
Abstract
Smoking cessation significantly reduces risk of smoking-related diseases and mortality. This study aims to determine the prevalence and factors associated with attempts to quit and smoking cessation among adult current smokers in Malaysia. Data from the National E-Cigarette Survey 2016 were analyzed. Forty nine percent of current smokers had attempted to quit at least once in the past 12 months and 31.4% of the respondents were former smokers. Multivariable analysis revealed that current smokers with low nicotine addiction and aged below 45 years were more likely to attempt to quit smoking. Being married, older age group, and having tertiary education were significantly associated with smoking cessation. Only half of the current smokers ever attempted to quit smoking and only a third of smokers quit. Stronger tobacco control policies are needed in Malaysia to encourage more smokers to quit smoking. Improved access to cessation support for underprivileged smokers is also needed.
Keywords
Smoking prevalence is significantly higher among male adults in Malaysia compared to female adults
Prevalence of smoking among Malaysian adults plateau since the last two decades.
The smoking cessation rate among Malaysian adult
The attempts to quit smoking among current smoker in Malaysia
Introduction
Tobacco-induced diseases are the major causes of premature mortality in Malaysia over the past 3 decades, of which 20 000 deaths are reported annually. 1 A total of 10.7% of the disability-adjusted life years among males are attributable to smoking. 2 Smokers would enjoy a better quality of life after smoking cessation. 3 Their circulatory function would improve immediately, lungs begin to heal within 1 year, and risk of developing heart diseases and stroke would reduce by 50%. 4 In addition, the mortality risk for those who have stopped smoking at and under the age of 35 years is comparable to nonsmokers. 5
The prevalence of smoking among the adult population in Malaysia has plateaued in the past 3 decades. The percentage of the Malaysian population who smoke was 24.8% in 1996, 21.5% in 2006, and 22.8% in 2015. 6 To address this, the Malaysian government through the Ministry of Health has initiated various health promotion programs, such as the incorporation of anti-smoking elements in the community-based intervention program “Komuniti Sihat, Pembina Negara” (KOSPEN; loosely translated to “Healthy Community Builds the Nation”). The Ministry has also provided stop smoking services in public clinics and collaborated with various agencies. The measures taken are in line with the provision of Article 15 of the Framework Convention on Tobacco Control, which urges member countries to assist smoking cessation by providing adequate facilities. 7
Apart from counseling and pharmacological approaches, identifying factors associated with smoking cessation attempts and characteristics of smokers who had successfully quit smoking might enhance the smoking cessation rate. Ample studies have reported that smokers who are female, young, have lower addiction to nicotine, 8 perceive smoking negatively, have more knowledge of tobacco-related harm, 9 and those with medical conditions are more likely to make attempts to quit smoking. On the other hand, smokers who are in the elderly age group, received junior or high school education, married, smoke fewer than 20 cigarettes per day, started smoking late, smoke for shorter duration, perceive good or excellent self-rated health, with higher level of self-efficacy, 10 higher income, and lower level of stress, were more likely to cease smoking. 11 This information remains scarce among Malaysian adult smokers. Determining and distinguishing characteristics of smokers who attempt to quit or have succeeded in quitting smoking may assist in the formulation of anti-smoking policies. Hence, this article aims to describe the prevalence and factors associated with quit attempts and smoking cessation among Malaysian adult smokers using the latest data obtained from a representative sample of Malaysians aged 18 years and older.
Methods
Data were derived from the National Electronic Cigarette Survey (NECS) 2016, which used a cross-sectional study utilizing 2-stage proportionate-to-size sampling method to select a representative sample of Malaysian population aged 18 years and older. The first strata consisted of 15 states in Malaysia followed by stratification by urban and rural area for each state. Enumeration blocks, which are artificial geographical areas created by the Department of Statistics Malaysia, were the primary sampling units, whereas living quarters (LQs) were the secondary sampling units. Twelve LQs were selected from each selected enumeration block. All eligible household members aged 18 years and above from the selected LQs were invited to participate in this study. A total of 3494 LQs were selected (2028 from urban and 1466 from rural areas). A total sample size of 5722 was determined based on a previous finding and expert opinion prevalence rate of 5%, 12 precision rate of 1.5%, design effect of 2, 2-stage stratification, and nonresponse rate of 20%.
Data from selected respondents were obtained from face-to-face interviews by a trained research assistant. Prior to each interview, respondents were given an explanation of the purpose of the study, voluntary participation, and on their rights to refuse to answer any questions and to withdraw at any juncture of the study. In addition, the respondents were assured on protection of their confidentiality and that all the information gathered would be utilized for research purposes only. Each interview session commenced after written consent were given by the respondents. The ethical approval for this study was granted by the Medical Research and Ethics Committee of the Ministry of Health of Malaysia (NMRR 16-171-28819 [IIR]). The details of the study have been described by Ab Rahman et al. 12
Measures
A prevalidated questionnaire was used to collect data on sociodemographic background, awareness and usage of “e-cigarettes,” cigarette smoking status, exposure to “e-cigarette” smoke/vapor, exposure to e-cigarettes promotion and anti-smoking campaign, and perception of “e-cigarettes.”
The dependent variables were smoking cessation and attempt to quit smoking. Smoking cessation was assessed among ever smokers and defined as smoked more than 100 sticks in their lifetime but did not smoke in the past 30 days. Those who have ceased smoking are hereafter referred to as former smokers. Attempt to quit was assessed among current smokers and defined as smoked more than 100 sticks of cigarettes in their lifetime, at least once during the past 30 days, and have attempted to quit at least once during the past 12 months.
Independent variables were social demographic variables and nicotine addiction. The social demographic variables were gender, ethnicity (Malay, Chinese, Indian, and others), education attainment (no formal education, completed primary education, completed secondary school, and completed university/college), age group (15-24 years old, 25-44 years old, 45-64 years old, and 65+ years old), locality (urban, rural), marital status (single, widow/widower, separated, and married), and occupation (government servant, private sector employee, self-employed, and others). Nicotine addiction was measured using the Fagerstrom Test for Nicotine Dependence, which consisted of 6 items, whose total score ranged from 0 to 10. Nicotine addiction was further categorized into “no to low addiction” (scores from 0-4) or “moderate to high addiction” (scores from 5-10).
Statistical Analysis
Data were cleaned prior to analysis. Descriptive statistic was used to describe the social demographic distribution of the respondents. Pearson’s χ2 analysis was used to test associations between attempt to quit smoking among current smokers and smoking cessation and the independent variables. Univariate associations with P value ≤.25 were included in multivariable analysis. Two separate multivariable logistic regression analyses were carried out to determine independent variables associated with attempt to quit smoking among current smokers and smoking cessation (current/former). The final models were assessed by the Hosmer-Lemeshow goodness-of-fit test, which showed P values of .167 (former smokers) and .321 (attempt to quit), indicating that both models were fit. All statistical analyses were performed at significance level (α) of .05 using SPSS statistics software version 22.
Results
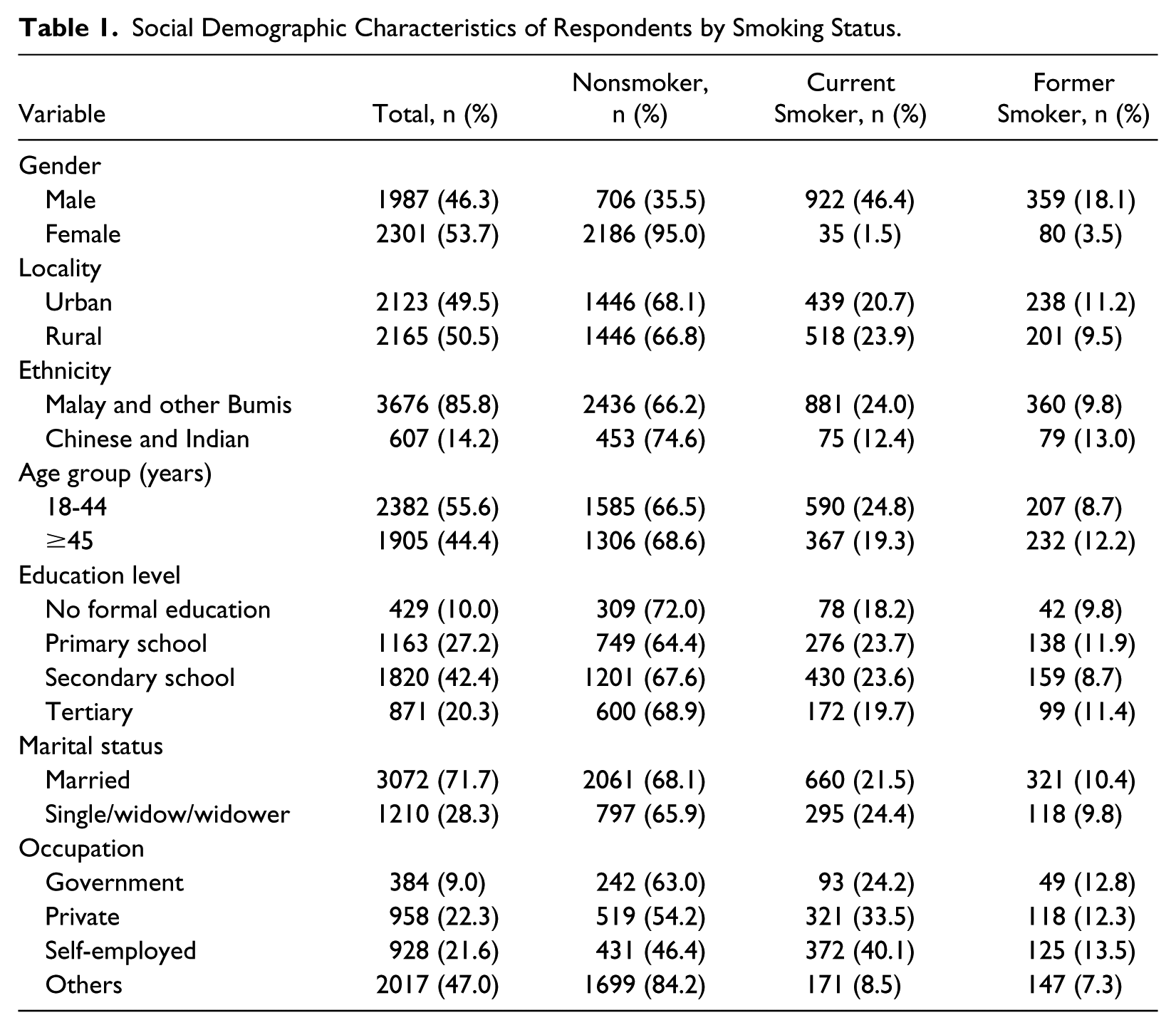
The response rate of the study was 62.1% (n = 4288/6906: 59% and 65% of response rate from the urban and rural areas, respectively). Of the 4288 respondents, more than half of the respondents (53.7%) were female, and most of the respondents are of Malay and Bumiputra descent (85.8%) and married (71.7%). Almost half of them were urban dwellers. Approximately one-fifth of the respondents attained tertiary education. The proportion of smoking was significantly higher among males and in those working in the private sector and self-employed. The prevalence of smoking among Malay and others Bumiputras was almost 2 times as high as among those of Chinese and Indian descent (Table 1). Table 2 shows that among ever smokers, the prevalence of former smoking was significantly higher among females, urban dwellers, people of Chinese or Indian descent, aged 45 years and older, and those working in the government. No significant association was observed between marital status and being a former smoker rather than a current smoker. Bivariate analysis showed that a higher proportion of smokers from the younger age group (18-44 years) and those with lower nicotine addiction attempted to quit smoking in the past 12 months.
Social Demographic Characteristics of Respondents by Smoking Status.
Smoking Cessation Among Ever Smokers and Attempt to Quit Among Current Smokers.

Abbreviation: NA, not available.
Multivariable logistic regression revealed that respondents aged 45 years and older (adjusted odds ratio = 2.39, 95% confidence interval = 1.58-3.61) and those who were married (adjusted odds ratio = 1.62, 95% confidence interval = 1.03-2.53) were more likely to be former smokers, whereas respondents with lower educational attainment were more likely to be current smokers. Smokers with higher levels of addiction to nicotine and those working in the private sector and the self-employed were less likely to make an attempt to quit smoking in the past year (Table 3).
Multivariable Logistic Regression to Determine Smoking Cessation and Attempt to Quit Among Malaysian Aged 18 Years and Above a .
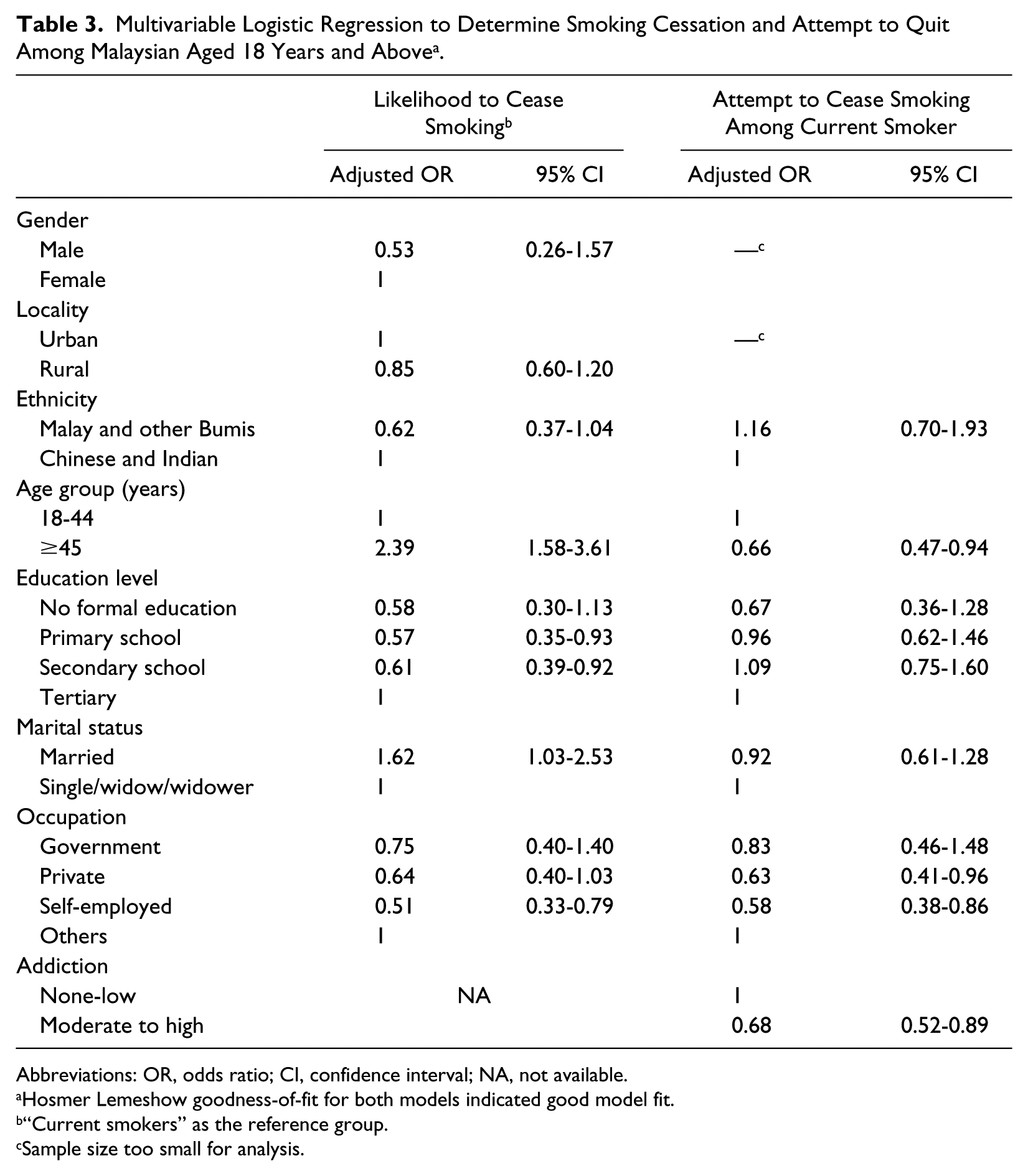
Abbreviations: OR, odds ratio; CI, confidence interval; NA, not available.
Hosmer Lemeshow goodness-of-fit for both models indicated good model fit.
“Current smokers” as the reference group.
Sample size too small for analysis.
Discussion
This is the first nationally representative survey to study the prevalence and factors associated with former and current smoking status and attempts to quit smoking among Malaysian adult smokers. Our findings revealed that the proportion of ever smokers in Malaysia who have ceased smoking (31.4%) was almost identical to the natural quit rate among adults in America. 13 Although this rate is encouraging, more efforts are needed to increase the cessation rate among Malaysian adult smokers. The proportion of respondents who attempted to quit at least once in the past year (49.1%) was similar to the 48.6% reported by the Global Adult Tobacco survey study in 2011. 14 This finding indicates that no significant progress has been made in the rate of those attempting to quit smoking among Malaysian adult smokers over the past 5 years. Hence, more aggressive measures should be implemented to encourage more quit-smoking attempts in order to increase smoking cessation rate. In comparison to other countries, the proportion of smokers who attempted to quit was significantly higher than the 40% reported among current smokers in the United States. 13 This might be due to a lower proportion of hard-core smokers in Malaysia compared with the United States.
Factors Associated With Attempt to Quit Smoking Among Current Smokers
In line with previous studies,9,15 our study also found that smokers with lower nicotine addiction are more likely to make an attempt to quit smoking. Respondents with moderate to high dependency might encounter more severe withdrawal symptoms including irritability, frustration, anger, anxiety, increased appetite, and difficulty concentrating, since their last quit attempt, therefore making quitting difficult. 16
Consistent with previous studies among current smokers in Thailand, 17 Bangladesh, 10 and the United States, 13 our study revealed that younger aged respondents were more likely to make an attempt to quit smoking. Shorter duration of smoking and lower addiction to nicotine might be the plausible reasons why younger smokers are more likely to attempt quitting compared with older smokers.
Although there were significant associations between both marital status and education level with quitting attempt in univariate analysis, the associations diminished after adjustment for other variables. Contrary to general belief that higher educated smokers are more likely to attempt and to quit smoking due to higher awareness of smoking hazards. As for marital status, married smokers are expected to be more motivated to quit smoking because they have better social support and prioritize family expenses and therefore have less disposable income to support a smoking habit. More in-depth qualitative future studies are necessary to elucidate the effect of education and marital status on attempt to quit.
Factors Associated With Smoking Cessation
Former smokers were more likely to be of older age; this is in agreement with findings by Goren et al 13 (among US adults), Li et al 18 (among adult smokers in Malaysia and Thailand) in the International Tobacco Control study, among adults smokers in Romania 19 as well as Jampaklay and colleagues 17 in their longitudinal study on smoking cessation among adult Thai smokers. There are several possible reasons for this. First, older smokers are more likely to have made more quit attempts than younger smokers simply because they have lived longer and hence they have had more chances to become smoke-free. Second, this could also be due to different mortality rates between smokers and former smokers (continuing smokers are more likely to die at a younger age and therefore those who quit outlive them into older age). Third, older smokers are more likely to have smoking-related health conditions; therefore, they tend to make more visits to health care facilities due to this, and thus are more likely to have received advice to cease smoking by health care personnel. However, we did not investigate the age at which respondents quit smoking. Future studies are strongly suggested to include age at smoking cessation to confirm this.
Similar to findings from a systematic review by Vangeli et al, 20 our study revealed no significant association between gender and smoking cessation after adjusting for confounders. However, this was contradictory to a study in Korea, which reported female smokers were more likely to successfully quit smoking due to pregnancy and childcare responsibilities. 11 A possible explanation for the lack of association is the relatively low number of female smokers in this study. Therefore, we suggest a longitudinal study focused on smoking women of childbearing age during pregnancy and after delivery to examine the effect of pregnancy and delivery on smoking cessation.
In line with a previous study in Korea, 11 we found that respondents with tertiary education were more likely to cease smoking. However, a study by Jampaklay et al 17 reported no significant association between education attainment and smoking cessation. Our findings suggested that respondents with high education level have greater knowledge of the dangers of smoking. 21 These perceptions are the main driving force of smoking cessation, as posited by the health belief model. 22 The likelihood of smoking cessation among smokers with higher education is high as they are more likely to work and stay in smoke-less environments surrounded by family members, peers, or colleagues who are nonsmokers and do not view smoking as a norm. 23 This increases the success rate of quit attempts among this group due to reduced exposure to smoking cues. Besides, smokers with higher educational attainment tend to have greater economic resource and psychological support in their endeavors to quit smoking compared with those with lower education. Furthermore, smokers with higher education and less financial constraints can afford to purchase additional effective cessation aids. Having more psychological resources, this group of smokers is also more resilient to psychological stresses as shown in previous studies17,24; and therefore, they have better capability to cope with withdrawal syndromes to further encourage their quit attempts.
Our finding that married respondents were more likely to cease smoking is consistent with studies from developed and developing countries, which documented that the cessation rate is most likely reflecting the social influence within marriage. 25 Wives in Western countries have a powerful influence on their husbands’ behaviors (eg, in encouraging smoking cessation). 25 This is best explained by the “marriage protection” and “marriage selection” theories. 26 According to the marriage protection theory, marriage has a positive association with beneficial health effects. From the Asian cultural perspective, the family is an important institution. 27 Married respondents are believed to have better economic and social support from their spouses. This consequently enhances their motivation to quit smoking. The marriage selection theory hypothesizes that healthier individuals are likely to marry and to stay married. Those who are married are more intent on living a healthy lifestyle and are willing to take initiatives to quit negative habits.
Limitations
There are some notable limitations in our study. First, several variables explored in previous studies that were associated with attempt to quit and smoking cessation were not investigated in this current study, these include: knowledge of health hazard of smoking, attitude toward health smoking, stress level, self-efficacy, motivational to quit smoking, free smoking policies at home, 28 working areas, 29 and medical condition of respondents and their family. Second, quit attempt was measured verbally and is thus subject to recall bias, particularly if the quit attempt only lasted a short duration or occurred a long time ago. Third, smoking status, smoking cessation, and attempt to quit were self-reported; therefore, there might be response bias. Research has shown that people tend to overreport socially desirable behaviors, and inversely, underreport socially undesirable behaviors. 30 Fourth, the duration of smoking cessation was not investigated in detail; therefore, this might affect the analysis of the association between age group and smoking cessation. However, the representativeness of the study sample enables inference of these findings to the general Malaysian population. Also, the response rate was high, and use of the face-to-face interview method assured the completeness and quality of responses.
Conclusion
In summary, low nicotine addiction and aged below 45 years were more likely to attempt to quit smoking, and being married, older age group, and having tertiary education were significantly associated with smoking cessation among Malaysian adults. The findings from this study may inform the design of interventions to enhance the smoking cessation and attempts to quit smoking among Malaysian smokers to protect the health of the Malaysian population.
Footnotes
Acknowledgements
We would like to thank the Director-General of Health Malaysia for his permission to publish this article. We would also like to thank those who were involved in the study and assisted in data collection and management for their support and cooperation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was funded by the National Institute of Health, Ministry of Health, Malaysia.