
Abstract
Background
Prisoners experience disproportionately high rates of mental illness. The incarceration rate in the Northern Territory (NT) is five times the national average but there is no existing research regarding the prevalence of mental disorder in this population.
Objectives
This cross-sectional observational study aimed to examine the prevalence of mental illness and substance use disorders among NT prisoners.
Methods
310 adult prisoner files were analysed, using four electronic medical record databases which captured a person’s lifetime contact with healthcare services in the NT. Descriptive statistical techniques were used.
Findings
First Nations people comprised 90.6% of the sample. First Nations prisoners were significantly younger with a median age of 32 years versus 40 years Non-First Nations (U 2747, p = .004). The lifetime prevalence of mental illness was 64.5% (54.4% of men and 76.9% of women (X2 (1, N = 310) = 19.7 p < .001). Substance use disorder was the most common diagnosis (51.6% lifetime prevalence). 14.3% of men and 20.3% of women had previously been admitted to a psychiatric hospital.
Conclusions
Prisoners in the NT have higher rates of mental illness than the general population. Females significantly suffered more mental illness. Given the overwhelming representation of First Nations people, culturally appropriate mental health services are crucial.
Introduction
The rates of mental illness in prisons are well recognised globally to be disproportionately higher than the general population, with Australia being no exception. The Australian Institute of Health and Wellbeing estimates a lifetime prevalence of mental illness in the general population of 43%, compared with 51% in prisoners. 1 A metanalysis by Yee and colleagues found identified a lifetime prevalence mental illness in prisoners of 69%, and 9.1% for psychosis. 2
The Northern Territory (NT) has the highest incarceration rate in Australia, currently five times the national average and continuing to rise. 3 Australian prison populations are disproportionately made up of First Nations people but nowhere is the incarceration gap more stark than in the NT, where First Nations prisoners account for 88.6% of the prisoner population, despite accounting for only 26.3% of the general population. National data indicates that First Nations people make up 36% of incarcerated people as compared with only 3.6% of the general population. 4
Prison mental health services across Australia are inadequately resourced to service demand. 5 Ensuring adequate mental health services for incarcerated people is essential, not only due to principles of equivalence of care and human rights, but because prisoners with untreated mental illness are more likely to re-offend post-release and enter a cycle of recurrent incarceration.6–8
In the NT, there is no secure forensic mental health facility. Specialised services to support prisoners with mental illness and substance use disorder have recently been closed. Closed units include a residential rehabilitation service, and a secure unit providing residential disability care for persons found not guilty by reason of mental impairment or unfit to plead. 9
Despite high incarceration rates, there is no data in the existing literature regarding the prevalence of mental illness in this unique setting or the associated demographic factors. This paper intends to address some of these gaps in knowledge.
Methods
The aim of this cross-sectional observational study was to describe the prevalence of mental illness, including substance use disorder, in an NT prison population. The study design was approved by the local Human Research Ethics Committee, and the requirement for informed consent of participants was waived by the Committee.
Design and participants
Data was collected on 30 January 2024. At that time there were two prisons in the NT, Darwin Correctional Centre (DCC) and Alice Springs Correctional Centre (ASCC), housing a total of 2064 prisoners, 128 women and 1936 men. Both ASCC and DCC housed male and female prisoners of all security classifications and all legal statuses (sentence, remand, other). Due to the comparatively low numbers of female prisoners the entire female prisoner population was captured, comprising of 91 females in DCC and 37 in ASCC. To match group sizes, 91 male records were randomly selected from both DCC and ASCC respectively (n = 182), using a randomly generated list of the male prisoners for both DCC and ACC respectively and taking the first 91 prisoners from the list. If there were missing data sets, the next prisoner in the list was selected, giving a total of 310 records. Correctional records allow for data to be recorded only in a binary format (male or female), and of those captured no transgender or intersex prisoners were identified on review of healthcare records.
Procedure and measures
The lists were generated using prison population lists containing unidentified prisoner ID numbers. Prisoner IDs were searched in prison health electronic health records (Primary Care Information System) which linked to additional electronic health records: Community Care Information System (CCIS) which documents mental health and AOD medical records; Jadecare Clinical Work Station which documents hospital records; and the national electronic Health Record. Between these databases the majority of contact with healthcare services for a person in the NT over their lifetime could be captured.
Clinical information was collected from files over the course of 3 months in 2024. The researchers collected demographic information (age, gender, cultural background, address), any previous psychiatric inpatient admissions, mental health diagnoses, other relevant medical diagnoses and any current psychotropic medication prescription. Diagnoses were gathered from the patient file home page, with review of psychiatric consultations, discharge summaries, and clinic letters undertaken if a psychiatric history was identified but no diagnosis or a non-diagnostic term was listed on the home page. Diagnoses were grouped in accordance with the Diagnostic and Statistical Manual of Mental Disorders, fifth edition, text revision (DSM-5-TR). 10
Data analysis
A descriptive study was undertaken of the demographic data for prisoners in the NT and the relationship to mental disorder.
Statistical analysis
All statistical analyses were performed using Jamovi (version 2.6), an open-source statistical software. 11 Data was firstly descriptively reviewed with gender (male vs female) as the main comparator groups. Goodness of fit was analysed using Chi Squared (X2) testing for significance. This was to ensure consistency of distribution across the gender groups and the demographic data collected (First Nation Status, Residents and Age). Normal distribution was not assumed and non-parametric tests were utilised to review statistical significance. Chi Squared tests were used for comparisons of proportions and Mann–Witney U-Test for comparing means. Proportions were expressed as percentages (%) for categorical data and means with standard deviation (SD) for continuous data. Measures of centrality included both means (SD) and medians.
Results
Results are summarised in Tables 1 and 2
Demographics of a Northern Territory prisoner population on 31st January 2024 (n = 310). a
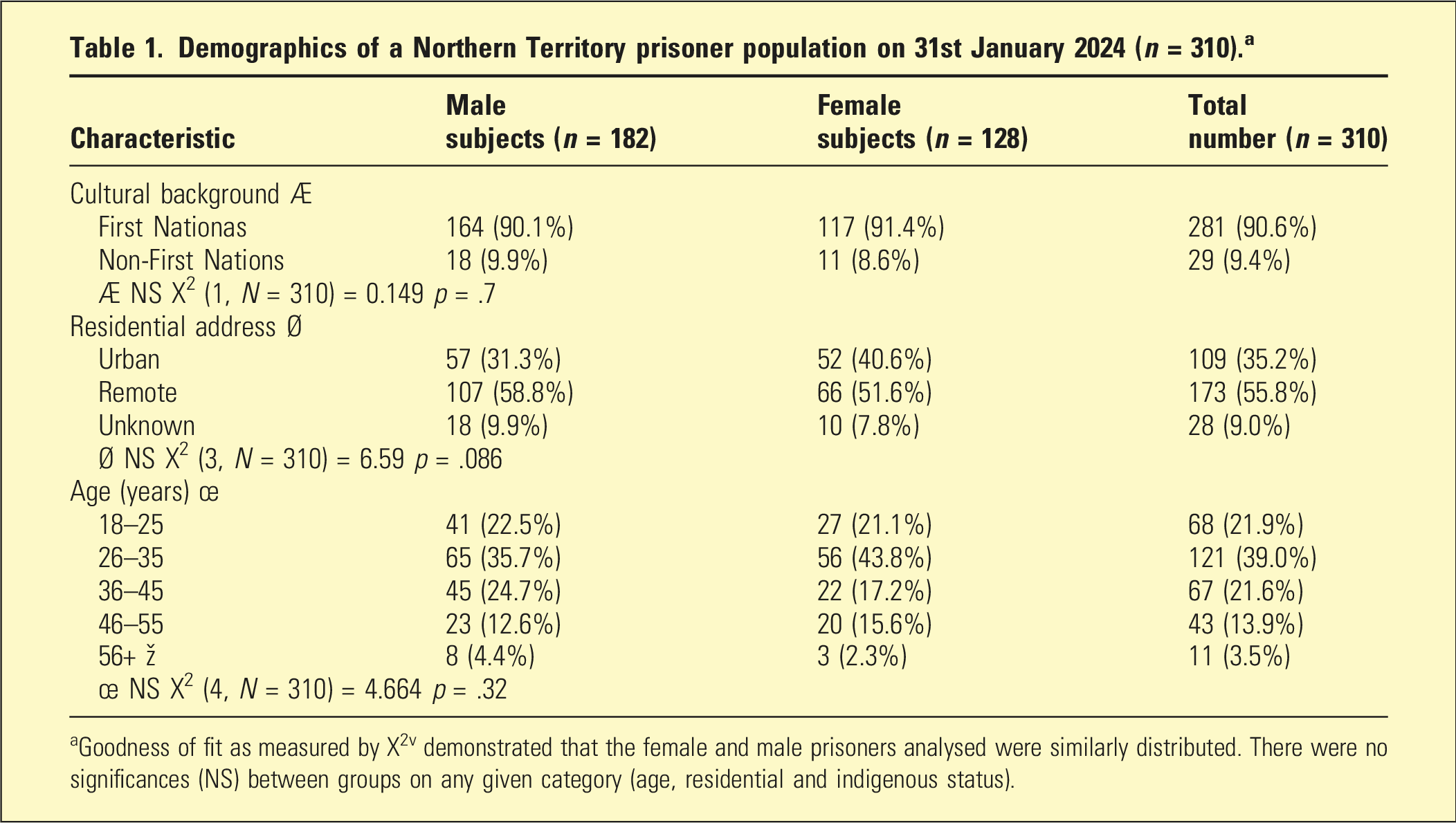
aGoodness of fit as measured by X2v demonstrated that the female and male prisoners analysed were similarly distributed. There were no significances (NS) between groups on any given category (age, residential and indigenous status).
The median age of both males and females was 32. Mean (SD) for ages was 34.1 (9.86) year for females and 34.6 (10.9) years for males. There was no statistically significance difference in median ages between genders (median age male and females 32 years, respectively, U = 1160, p = .096). However, First Nations prisoners were statistically younger than the non-First Nations prisoners (median age of First Nations 32 years vs Non-First Nations 40 years, U = 2747, p = .004). Mean (SD) ages were similarly younger for First Nations prisoners (33.8 (10.2) versus 40.0 (11.3) years). Most prisoners included were First Nations (90.6%), most of whom (55.8%) came from a remote community.
Prevalence of mental illness, prescription of psychotropic medications and previous inpatient admissions.
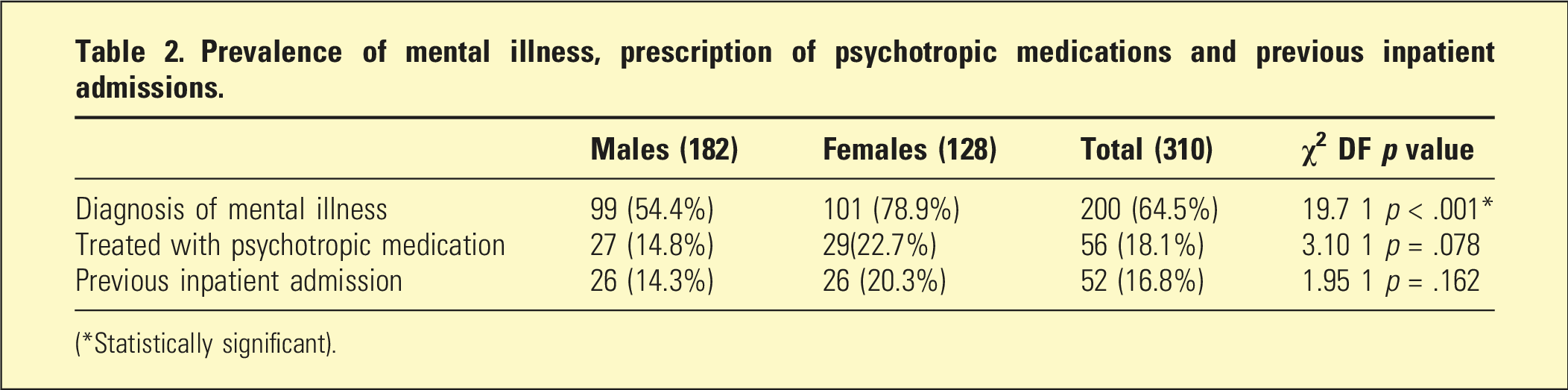
(*Statistically significant).
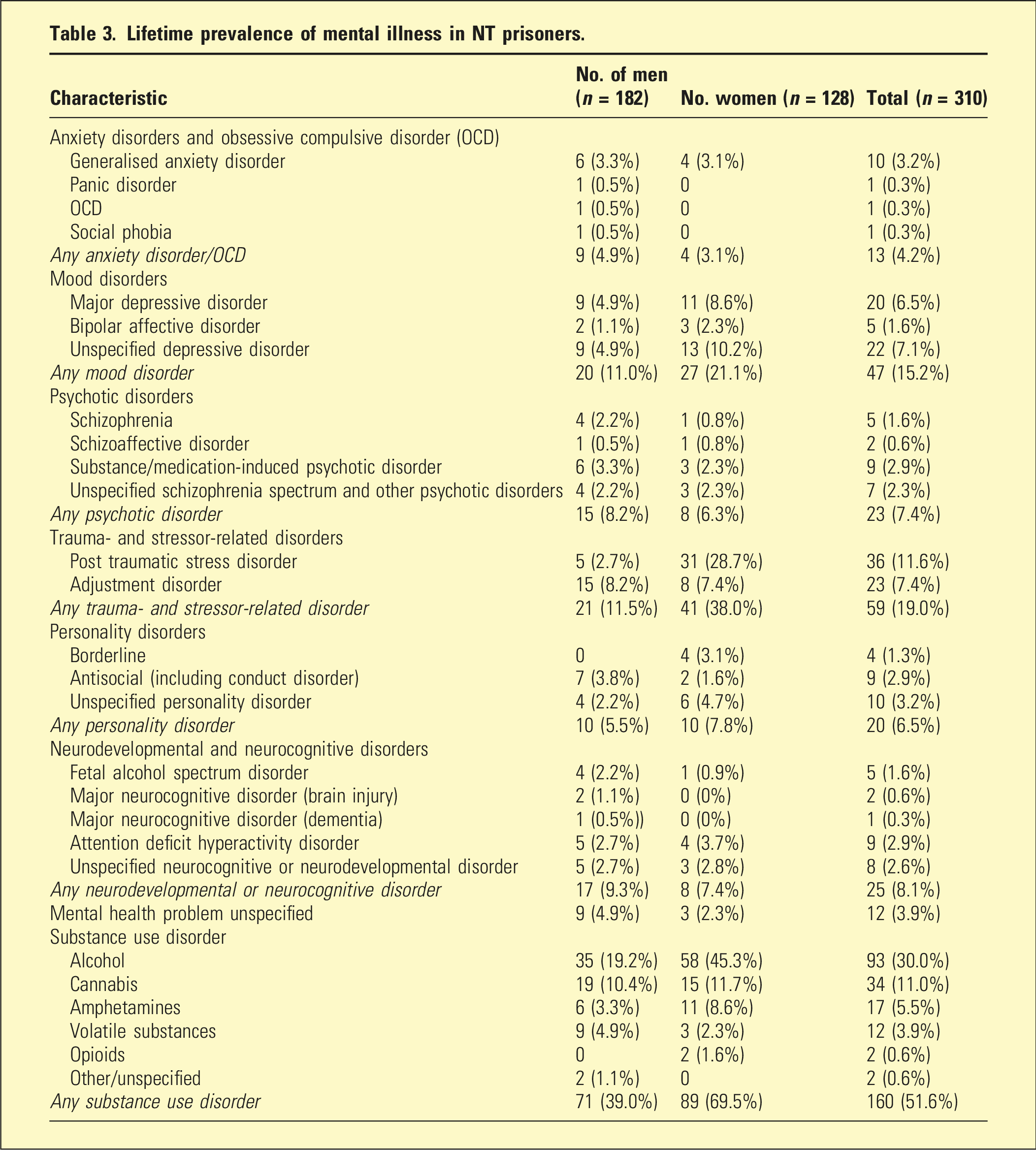
Lifetime prevalence of mental illness in NT prisoners.
Discussion
Among the 310 prisoner files reviewed, rates of mental illness were higher than the general population. Most men (54.4%) and a majority (78.9%) of women had been diagnosed with a mental illness (X2 (1, N = 310) = 19.7, p < .001). The results reflect previous data, with higher rates of mental illness in women compared to men in both the general population and prison well recognised globally and in Australia. The majority of this burden of disease was attributable to substance use disorders, however, a wide range of psychiatric conditions were identified including anxiety, mood, psychotic, and personality disorders, along with neurodevelopmental and neurodegenerative conditions.
Healthcare services for prisoners must be mindful of the diversity of mental disorder seen in this population, and be resourced to deal with the variety of diagnostic presentation. This data would suggest that there should be a prioritisation of alcohol and other drug (AOD) service provision for prisoners, particularly women. However, AOD services alone will not meet the complex needs of prisoners and must be complemented by primary healthcare, psychology, and specialist psychiatric services. There is also a need to ensure disability services are provided. In the setting of decreased AOD and disability service provision in the NT, these findings are very concerning.
The very high proportion of First Nations prisoners in this sample indicates that healthcare services provided to prisoners must be culturally appropriate, designed in consultation with First Nations people, and delivered by First Nations people to be effective.
The finding that First Nations prisoners were younger than the non-First Nations prisoners (median age of First Nations 32 years vs Non-First Nations 40, U = 2747, p = .004) emphasises this recommendation. It is suggestive that First Nations people in the NT have fundamental differences in their trajectories to imprisonment, with First Nations people in the NT imprisoned earlier and in much greater numbers. It is suspected that these differences are a result of the significant medical, social, economic, and historical disadvantages between these groups, however further research into this topic is required.
Around 15% of male prisoners and one-fifth of female prisoners have previously had a psychiatric admission however there were no statistically significant differences between genders. The authors consider this an interesting finding despite its lack of statistical significance as it reflects the similarities between prisoners with a mental illness and psychiatric inpatients. This is relevant when considering that in some Australian jurisdictions prisoners are admitted to general psychiatric wards, whereas in other jurisdictions this is considered impossible or even unacceptable due the supposed differences between these population subgroups.
Strengths and limitations
The study aimed to provide a preliminary landscape of mental illness in the NT prison population. The strength of this study lies in the researchers’ access to multiple databases containing health information from settings including prison, hospital, and the community. It is likely that almost all mental illness was captured from one of these datasets, enabling an estimation of lifetime prevalence to be provided.
By using medical records, the data relies on practitioners entering correct, relevant and current data into prisoner files. Diagnoses are updated by all practitioners including psychiatrists, but also non-psychiatric medical practitioners, mental health nurses, and primary healthcare clinicians. In the opinion of the authors, this study identified a surprisingly low prevalence of some conditions, as compared with their apparent prevalence in clinical practice in NT prisons. Two such examples are PTSD (particularly in men) and neurodevelopmental disorders including but not limited to fetal alcohol spectrum disorder. Due to the reliance on existing diagnoses rather than undertaking diagnostic interviews, it is probable that whilst this study was able to capture the prevalence of mental illness in general, the accuracy of individual diagnostic prevalence was limited. Future studies should use self-report questionnaires and structured interviews to assess the prevalence of identified conditions.
Conclusions
This study contributes to the literature by providing an overview of the prevalence of mental illness (including substance use disorder) in an NT prison population. Prisoners in the NT experience a higher burden of mental illness as compared with the general population, and women experience a significantly higher burden than men. Healthcare services provided to prisoners must incorporate specialist AOD, psychiatric, and psychological care in addition to primary healthcare, and be culturally appropriate due to the overwhelming majority of First Nations prisoners.
Footnotes
Acknowledgements
The authors thank A/Prof. Mrigendra Das for his support and expertise.
Ethical considerations
The study design was approved by the Human Research Ethics Committee of NT Health and Menzies School of Health Research, approval number NT HREC 2024-4796.
Consent to participate
The requirement for informed consent of participants was waived by the Human Research Ethics Committee of NT Health and Menzies School of Health Research.
Author contributions
SD conceived the study, SD, WK and DM collaborated on methodology. SD and WK collaborated on submission for ethics approval. SD did initial literature search, WK did remaining background research. WK collected the data and it was analysed by WK and DM. WK wrote the initial draft and created tables and figures, SD and DM reviewed and edited.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.