
Abstract
Objective:
Patients admitted to mental health services may exhibit behaviours of concern (BOCs) such as aggression, self-harm, absconding and sexual harm. BOCs can lead to restrictive interventions, which have adverse effects on patients, carers and staff. This paper aims to explore the nature and outcome of BOCs within an adult inpatient mental health setting.
Methods:
A retrospective audit was conducted at a metropolitan inpatient service between 1 August 2016 and 31 July 2017. The frequency, nature and outcomes of BOC episodes were described and thematic analysis was used to summarise BOC antecedents.
Results:
A BOC was documented for 179 (18.2%) patients who also showed high rates of drug abuse, homelessness and longer admission. Most self-harm and sexual harm events occurred outside of normal business hours. Medications and verbal de-escalation were commonly used interventions. Episodes of deliberate self-harm were likely to result in patient and staff injury or mechanical restraint, whereas aggression was associated with seclusion. Mental state, care engagement, physiological stress and situational stressor were identified as BOC antecedents.
Conclusion:
Multiple forms of BOCs were experienced with mental state, physical and interpersonal contributors identified. Improving multidisciplinary input into early assessment and treatment of BOC causes is needed to improve safety.
Patients are admitted to inpatient mental health services to maintain the safety of themselves and others. 1 Treatment may be involuntary and coercive, or patients may be highly distressed, fearful of others, or displaying impulsive and poorly reasoned behaviour potentially resulting in aggression, self-harm, absconding or sexual harm. 1 Such behaviours of concern (BOCs) can cause harm for patients, carers and worsen staff burnout and attrition.2,3 Furthermore, staff concern about BOCs is a common reason for restrictive interventions as shown in a South Australian retrospective audit. 1 Prevention and early non-restrictive intervention to BOCs is in keeping with the recently revised National Safety and Quality Health Service Standards to respond and recognise mental state deterioration. 4
Despite the importance of BOCs, outside of aggression, there is little research about the nature of their occurrence, antecedents, management practices and admission outcomes in Australia. This is pertinent given the Victorian Mental Health Complaints Commissioner recently recommended that sexual safety in the inpatient mental health setting needs urgent attention. 5 There is also an increasing number of presentations with recent methamphetamine use, which is associated with higher rates of aggression 6 ; however, its impact on other BOCs is yet known. Furthermore, existing research has focused on individual types; thus, it is unknown whether there are common characteristics of patients and their outcomes as suggested in the Safewards Model. 2
Better understanding of BOCs can aid mental health services in multiple ways. The information can be used in staff training to identify at-risk patients and intervene early. By knowing when and where BOCs commonly occur, it can better inform resource allocation. Furthermore, it will also help identify which interventions need further investment and interdisciplinary input. 7
Methods
Participants
We conducted a retrospective audit of all documented BOCs in the adult inpatient psychiatric unit at The Alfred between 1 August 2016 and 31 July 2017.
To compare, we audited all 981 patients (1356 episodes of care) admitted to the unit, who averaged a length of stay (LOS) of 16.0 days (SD = 21.2). The mean age was 38.7 years (SD = 11.5), with 551 males, 428 females and 2 intersex. Their diagnoses were schizophrenia (25.5%), other psychosis (16.6%), schizoaffective (12.7%), bipolar affective disorder (12.3%), affective disorder (10.9%), borderline personality disorder (6.2%) and for alcohol and other drugs (AOD) use (3.1%).
Procedure
This project was approved by the Hospital’s ethics committee.
All staff-reported BOC events were extracted from RiskMan, the state-wide incident reporting system. We also extracted data from the Alfred Psychiatry Seclusion Register to identify seclusion/restraint episodes.
We collected data using an audit checklist within an Excel spreadsheet. To ensure reliability, two mental health nurse researchers jointly extracted and cross-checked data for the first five episodes, then separately collected data from separate 6-month periods. Collected variables are shown in Table 1.
Information gathered via audit
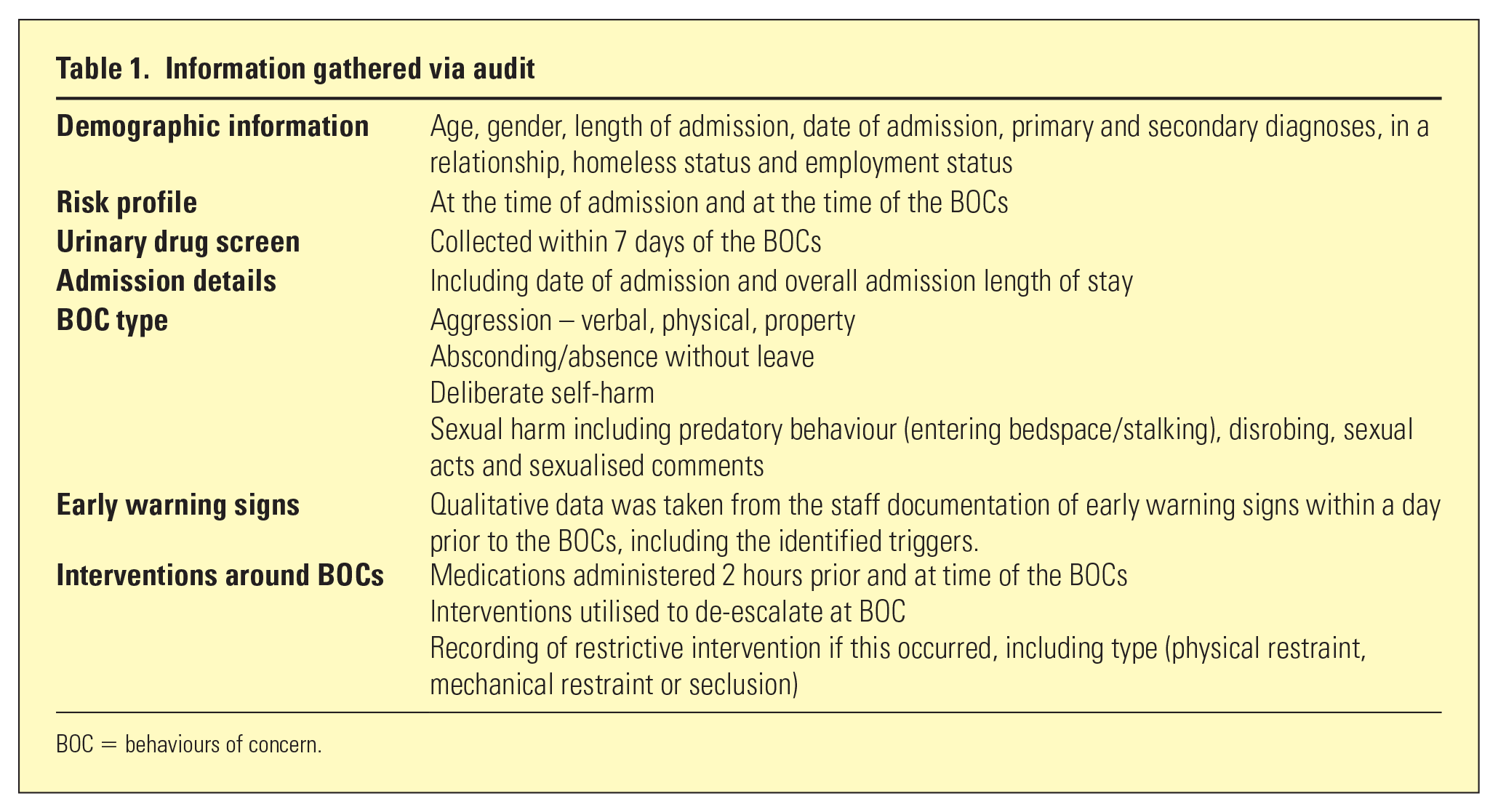
BOC = behaviours of concern.
Data analyses
Descriptive statistics were used to report patient characteristics, BOC form and frequency, and the nature of responses and adverse events. Thematic analysis of BOC antecedents was performed using text summarised for ‘early warning signs’. This was performed by MK, an inpatient psychiatry registrar, following Braun and Clarke’s six-stage method involving familiarisation with data, generation and collation of codes into themes, reviewing themes in relation to the data set and defining and reporting on the hierarchy. 8 The hierarchy was cross-checked by SL, an academic without inpatient clinical experience to protect against any bias in coding with feedback used to refine the structure and code/themes labels. All authors then viewed the coding hierarchy for relevance and completion.
Results
Characteristics of BOC episodes
Characteristics for patients involved and different forms of BOCs are presented in Table 2. LOS days was longer for patients engaging in BOCs (36.7) than the overall inpatient sample (16.0).
How patients engaging in BOC types differed
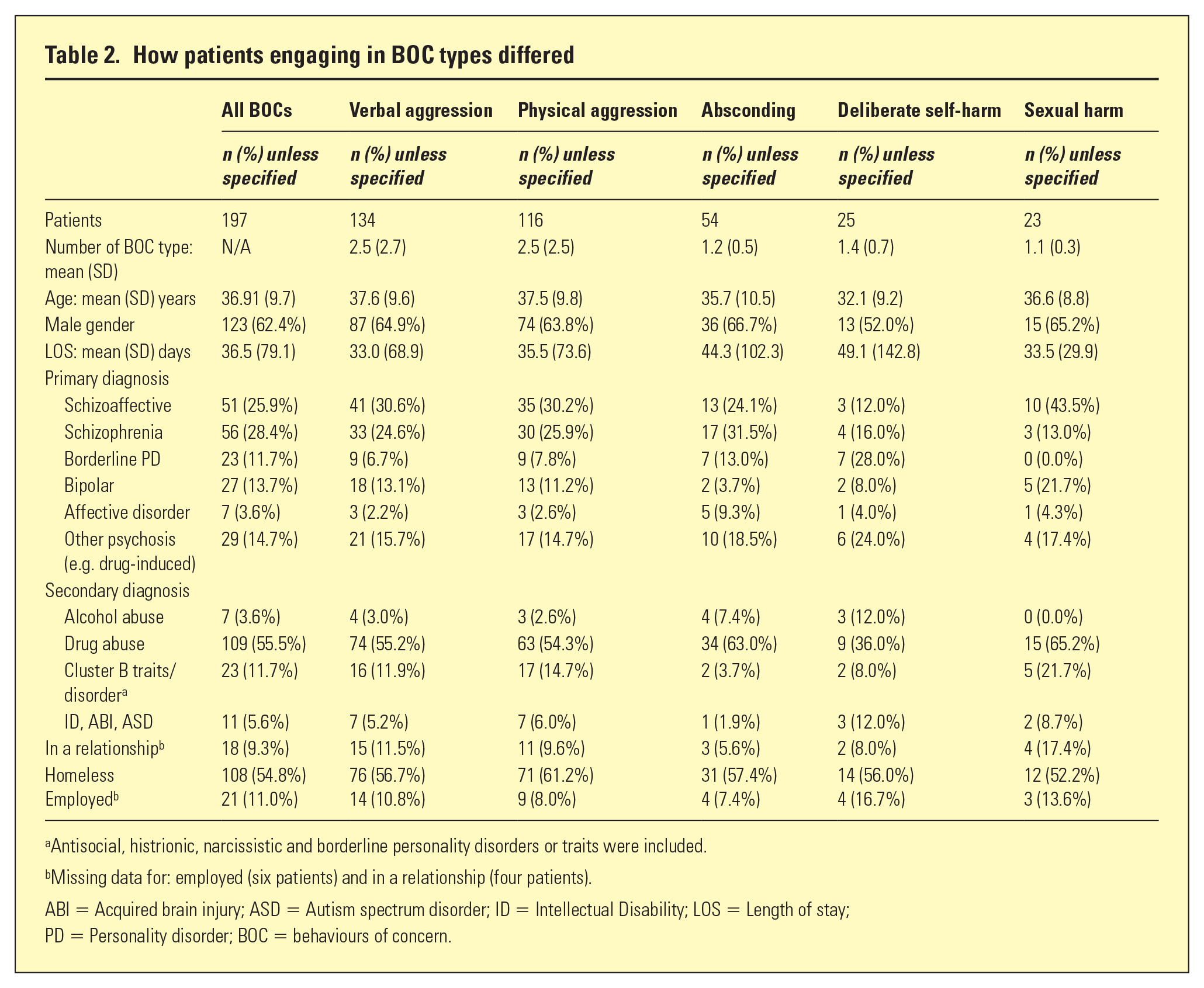
Antisocial, histrionic, narcissistic and borderline personality disorders or traits were included.
Missing data for: employed (six patients) and in a relationship (four patients).
ABI = Acquired brain injury; ASD = Autism spectrum disorder; ID = Intellectual Disability; LOS = Length of stay; PD = Personality disorder; BOC = behaviours of concern.
Table 3 summarises the BOC episodes by type, how they occurred and risk indicators present. As verbal and physical aggression frequently co-occurred, they were combined with ‘any aggression’.
Characteristics and risk indicators for all BOCs during the 12-month study period
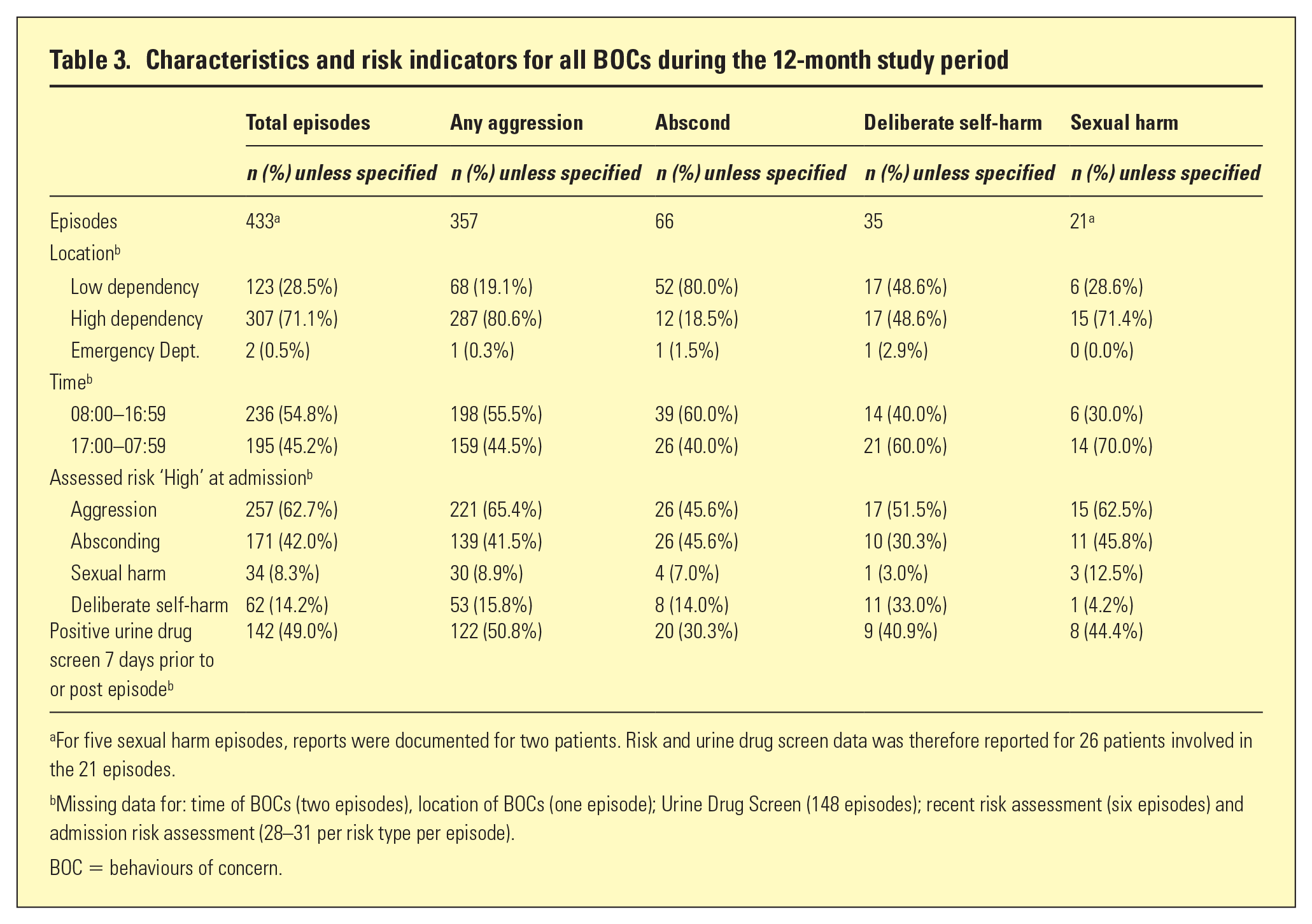
For five sexual harm episodes, reports were documented for two patients. Risk and urine drug screen data was therefore reported for 26 patients involved in the 21 episodes.
Missing data for: time of BOCs (two episodes), location of BOCs (one episode); Urine Drug Screen (148 episodes); recent risk assessment (six episodes) and admission risk assessment (28–31 per risk type per episode).
BOC = behaviours of concern.
Aggression and sexual harm episodes were more likely to occur within the high dependency unit, whereas absconding occurred most within the low dependency unit. For 290 of the total episodes, a urinary drug screen had been documented within 7 days of the episode occurring, and this was positive in almost half of these episodes.
Table 4 shows the management and outcomes for BOCs. Medication and verbal de-escalation were used most, whilst sensory modulation was used in approximately one quarter of the episodes.
Management and outcomes for all BOCs during the 12-month study period
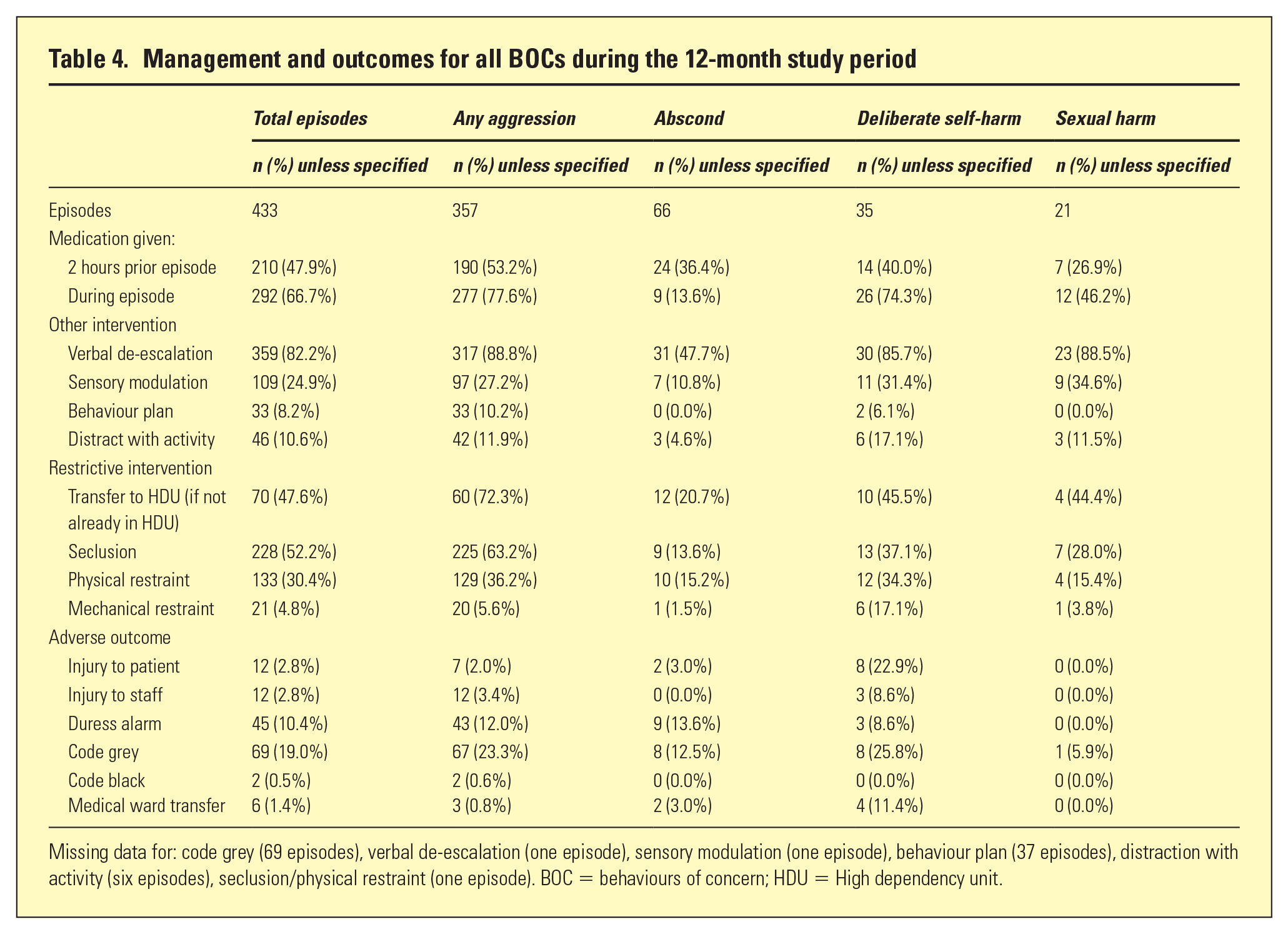
Missing data for: code grey (69 episodes), verbal de-escalation (one episode), sensory modulation (one episode), behaviour plan (37 episodes), distraction with activity (six episodes), seclusion/physical restraint (one episode). BOC = behaviours of concern; HDU = High dependency unit.
BOC antecedents
As shown in Table 5, four themes summarised BOC antecedents observed from the notes: engagement with care, mental state, physiological stress and situational stressors. A detailed comparison of how antecedents differed for the BOC types is beyond the scope of this paper. Instead, the overall antecedent hierarchy is shown to illustrate the diversity of contributing factors.
BOC antecedent themes and subthemes (code examples)
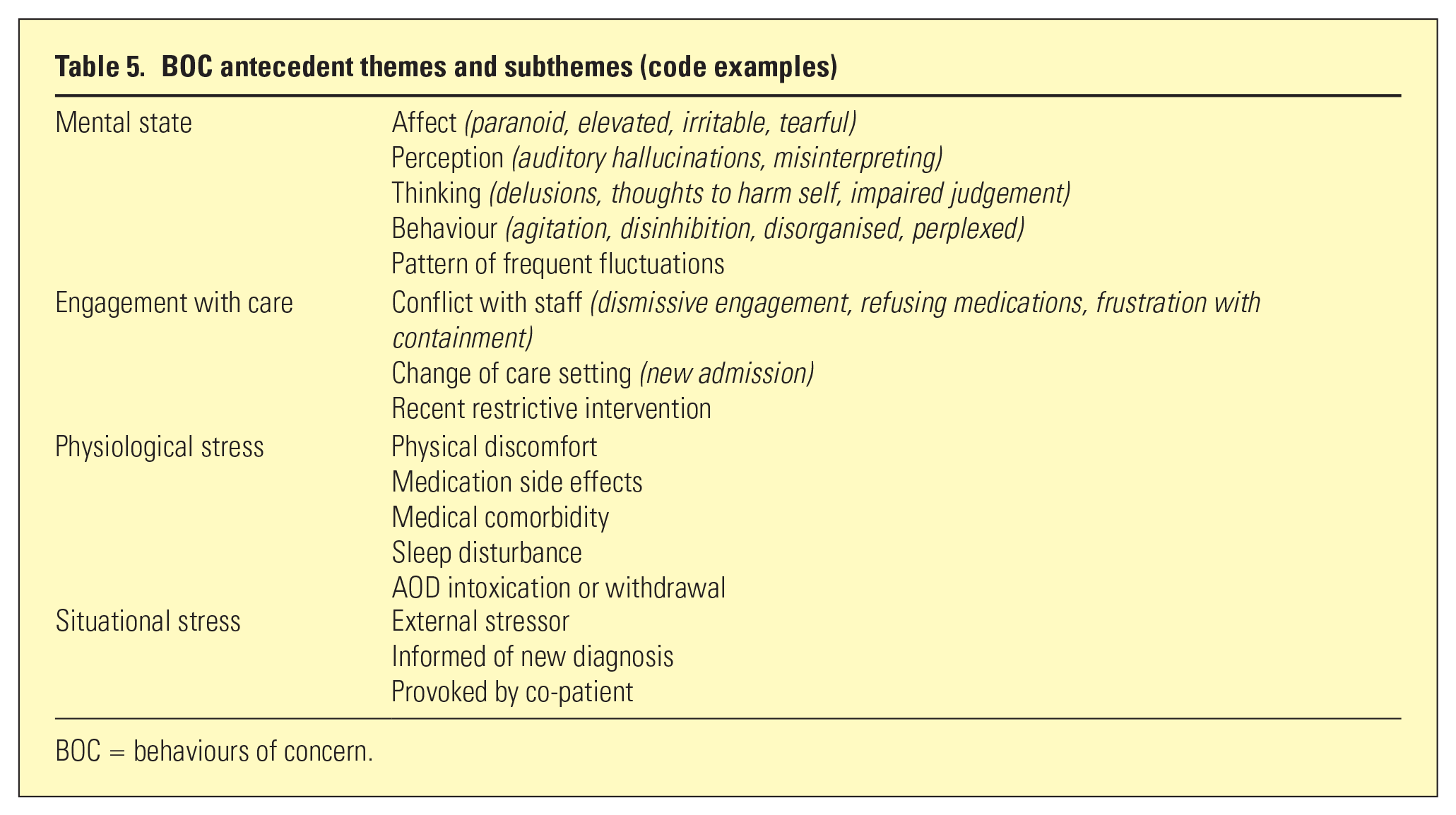
BOC = behaviours of concern.
As expected in a cohort of patients with psychiatric illnesses, mental state features often preceded BOCs. These pertained to a range of disturbances in thinking, perception, affect and behaviour. Fluctuation of their mental state was also often documented.
‘Aggressive in accommodation, carrying knife on self. Observed to be responding to be internal stimuli, and grandiose. Fluctuating presentation with bizarre behaviours’.
Delusional thoughts about being unsafe were often observed for patients involved in aggression.
‘(Patient) was fearful for life re: delusions (that) others are out to kill patient’.
Thought content, lability and beliefs about care also interacted in some aggressive patients.
‘(Patient was) delusional re: pregnant to 4 babies and psychic abilities. Labile, (ranging from) swearing at co-patient to pleasant and polite. Frustrated with containment and wanting to smoke’
Prior to self-harm episodes, emotional distress and expressed lack of available avenues for support were more often observed.
‘(Patient was) tearful and irritable. Seeking compassion from co-patient’s’.
Another identified theme was the engagement with care. This reflected the experience of physical boundaries such as change of care setting, restrictive intervention and conflict with staff about aspects of care.
‘Frustrated with containment and the inability to smoke’ ‘(Patient was) guarded in their mental state. . . (recently) de-secluded. Dismissive of lengthy engagement with staff’.
Physiological stress, including drug intoxication, sleep disturbance, physical pain and medication side effects were cited often as stressors contributing to irritability and agitation.
‘(Patient recently) transferred to LDU. Nil BOC. Appropriate. Expressing concern over dogs that have been stolen (reality) at group walk during escorted leave’
Life and interpersonal stressors also contributed to BOCs occurring. The following illustrates how concern about dependents, pets, housing or theft of belongings while in hospital was in particular an antecedent for absconding.
‘(Patient recently) transferred to LDU. Nil BOC. Appropriate. Expressing concern over dogs that have been stolen (reality) at group walk during escorted leave’
Witnessing or being a victim of aggressive or harassing behaviour from co-patients was also an antecedent for aggression.
‘Patient was thought disordered, perplexed, psychotic and provoked by co-patient escalating’
While the above examples illustrated aspects of the observed themes, also highlighted was the interplay of multiple antecedents. In many cases, mental state, physiological stressors (in particular drug-related) and negative beliefs about care escalated arousal.
‘(Patient was) restless, aggressive, irritable, volatile, hostile, uncooperative, intense stare. Ongoing psychosis and drug withdrawal. Threatening to rape staff, frustrated with containment and no smoking policy’
Discussion
This paper explored BOCs occurring in an Australian adult inpatient psychiatry setting to better understand their pattern, management strategies and outcomes. Aggression was the most frequent BOC, but multiple episodes of absconding, self-harm and sexual harm also occurred. Patients engaging in BOCs shared several factors such as high rates of substance and social comorbidities (e.g. homelessness) as well as negative attitudes towards hospital care. This likely increased the complexity of care as well as contributing to the occurrence of BOCs, which may explain the longer LOS being approximately 1 SD higher than the overall population.
Frustration with containment was a consistent antecedent, thus highlighting the need to address BOCs before they occur to avoid a longer LOS. Patients presenting with BOC may require access to physical spaces and structured groups to reduce their environmental stress and perception of coercive care which may exacerbate their behaviour. 2
This paper demonstrates the interplay among antecedent factors that contribute to emotional/behavioural dysregulation and associated enactment of harmful behaviours. This highlights the importance of tailored behaviour plans, which research has shown can be informed by use of tools that examine individual triggers and de-escalation interventions. 9 Furthermore, the low utilisation of sensory modulation suggests the need for greater multidisciplinary involvement. 7
Fluctuating mental state was another common BOC antecedent. This highlights the importance of regular monitoring of changes in arousal, attitudes towards care, interpersonal interaction, reasoning and control of behaviour, which could inform dynamic risk assessment and implementation of management plans for patients at risk. 10 These findings can be integrated into a training programme to better inform clinicians in detecting escalating patients to intervene and prevent potential complications.
A proportionally large number of patients engaging in BOC had a positive urinary drug screen, and were documented by staff to exhibiting drug intoxication, withdrawal and seeking-behaviour. This supports the increasing burden of illicit substance use in mental health services as suggested in another Australian study, 6 thus highlighting the need for AOD specialist input as part of the inpatient team. Furthermore, greater emphasis is needed for patients with AOD history to orient them to calm down spaces and opportunities to develop alternative coping strategies.
Preventative intervention may also be needed for people vulnerable to self-harm or sexual harm. Most self-harm and sexual harm episodes occurred outside of normal business hours (17:00–07:59). Given a typical service has less staffing and senior support during these hours, it highlights the need for better resourcing, especially given the impact of staff burnout and understaffing affect care delivery.1,3 This includes use of care zones (e.g. female-only spaces), self-harm specific crisis plans and increasing the amount of structured activities in the evening.
Limitations
This study has a number of limitations including use of routinely collected clinical data, where under-reporting of less serious aggressive behaviour is common. 11 Prospective studies with on-site BOC monitoring are needed to validate the findings. Repeating data collection in different services is needed to examine whether BOC frequency, antecedents, responses and outcomes is consistent. Conducting a double audit of all episodes would have strengthened data reliability, however, as both researchers were experienced mental health nurses and cross-checked their coding methods, this increased data quality.
As this study only presented descriptive data, statistical analysis was not used to examine if clinical/demographic risk factors were predictive of BOC forms, or episodes involving multiple BOC types. This will be examined in a future paper. The interaction among BOCs occurring in multi-BOC episodes needs further examination. While the proportion of staff injury was higher for episodes with self-harm than aggression (8.6% versus 3.4%), all three self-harm episodes also involved aggression, with the response to the identified self-harm escalating and resulting in aggression towards staff. The Safewards Model proposes that how conflict is responded to escalates or de-escalates perceived threat, distress, and subsequent patient behaviour. 3 Responses to inpatient self-harm should therefore prioritise understanding and addressing the causes of distress and establishing trust about how the person will be upskilled in coping with crises.
Conclusion
BOCs are common in inpatient mental health services. Although aggression was the most frequent, self-harm, sexual harm and absconding were present and associated with negative consequences. Several common factors relating to the antecedents and the event itself were identified, which can be used to better inform clinician training to build staff expertise in prevention and early intervention. Furthermore, these should be accompanied by provision of patient-oriented interventions and systems for monitoring change in risk to improve safety.