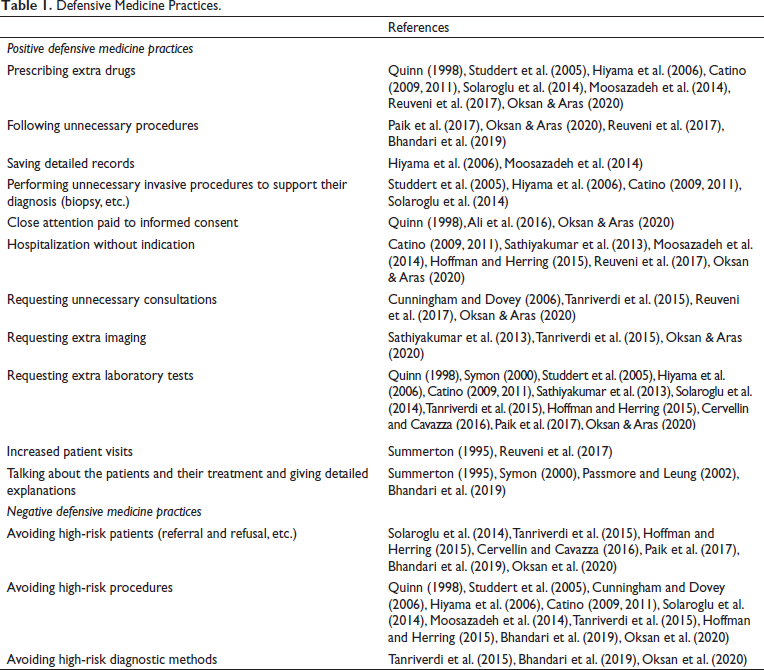
In the literature, the research on defensive medicine has been emphasised in the studies conducted between 1993 and 2020 (Appendix A). Twenty-two studies referring to positive defensive medicine practices and 16 studies referring to negative defensive medicine practices were identified. Positive defensive medicine practices and negative defensive medicine practices are shown in Table 1.
Defensive Medicine Practices.
The Antecedents of Defensive Medicine Practices
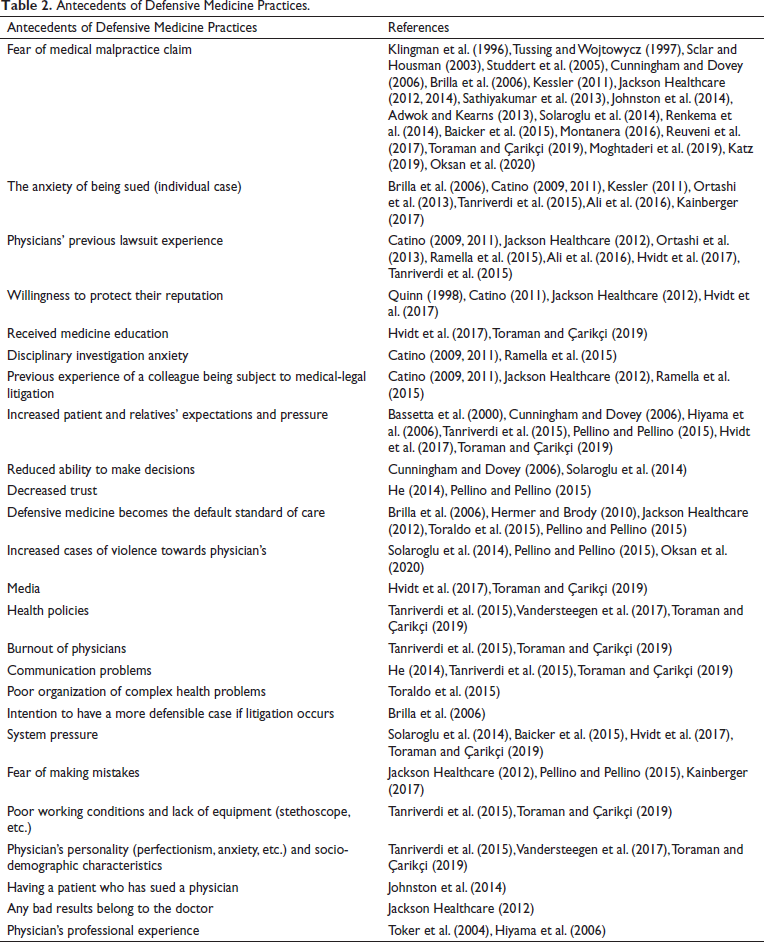
Based on the chosen studies, the question of why physicians apply to defensive medicine practices is commonly due to malpractice anxiety. Malpractice anxiety undoubtedly affects the physician’s practice of defensive medicine. However, it is not sufficient to explain why physicians apply defensive medicine practices. When the literature is evaluated, it is seen that there are other premises which are emphasised in different studies. So, it is important to compile these premises and look at the causes of defensive medicine practices from an extensive perspective. According to the word cloud, using the premises discussed in 48 studies in the literature, the most frequently used words were malpractice, fear and litigation. Physicians’ fear of malpractice cases is seen as the most important antecedent of defensive medicine. In addition to malpractice anxiety, the antecedents of other defensive medicine practices that have been discussed in the literature are as follows (Appendix A).
While the defensive medicine antecedents are listed in Table 2, it is seen that defensive medicine not only results from malpractice or fear of litigation but also many other reasons lead physicians to act defensively.
Antecedents of Defensive Medicine Practices.
Results of Defensive Medicine Practices
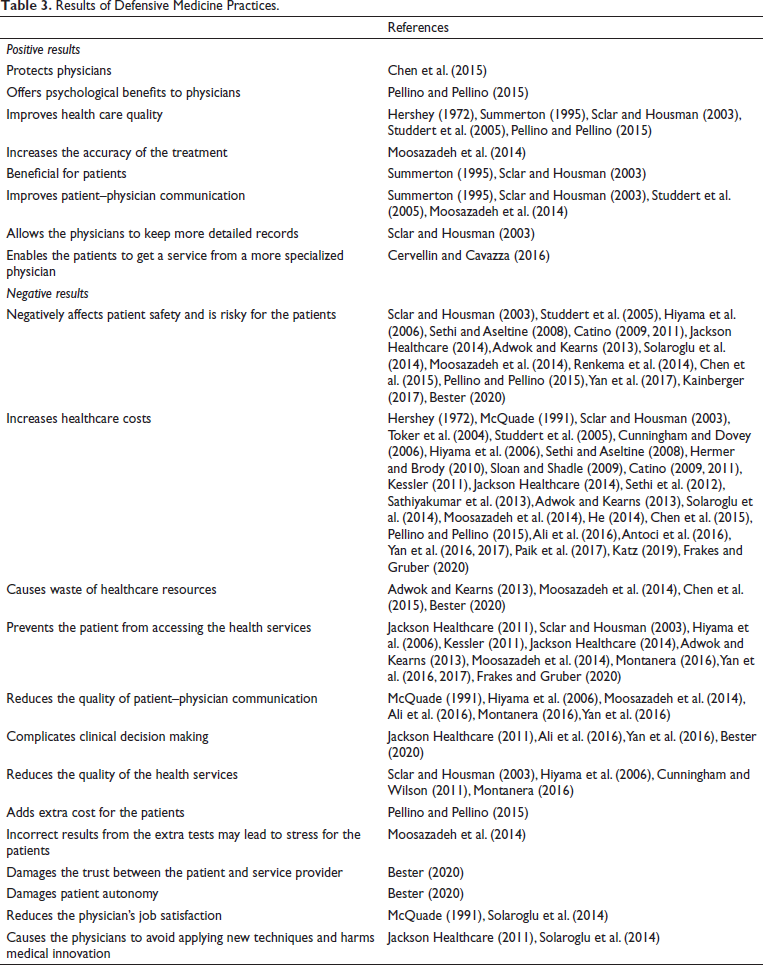
The results of defensive medicine practices have been discussed in 37 studies. The most frequently used words in these studies were harm, risk, quality, costly, relationship, communication and radiation. According to the literature, defensive medicine practices are determined as follows: cost-increasing, quality-lowering and risk-creating applications for the patients. Defensive medicine practices, referring to those compiled from the collected studies, have positive and negative consequences. The positive and negative results of defensive medicine practices are shown in Table 3.
Results of Defensive Medicine Practices.
Discussion
The present study was carried out to conduct a systematic analysis of defensive medicine literature. As a result of the review, four inferences were made. The first inference is about the definition of defensive medicine practices. As previously mentioned, defensive medicine practices have been defined in many studies. These definitions contain some similarities and some differences. According to the literature (Catino, 2009; He, 2014; Hershey, 1972; Montanera, 2016; Paik et al., 2017), defensive medicine practices are about either extra applications of treatment to the patient or the avoidance of the patient. From the definitions, it may be said that there is a consensus on this issue. On the other hand, a consensus was not reached regarding the definitions of why defensive medicine was applied. In this study, the wider definition created by analysing the definitions in the literature minimises the differences and appears to cover all definitions. According to this review, defensive medicine can be defined as ‘Defensive medicine is physicians’ attitudes and behaviours like asking for extra tests and examinations, following unnecessary procedures, requesting extra consultations, hospitalising the patient more than necessary, or avoiding risky patients and risky diagnostic treatment methods in order to protect physicians from malpractice anxiety, possible cases and criticism’.
When the literature was evaluated, it was seen that there are two types of application: positive defensive medicine practice and negative defensive medicine practice. Based on the definitions of positive defensive medicine in the literature (see Appendix A), positive defensive medicine can be defined as follows: ‘Physicians resorting to extra diagnostic methods to lessen their malpractice anxiety and proving to the legal authorities that they can fulfil their responsibilities. It also provides the patients with services with a very low marginal benefit (hospitalisation, prescribing drugs, etc.)’.
Based on the definitions of negative defensive medicine in the literature (see Appendix A), negative defensive medicine can be defined as follows: ‘Physicians’ avoiding risky patients and cases, refusal to apply treatments that may be beneficial for the patient due to a fear of malpractice and a fear of being sued.’
As a result of the systematic review, there is information in all the chosen studies about defensive medicine practices (see Table 1). According to some studies, positive defensive medicine practices involve prescribing extra medication (Passmore & Leung, 2002; Studdert et al., 2005), following unnecessary procedures (Antoci et al., 2016; Paik et al., 2017), keeping detailed records with a long retention (Çalıkoğlu & Aras, 2020; Summerton, 1995), performing unnecessary invasive procedures to support the diagnosis (Catino, 2009; Hiyama et al., 2006; Studdert et al., 2005), paying close attention to obtaining informed consent (Cunningham & Dovey, 2006; Tanriverdi et al., 2015), hospitalisation without indication (Catino, 2011; Hoffman & Herring, 2015), requesting unnecessary consultations (Çalıkoğlu & Aras, 2020; Reuveni et al., 2017), requesting extra imaging (Sathiyakumar et al., 2013; Solaroglu et al., 2014), requesting extra laboratory testing (Adwok & Kearns, 2013; Cervellin & Cavazza, 2016), increased follow-up (Moosazadeh et al., 2014; Reuveni et al., 2017) and providing more detailed explanations about the disease and treatment for the patients (Çalıkoğlu & Aras, 2020; Passmore & Leung, 2002). When these applications are examined, it can be seen that they are applications that are not cost-effective in general. They add extra costs to both the patient and the health system.
Negative defensive medicine practices are described as avoiding high-risk patients (Bhandari et al., 2019; Paik et al., 2017), avoiding high-risk procedures (Catino, 2011; Paik et al., 2017) and trying to avoid high-risk diagnoses (Hiyama et al., 2006; Studdert et al., 2005). Although the direct cost of these applications is limited, it should be taken into consideration that the indirect costs such as late treatment, death and limb loss will be high due to the lack of service overall (see Table 1).
In the literature, prescribing unnecessary drugs is considered to be a negative defensive medicine practice in some studies (Bhandari et al., 2019; Cunningham & Dovey, 2006; Summerton, 1995). It is also considered to be a positive defensive medicine practice in others (Çalıkoğlu & Aras, 2020; Catino, 2009, 2011; Moosazadeh et al., 2014; Tanriverdi et al., 2015). It is, therefore, useful to evaluate the context and application before deciding whether prescribing extra medication is negative or positive defensive medicine. According to this subject, while prescribing drugs to the patients is done instead of avoiding the patient, they offer a treatment that there is little or no need for. Considering the definition of negative and positive defensive medicine practices, providing extra services to the patient is within the scope of positive defensive medicine practices. According to this, it may be thought that it is more accurate to evaluate extra drug prescribing practices within the scope of positive defensive medicine.
Another result of the study is ‘why doctors resort to defensive medicine practices’. Although it is stated that physicians apply defensive medicine practices out of certain anxiety related to malpractice, being sued and not being criticised, there are different antecedents of defensive medicine in the definitions found in the literature. However, the number of studies supporting the antecedents of defensive medicine practices with empirical findings is quite limited. In this regard, Catino’s (2011) and Jackson Healthcare’s (2012) studies have come into prominence. In these studies, the fear of being sued was found to be the most important precursor of the physician’s use of defensive medicine practices. However, the anxiety of being sued is not sufficient alone to explain defensive medicine (see Table 2).
Another important result of this study is the ability to respond to the results of defensive medicine practices. No study in the literature evaluates the results of defensive medicine practices and supports them with either quantitative or qualitative findings. In contrast, different studies focus on the possible consequences of defensive medicine. In the literature, some researchers claim that it is beneficial for patients and some researchers draw attention to the negative consequences of defensive medicine (see Table 3). Within the scope of defensive medicine, physicians keep their records more regularly and attentively, strengthening their hand in case of possible complaints (Catino, 2011; Passmore & Leung, 2002; Summerton, 1995). Regular health records provide important advantages such as providing reliable health information, strengthening the patient–physician communication and supporting clinical decisions (Tang et al., 2006).
The fact that physicians follow up with their patients more frequently may affect the patient’s emotions and treatment. This results in a positive response and reduces the risk of the physician being sued (Hauser et al., 1991). The efforts of physicians also have some positive results in that they allocate more time to their patients and provide a detailed explanation within the scope of defensive medicine. According to Schwartz (2016), patients may tend to sue their physicians when they are afraid, disappointed and not properly informed. A defensive physician is a physician that enables their patients to understand the diagnosis, who listens to the patient’s concerns and where informed consent is an opportunity to answer the patient’s questions (Schwartz, 2016).
Within the scope of positive defensive medicine, applications such as an extra examination request may provide several benefits for the patients (Perry, 2013; Studdert et al., 2005). It is also possible to diagnose diseases that are likely to escape a single examination through the demand for extra diagnoses and examinations (Vandersteegen et al., 2017). Besides, the delivery of difficult cases to other physicians or hospitals within the scope of negative defensive medicine care is another factor that may increase the quality of the health services (Cervellin & Cavazza, 2016; Studdert et al., 2005). Therefore, the referral of the patient to another physician or institution may provide benefits as a factor that increases the technical quality of the provided service.
The most emphasised matter in the literature about the negative results of defensive medicine is the increase in the cost of the health services overall (Ali et al., 2016; Sethi et al., 2012). It is obvious that the payments for defensive medicine procedures include the excessive and/or unnecessary use of the health services. Therefore, one of the harms associated with defensive medicine is the increase in the cost of health services. Defensive medicine is a waste of resources devoted to the health services and it is a threat to the sustainability of the health system for all nations. Another issue that was stated in the literature is that defensive medicine has negative results within the scope of negative defensive medicine practices. In negative defensive medicine, physicians seek to avoid risky procedures and risky patients; this reduces or completely blocks access to health services. In this situation, the patients are deprived of health services that may be beneficial for them.
Another negative side of defensive medicine is that the excessive use of medical services may reveal a higher risk of mortality and morbidity (Cervellin & Cavazza, 2016; Yan et al., 2016). For example, excessive imaging causes unnecessary radiation exposure. Thus, it may cause an allergic reaction in the short term and radiation-related diseases in the long term (Cervellin & Cavazza, 2016; Sethi & Aseltine, 2008). A study performed by Studdert et al. (2005) stated that unnecessary invasive procedures may pose a threat to the patient’s health, while false-positive results and uncertain findings can both lay the ground for additional interventions and may negatively affect the psychology of the patient.
Results
The presented study has been re-defined more comprehensively using defensive medicine literature referring to the positive and negative defensive medicine practice points. The positive and negative defensive medicine practices have been compiled, and a guide for defensive medicine practices has been created for use by future studies. Another study result provides comprehensive information on the antecedents of defensive medicine practices. In conclusion, it is thought that the information obtained from the literature will contribute to defensive medicine practices in terms of understanding the importance of the topic.
Limitations
An important limitation of this systematic review study was that non-accessible resources were not used. However, it is important to evaluate all studies in a comprehensive literature review to the best of the researchers ability.
Supplemental material
Supplemental material is available for this article online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.