
Abstract
Background
While workers’ compensation (WC) patients often experience worse orthopedic outcomes, complication patterns following distal radius fracture (DRF) open reduction and internal fixation (ORIF) remain poorly defined. Prior DRF-specific studies include only small, regional cohorts. This study leverages Epic Cosmos to conduct the first nationwide analysis comparing complications between WC and non-WC populations.
Methods
This retrospective study queried the Epic Cosmos database for DRF ORIF procedures (2017–2024). WC patients (N = 4,101) were matched 1:5 with non-WC patients (N = 20,505) based on demographic and comorbidity characteristics. Patients required ≥6-month follow-up (mean 48.2 ± 28.6 and 48.9 ± 27.3 months for WC and non-WC patients, respectively). A subgroup analysis excluding patients with prior tendon injuries evaluated if WC status independently contributed to complication risk.
Results
WC patients had higher odds of complex regional pain syndrome (CRPS) (1.6% vs. 0.8%; OR 2.17, 95% CI [1.60, 2.91],
Conclusions
WC status is associated with higher risks of CRPS, subsequent hardware removal, and stiffness. Notably, CRPS risk remains elevated even after controlling for prior tendon injuries. As the largest WC-specific complication analysis for DRF ORIF to date, this exploratory study suggests that payer status may be a clinically meaningful correlate of postoperative morbidity. Future prospective studies are needed to confirm these associations.
Introduction
Management of distal radius fractures (DRFs) constitutes a substantial portion of orthopedic practice. While most distal radius fractures are managed non-operatively, ORIF is the most frequently selected operative treatment, followed by external fixation and closed reduction with percutaneous pinning (CRPP) in select cases. 1 While surgical techniques have advanced considerably, patient outcomes are influenced by a multitude of factors beyond the technical success of the procedure. A growing body of evidence suggests that socioeconomic and system-level variables, such as a patient’s workers’ compensation (WC) status, may play a profound role in postoperative recovery.2–8 Patients within the WC system have consistently demonstrated inferior outcomes across a range of orthopedic procedures, including those involving the spine,3,4,9–11 upper extremity,5,12–16 and hip. 17 Nevertheless, the complication profile following DRF ORIF within this population has not been clearly delineated in a large, nationwide cohort.
Previous studies have investigated a range of postoperative outcomes for WC patients, including quality of life,2,11 patient satisfaction,3,11 surgeon personal judgment, 2 return to work,3,11 and time off work. 12 While large meta-analyses of WC outcomes exist for other orthopedic procedures, the DRF-specific literature remains limited to small, regional cohorts or claims data, impeding generalizability and the ability to assess rare but clinically meaningful complications. Therefore, there remains a need to analyze more concrete postoperative outcomes, such as objective postoperative complications, using a large, nationally representative dataset. Specifically, within upper extremity surgery literature, there remains a major gap in the literature regarding DRF ORIF outcomes among the WC patient population.
The purpose of this study was to leverage a large, nationwide database to analyze data from WC patients undergoing DRF ORIF and compare complications between WC and non-WC patients. We hypothesized that WC status would be associated with a higher risk of postoperative complications, specifically stiffness and complex regional pain syndrome (CRPS) following distal radius fracture ORIF. This hypothesis is supported by documented WC effects on broader orthopedic outcomes,2–4,6,18 mechanistic pathways linking WC status to impaired healing,7,8 and established DRF ORIF complication baselines. 19
Materials and methods
A retrospective cohort study was conducted using de-identified patient data from the Epic Cosmos database, a multicenter network aggregating electronic health records from over 300 million patients across participating U.S. health facilities. The study was conducted in compliance with the database’s data use agreement and was exempt from institutional review board approval due to the de-identified nature of the data. All analyses were performed in R (version 4.5.1). Postoperative complications were compared using Fisher’s exact test, selected over the chi-square test because several outcomes had very low event frequencies despite the large overall cohort size, for which the chi-square approximation may be unreliable. To account for the number of outcomes examined, a Bonferroni correction was applied across all 16 complication comparisons, resulting in a corrected significance threshold of 0.003.
The Epic Cosmos database was queried on 10th June, 2026. Adult patients who underwent DRF ORIF between January 1st, 2017 and December 31st, 2024 were identified using Current Procedural Terminology (CPT) codes: 25607 (extra-articular), 25608 (intra-articular with 2 fragments), and 25609 (intra-articular with 3+ fragments). Patients with ICD-10 codes for pathological fractures (M84.5) or neoplasms (D49) or uncertain insurance status were excluded. To prevent inclusion of patients lost to follow-up immediately after surgery, only those with a minimum of 180 days (6 months) of continuous records post-index procedure were included. This threshold was selected to ensure sufficient postoperative surveillance to capture clinically meaningful complications, including those with delayed presentation such as hardware-related issues and postoperative stiffness, while the one-year window defined the outer boundary of the complication assessment period. To confirm adequate longitudinal follow-up, patients were additionally required to remain active in the Cosmos database for a minimum of two years following the index procedure, ensuring continuous data availability well beyond the one-year surveillance period. Patients with masked or missing sex, race, body mass index, or insurance status were also excluded; the complete cohort-selection process, including all exclusions, is summarized in Figure 1. Cohort selection flow diagram. Adult patients who underwent distal radius fracture open reduction and internal fixation (2017–2024) were identified in the Epic Cosmos database and screened against the study exclusion criteria; eligible workers’ compensation and other-payer patients were then matched 1:5 by nearest-neighbor propensity-score matching.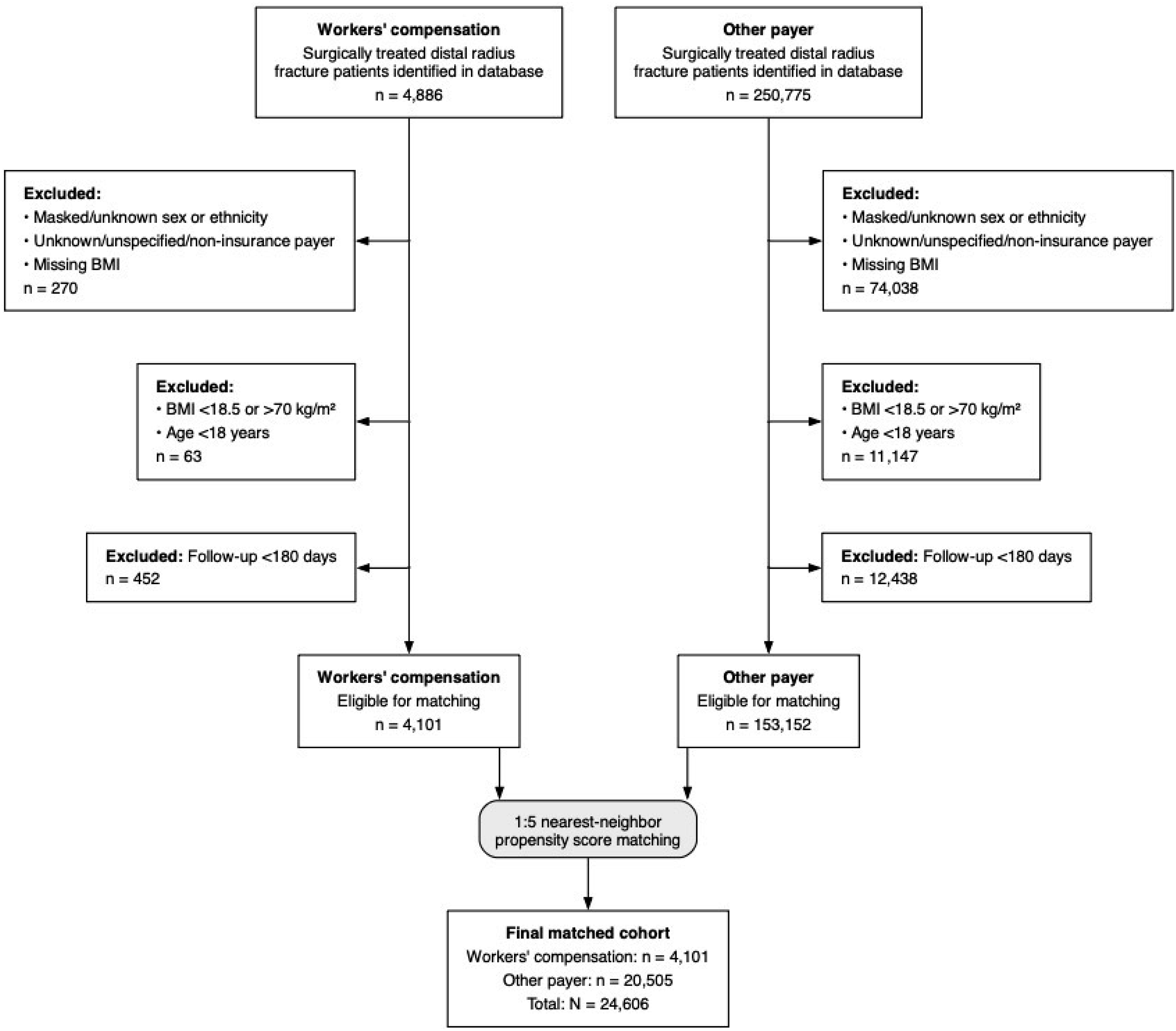
Patient demographics and comorbidities before and after matching (primary cohort).
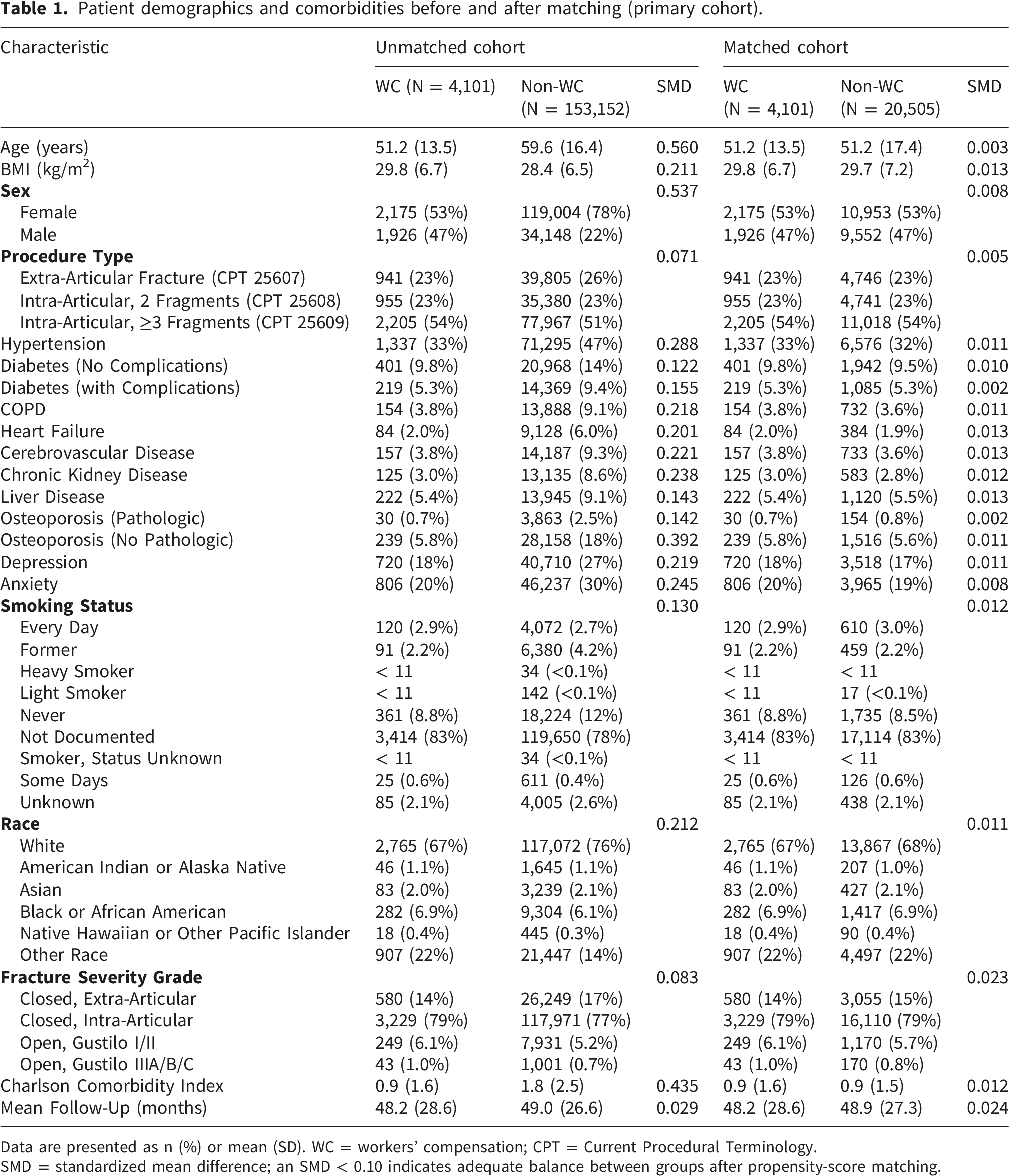
Data are presented as n (%) or mean (SD). WC = workers’ compensation; CPT = Current Procedural Terminology.
SMD = standardized mean difference; an SMD < 0.10 indicates adequate balance between groups after propensity-score matching.
Primary analysis compared the following postoperative complications within 1 year of surgery. Postoperative complications were identified using ICD-10 or CPT codes: CRPS (G90.50, G90.51, G90.59), postoperative stiffness (M25.63, M25.64), myocardial infarction (I21), stroke (I63), acute kidney injury (N17, N18, N19), nonunion (S52.90XK, S52.90XJ, S52.90XM, S52.90XN), malunion (S52.90XP, S52.90XQ, S52.90XR), skin/soft tissue infection (L00-L08), deep vein thrombosis (I82.40, I82.4), sepsis (A41.89, A41.9), wound disruption (T81.30, T81.3), vessel/nerve injury (S45, S45.9, S44), pulmonary embolism (I26), mechanical complication (T84.1), and subsequent hardware removal (CPT: 20680). This procedure was used as a nonspecific proxy for symptomatic hardware or soft-tissue complications.
A post-hoc subgroup analysis was performed to exclude patients with a history of tendon injury. Patients were excluded based on the presence of ICD-10 codes indicating traumatic injury to the flexor or extensor tendons of the forearm, wrist, or hand (S66.0-S66.9 and S56.0-S56.9; excluding S66.6 and S56.6), as well as spontaneous tendon ruptures (M66.241, M66.242, M66.249, M66.341, M66.342, M66.349).
Results
Demographics
Patient demographics and comorbidities before and after matching (tendon injury exclusion subgroup).
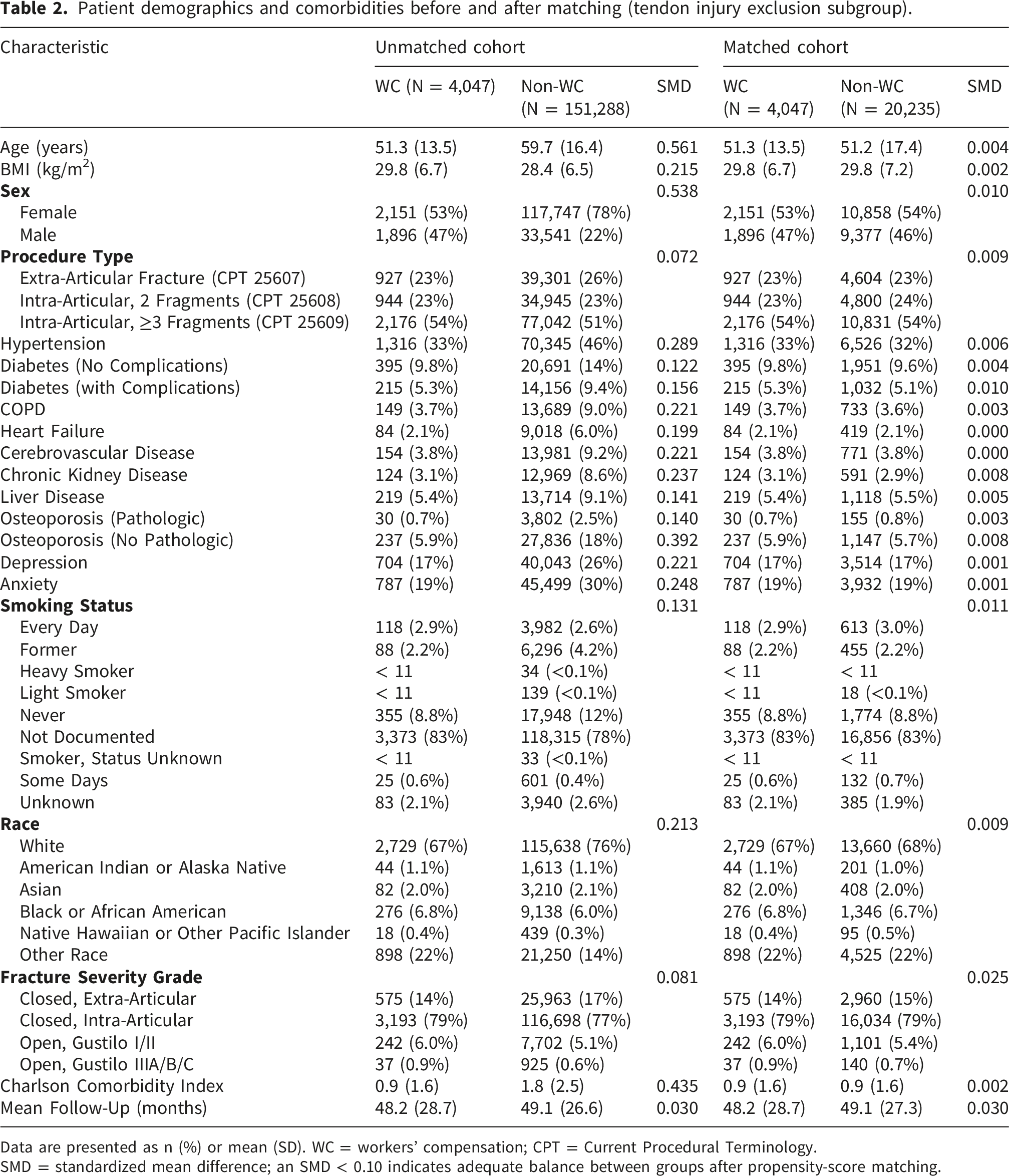
Data are presented as n (%) or mean (SD). WC = workers’ compensation; CPT = Current Procedural Terminology.
SMD = standardized mean difference; an SMD < 0.10 indicates adequate balance between groups after propensity-score matching.
Complication rates
Fisher’s exact test of postoperative complications in the primary matched cohort.
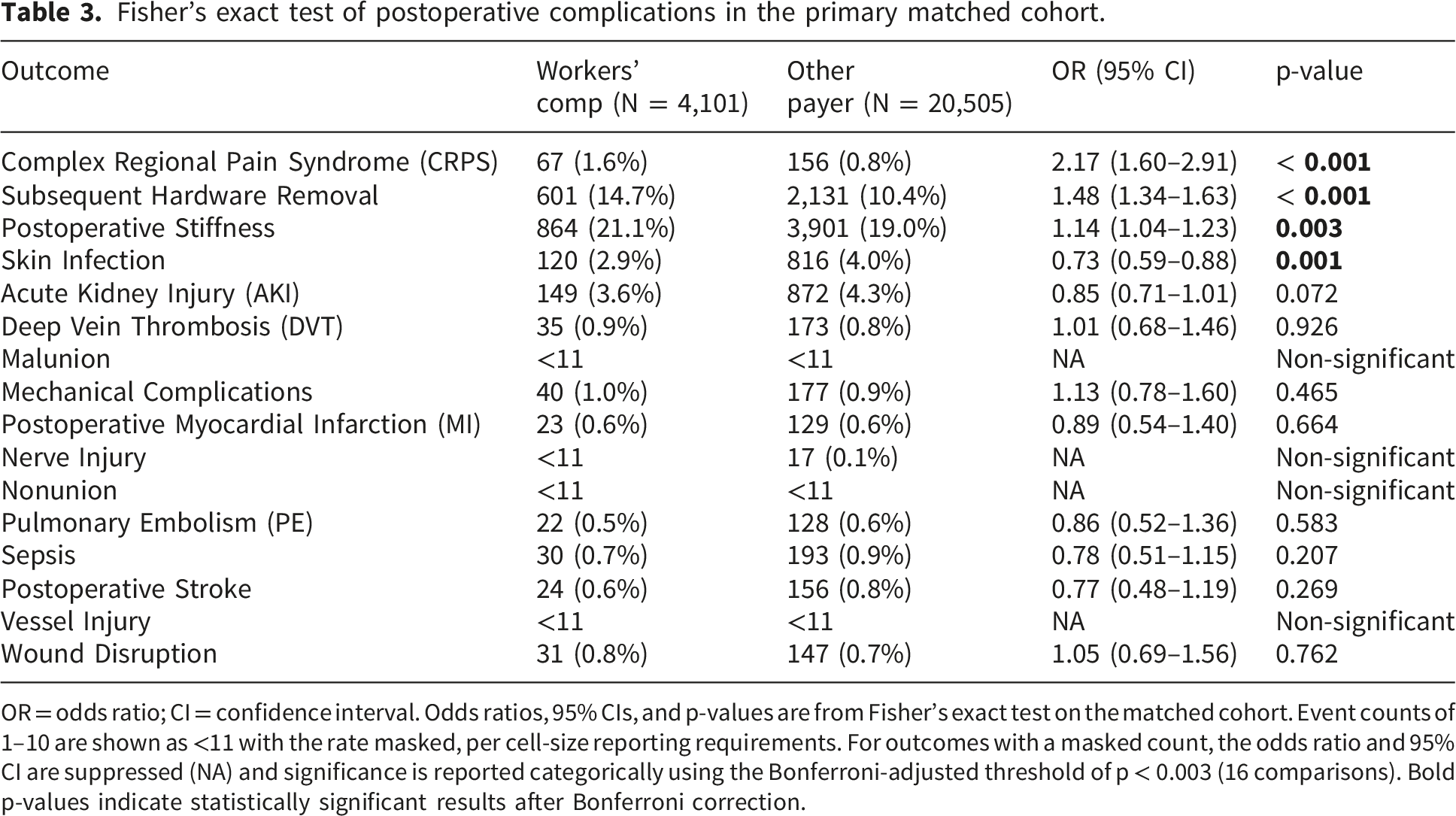
OR = odds ratio; CI = confidence interval. Odds ratios, 95% CIs, and p-values are from Fisher’s exact test on the matched cohort. Event counts of 1–10 are shown as <11 with the rate masked, per cell-size reporting requirements. For outcomes with a masked count, the odds ratio and 95% CI are suppressed (NA) and significance is reported categorically using the Bonferroni-adjusted threshold of p < 0.003 (16 comparisons). Bold p-values indicate statistically significant results after Bonferroni correction.
Subgroup analysis
A post-hoc subgroup analysis excluding patients with prior tendon injury was performed. After applying these exclusion criteria, 4,047 WC patients were matched to 20,235 non-WC patients. Cohorts were well-matched, as indicated by balanced baseline characteristics and SMDs less than 0.1 (Table 2).
Fisher’s exact test of postoperative complications in the subgroup analysis.
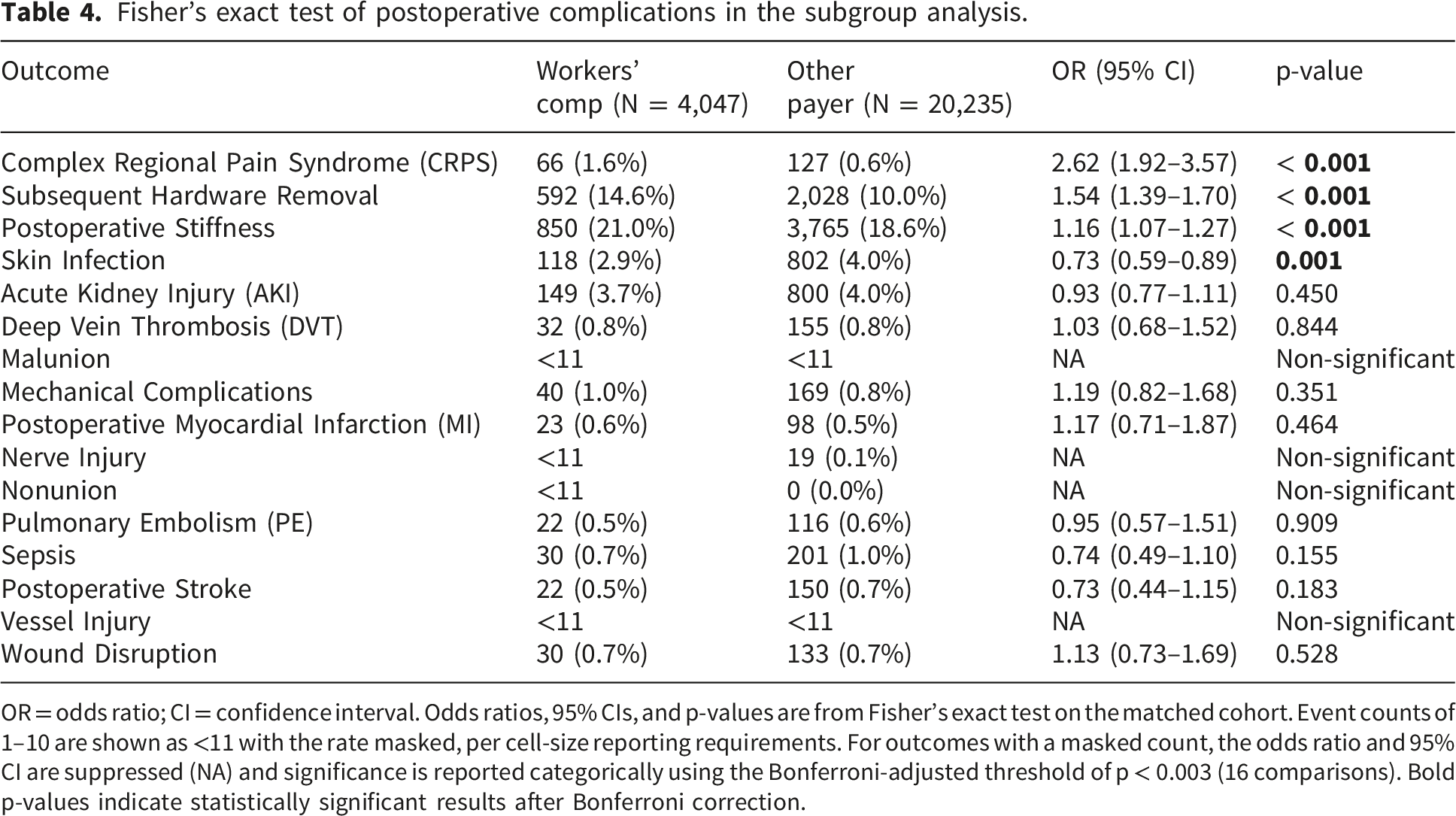
OR = odds ratio; CI = confidence interval. Odds ratios, 95% CIs, and p-values are from Fisher’s exact test on the matched cohort. Event counts of 1–10 are shown as <11 with the rate masked, per cell-size reporting requirements. For outcomes with a masked count, the odds ratio and 95% CI are suppressed (NA) and significance is reported categorically using the Bonferroni-adjusted threshold of p < 0.003 (16 comparisons). Bold p-values indicate statistically significant results after Bonferroni correction.
Discussion
Although WC status is broadly recognized as a risk factor for poor orthopedic outcomes, its specific impact on complications following DRF ORIF remains understudied. Previous literature has largely relied on small, regional cohorts or subjective measures, limiting statistical power and generalizability. To address this gap, we utilized a large, nationwide database to compare objective postoperative complication rates between matched WC and non-WC DRF ORIF patients.
This study, leveraging Epic Cosmos, suggests that workers’ compensation status is associated with increased adverse outcomes following DRF ORIF. Our analysis demonstrates that after controlling for a host of demographic and clinical variables, WC patients have increased odds of developing several complications, including CRPS, subsequent hardware removal, and postoperative stiffness. The more than two-fold increase in CRPS (OR=2.17) is particularly concerning, as CRPS is associated with chronic pain and permanent functional loss. 20 The elevated rate of subsequent hardware removal (OR=1.48) represents a major setback in recovery, as patients are subjected to the risks, costs, and additional rehabilitation time associated with a second operation. Furthermore, although the increased risk of postoperative stiffness reached statistical significance (OR=1.14), the modest absolute difference (21.1% vs. 19.0%) warrants cautious interpretation given the large sample size, in which small differences can attain significance; nonetheless, it may still reflect a greater burden of morbidity, impairing functional recovery and often requiring prolonged, resource-consuming physical therapy. A subgroup analysis was performed to control for the potential confounding role of existing tendon injury. WC patients remained significantly more likely to experience CRPS (OR=2.62), to undergo subsequent hardware removal (OR=1.54), and to develop postoperative stiffness (OR=1.16) compared to non-WC patients, with all three associations surviving Bonferroni correction. This pattern suggests that the observed disparities are not solely attributable to patient-level health factors but may be influenced by systemic elements inherent to the workers’ compensation system. We hypothesize that the interplay between litigation stress, job insecurity, and fear of claim denial may create a psychosocial environment different from that of non-WC patients, which could contribute to increased postoperative complications. 8 Pain catastrophizing and related cognitive-behavioral factors, which are more prevalent among workers’ compensation claimants, may further mediate this relationship. 21
The findings from this study align with existing literature, which demonstrate that WC patients are more likely to experience complications and poorer orthopedic outcomes.3–5,9–17,22,23 In a single institution study, Lu et al. found that following biceps tenodesis surgery, WC patients scored lower on all post-operative patient-reported outcome measures, including shoulder function, quality of life, and mental health outcomes. 14 Additionally, in a small cohort study, WC patients who underwent arthroscopic rotator cuff repair had poorer compliance to protocol, worse postoperative outcomes, and increased postoperative pain compared to non-WC patients. 15 In concordance with our findings, Ortiz-Romero et al. found WC status to be a significant predictor of CRPS (OR=14.3) in 249 DRF ORIF patients at their single institution. 24 Our substantially lower effect estimate (OR=2.17) likely reflects our larger, propensity-matched cohort and more conservative, adjusted analysis. However, to our knowledge, our study is the first to examine the effect of WC status on postoperative complications following DRF ORIF using a large, matched cohort.
The results of this study offer a practical foundation for clinicians to refine WC patient care. These findings can inform preoperative counseling, allowing surgeons to set clearer expectations and discuss the non-surgical factors that may affect outcomes. The two-fold observed increase in CRPS suggests that a proactive approach may be beneficial in these patients. Potential risk-reduction strategies may include the implementation of early multimodal pain regimens and vigilant screening for neuropathic pain. Similarly, the elevated risk of postoperative stiffness suggests that accelerated rehabilitation protocols may help reduce morbidity. Structural features of the workers’ compensation system, such as wage replacement and extended leave, have been hypothesized to influence rehabilitation engagement and timely return to function, although these factors were not directly assessed in this study.6,18 Future studies utilizing patient-reported outcomes may clarify how psychosocial variables mediate the observed outcomes in this population.
This study has several limitations that warrant consideration. Due to the retrospective design of the study, we could not establish a causal relationship between WC status and postoperative complications following DRF ORIF. Our findings may also be vulnerable to follow-up bias, as WC patients may receive prolonged or more intensive postoperative surveillance mandated by claim processes, which could elevate the detection rate of complications. Use of medical records and administrative data may introduce coding inaccuracies for articular fractures, postoperative complications, and prior tendon injury. Moreover, to protect reliability and patient confidentiality, patient counts lower than ten were suppressed, leading to the inevitable disregard of some data points that may have been included if the sample were larger. Additionally, multiple factors that may influence postoperative complications were not taken into account, including postoperative physical and pharmacologic therapy compliance, injury severity, and time to surgery. WC patients may perform high-risk physical labor and have higher severity injuries on average than non-WC patients. Although fracture severity was assessed and balanced using available ICD-10 codes, these codes capture injury complexity imperfectly, and residual confounding from unmeasured differences in fracture severity therefore cannot be excluded and may have influenced the observed associations, given the known influence of fracture complexity on postoperative outcomes. Time to surgery could also vary between WC and non-WC patients due to delay in WC status verification and claims processing. Furthermore, our study used the CPT code for hardware removal as a proxy for symptomatic hardware-related complications. Specific operative indications cannot be individually verified, and it is possible that hardware was removed for other reasons, such as prominence without tendon irritation or patient preference. In workers’ compensation populations in particular, hardware removal may be driven by unexplained or persistent pain, administrative or claim-related factors, or elective considerations rather than confirmed tendon pathology, and this outcome should therefore be interpreted with caution and not equated with tendon irritation. Finally, the included analyses solely focused on objective information in medical records, such as CPT and ICD-10 codes and WC status. There is a potential for future studies to include more subjective, patient-reported outcomes, including subjective ratings of postoperative pain after DRF ORIF, quality of life, functional mobility, and satisfaction with care. Additionally, although a Bonferroni correction was applied to reduce the likelihood of type I error from the multiple comparisons performed, the number of outcomes examined and the exploratory nature of this analysis warrant cautious interpretation. The paradoxically lower odds of skin infection in WC patients is also counterintuitive and may reflect differences in postoperative surveillance, documentation, or unmeasured confounding rather than a true protective effect.
This study is the first large-scale nationwide analysis of DRF ORIF complications among WC patients, observing that WC status is associated with several postoperative complications. Specifically, markedly increased rates of CRPS and subsequent hardware removal were noted in WC patients, along with more modest elevations in postoperative stiffness. Crucially, even after controlling for prior tendon pathology, risk for CRPS remains significantly elevated in the WC population, indicating that these outcomes are not driven solely by injury complexity. These findings suggest that payer status may act as a marker of increased postoperative morbidity. Although no intervention was evaluated in this study, proactive management strategies for WC patients (such as transparent preoperative counseling, early multimodal pain control, vigilant neuropathic pain screening, and graded return-to-work planning) may warrant consideration and represent a potential area for future investigation. Given the exploratory and retrospective nature of this analysis, prospective multicenter cohort studies designed to better account for psychosocial, occupational, and injury-related confounders are needed to confirm these associations.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.