
Abstract
This article provides a cross-sectional weighted measurement of noncommunicable diseases (NCDs) and risk factors prevalence among Brunei adult population using WHO STEPS methodology. A 2-staged randomized sampling was conducted during August 2015 to April 2016. Three-step surveillance included (1) interview using standardized questionnaire, (2) blood pressure and anthropometric measurements, and (3) biochemistry tests. Data weighting was applied. A total of 3808 adults aged 18 to 69 years participated in step 1; 2082 completed steps 2 and 3 measurements. Adult smoking prevalence was 19.9%, obesity 28.2%, hypertension 28.0%, diabetes 9.7%, prediabetes 2.1%, and 51.3% had fasting cholesterol level ≥5 mmol/L. Inadequate consumption of fruits and vegetables prevalence was high at 91.7%. Among those aged 40 to 69 years, 8.9% had a 10-year cardiovascular disease (CVD) risk ≥30%, or with existing CVD. Population strategies and targeted group interventions are required to control the NCD risk factors and morbidities.
Keywords
Introduction
Brunei Darussalam is an oil and gas producing country situated on the northern coast of Borneo Island in Southeast Asia. It has a population of 417 200 and a gross domestic products per capita of USD 30 942. 1 Despite major achievements in controlling the burden of communicable diseases, the country has observed an epidemiologic transition in disease pattern toward noncommunicable diseases (NCDs). 2 Committed to the WHO Global Action Plan for the Prevention and Control of NCDs and the ASEAN Strategic Framework on Health Development, 3 the Brunei Darussalam Multisectoral Action Plan on NCD (BruMap-NCD) 2013-2018 outlines measures for prevention and control of NCDs and risk factors, including a 30% reduction in smoking prevalence and 10% reduction in physical inactivity prevalence by 2018 from 2013 level. 4
Previous studies on selected NCD risk factors have been conducted in Brunei, they are the Integrated Health Survey for Civil Servants 5 and National Health and Nutritional Status Survey (NHANSS). 6 The Integrated Health Survey found 28% of civil servants were obese, 38% had high blood pressure (BP), and 11% had high fasting blood glucose (FBG), while NHANSS reported obesity prevalence of 27%, hypertension prevalence 34%, and diabetes prevalence 12%. However, data analysis from these previous studies were unweighted, assuming equal representation among study participants. Weighted data analysis yields more precise estimates as it incorporates a weight to the pooled observations. 7 This study conducted in 2015-2016 was the first national health survey to adopt WHO STEPwise approach to Surveillance (STEPS) for a population-based health survey. The aim of this study is to provide a cross-sectional weighted measurement of NCDs and risk factors prevalence among Brunei adult population using STEPS for benchmarking and monitoring.
Methods
Participant Recruitment
Participants were randomly selected through 2 stages: (1) households were randomly selected from a list of available households in the district. Brunei has 4 districts; each of the 4 districts was used as the primary sampling unit. (2) One resident within each household (secondary sampling unit) was randomly selected via the Kish method. The selection criteria were Brunei citizens or permanent residents aged 18 to 69 years with regular stay throughout the year, not pregnant or diagnosed with terminal or incapacitating illnesses.
Ethics approval of the study was granted through the Medical and Health Research Ethics Committee, Ministry of Health Brunei Darussalam, prior to data collection (MHREC/MOH/2015/11(9)).
Data Collection
Data collection ran from August 2015 to April 2016. Three steps were taken following WHO STEPS methodology 8 —step 1, questionnaire interview; step 2, anthropometric and BP measurements; and step 3, biochemistry tests.
For step 1, handheld devices loaded with eSTEPS software and WHO STEPS questionnaire were used by trained data collectors at respondents’ residences. Questions include tobacco use, alcohol consumption, dietary habits, the amount of physical activity (PA), history of raised BP, diabetes, raised total cholesterol (TC), cardiovascular diseases, and sociodemographic profiles. Show cards on different types of tobacco products, alcohol, physical activities, and servings of fruits and vegetables were used to facilitate understanding of the questions by the respondents.
Daily fruit and vegetables (FAV) intake were calculated from the number of servings of FAV consumed per day in a typical week. PA level was calculated from the duration of moderate and vigorous physical activities, whether at work, transport and recreation in a typical day and week. Insufficient PA is defined as not fulfilling 150-minute activity of moderate intensity per week or equivalent, as per WHO Global Physical Activity Questionnaire. 8
Steps 2 and 3 were conducted at selected health centres in all the 4 districts. It involved taking anthropometric measurements, fasting blood samples and spot urine specimens by trained nurses and research assistants using WHO STEPS standard methodology.
Step 2 involved taking height, weight, waist circumference, and BP measurements. The OMRON HEM-7322 automatic BP monitor was used to take readings of the participants’ BP. Three BP readings were taken with three minutes interval. Three sizes of cuff were provided to ensure the best possible readings were taken. Participants’ heights and weights were measured with calibrated body mass index (BMI) devices, TANITA WB-3000, ADE M304641-01, and SECA 703, they had a range difference of 0.01 to 0.4 kg between the calibrated weights and displayed values. Overweight is defined as having BMI between 25 and 30 kg/m2 while obesity is having BMI ≥30 kg/m2. Raised BP is defined as systolic BP ≥140 mm Hg and/or diastolic BP ≥90 mm Hg or where the participant is currently on antihypertensive medication.
Step 3 involved taking biochemical measurements; fasting blood glucose (FBG), fasting TC level, and spot urine test using Architect c8000 (ISO 15189). Prediabetes or impaired fasting glycaemia was defined as having FBG ≥6.1mmol/L (110 mg/dL) and <7.0 mmol/L (126 mg/dL). Diabetes was defined as having FBG ≥7.0 mmol/L (126 mg/dL). Hypercholesterolemia is defined as having raised fasting TC ≥5.0 mmol/L or ≥190 mg/dL or currently on medication for raised cholesterol.
Training was conducted for all data collectors to standardize interview techniques, anthropometric and blood pressure measurements. The training sessions were facilitated by WHO technical experts on STEPS methodology.
Data Analysis
Data analyses were conducted using EpiInfo 8 and SPSS 23.0 for Windows. Poststratification weighting accounted for population distribution by districts, gender and age groups from the national population census. 9 The probability of individual weight selection was obtained from the inverse of the probability of household selection in a district (number of household to select/ number of households in list) multiply by the probability of household member selection from Kish data. Overall weight is individual weight multiplied by population distribution which factor in proportion of sample, stratified by age and sex. Weighting was performed for steps 1, 2 and 3 data.

Descriptive statistics on frequency, weighted prevalence and 95% confidence intervals (CI) was performed for sociodemographic and risk factor variables.
Results
Baseline Characteristics
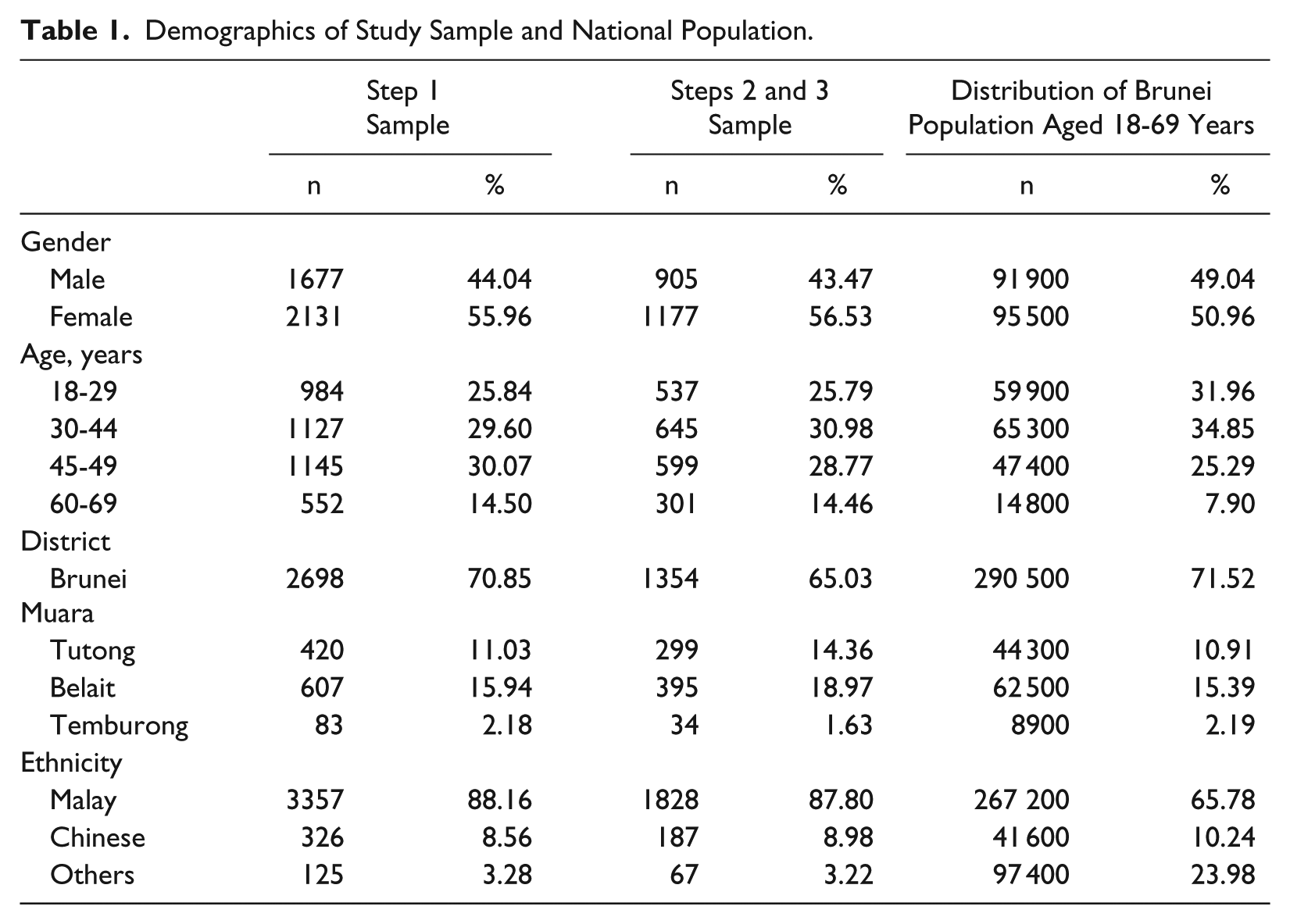
Table 1 shows respondents’ gender, age, district, and ethnic groups. A total of 3808 out of 7229 (52.6%) respondents participated in step 1. Out of 3808 respondents, 2082 participated in steps 2 and 3.
Demographics of Study Sample and National Population.
NCD and Risk Factors Prevalence Among Brunei Adult Population
Table 2 shows the weighted prevalence of NCDs modifiable risk factors, physical measurements and biochemistry blood tests. Further breakdown by age groups and genders are shown in Table 3.
Frequencies (n) and Weighted Prevalence (%) of Behavioral Risk Factors and Anthropometric and Biochemical Measurements by Gender.
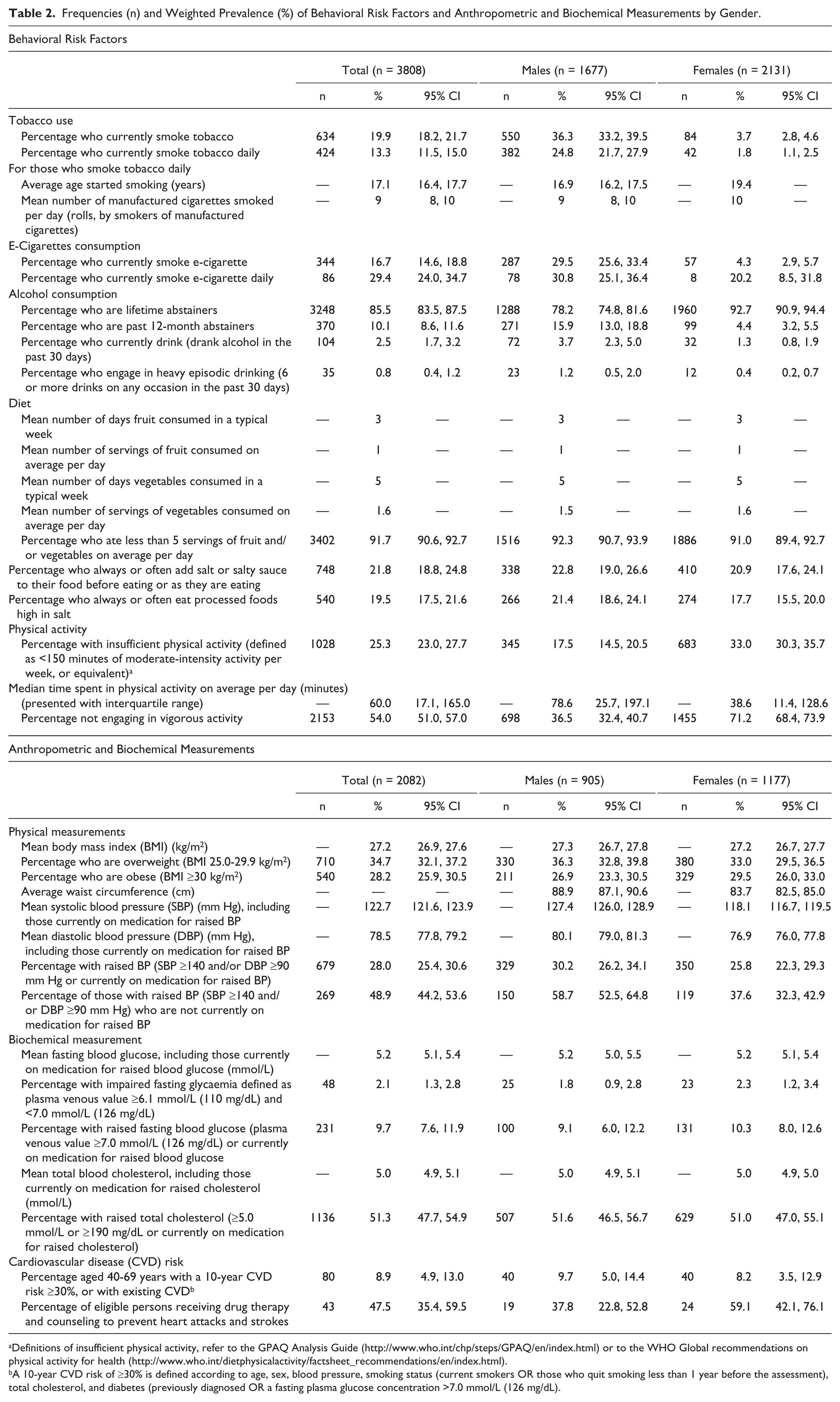
Definitions of insufficient physical activity, refer to the GPAQ Analysis Guide (http://www.who.int/chp/steps/GPAQ/en/index.html) or to the WHO Global recommendations on physical activity for health (http://www.who.int/dietphysicalactivity/factsheet_recommendations/en/index.html).
A 10-year CVD risk of ≥30% is defined according to age, sex, blood pressure, smoking status (current smokers OR those who quit smoking less than 1 year before the assessment), total cholesterol, and diabetes (previously diagnosed OR a fasting plasma glucose concentration >7.0 mmol/L (126 mg/dL).
Frequencies (n) and Weighted Prevalence (%) of Noncommunicable Disease Risk Factors and Morbidities by Age Group.
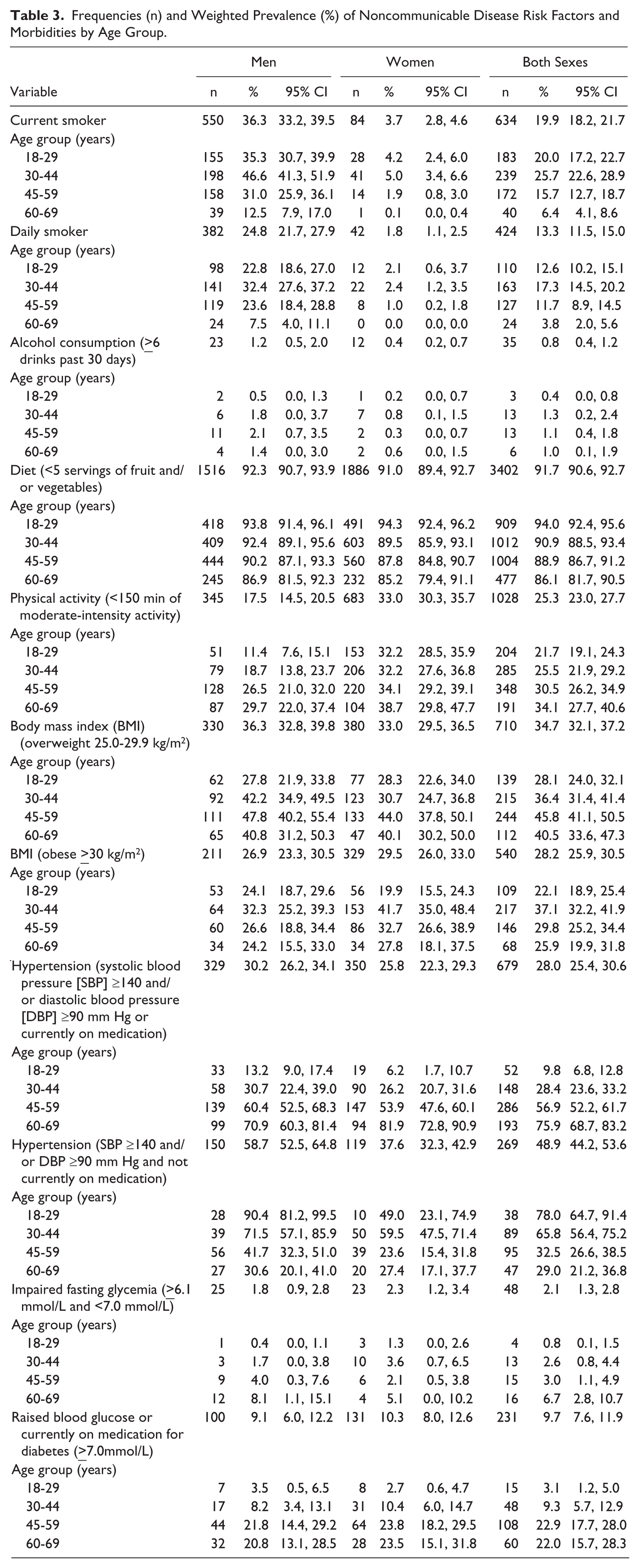
A total of 36.3% (95% CI = 33.2-39.5) males and 3.7% (95% CI = 2.8-4.6) females currently smoke, with overall prevalence 19.9% (95% CI = 18.2-21.7). 13.3% (95% CI = 11.5-15.0) reported smoking daily with 9 cigarette rolls per day on average. The prevalence is higher in younger groups, 20.0% (95% CI = 17.2-22.7) aged 18 to 29 years and 25.7% (95% CI = 22.6-28.9) aged 30 to 44 years were smokers as compared with 15.7% (95% CI = 12.7-18.7) aged 45 to 59 years and 6.4% (95% CI = 4.1-8.6) aged 60 to 69 years.
In all, 2.5% (95% CI = 1.7, 3.2) reported drinking alcohol in the past 30 days, and about one-third of them reported heavy episodic drinking.
Overall, 91.7% (95% CI = 90.6-92.7) consumed less than 5 servings of FAV daily. The prevalence is higher among the younger group, 94.0% (95% CI = 92.4-95.6) aged 18 to 29 years did not meet the recommended intake as compared with 86.1% (95% CI = 81.7-90.5) aged 60 to 69 years. One in 5 (21.8%) added salt when eating.
A total of 25.3% (95% CI = 23.0-27.7) reported insufficient activity, with nearly twice the number of females (33%) compared with males (17.5%). The prevalence is higher among the older groups, 34.1% (95% CI = 27.7-40.6) aged 60 to 69 years did not meet the recommended PA as compared with 21.7% (95% CI = 19.1-24.3) aged 18 to 29 years.
In all, 34.7% (95% CI = 32.1-37.2) were overweight (BMI 25.0-29.9 kg/m2) and 28.2% (95% CI = 25.9-30.5) was found obese with BMI ≥30 kg/m2. Men were found to have wider mean waist circumference (88.9 cm) than women (83.7 cm).
A total of 28.0% (95% CI = 25.4-30.5) have raised BP or were on antihypertensive medications; 30.2% (95% CI = 26.2-34.1) males and 25.8% (95% CI = 22.3-29.3) females. Out of those with raised BP, 48.9% (95% CI = 44.2-53.6) were not previously diagnosed and not treated with medications. The diabetes prevalence was 9.7% (95% CI = 7.6-11.9), 9.1% (95% CI = 6.0-12.2) males, and 10.3% (95% CI = 8.0-12.6) females. Overall, 51.3% (95% CI = 47.7-54.9) have a fasting TC of ≥5.0 mmol/L with no difference between sexes. The prevalence of a 10-year cardiovascular disease (CVD) risk greater than 30% or with existing CVD among those aged 40 to 69 years was 8.9% (95% CI = 4.9-13.0). Less than half (47.5%) of those with existing CVD were receiving drug therapy and lifestyle counseling to prevent heart attacks and strokes.
Discussion
Key findings from the national survey on the weighted prevalence of behavioral risk factors and morbidities associated with NCDs in Brunei adult population are reported.
Smoking
One in 5 adults currently smokes, while e-cigarette consumption was prevalent in 17% of adult population. The prevalence of smoking is higher than in Singapore (15%) 10 but lower than Malaysia (23%), 11 Thailand (24%), 12 and Indonesia (35%). 13 The age of smoking initiation was 17.1 years (95% CI = 16.4-17.7), which is lower than the legal age of smoking in Brunei. 14 Brunei has increased tobacco import duties and taxes significantly from BND 0.25/USD 0.18 per cigarette stick in 2010 to BND 0.50/USD 0.36 in 2017. 15 (http://www.tradingacrossborders.gov.bn/Downloadable/Siaran Akhbar Perubahan Kadar-Kadar Cukai (BM).pdf). Since 2014, there has been no licensed cigarette seller in Brunei due to high cost of import tax and license fee. 16 However, significant quantities have been brought in illegally. 17
Harmful use Of Alcohol
Brunei has prohibited alcohol sale since 1984. 18 A non-Muslim person older than 17 years is allowed to bring 2 bottles of liquor and twelve 330 mL cans of beer for personal consumption per entry into Brunei. This policy has markedly contributed to low prevalence (less than 1%) of harmful use of alcohol or episodic heavy drinking reported in the study population. However, the alcohol consumption prevalence found may be underreported due to the prohibition on alcohol in the country.
Physical Activity and Diet
Three in 4 adults met the recommended PA level. The physical inactivity prevalence increased with age for both genders (Table 3), suggesting for more efforts in community initiatives for active ageing. The implementation of the Health Promotion Blueprint 2011-2015 has driven several key government initiatives in the community and private sectors to promote PA. A milestone PA promoting initiative was introduced in September 2016 by zoning of urban areas for car-free Sundays.
Improving FAV intake is key to achieving better nutritional health. A daily diet that includes FAV reduces the risk of coronary heart disease, stroke, and certain types of cancer. 19 Our study revealed a high prevalence of adults (92%) with inadequate intake, which is worse in younger groups, for both sexes. In addition, about one-fifth Bruneians regularly consumes processed food and has the habit of adding salt and sauces to food.
There is wide availability of processed food in Brunei. 20 Recently, several multisectoral initiatives have been undertaken, including healthy school canteen and healthy workplace initiatives, healthier choice initiative, and community-based weight management programs. A fiscal policy, effective on April 1, 2017, was implemented to reduce consumption of unhealthy food, specifically introducing a tax on sugar-sweetened beverages. 15 Further actions should include lowering the cost of FAV; promotion and support of community gardening; increase access to fresh FAV in food venues. Food industry interventions should include regulation of unhealthy food marketing; product reformulation to reduce sugar, fat and salt content; business licensing policies to increase the retail and distribution of healthier options.
Obesity, Hypertension, Diabetes, Hypercholesterolemia, and CVD Risks
Adult obesity rates reported in other Southeast Asian countries were 18% in Malaysia, 11 11% in Singapore, 10 4.8% in Thailand, 21 4.8% in Indonesia, 13 4.0% in Myanmar, 22 2.6% in Laos, 23 2.1% in Cambodia, 24 and 1.7% in Vietnam. 25 Our finding of 28% obesity prevalence in Brunei highlights the urgency of tackling obesity due to its links to increased risks of type 2 diabetes, cardiovascular diseases, and other metabolic and inflammatory disorders. 26 A strong food-centric culture, 27 processed food availability, 20 and automobile dependence 28 in Brunei have contributed to an obesogenic environment.
Our study found a high prevalence (28%) of hypertension, this is comparable to the prevalence in Malaysia (30%) 11 and Singapore (24%). 10 In Brunei, nearly half (48.9%) of those with hypertension were undiagnosed. This is of concern as hypertension increases the risk of developing cardiovascular and cerebrovascular diseases, which are the leading causes of deaths in Brunei.
The diabetes prevalence of 10% is lower than Singapore (11%) 10 and Malaysia (18%). 11 Our study found that 2.1% have prediabetes or have the risk of developing diabetes with FBG between 6.1 and 7.0 mmol/L. Prediabetes is associated with impaired microvascular function and thus may contribute to diabetes-associated cardiovascular disease and other complications such as impaired cognition and heart failure. 29 Hypercholesterolemia prevalence is high with over half of the adult population having fasting TC of ≥5.0 mmol/L, higher than Singapore (17%) 10 and Malaysia (48%). 11 The study found that nearly one-tenth of adults are at high risk of developing CVD in the next 10 years. Immediate pharmacological management and lifestyle intervention are necessary for such individuals as ischemic heart diseases is one of the three leading causes of mortality in Brunei. 2 Studies of health seeking or screening behaviors among those with increased NCD risk, and if there is any association of the risk factors and morbidities would be useful future work.
Strength of This Study
This is the largest national health survey conducted in Brunei’s adult population that uses WHO STEPS methodology. The use of standardized methodology and objective physical and biochemical measurements increased the validity of survey findings. Furthermore, data collection done through handheld devices (IPAQs) reduced errors and time to data acquisition.
We are aware that NHANSS was previously conducted to assess NCD and risk factors prevalence among the Brunei adult population. 6 NHANSS was a cross-sectional study with a smaller sample size (n = 2184 for step 1 and n = 1488 for steps 2 and 3), there was no weighting was performed for the data analysis in NHANSS, thus prevalence rates comparison between studies must be made with caution.
Our findings provided a weighted measurement and confirmed the presence of significant prevalence of key NCD risk factors and morbidities (smoking, inadequate FAV consumption, obesity, hypertension, and hypercholesterolemia) in the population.
Limitations of This Study
The response rate for step 1 was 53% (3808 out of 7229 participants). There was also drop in participation in steps 2 and 3, due to respondents’ lack of transportation to health centers or refusal to participate in blood tests. Future national health surveys should address these factors when designing the survey logistics. During the health survey, contributing factors of low responses were identified and mitigated with the survey extending for 3 months, additional recruitment and training of data collectors were undertaken. Weighting was performed to adjust for disproportionate representation of the adult population due to nonresponse and dropouts.
Conclusion
A significant proportion of Brunei adults were found to have NCD risk factors (smoking, low FAV consumption, and low physical inactivity) and NCD morbidities (obesity, diabetes, hypertension, and hypercholesterolemia). Many individuals were not previously diagnosed. Both population strategies and targeted group interventions are required to effectively control NCDs and risk factors. Using standardized methodology is essential for monitoring of public health interventions. It allows policy makers to better assess the health needs of the population, identify priority settings, and set appropriate targets. Further studies are needed to evaluate the recent national health policies implemented in the prevention and control of noncommunicable diseases.
Footnotes
Acknowledgements
The authors would like to express sincere appreciation to the technical assistance and support from the World Health Organization, Department of Economic Planning and Development Brunei Darussalam, Centre for Strategic and Policy Studies Brunei Darussalam, Discovery Year students, data collectors from the Universiti Brunei Darussalam, research assistant and managers from the Ministry of Health Brunei Darussalam, and participation from the survey respondents.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The national health survey was conducted with support from the Ministry of Health Brunei Darussalam and Brunei Research Council, Department of Economic Planning and Development, Brunei Darussalam (Grant No. SM01A/600108/B00606).