
Abstract
Health risk behaviors and mental health problems are associated with morbidity and premature mortality among adolescents. Understanding the magnitude of the problem may improve adolescent health status. The Adolescent Health Survey was conducted to collect data on health risk behaviors among Malaysian school-going adolescents using self-administered questionnaires. A 2-stage stratified cluster sampling design was used and samplings weights were calculated to ensure representativeness to the general population. A total of 27 497 out of 30 823 school-going adolescents completed the questionnaires, yielded an 89.2% overall response rate. The methodology was robust to ensure valid estimation on the prevalence of health problems among Malaysian school-going adolescents.
What We Already Know
Conducting adolescent health survey using self-administered questionnaire is to monitor the health status of Adolescents.
What This Article Adds
This article explained on the representativeness of the selected sample with consideration of complex sampling design to achieve the best estimation for each prevalence of health risk behaviours among Malaysian Adolescents.
Introduction
Adolescence is the period of maturation from childhood to adulthood in terms of biological and physical appearance, emotional well-being, and psychosocial relationships. 1 Adolescents face many challenges during this period such as academic performance and expectation, besides social relationships with family members, teacher, and peers. During this period, they also start to make their own decisions in life. Generally, adolescents are perceived as the healthiest group in the population, therefore they suffer from lack of attention until problems materialize in adulthood as the result of engaging with health risk behaviors during adolescence.2,3 Biological changes of puberty and cognitive development act as internal influencers to shape their behavior. However, their engagement with health risk behaviors is influenced by many social determinants such as peer pressure, poverty, inadequate education, early marriage, familial problems, and culture of the society that they live in. 4 Health risk behaviors increase the risk for morbidity and premature mortality among adolescents, of which some of the causes are preventable. The World Health Organization (WHO) estimates that the leading causes of death among adolescents globally are road-traffic injury, followed by human immunodeficiency virus (HIV) infection, suicide, lower respiratory infections, and interpersonal violence. 5 A recent local study observed that the major cause of mortality among male adolescents aged 10 to 24 years in Malaysia was mainly contributed by road-traffic injuries, which is a preventable cause. 6
Health risk behaviors among adolescents is monitored worldwide. The renowned collaborative study involving many participating countries to monitor adolescent health in Europe and North America is the “Health Behavior in School-aged Children” (HBSC), while the “Global School-based Student Health Survey” (GSHS) is conducted among low- and middle-income countries.7,8 Both surveys select samples from different age groups. The HBSC conducts survey among 11-, 13-, and 15-year-old adolescents while the GSHS is conducted among 13- to 17-years-old adolescents. The age definition for adolescent, youth, or young people varies according to literature. 9 The WHO has traditionally defined adolescence to be the age between 10 and 19 years, youth between 15 and 24 years, and young people between 10 and 24 years. 10 Adolescence can be further divided into early (10-13 years), middle (14-16 years), and late adolescence (17-19 years) according to Sawyer et al. 4 The GSHS compares the prevalence of health risk behaviors between the younger group of adolescents aged 13 and 15 years with the older group of 16 and 17 years. 7 In Malaysia, the first group is also referred to the lower secondary and the latter as upper secondary according to local school categorization. In this survey, the majority of questionnaires assessing the health risk behaviors among adolescents covered the important scopes typically studied in adolescents such as substance use, violence and unintentional injury, sexuality, mental health conditions, parental relationship, hygiene practice, dietary behavior, and physical activity. 11
The Ministry of Health Malaysia started their own Adolescent Health Unit to focus on adolescent health in 1995. 12 The nationwide survey on adolescent health risk behavior was carried out in 1996 under The Seventh Malaysia Plan. The study covered the main health risk behaviors, which were smoking, drinking alcohol, drug usage, and sexual experience using the PRIDE Drug Usage Prevalence Questionnaire. The reported prevalence was 16.9 %, 9.0%, 2.2%, and 1.8 % for smoking, drinking alcohol, using drugs, and involvement in sexual activity, respectively. 13 After a long gap, the Youth Behaviour Risk Factor Surveillance (YBRFSS) was conducted in 2010 among school-going adolescents aged 13, 14, and 16 years throughout Malaysia. 14 Finally, Malaysia conducted the GSHS in 2012 covering students aged 13 to 17 years (Form 1 to Form 5). The Malaysian GSHS in 2012 observed that 11.5% of the students were current smokers, 1.5 % were current drugs users, and 8.9 % were current drinkers. A total of 8.3% engaged in premarital sexual activity, 17.9% had ever been bullied, and 6.8% reported suicidal attempts in the past 12 months. 15
Regular monitoring of adolescents’ health risk behaviors is undeniably important, not only to observe trends but also to evaluate the existing or previously conducted adolescent health programs and policies. The use of standard methodology is important for ensuring the national representativeness of the selected sample to ensure internationally comparable findings. While the overarching objective of this study was to estimate the prevalence of health risk behaviors and mental health problems among adolescents, the aim of the current article is to elaborate on the methodology of the AHS and its representativeness toward all Malaysian adolescents.
Materials and Methodology
Scope and Tools
The AHS focused on health risk behaviors and protective factors among adolescents. The main tool was based on the Malaysian GSHS 2012 questionnaires. 16 The original questionnaire was developed by the WHO and Centers for Disease Control and Prevention (CDC) of the United States in collaboration with the United Nations Children’s Fund (UNICEF), the United Nations Educational, Scientific, and Cultural Organization (UNESCO), and the Joint United Nations Programme on HIV and AIDS (UNAIDS) in 2001. It has been widely used by more than 100 countries, which enables international comparisons of findings. The GSHS questionnaire consisted of 10 core components, which were alcohol, tobacco and drug use, dietary behaviors, hygiene, mental health, physical activity, protective factors, sexual behaviors, violence, and unintentional injury. The answers ranged from a dichotomous “yes” or “no” to a few sets of multiple choices answers for questions asking about age, frequency, and type of injuries. Another type of answer option adapted the 5-point Likert-type Scale, which consisted of “never,” “rarely,” “sometimes,” “most of the time,” and “always.” The process of development of this tool involved several workshops attended by experts from the Ministry of Health, Malaysia and the WHO representative for technical support within the year of 2011 to 2012. 15
The added scope in the GSHS was the “extended mental health” components to assess the level of depression, anxiety, and stress among adolescents using the DASS-21 (Depression, Anxiety and Stress Scale) questionnaire. The DASS-21 questionnaire was self-administered with a 4-point Likert-type scale response ranging from “0” to “3” points. It consisted of 3 domains to assess depression, anxiety, and stress, where each domain had 7 items each. The summed scores for each domain were multiplied by 2 as DASS-21 is a modified-simpler version of the DASS-42. The final scores of 14 and greater were used to categorize respondents into those suspected of having depression, scores of 10 and above for anxiety and scores of 19 and above for stress. 17
In-line with the evolution of information and technology via the internet, the scope of internet addiction was introduced in this survey. The Malay Version of Internet Addiction Test (MVIAT) is the validated version of the original questionnaire developed by Young et al 18 in 1998. The MVIAT consists of 20 items with a 5-point Likert-type scale. The response scale ranges from “1 = rarely” to “5 = always.” Guan et al observed that MVIAT had good internal consistency (Cronbach’s α = .91), intraclass coefficient = 0.88, P < .001, and concurrent validity with Compulsive Internet Use Scale (Pearson’s correlation = 0.84). Respondents who scored 43 and above points were considered as having internet addiction. 19
All the selected questionnaires were compiled into 1 booklet with a corresponding optical reader mark (OMR) answer sheet. Anthropometric measurements were taken using the TANITA HD-319 digital weighing scale and the Seca 206 Bodymeter. Unnecessary items such as socks or belts were removed prior to measurement. Each measurement was repeated twice, and the average was taken as the final reading.
Study Design and Sampling Frame
This survey applied a cross-sectional study design to capture data on health risk behaviors of secondary school students in Malaysia. Secondary school students were defined as adolescents from 13 to 17 years old who were studying in Form 1 until Form 5 based on the local school categorization. The national secondary schools registered in 2016 were used as a sampling frame including government schools and private schools under the purview of the Ministry of Education as well as schools under the Ministry of Rural and Regional Development.
Sample Size
The sample size was calculated to ensure statistically sound findings and representativeness of the sample, considering the available budget. Sample size was calculated according to each objective using a single proportion formula based on previous Malaysian GSHS 2012 findings.
The initial calculated sample size nSRS based on the lowest prevalence figure was adjusted for the total number of the target population (based on the enrolment data of school-going adolescents in 2016), a design effect of 2 and expected nonresponse rate of 25%. The lowest prevalence used was 3.0% and a total sample of 1906 adolescents per state was required. In total, 30 496 adolescents aged 13 to 17 years were required to be recruited for this study. The number of selected schools are shown in Table 1.
Distribution of Secondary Schools Sampled by State.
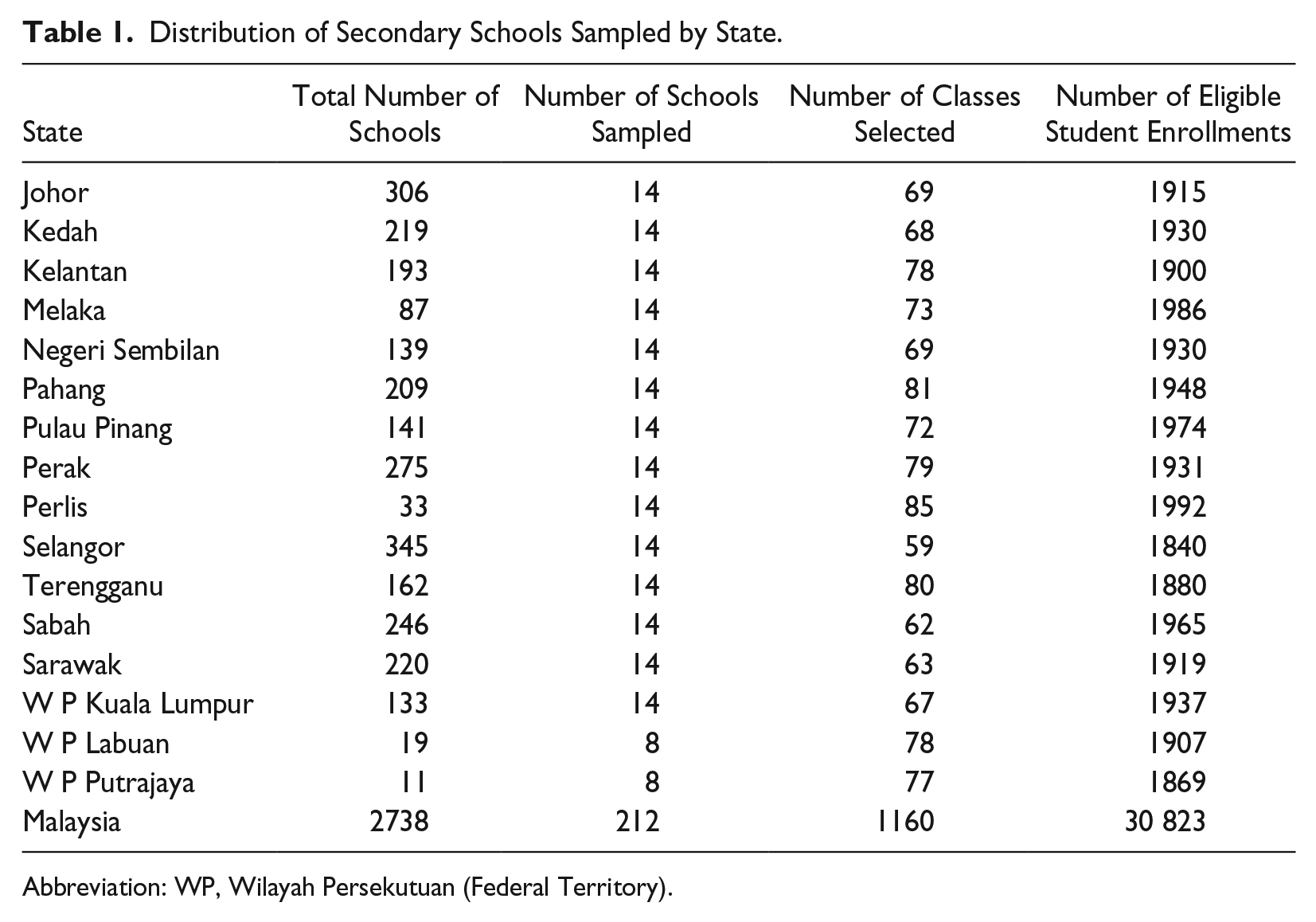
Abbreviation: WP, Wilayah Persekutuan (Federal Territory).
Sampling Design
Malaysia was stratified into 13 states and 3 Federal Territories. The sampling design was 2-stage stratified cluster random sampling to ensure the national representativeness of the chosen sample. The selection of schools and classes were performed using systematic random sampling. Schools were selected randomly with probability proportionate to school enrolment size, whereas classes were selected using systematic random sampling. The primary sampling unit was the school and classes were the secondary sampling unit. The list of classes for selected schools made up the second sampling frame. The class was selected by the central team, with an average of 5 to 6 classes per school. All students in the selected classes were eligible to participate in the survey.
Ethical Approval and consent Forms
The initial approval was obtained from the Medical Research and Ethics Committee (MREC) of the Ministry of Health, Malaysia (NMRR-16-698-30042) followed by approval from the Educational Planning and Research Division, Ministry of Education. The permission to conduct the survey was approved by the various State Education Departments and principals of the selected schools. A few meetings were conducted with the teachers to inform them about the survey, as well as to distribute parental consent a month before data collection at the respective schools. Student and their parents’ consents were collected just prior to the actual day of survey.
Field Implementation
A central team oversaw the implementation of the survey overall, while data collection teams consisted of 36 teams; 2 teams for each state in Peninsular Malaysia and 4 teams for Sabah and Sarawak during the 6-week data collection period (March 26 until May 6 2017). A field supervisor was assigned for each state to supervise the survey activities including facilities for data collectors. Data collectors were trained during a 1-week workshop prior to the survey. The central team monitored survey progress, besides providing technical and logistic support to the data collection teams in the field. On the day of appointment with the school, the survey was conducted either in the classroom, school hall, or canteen. The respondents were provided with the questionnaire booklet, OMR forms, pencil, eraser, and envelope. About 45 minutes to 1 hour were allocated to complete the survey. The answered OMR form was put in the envelope by each student to maintain confidentiality. The anthropometry measurement was conducted concurrently, and the respondents were given the result immediately to be filled in the OMR form.
Field Quality Control
The data collectors at the field were responsible for quality control by ensuring correct identification numbers (ID) of the respondents. The consent and OMR forms were packed together according to the list of visited schools.
Central Operation Center
The operation center was divided into 4 stations. Bundles containing the OMR forms and consent forms from the field were received by Station 1. The schools’ ID, class ID, and students’ ID were checked and compared with the original lists. Any discrepancy was referred to the team leader for clarification before sending the checked OMR forms to Station 2 for data scanning. Data verification was conducted at Station 3 before the final data were exported to the database. The fourth and final station was the OMR form questionnaire storage.
Data Analysis
Data analysis was conducted using IBM SPSS Statistics for Windows, Version 21.0. (IBM Corp, Armonk, NY). 20 The raw dataset in Microsoft Excel format was exported to SPSS. The data was checked for inconsistencies and cleaned if there were illogical sociodemographic findings especially in terms of age. The sample weight was calculated to adjust the sample data for ensuring sample representativeness in line with complex sampling analysis method. The weight used for the sample weight estimation was given as follows:

where W1 is the inverse of the probability of selecting the school; W2 is the inverse of the probability of selecting the classroom within the school; F is the inverse of the response rate of school level, class, and student; and PW is the poststratification adjustment factor based on gender and form of the students. The data analysis was conducted based on the objectives, working definition and dummy tables. Descriptive analysis was presented with 95% confidence intervals while analytical analysis was tested by paired t test, χ2, and logistic regression.
Results
The school response rate was 100%. The student’s response rate was 89.2 % based on 30 823 eligible respondents. A total of 27 497 OMR forms were received from 212 selected schools. The population estimation between AHS sample and national enrolment were compared as shown in Table 2. Geographic information system (GIS) on the mapping of selected secondary schools is shown in Figure 1.
Comparison Between AHS 2017 Respondents and National Enrolment of Secondary School Students in Malaysia, 2017.
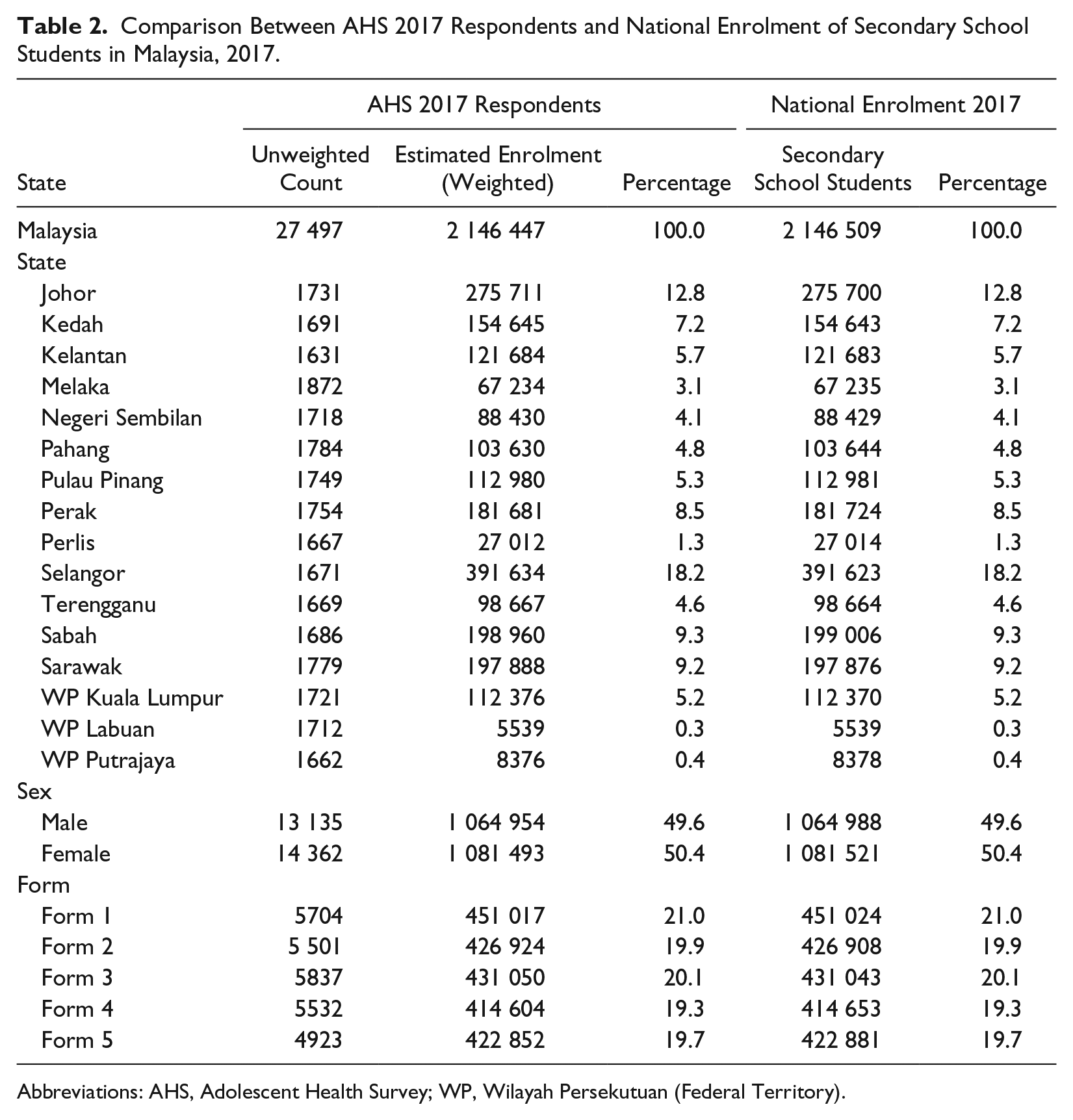
Abbreviations: AHS, Adolescent Health Survey; WP, Wilayah Persekutuan (Federal Territory).
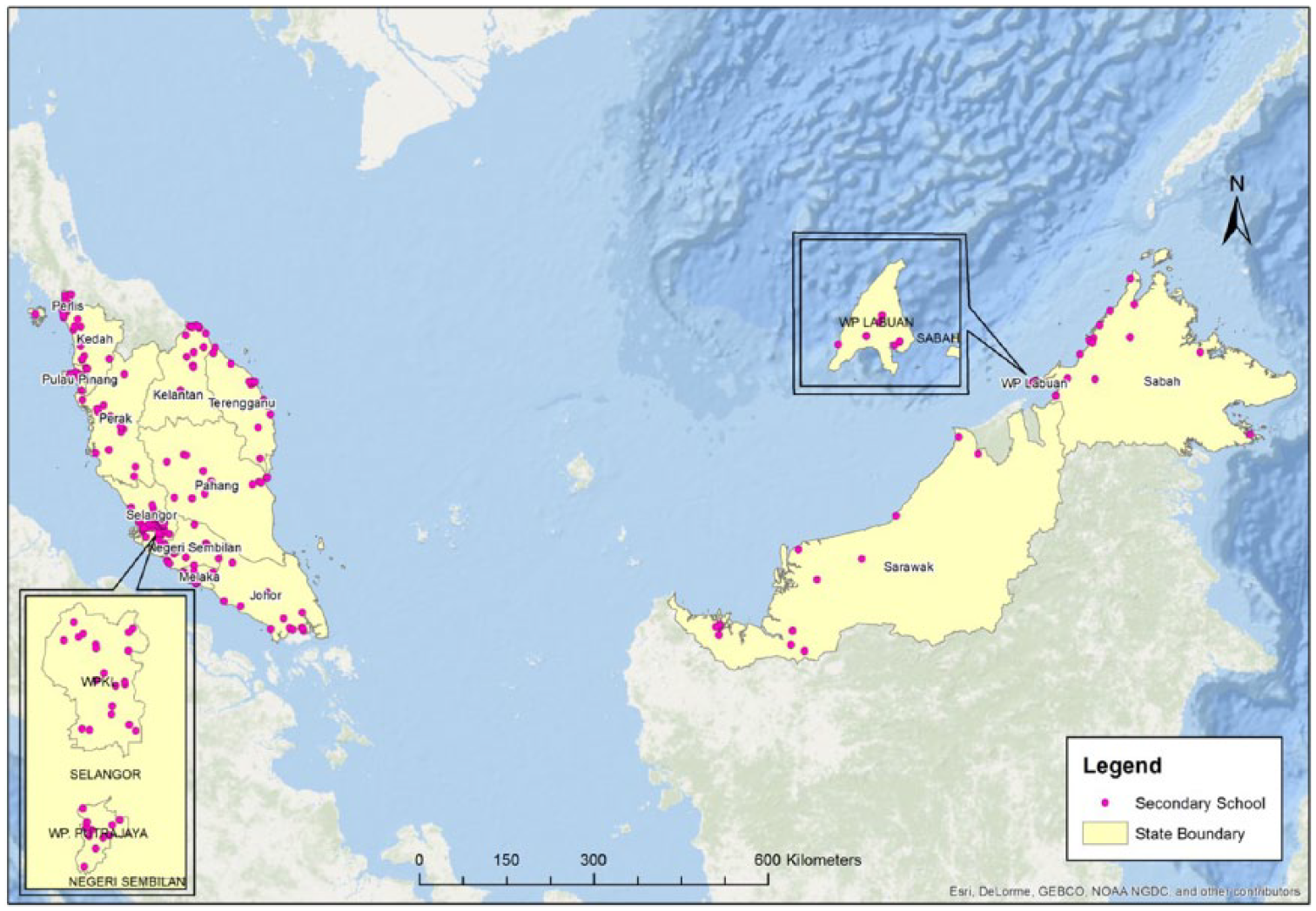
Geographic information system (GIS) mapping of the selected secondary schools in Adolescent Health Survey (AHS) 2017.
Discussion
Globally, the adolescent health survey is conducted routinely to monitor the trends of health risk behavior aiming to improve the adolescent health status using renowned surveys such as HBSC and GSHS.7,8 Majority of adolescents aged 10 to 19 years were in school thus the national school frame was the most practical in terms of feasibility, time management, and response rate compared with a household survey. The targeted age (13-17 years) for health risk behavior assessment was suitable as adolescents of this age can understand the terms used in the questionnaires and gave valid answers compared with those younger than 10 to 12 years old. 21
The target age for the HBSC survey were those at 11, 13, and 15 years as each group represented specific school grades with part of their milestones in lower secondary education where more life challenges were to be faced at these grades.8,22 Certain countries developed their own survey adapted from this renowned study to suit their adolescents such as the India Adolescent Health Survey and school-based surveillance system entitled CASPIAN-III Study in Iran.23,24 Another study to measure health risk behaviors among adolescents in the United States was the Youth Risk Behavior Surveillance System (YRBSS). The sample population was high-school students aged 15 years and above. The questionnaire measured prevalence of unintentional injuries and violence; tobacco, alcohol, and drug use; sexual behaviors; dietary behaviors and physical inactivity using the self-administered method; and computer scannable answer sheets. 25 The use of self-administered questionnaires should increase the rate of disclosure about their behavior.26,27 For international comparison and trending, countries should use similar aged group of respondents and questionnaire.
The response rate for school-based surveys generally was good as observed by the overall 89.2% in this study. The Thailand GSHS 2015 reported a response rate of 89% while Cambodia’s GSHS 2018 was 85%. 7 The Irish HBSC 2014 reported 59% of school’s response rate and 84.5% of student’s response rate. 28 The response rates were comparable between the countries that participated either in the GSHS or HBSC. The GSHS was considered the lower cost nationwide survey to monitor adolescents in low- and middle-income countries and enable comparison among the participating countries.
Strengths and Limitations
This survey used complex sampling design and sample weight calculation to represent the Malaysian adolescent population. The findings are internationally comparable as it used sets of questionnaires (GSHS, DASS, and MVIAT), which have been used widely in developed to developing countries. This survey observed an interministry collaboration for gathering data among adolescents and should be continued with preventive programs taking place in schools. This is the best strategy to target problematic students via school intervention. The use of self-administered questionnaire increases the chance of self-disclosure of health risk behaviors among adolescents. However, the cross-sectional study design limits the causal relationship of the predictors with the various health outcomes. The targeted age of 13 to 17 years limits the chance of younger adolescent who have engaged in health risk behaviors to be detected earlier. Although this survey methodology is unable to cater for the drop out adolescent, the findings still representing most of the Malaysian adolescents.
Conclusion
The methodology of this survey is reproducible for future studies on health risk behavior among adolescents. The findings can be inferred to the population thus, the estimation of health risk behavior is vital to understand the current burden in managing the adolescent health program.
Footnotes
Acknowledgements
The authors would like to express our gratitude to the Director General of Health Malaysia and the National Health and Morbidity Survey (NHMS) Steering Committee Team for supporting this research. We also would like to thank Director General of Education, Ministry of Education Malaysia for the permission to conduct the survey in school setting and to those who involved in this research team and the students who joined the survey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This survey was totally funded by Ministry of Health Malaysia research grant including the publication fees.