
Abstract
Susceptibility to smoking is a reliable predictor of smoking initiation. This article describes its prevalence and associated factors among Malaysian school adolescents. Data were obtained from the Global School-Based Student Health Survey (GSHS) 2012, a nationwide representative sample of school adolescents. The overall prevalence of susceptibility to smoking was 6.0% and significantly higher among males (9.5%) compared with females (3.6%). Multivariable analyses revealed that males (adjusted odds ratio [aOR] 3.34, 95% confidence interval [CI] 2.70-4.18) and school adolescents of indigenous Sabahan or Sarawakian descents (aOR 1.62, 95%CI 1.21-2.18) were significantly more likely to be susceptible to smoking. Susceptible school adolescents had a slightly higher likelihood to have symptoms of stress (aOR 1.31, 95% CI 1.02-1.70), anxiety (aOR 1.19, 95% CI 1.01-1.40), depression (aOR 1.56, 95% CI 1.25-1.96), including those whose one or both parents/guardians were smokers (aOR 1.48, 95% CI 1.21-1.82; aOR 2.33, 95% CI 1.22-4.44, respectively). The findings from this study point out the need for proactive measures to reduce smoking initiation among Malaysian adolescents with particular attention toward factors associated with susceptibility to smoking,
Introduction
Smoking is a habit that is learnt and initiated during adolescence. 1 The earlier an individual starts smoking, the higher the risk in contracting smoking-related illnesses. Male and female adolescents who started smoking before the age of 15 years had twice the risk to develop lung cancer compared with those who started at age 20 years or more. 2 At the same time, those who initiated smoking during adolescence were more prone to become heavy smokers in their adulthood and would continue smoking for a long time before successfully quitting. 3 Hence, reducing the incidence of smoking initiation is one of the long-term measures to reduce smoking prevalence and health consequences associated with cigarette smoking.
The identification of adolescents susceptible to smoking is the prerequisite for reducing smoking initiation among them. The concept “susceptibility to smoking,” which is the lack of cognitive commitment to not smoke in the future is recognized as a reliable predictor of smoking habit among adolescents. 4 This has been proven through local and international research. Difranza et al 5 reported that adolescents who were susceptible to smoking were 2 to 3 times more likely to become experimental smokers. Meanwhile, among elementary school students, Jackson 1 reported that cognitive susceptibility was the main predictor of smoking initiation after 2 years. Pierce et al 4 reported that susceptibility to smoking was the main independent variable that contributed to smoking compared with other independent variables such as smoking among family members (father or brothers) and peer smoking. Local research carried out by Lim et al 6 among secondary school adolescents aged 13 to 17 years in Kota Tinggi district revealed that nonsmoking adolescents who were susceptible to smoking were 3.7 times more likely to initiate smoking after a year compared with those who were not susceptible.
The identification of adolescents susceptible to smoking and its associated factors would enable efficient allocation of resources for prevention. Among other factors, female adolescents, having peer and family smokers, and positive expectations about smoking were reported to have associations with susceptibility to smoking.7 -9 However, these findings are not consistent and are based on Western populations. Social and cultural differences may render them unsuitable in the Malaysian context. Moreover, only a few Western studies have looked into associations between susceptibility to smoking and cognitive factors, such as stress, anxiety, and depression.10,11 Although a study on susceptibility to smoking has been done in this country, it only involved adolescents from a single district and majority of them was from a single ethnic group. 6 Thus, the findings from the study cannot be generalized to all adolescents in Malaysia. This article aims to fill the knowledge gap on prevalence, inter- and intrapersonal and cognitive factors (stress, anxiety, and depression) related to “susceptibility to smoking” in a representative sample of secondary school adolescents in Malaysia.
Methods
Sampling Procedure
This cross-sectional national survey among school adolescents was conducted from February to April 2012. The sample was selected using a 2-stage stratified cluster sampling to produce a representative sample of school adolescents in form 1 to form 5, aged 12 to 17 years. The sampling frame was all secondary schools under the Malaysia Ministry of Education. The first stage was selection of school in proportion to school enrollment and the second stage was the selection of classroom from the selected school. All school adolescents from the selected classroom were eligible to participate in the study. A total of 234 schools and 28 732 respondents were selected to participate in this survey. 12
The survey instrument used was a questionnaire adapted from Global School-Based Student Health Survey, World Health Organization, 13 which was translated into Malay, and validated by a research panel. The questionnaire was self-administered. Prior to data collection, trained research assistants explained in detail to the selected respondents regarding the survey, namely, its objectives, voluntary participation, confidentiality, and the content of the questionnaire. Any doubts were clarified by the research team members. Completed questionnaires were collected and sealed in front of the respondents. Only respondents who obtained written consent from their parents/guardian were allowed to participate in this study. The survey protocol was approved by Malaysia Ministry of Education, whereas approval to recruit the students as participants was given by individual schools and their respective District and State Departments of Education. Ethical approvals were obtained from the Medical Research and Ethics Committee of Ministry of Health and Ministry of Education.
Measurements
The dependent variable in this survey “Susceptibility to Smoking” was measured using 2 questions: (a) Do you think you will smoke a cigarette in the next year? (b) If one of your best friends were to offer you a cigarette, would you smoke? The choices of answers were (a) Yes, (b) Probably yes, (c) Probably no, and (d) Not at all. If the respondent answered “Not at all” to both questions, they were categorized as “Not susceptible to smoking,” while those who gave other combinations were categorized as “Susceptible to smoking.”
The independent variables in this survey were gender, age-group, ethnicity, school sessions, parental marital status, and parental tobacco consumption. Stress, anxiety, and depression levels among respondents were measured using validated Mental Health Survey with administered Depression, Anxiety, Stress Scale (DASS 21) questionnaire in Malay. 14 The final score of each item groups (Depression, Anxiety, and Stress) was multiplied by 2. 15 Respondents who scored more than 9,8 and 15 for depression, anxiety, and stress were classified as “having the abovementioned symptoms.”
Data Management and Analysis
A total of 25 507 school adolescents participated in the survey, giving an overall response rate of 89.0%. The data on 18 870 of respondents classified as nonsmoking were analyzed using SPSS version 21. Data entry was done using scanner for DASS and GSHS. Data were weighted in the analysis to account for the complex study design and response rate. Descriptive statistics were used to elaborate the social demographic characteristics of the sample and to estimate the prevalence of susceptibility to smoking. Chi-square analysis was used to test the associations between the categorical independent variables (gender, schooling session, etc) with susceptibility to smoking. Variables with P ≤ .25 were included into the binary multivariable logistic regression to determine the influence of each variable on susceptibility to smoking while simultaneously controlling for potential confounding effects by other variables. Analysis of 2-way interaction revealed no significance for all variables in the final model. All statistical analyses were performed at 95% confidence level.
Results
The majority of the 18 870 nonsmoking respondents consisted of adolescents aged 13 to 15 years (72.8%), females (59.5%), and those who attended morning school sessions (59.1%). Similar to the Malaysian population as a whole, the distribution of nonsmoking school respondents by ethnicity was 58.0% Malay, 23.5% Chinese, 7.2% Indian, and 9.7% Indigenous Sabahan and Sarawakian. Bivariate analysis showed that intra- and interpersonal factors were significantly associated with susceptibility to smoking, The overall prevalence of adolescents susceptible to smoking was 6.0%, with a significantly higher proportion of males compared with females (9.5% vs 3.6%, P < .001). In addition, indigenous Sabahan and Sarawakians were significantly more susceptible to smoking compared with Malay or Chinese (9.1% vs 5.9% and 4.5%, P < .001). Furthermore, Chinese adolescents showed a significantly lower susceptibility to smoking compared with adolescents of other ethnicities (P < .001; Tables 1 and 2). The proportions of respondents whose father/male guardian, mother/female guardian, or both parents/guardians smoked were also significantly higher compared with those whose parents/guardians were non-mokers (6.8%, 14.3%, 12.0%, and 5.1%, respectively, P < .001). Finally, the susceptibility to smoking was higher among respondents who had symptoms of stress (8.6% vs 5.7%, P < .001), anxiety (7.2% vs 5.3%, P < .001), and depression (9.1% vs 5.4%, P < .001) than their counterparts without these symptoms.
Sociodemographic Characteristic of Respondents.

n = sample and N = estimated population.
Malaysia implements a triple-shift school-day system comprising a morning session, an afternoon session, and a morning until afternoon session.
Prevalence of Susceptibility to Smoking Among Secondary School Adolescents in Malaysia.
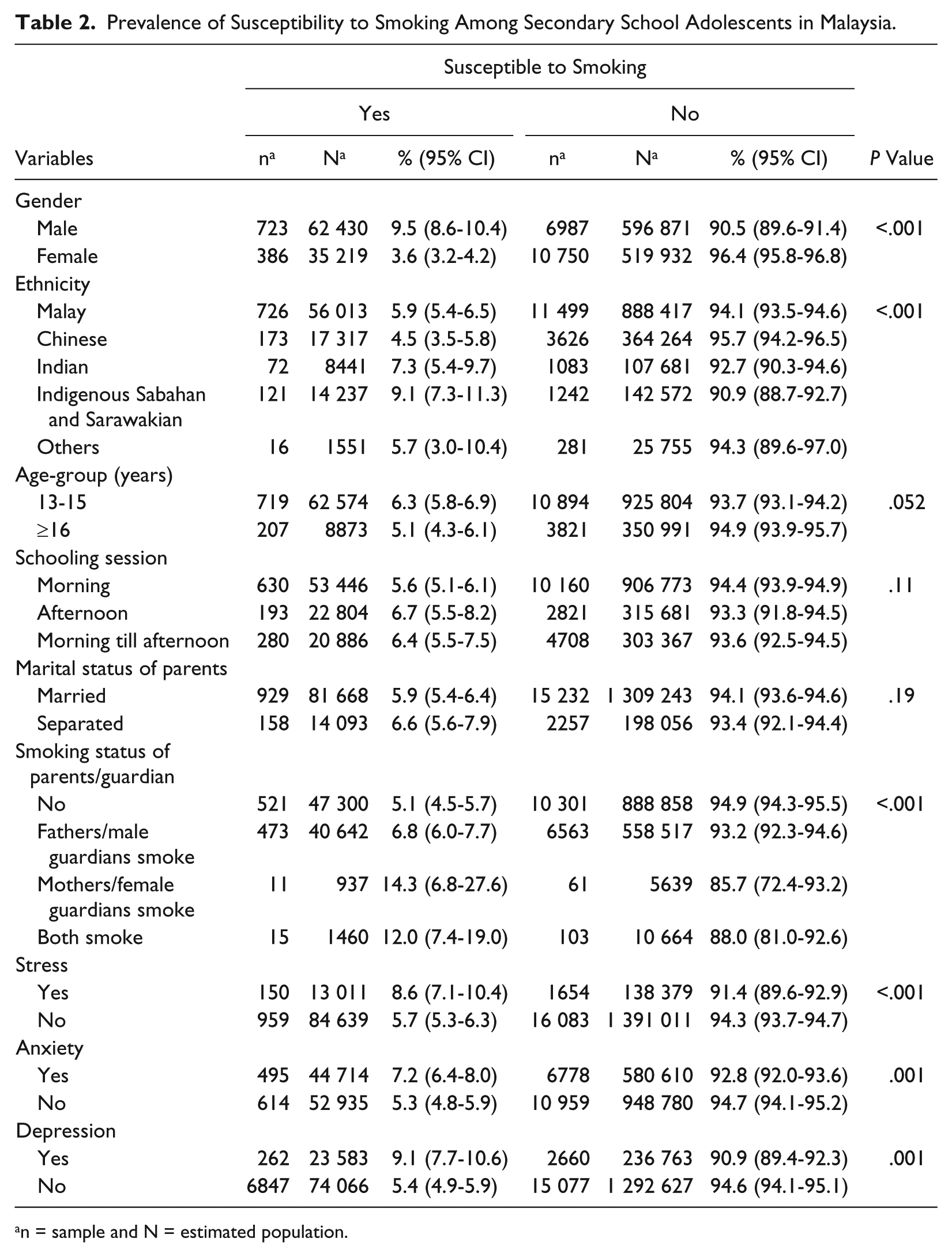
n = sample and N = estimated population.
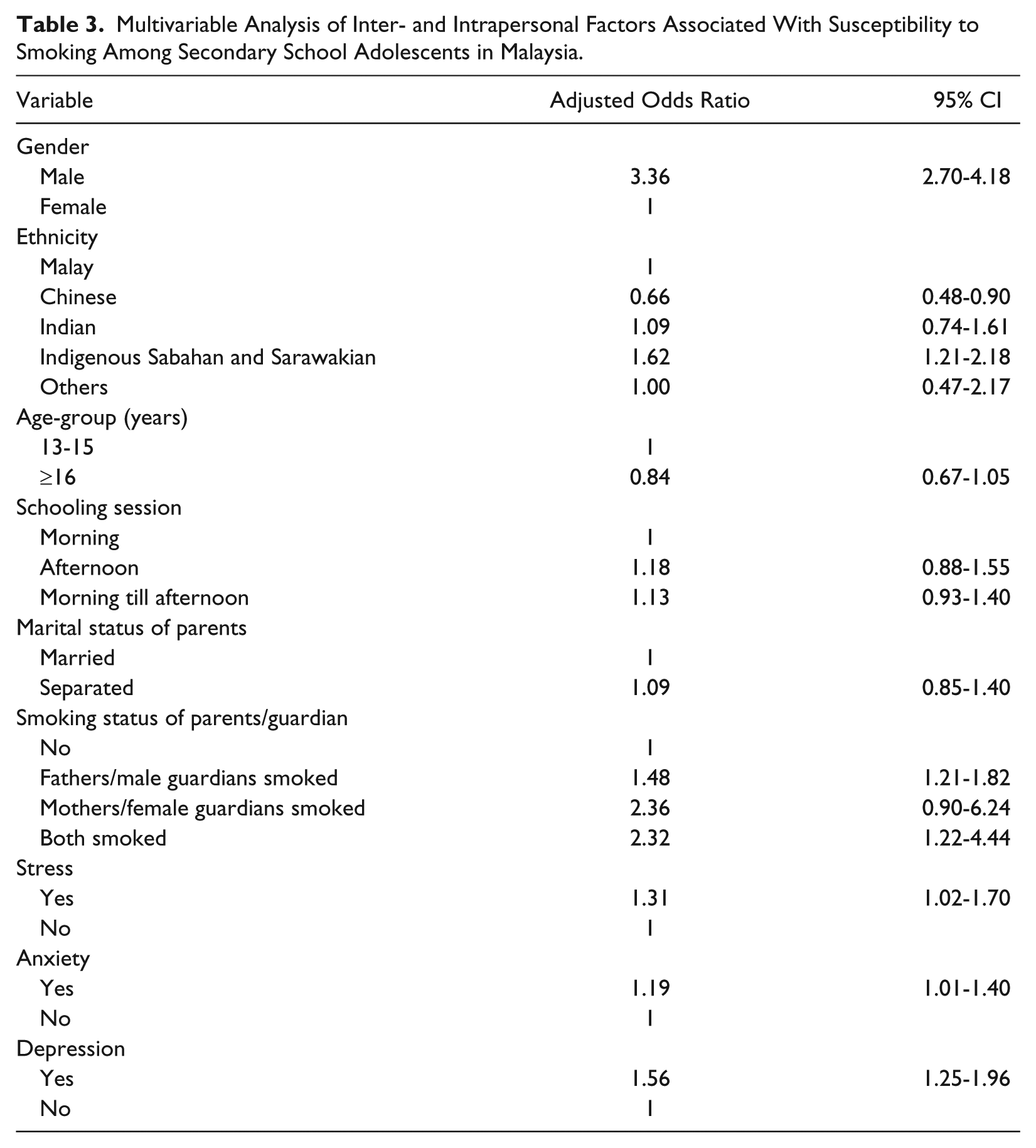
After adjusting for other independent variables, multivariable analysis revealed that respondents susceptible to smoking were more likely to be male (adjusted odds ratio [aOR] 3.36, 95% confidence interval [CI] 2.70-4.18), indigenous Sabahan and Sarawakian (aOR 1.62, 95% CI 1.21-2.18), had father/male guardian or both parents who smoked (aOR 1.48, 95% CI 1.21-1.82; aOR 2.32, 95%CI 1.22-4.44, resoectively); reported stress (aOR 1.31, 95% CI 1.02-1.70), Anxiety (aOR 1.19, 95% CI 1.01-1.40), or depression (aOR 1.56, 95%CI 1.25-1.96; Table 3).
Multivariable Analysis of Inter- and Intrapersonal Factors Associated With Susceptibility to Smoking Among Secondary School Adolescents in Malaysia.
Discussion
This article is the first report on susceptibility to smoking among a representative sample of school-going adolescents in Malaysia. This survey revealed that susceptibility to smoking was 6.0%, which was lower than 15.5% that was reported by Manimaran 16 in 2003 and 16.3% by Lim et al 6 among adolescents in Kota Tinggi district in 2011. It was also twice as low compared with global susceptibility to smoking of 12.5%, and 10.1% among adolescents in Southeast Asia. 8 The decrease in susceptibility to smoking in comparison with 2003 is very encouraging. This could be attributed to the government’s legislative and financial efforts in antitobacco campaigns. Among them, banning smoking in public and work places, requiring pictorial health warnings on all cigarette packs, prohibiting most forms of tobacco advertising and promotion, launching “Tak Nak” or “Say No,” a nationwide antismoking mass and print media campaign, increasing tobacco excise taxes and prices, and cracking down all forms of illicit trade in tobacco products. All these measures may have contributed to the denormalization of smoking behavior among adolescents and they now perceive this habit to be unacceptable in the community. 17 However, further study is recommended to explore the real factors causing the decrease.
Multivariate analysis showed that male adolescents were more susceptible to smoking. This finding was consistent with that of Lim et al 6 among school adolescents in Kota Tinggi district, and Jeganathan et al, 18 which reported aORs of 3.08 (95% CI 2.32-4.09) and 1.93 (95% CI 1.29-2.89), respectively. However, it contradicted the findings by Chen et al 19 based in Canada. This finding could be explained by 3 factors in the Malaysian context. First, smoking is a habit largely among males. Second, smoking among males is accepted as a social norm. Last, parents/guardians give more attention to female adolescents. Existing norms and excessive freedom may cause male adolescents to learn smoking through observing almost half of Malaysian male adults practice this habit, which in turn could be explained by social learning theory, which suggests learning among the same gender is more effective. 20 In view of this, school-based antitobacco programs are recommended to put more emphasis on male adolescents.
This study revealed a new finding that indigenous Sabahan and Sarawakian had higher likelihood of susceptibility to smoking. The reason could be easy accessibility to illicit tobacco products as a result of smuggling from neighboring tobacco-producing countries across the extensive maritime and inland borders of these Borneo states. However, further study is needed to determine the actual causes to effectively curb this problem.
The finding of low susceptibility to smoking among Chinese adolescents compared with other races was in line with the finding of low smoking prevalence among Chinese adults in Malaysia. 21 However, it contradicts the finding among Canadian adolescents of Chinese descent as compared to the Whites/Caucasians where ethnicity did not explain susceptibility to smoking. 19 The disparity confirms the findings by Unger et al 22 that environment influenced the early stages of smoking behavior greater than genetic effects in a study of adolescent twins in Qingdao, China. This is an interesting fact that is worth studying further, to explore genetic and environmental influences on smoking behavior among adolescents of different ethnicities.
Although susceptibility to smoking was lower among respondents aged 16 to 17 years, the difference between this age-group and that of the younger respondents (aged 13-15 years) was not significant. The latter finding contradicted that of Ertas, 23 which reported increasing susceptibility to smoking with increasing age. This finding may be explained on the basis of maturity level, whereby respondents who are older may be able to make more rational decisions than their counterparts aged 13 to 15 years, who were still in the search for self-identification and were easily influenced by the environment. Another reason behind this may be due to the dropout rate in the older age-group after “Penilian Menengah Rendah”; a public national examination taken by all form 3 students (15-year-olds), as older adolescents still in school captured by the survey may be the ones less likely to adopt smoking behaviors.
The fact that adolescents whose parents/guardians both smoked were far more susceptible to smoking than those where only the father/male guardian smokes suggests the existence of a dose–response relationship. This finding concurs with the study by Lim et al 6 in 2011 and Wilkinson et al 7 in 2008, which reported higher likelihood of susceptibility to smoking among adolescents with a smoking parent, OR 1.79 (95% CI 1.09-2.95) and OR 2.65 (95% CI 1.48-4.76), respectively. It also correlates with the finding by Shamsudin and Haris 24 about parental influence on adolescent smoking behavior in Kota Bharu but not with the study by Schultz et al 25 among Canadian adolescents. The disagreement of Asian and Western findings may be a result of social and cultural differences. Asians stress on filial piety, whereby the parents’ behaviors, whether good or bad, would be examples for adolescents to emulate. In this case, parents who smoke might trigger the adolescents to follow them as role models. In addition, parental smoking might contribute to a prosmoking attitude among adolescents, which increases their susceptibility to smoking. However, further detailed studies are needed to determine the pathway of how parental smoking influences adolescent susceptibility to smoking. Nevertheless, family-based antitobacco programs can be designed to help smoking parents quit and create a smoke-free environment at home.
According to this study, adolescents who reported symptoms of stress, anxiety, or depression were found to be more susceptible to smoking than those without, even after statistically adjusting for other independent variables. With regard to studies on susceptibility, Huang et al 9 reported that susceptibility to smoking was significantly associated with positive depression screen among adolescents aged 14 to 17 years in America. Okoli et al 26 also reported that susceptible adolescents were more likely to have “high” depressed mood (OR 1.01, 95% CI 1.01-1.02). In addition, Weiss et al 27 found in their longitudinal study among sixth-graders in California that higher depression score at baseline and increases in depression at 1-year follow-up were risk factors for smoking initiation.
Although not specifically focused on susceptibility to smoking, various studies have demonstrated the significant association between stress, anxiety, or depression with different stages of smoking behaviour.10,11 Among them, a qualitative study by Kwai et al 28 concluded that smoking is one type of mechanism used to deal with the pressures of everyday life, including stress and depression. Simon et al 10 reported that stress was modestly but significantly associated with having tried smoking in both pubertal boys and girls among school adolescents in London. Furthermore, Okeke et al 11 found that there were significantly higher proportions of smokers, whether puffer or experimenter, who had anxiety than those without, among adolescents of Mexican-origin in Houston, Texas. Together with this study, they showed that these psychological conditions might affect adolescents to progress from being susceptible to smoking to addiction.
In contrast, Bush et al 29 reported that susceptible nonsmoking youths aged 11 to 17 years in Washington state, the United States were not significantly associated with anxiety disorders. This discrepancy of results might be because data were collected only among asthmatic adolescents recruited from the registration data of a large nonprofit health maintenance organization in their study, which may not represent the whole adolescent population. Another prospective study by Grenard et al 30 found that stress and depression did not predict past 30-day smoking at 1-year follow-up among adolescents in China. This might indicate that each psychological condition studied affects different stages of smoking development among adolescents at different intensity. Nonetheless, school-based screening programs are recommended to detect stressful, anxious and depressed adolescents and provide them appropriate counseling before they distract themselves with unhealthy habits. This program may be incorporated into the activities of existing counseling club or assigned to the school counselors.
This study has several limitations. First, causal relationships between dependent and independent variables cannot be identified in this study because of its cross-sectional design. Second, susceptibility to smoking was self-reported and may be subjected to respondents’ reluctance to disclose their intention to smoke in the future. Besides, risk factors shown to be associated with susceptibility to smoking such as receptivity to tobacco advertisement (direct or indirect), self-efficacy, social image, socioeconomic status, exposure and access to health information, peer smoking, perceived prevalence of peer smoking, and academic achievements, all were previously shown to be associated with susceptibility to smoking were not not investigated in the current study. In view of this, a future longitudinal study is recommended to explore in further detail various factors and their causality with susceptibility to smoking.
Nevertheless, assurance of confidentiality and absence of school personnel during survey allowed respondents to provide information without fear and stress, increasing their willingness to disclose adequate and true information on factors associated with susceptibility to smoking. The large sample size representative of the Malaysian school population and very high response rate adds to the strength of this study. Thus, the findings from this study may still provide useful cues for the development of effective strategies within future programs designed to stem out the smoking scourge among Malaysian adolescents.
Conclusion
The findings from this study point out the need for proactive measures to reduce the risk factors of smoking initiation among Malaysian adolescents with particular attention toward factors associated with susceptibility to smoking. These were being males, of indigenous Sabahan and Sarawakian descent, having a smoking father/male guardian or parents, and having symptoms of stress, anxiety, and depression. Only with prompt actions can we see a future smoke-free generation of healthy Malaysians.
Footnotes
Acknowledgements
The authors would like to thank the Director General of Health, Malaysia, for his permission to publish this article. We would also like to thank the Ministry of Education, the students who participated and those who were involved in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of the article: Research was funded by the Ministry of Health Malaysia and World Health Organization (WHO), Geneva, Switzerland.