
Abstract
The association between smoking cessation period and metabolic syndrome (MS) is currently unknown. We studied 6032 men aged >19 years who participated in the Korean National Health and Nutrition Examination Surveys between 2010 and 2012. The risk of MS according to the amount of smoking and duration of smoking cessation was examined, and adjusted for age, amount of alcohol consumed, physical activity, body mass index, income, and education levels. Compared with never-smokers, there was a significant increase in the risk of MS among current smokers >10 pack-years and former smokers with a history of pack-years >30. The odds ratio for MS increased with smoking amount in both current and former smokers. But the risk of MS in former smokers was no longer significant after 20 years of smoking cessation adjusted for past smoking amount. Thus, to prevent MS, current smokers should quit smoking early and former smokers should continue quitting.
Introduction
According to the World Health Organization, in 2017, the average overall smoking rate for men was 35% and for women 5%. Additionally, approximately 7 million people died from diseases associated with smoking each year. 1 Average smoking rate for males in Asian countries was high at 34.3% in 2016 as per reports from the OECD (Organisation for Economic Co-operation and Developments), and smoking is a major public health issue in the Asia-Pacific region. 2 Smoking increases the risk of cardiovascular disease, a major cause of death among adults, and insulin resistance.3,4 Metabolic syndrome (MS) is characterized by the simultaneous occurrence of high blood pressure (BP), abdominal obesity, dyslipidemia, and impaired fasting glucose. MS increases the risk for type 2 diabetes and cardiovascular diseases by increasing insulin resistance.5,6 Numerous studies have reported that smoking is associated with MS.7,8 Moreover, smoking decreases high-density lipoprotein cholesterol (HDL-C) levels, a major factor of MS, while increasing triglyceride (TG) levels. 9 Smoking is also associated with high rates of abdominal obesity, hypertension, and impaired fasting glucose. 7
The risk for MS was found to be higher among former and current smokers than among nonsmokers. 10 A study involving Korean individuals suggested that smoking was associated with MS.7,9 Furthermore, the risk for MS has a dose-response association with the level of cigarette consumption.10,11 Previous studies have investigated the risk for MS among current and former smokers and the association between the risk and level of cigarette consumption. There is limited evidence on the association between cumulative cigarette consumption and smoking cessation period, and the findings have been inconsistent.11-13 Therefore, it is difficult to draw any clear conclusions on the association between smoking cessation and MS.
This study assessed the risk of MS according to cumulative cigarette consumption by former and current smokers using data from the Korea National Health and Nutrition Examination Survey (KNHANES) and examined the association between MS and duration of smoking cessation among former smokers.
Methods
Participants and Study Period
This cross-sectional study evaluated the association between the risk of MS, duration of smoking cessation, and amount of smoking using data derived from the fifth KNHANES conducted between 2010 and 2012. 14 The KNHANES is a nationwide survey providing statistics on health status, health-related awareness and behavior, level of food consumption, and nutritional status among Koreans. The participant group included 8280 men aged >19 years who responded to the survey. The following exclusion criteria were adopted: failure to respond to questions related to smoking (714 individuals); lack of data regarding waist circumference, BP, physical activity, body mass index (BMI), blood glucose level after 8 hours of fasting, HDL-C, and TG levels (533 individuals); and a diagnosis of cancer (244 individuals), cirrhosis (34 individuals), history of myocardial infarction or angina (421 individuals), thyroid diseases (87 individuals), and renal failure (28 individuals). Finally, 6032 men were included in this study, which was approved by the institutional review board of the Soonchunhyang University Hospital, Cheonan, Korea (SCHCA 2016-11-010). The KNHANES data are openly published, and informed consent from participants was not required since data were fully anonymized prior to analysis.
Body Measurements and Blood Tests
A trained examiner measured the height and body mass of each participant dressed in light clothes. BMI was calculated by dividing the body weight by the square of the height. Waist circumference was measured using a tape measure at the midpoint between the level of the lowest rib and the upper margin of the iliac crest, after the participant exhaled, without pressing hard on the 2 measurement points. BP was measured following a 15-minute rest, every 5 minutes, on 3 occasions. The second and third BP measurements were used to calculate the mean BP. Serum blood glucose, HDL-C, and TG levels were measured after 8 hours of fasting.
Smoking, Drinking Habits, Physical Activity Questionnaire, Education, and Income Levels
Sex, age, and health behavior parameters, including smoking status, drinking habits, and the level of physical activity were investigated via self-reported questionnaires. Each medical history was elicited through patient interviews. The participants were classified as nonsmokers, former smokers, and current smokers. Former and current smokers were divided according to the number of pack-years (PY; 20 cigarettes in a pack): PY ≤ 10, 10 < PY ≤ 20, 20 < PY ≤ 30, and PY > 30. Former smokers were also stratified according to the duration of smoking cessation (CY): CY ≤ 10, 10 < CY ≤ 20, 20 < CY ≤ 30, and CY > 30. Excessive alcohol consumption was defined as the ingestion of ≥5 glasses (8 g of alcohol as one glass) of alcohol on a single drinking occasion. Physical activity levels were classified according to the amounts of exercise per week, measured as metabolic equivalents (METs): 600 ≤ METs < 3000 for medium-intensity exercise, and METs ≥3000 for high-intensity exercise. Education levels were classified according to the duration of education: ≤6years, 7 to 9 years, 10 to 12 years, and ≥13 years. Average monthly household incomes were divided into 4 quartiles (US$ ≤ 1500, 1500 < US$ ≤ 2700, 2700 < US$ ≤ 4400, and US$ > 4400) to calculate income level.
Diagnostic Criteria for MS
A diagnosis of MS was made if 3 of the following 5 conditions set by the National Cholesterol Education Program/Adult Treatment Panel III were satisfied. 15 Abdominal obesity was defined according to waist circumference, following the criteria set by the Korean Society for the Study of Obesity 16 :
Waist circumference ≥90 cm
TGs ≥ 150 mg/dL
HDL-C < 40 mg/dL
Systolic pressure ≥130 mm Hg, or diastolic pressure ≥85 mm Hg, or use of antihypertensive drugs
Fasting blood glucose level ≥100 mg/dL, or use of oral antidiabetic drugs or insulin
Statistical Analysis
Clinical and metabolic characteristics, including patient characteristics, age, BMI, waist circumference, BP, fasting blood glucose levels, TG, and HDL-C levels, were measured as continuous variables and one-way analysis of variance was performed. Categorical variables, which included the amount of alcohol consumed, the level of physical activity, education, and income levels, were compared among nonsmokers, former smokers, and current smokers using the χ2 test. Differences in risks of MS and other metabolic abnormalities according to smoking status were also compared using the χ2 test.
To investigate the association between cumulative cigarette consumption of current smokers and the risk for MS or constituents of MS, and between cumulative cigarette consumption of former smokers and the risk for MS, cigarette consumption was measured in PY (PY ≤ 10, 10 < PY ≤ 20, 20 < PY ≤ 30, and PY > 30). Multivariate logistic regression analysis adjusted for age, amount of alcohol consumed, physical activity, income, and education levels was also performed.
Three analysis models were used to assess the association between the duration of smoking cessation of former smokers and MS. The duration of smoking cessation was divided into CY ≤ 10, 10 < CY ≤ 20, 20 < CY ≤ 30, and CY > 30. Model 1 was adjusted for age, drinking amount, physical activity, BMI, income, and education levels. Model 2 was based on Model 1, with additional adjustment for tobacco consumption. Model 3 was based on Model 2, with additional adjustment for abdominal obesity. All statistical analyses were performed using SPSS version 14.0 (IBM Corp, Armonk, NY). The level of statistical significance was set at P < .05 at a 95% confidence interval.
Results
General Characteristics of the Participants According to Their Smoking Status, Prevalence Rates of MS, and Metabolic Abnormalities (Table 1)
A total of 6032 participants with a mean age of 49.3 ± 15.9 years were included. The rate of current smoking was 45.3%, and the prevalence rate of MS was 29.6%. There were 1221 (20.2%) nonsmokers and 2079 (34.5%) former smokers.
Participant Characteristics Based on Smoking Status*.
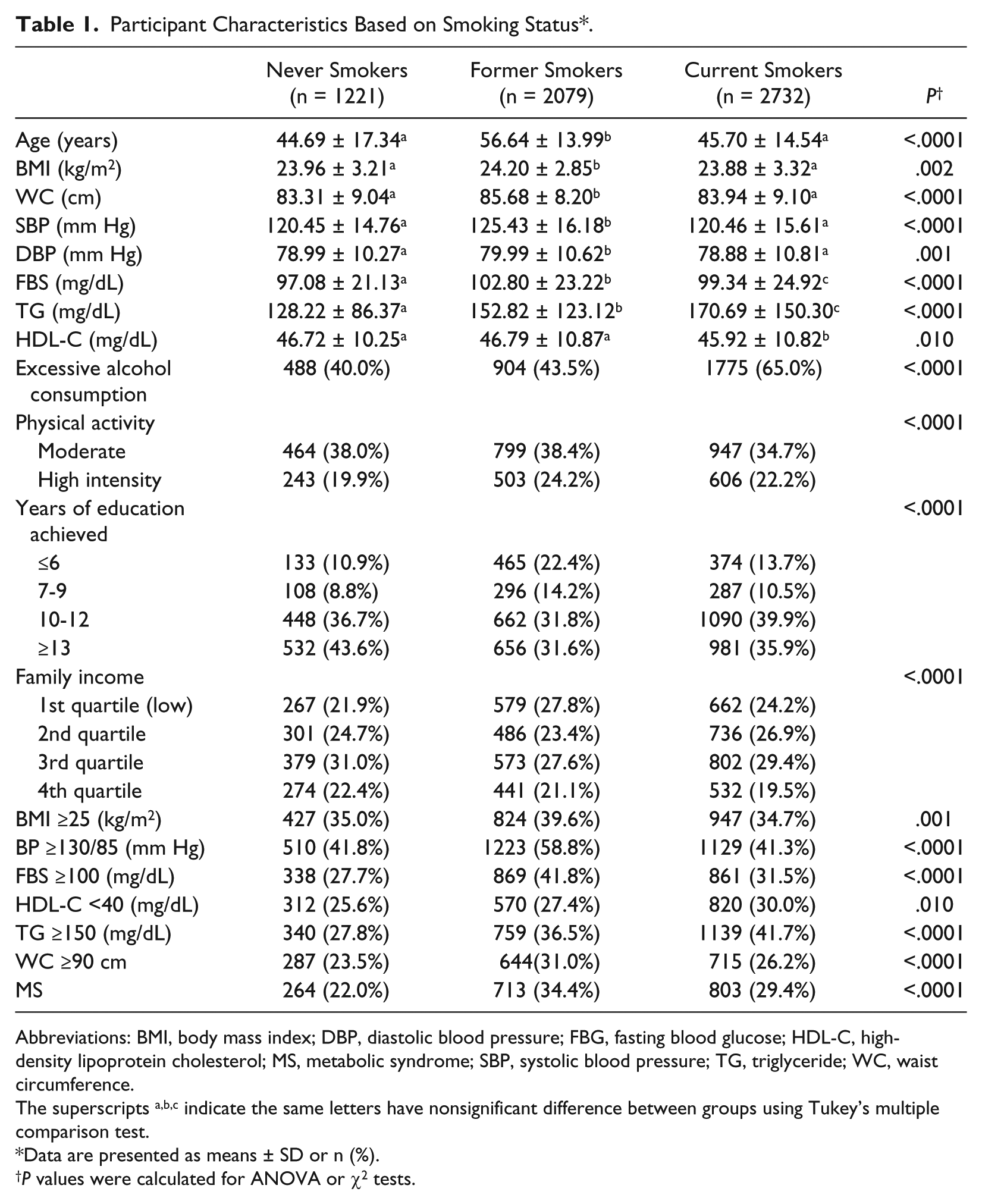
Abbreviations: BMI, body mass index; DBP, diastolic blood pressure; FBG, fasting blood glucose; HDL-C, high-density lipoprotein cholesterol; MS, metabolic syndrome; SBP, systolic blood pressure; TG, triglyceride; WC, waist circumference.
The superscripts a,b,c indicate the same letters have nonsignificant difference between groups using Tukey’s multiple comparison test.
Data are presented as means ± SD or n (%).
P values were calculated for ANOVA or χ2 tests.
Among former smokers, rates of obesity, abnormal BP, impaired fasting glucose, and abdominal obesity were significantly higher than nonsmokers and current smokers. Abnormal levels of HDL-C and TG were higher among former and current smokers than among nonsmokers.
There were also significant differences in the prevalence rate of MS according to smoking status: 22.0% among nonsmokers, 34.4% among former smokers, and 29.4% among current smokers.
The Risks for MS and Other Metabolic Abnormalities According to the Level of Cigarette Consumption Among Current Smokers and Former Smokers (Table 2)
Significant differences in the risks of MS and other metabolic abnormalities, adjusted for age, amount of alcohol consumed, exercise, education, income levels, and BMI were found among current smokers, according to the level of cigarette consumption.
Odds Ratios (Adjusted) for Metabolic Parameters Among Current Smokers and Former Smokers Based on the Level of Smoking Among Current Smokers and Former Smokers a .
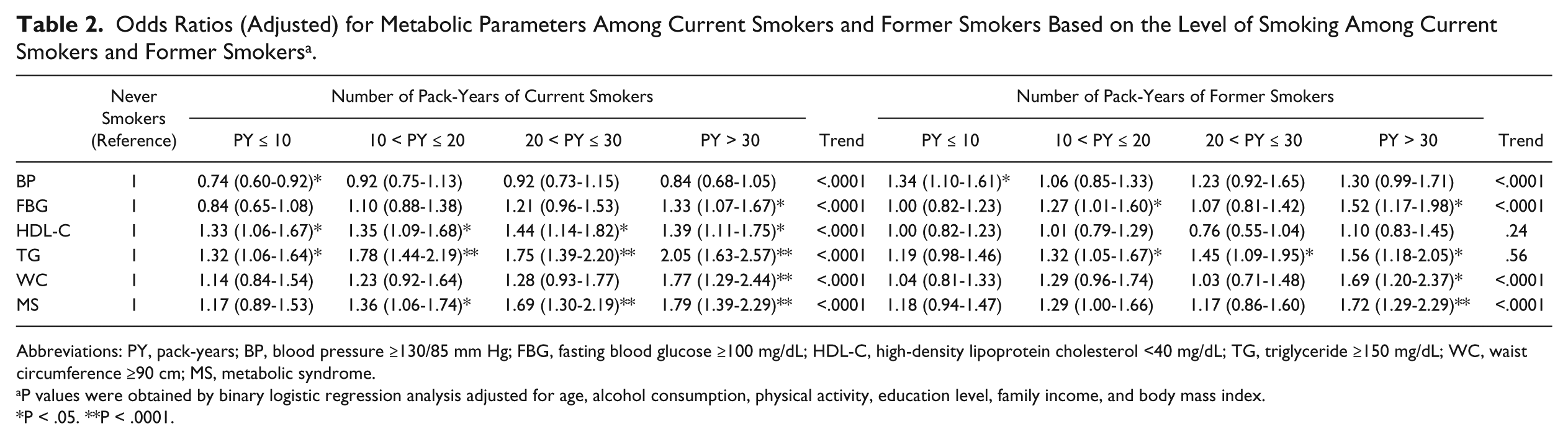
Abbreviations: PY, pack-years; BP, blood pressure ≥130/85 mm Hg; FBG, fasting blood glucose ≥100 mg/dL; HDL-C, high-density lipoprotein cholesterol <40 mg/dL; TG, triglyceride ≥150 mg/dL; WC, waist circumference ≥90 cm; MS, metabolic syndrome.
P values were obtained by binary logistic regression analysis adjusted for age, alcohol consumption, physical activity, education level, family income, and body mass index.
P < .05. **P < .0001.
The risk of MS was 1.36 (95% confidence interval [CI] = 1.06-1.74), 1.69 (95% CI = 1.30-2.19), and 1.79 (95% CI = 1.39-2.29) for current smokers with 10 < PY ≤ 20, 20 < PY ≤ 30, and PY > 30, respectively, relative to nonsmokers. The risk for MS was 1.72 (95% CI = 1.29-2.29) for the former smokers with PY > 30.
In the current smokers, the risk of abnormal levels of HDL-C and TGs were higher than nonsmokers in all PY groups. Smokers with PY > 30 cigarette consumption had a higher risk of abdominal obesity and impaired fasting glucose, and those with PY ≤ 10 had a lower risk of abnormal BP.
Among former smokers with PY > 30, the risk of impaired fasting glucose, abdominal obesity, and abnormal levels of TGs were higher than nonsmokers. The risk for abnormal BP was higher among former smokers with PY ≤ 10.
Odds Ratios for MS According to the Duration of Smoking Cessation (Table 3)
Odds Ratios (Adjusted) for MS Among Former Smokers Based on the Duration of Smoking Cessation a .
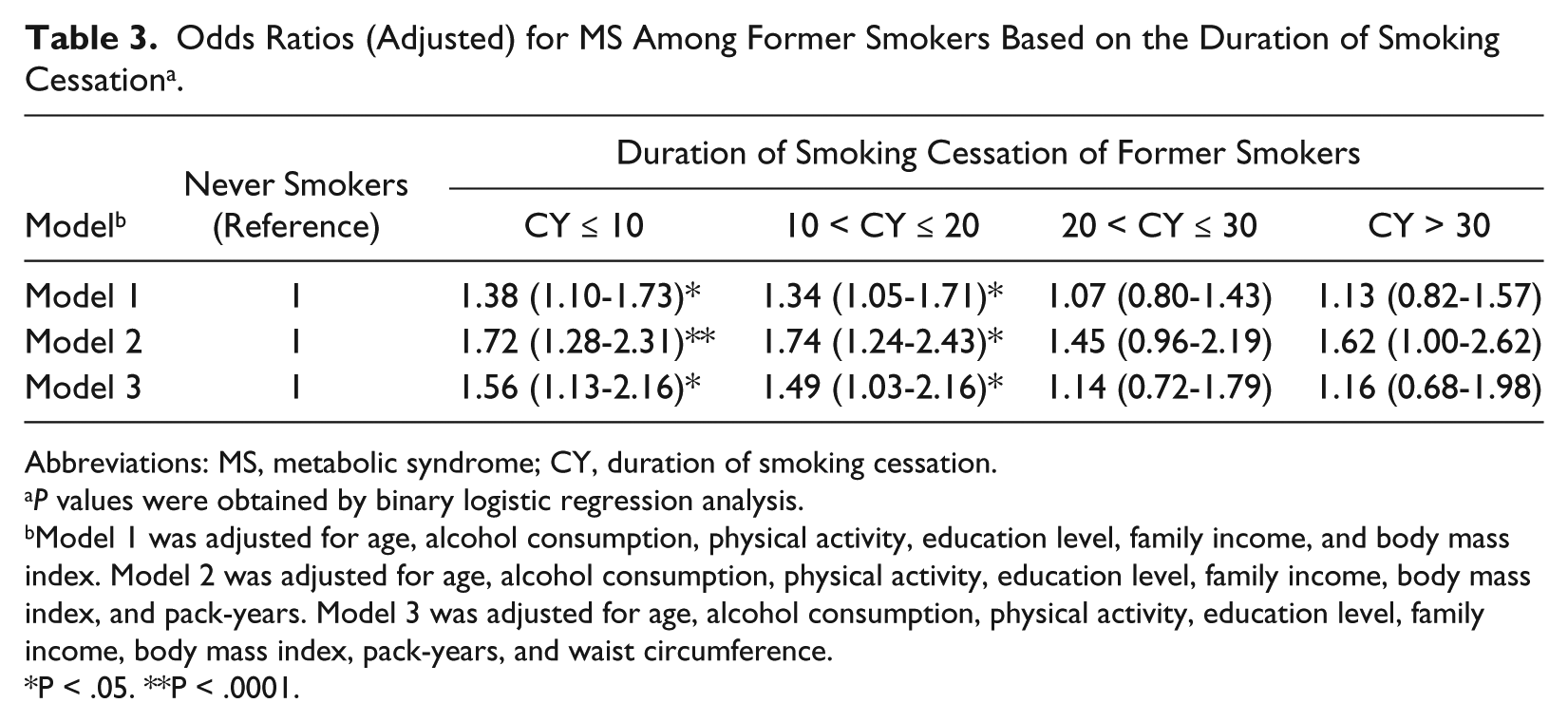
Abbreviations: MS, metabolic syndrome; CY, duration of smoking cessation.
P values were obtained by binary logistic regression analysis.
Model 1 was adjusted for age, alcohol consumption, physical activity, education level, family income, and body mass index. Model 2 was adjusted for age, alcohol consumption, physical activity, education level, family income, body mass index, and pack-years. Model 3 was adjusted for age, alcohol consumption, physical activity, education level, family income, body mass index, pack-years, and waist circumference.
P < .05. **P < .0001.
The odds ratio for MS in Model 1 adjusted for age, amount of alcohol consumed, exercise, income, education levels, and BMI was significantly higher in the groups with a smoking cessation period CY ≤ 10 and 10 < CY ≤ 20 compared with nonsmokers (1.38 [95% CI = 1.10-1.73] and 1.34 [95% CI = 1.05-1.71], respectively). However, no significant increase in the odds ratio for MS was found in the group with a smoking cessation period CY > 20.
Also in Model 2 (additionally adjusted for PY) and Model 3 (additionally adjusted for abdominal obesity), the odds ratio for MS was significantly higher in the groups with a smoking cessation period CY ≤ 10 and 10 < CY ≤ 20 than among nonsmokers. No significant increase in the odds ratio for MS was observed in the group with a smoking cessation period CY > 20.
Discussion
In this study on 6032 male adults included from the KNHANES in 2010 and 2012, the risk for MS was found to increase as the level of tobacco consumption increased in both current and former smokers. Furthermore, while the risk for MS increased among former smokers who quit smoking for 20 years or less, increased risk for MS was no longer present for smokers who quit smoking for >20 years.
Previous studies have reported that insulin resistance developing in the early period of smoking cessation decreases as smoking cessation continues, and that the risks for MS and diabetes decreased among former smokers who had quit smoking for a long term.11,12,17 In this study, the increased risk for MS was not seen after 20 years of smoking cessation. While the risk for MS adjusted for past smoking consumption increased for smokers with under 20 years of smoking cessation, it did not increase significantly for those who quit for over 20 years. Wada et al 11 reported that the risk of MS is eliminated after >20 years of smoking cessation. Previous studies calculated the amount of smoking among former smokers using daily consumption of tobacco,11,12 while this study used not only daily consumption of tobacco but also total smoking period; therefore, direct comparisons are difficult. These findings suggest that eliminating the risk of MS requires a long period of smoking cessation, not a short time.
In this study, the risk of MS was 1.36 (95% CI = 1.06-1.74), 1.69 (95% CI = 1.30-2.19), and 1.79 (95% CI = 1.39-3.29) for current smokers with 10 < PY ≤ 20, 20 < PY ≤ 30, and PY > 30, respectively. Therefore, the risk increased as the level of tobacco consumption increased. A previous study involving current smokers reported a positive correlation between the level of tobacco consumption and the risk of MS. 7
Ishizaka et al 10 and Chen et al 18 reported that the risk of MS in former smokers increased with increased cumulative cigarette consumption. In the present study, among former smokers with cumulative cigarette consumption of over 30 PY, the risk for MS, 1.72 (95% CI = 1.29-2.29), increased even after smoking cessation. Visceral fat accumulation is a major cause of abdominal obesity in smokers and increases with cigarette consumption. 19 Canoy et al 20 investigating waist-to-hip ratios according to the level of cigarette consumption, the rate of abdominal obesity was found to increase with increased cigarette consumption among both current and former smokers. These findings suggest that the risk of abdominal obesity increases among former heavy smokers even after smoking cessation and that insulin resistance is likely to continue and induce MS.
In this study, levels of HDL-C decreased among current smokers, and TG levels increased among current and former smokers. Smoking induces insulin resistance and affects lipid metabolism, reducing levels of HDL-C and increasing TG levels, and that insulin resistance is continuing after smoking cessation.10,13,21 Findings regarding the effect of smoking on fasting blood glucose levels are contradictory. A previous study did not find a significant association between fasting blood glucose levels and tobacco consumption, 18 while another reported that the incidence of type 2 diabetes increases with increased tobacco consumption. 17 In the present study, the risk of impaired fasting glucose significantly increased among current smokers with PY > 30. While nicotine is known to increase BP by inducing catecholamine and aldosterone release,22,23 the risk for hypertension was significantly low for smokers with PY < 10. Several studies have not found any significant differences in BP according to smoking status,12,24 while others have reported significantly lower BP among smokers.25,26 It is difficult to conclude that cumulative cigarette consumption among participants with <10 PY is associated with decreased BP, and further research is required.
While nicotine reduces blood leptin levels through the effects of catecholamine, leptin levels increase after smoking cessation, resulting in increased appetite and weight gain.27,28 In this study, mean BMI and waist circumference of former smokers were higher than of non-smokers and current smokers. Weight gain and abdominal obesity occur in the early period after smoking cessation, and an earlier study has reported an increased incidence of MS due to weight gain and abdominal obesity among former smokers who quit smoking for a short term. 29 Therefore, to prevent and manage MS, it is necessary for antiobesity education to take place with smoking cessation education. And further research is needed to consider weight changes according to the duration of smoking cessation.
This study has several limitations. First, due to the cross-sectional design, the sequential relationship between smoking status and MS could not be determined. Second, participant smoking status was based on self-reports and may not be accurate. Third, only men were included in this study because the proportion of female smokers was too low (former female smokers 3.9% [n = 316], current female smokers 5.8% [n = 473]) for a detailed analysis. Fourth, we did not apply weights, strata, and clusters in analyzing the data, and the study was conducted only among Koreans. Therefore, the sample was not representative of the adult population in Korea and the Asia-Pacific region. This study was based on the 2010 to 2012 KNHANES, so ongoing research using recent data is needed.
In conclusion, the risk of MS significantly increased with increased cigarette consumption in both current and former smokers. But the risk of MS in former smokers was no longer significant after 20 years of smoking cessation. Thus, to prevent MS, current smokers should quit smoking early and former smokers should continue quitting. Simultaneously, efforts to prevent their weight gain is needed. Further prospective research is also required to establish the causal relationship between the smoking status and MS considering the smoking cessation period.
Footnotes
Acknowledgements
We thank the Korea Institute for Health and Social Affairs (KIHASA) for providing the 2010 to 2012 Korea National Health and Nutrition Examination Survey data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the institutional review board of the Soonchunhyang University Hospital, Cheonan, Korea (SCHCA 2016-11-010).