
Abstract
Introduction:
Asian Americans are at heightened risk for type 2 diabetes, yet research on cultural and intergenerational dynamics remains limited.
Methods:
Guided by Family Systems Theory and Leininger’s Transcultural Nursing Theory, this cross-sectional study examined diabetes knowledge and family support in 102 Chinese and Filipino American dyads (parent with diabetes + adult child) in Northern California.
Results:
Using the Diabetes Knowledge Questionnaire and the Family Supporters National Survey Tool, we found that Filipino parents scored higher in diabetes knowledge than Chinese parents. T-tests revealed significant differences in knowledge scores between Chinese and Filipino parents, t(102) = −2.91, p < .004, d = .45. Four significant predictors emerged: dyadic roles, age, English proficiency, and health status, F(9, 94) = 4.66, p < .001, R2 = .31. A two-way analysis of variance (ANOVA) showed a positive correlation between diabetes knowledge and family support among Filipino children but an inverse trend among Chinese children, F(1, 97) = 4.22, p = .043.
Discussion:
Findings suggest the importance of culturally tailored, family-centered diabetes interventions for Asian American communities.
Introduction
Type 2 diabetes (T2D) affects over 37 million U.S. adults and remains a leading cause of mortality and chronic health complications, including cardiovascular disease, kidney failure, and dementia (Centers for Disease Control and Prevention [CDC], 2022; Xu et al., 2022). While often associated with obesity, T2D is prevalent among Asian Americans even at normal BMI levels (≤25), with many remaining undiagnosed (CDC, 2022; Joslin Diabetes Center & Joslin Clinic, 2016). In response, the CDC lowered the BMI threshold for screening to ≥23 for this population (CDC, 2019). Despite these trends, Asian Americans are frequently underrepresented in diabetes research, due in part to sociocultural and linguistic barriers (Doan et al., 2023; Peregrina et al., 2022).
This study focuses on two distinct subgroups, Chinese Americans (East Asian) and Filipino Americans (Southeast Asian), who exhibit different diabetes risk profiles. For example, the prevalence of diagnosed T2D among Filipinos has reached 13%, compared with 5.6% among Chinese Americans (Raquinio et al., 2021). Yet, beyond prevalence data, little is known about how intergenerational dynamics and culturally specific values influence diabetes knowledge and caregiving practices within these families. While it is widely acknowledged that family support plays a critical role in diabetes self-management, previous studies have varied in how “family” is defined, ranging from spouses and household members to broader social networks (Busebaia et al., 2023). In contrast, our study focuses on a clearly intergenerational dyad: an older parent with diabetes and their adult child. This focus allows us to explore how culturally rooted expectations, such as filial piety and tiwala, shape knowledge, support, and caregiving roles within a specific relational context.
In Chinese American families, filial piety emphasizes duty and deference to parents, often translating into caregiving responsibilities for adult children. In contrast, Filipino culture is shaped by tiwala, a multifaceted concept meaning trust, reliance, belief, and confidence in others and oneself. Tiwala not only facilitates open communication but also reinforces interdependence within Filipino families, encouraging collaborative caregiving and emotional support (Turalba-Khalil, 2024). Understanding how these values shape caregiving behaviors is essential to delivering culturally congruent care.
To guide our analysis, we applied Family Systems Theory (Bowen, 1993), which conceptualizes the family as an interconnected unit in which each member influences the others. This perspective helps explain intergenerational dynamics. In addition, Leininger’s Culture Care Diversity and Universality Theory (Leininger, 1991) further frames how culturally embedded beliefs such as filial piety and tiwala affect caregiving roles, communication, and family decision-making.
We also considered how diabetes knowledge is typically measured. Validated tools include the 24-item Diabetes Knowledge Questionnaire (DKQ), which assesses general knowledge; the 23-item Michigan Diabetes Knowledge Test (DKT), which includes insulin-related items; and the DISTANCE survey module. Of these, the DKQ is widely used and validated across diverse populations, making it particularly appropriate for cross-cultural studies (Garcia et al., 2001; Nguyen et al., 2022; Zakiudin et al., 2022).
This study aims to (a) describe diabetes knowledge among Chinese and Filipino Americans; (b) explore factors associated with diabetes knowledge between the groups; and (c) examine relationships between adult children’s diabetes knowledge, family support, and ethnicity.
Method
Study Design
This study presents quantitative findings on diabetes knowledge and family support from the CARE-T2D study (Caring for Asian Americans through Research and Education about Type 2 Diabetes). The original mixed-methods study combined quantitative surveys with individual and dyadic interviews to explore family support dynamics among Chinese and Filipino Americans in Northern California. Each dyad consisted of an older parent with type 2 diabetes and an adult child (aged 18 and over) without diabetes. The dyadic design allowed for a dual perspective on family dynamics, essential for understanding intergenerational support systems (Li & Tong, 2023; Pamungkas et al., 2017).
Measurement Instruments
The CARE-T2D quantitative survey, developed by three researchers, incorporated two validated instruments:
Diabetes Knowledge Questionnaire (DKQ)
Originally developed for research in Starr County, Texas, the DKQ is a 24-item scale assessing general diabetes knowledge (Garcia et al., 2001). Items are scored dichotomously (1 = Yes, and 0 = No/Don’t Know), with total scores ranging from 0 to 24. Higher scores reflect greater diabetes knowledge (Dawson et al., 2017). The DKQ has been widely used in diabetes studies (Hanis et al., 1983) and validated across diverse populations with strong internal consistency in Indonesian, Cronbach’s α = .757 (Zakiudin et al., 2022); Malaysian, α =.806 (Ahmad et al., 2010); and Urdu, α =.702 (Bukhsh et al., 2017).
Family Supporters National Survey Tool (FSNST)
The FSNST assesses family support dynamics between older adults with T2D and their adult children (Lee et al., 2017). It includes 17 items across three sections:
Mention (six items)—frequency of parents discussing health concerns with adult children.
Happen (six items)—adult children’s experiences with parental health issues.
Communication (five items)—adult children’s involvement in health care provider communication.
Items are rated on a 5-point Likert-type scale (1 = Never to 5 = Every Time).
Data Collection
Data collection took place from September 2018 to April 2019 following approval by San Francisco State University Institutional Review Board (IBR No. X17-73). Informed consent was obtained from all participants prior to their enrollment in the study. Recruitment occurred in community-based settings throughout the San Francisco Bay Area, targeting self-identified Chinese and Filipino American adults. Detailed recruitment protocols and community engagement strategies for Chinese Americans (Doan et al., 2023) and Filipino Americans (Peregrina et al., 2022) have been published elsewhere. Participants completed structured surveys assessing diabetes knowledge and family support, either in person or online. Surveys were administered in English and Chinese as appropriate, and participants were informed of this availability during recruitment. The Chinese-language version of the survey was translated using the World Health Organization protocols for translating research instruments (World Health Organization, 1998), as detailed in Doan et al. (2023). To further address language needs, bilingual/bicultural research staff fluent in Cantonese, Mandarin, and Tagalog were present during in-person sessions and available remotely by phone to assist participants. Participants’ self-rated English proficiency was also documented and included as a predictor in our statistical analyses. Follow-up support was offered as needed.
Data Analysis
Descriptive statistics were used to summarize demographics and DKQ scores. Independent samples t-tests compared mean DKQ scores between Chinese and Filipino subgroups, and FSNST mean scores between Chinese and Filipino adult children. Multiple linear regression identified predictors of diabetes knowledge across all participants. A two-way analysis of variance (ANOVA) was used to test the interaction between ethnicity and DKQ scores on FSNST scores. Levene’s test was conducted for homogeneity of variances, which was nonsignificant (p = .21), confirming that the ANOVA assumption of equal variances met. Analyses were conducted using SPSS Version 30.
Results
Participant Characteristics
Table 1 presents participant demographics. Filipino parents had significantly higher educational attainment, with 70% holding a bachelor’s degree or higher, compared with 46% of Chinese parents with less than a high school education. Employment patterns were similar across groups, with most parents retired (Chinese: 57%, Filipino: 52%) and most adult children employed full-time (Chinese: 89%, Filipino: 84%). Approximately 25% of the Chinese participants (n = 25) and 15% of the Filipino participants (n = 13) declined to report their income. All subgroups had average BMIs above the threshold for Asian-defined overweight status (BMI ≥ 23). Both Filipino and Chinese parents had mean American Diabetes Association (ADA) risk scores ≥5, indicating elevated T2D risk. Roughly three-quarters of parents had hypertension (HTN), and approximately 10% of adult children reported the same.
Participant Demographics.
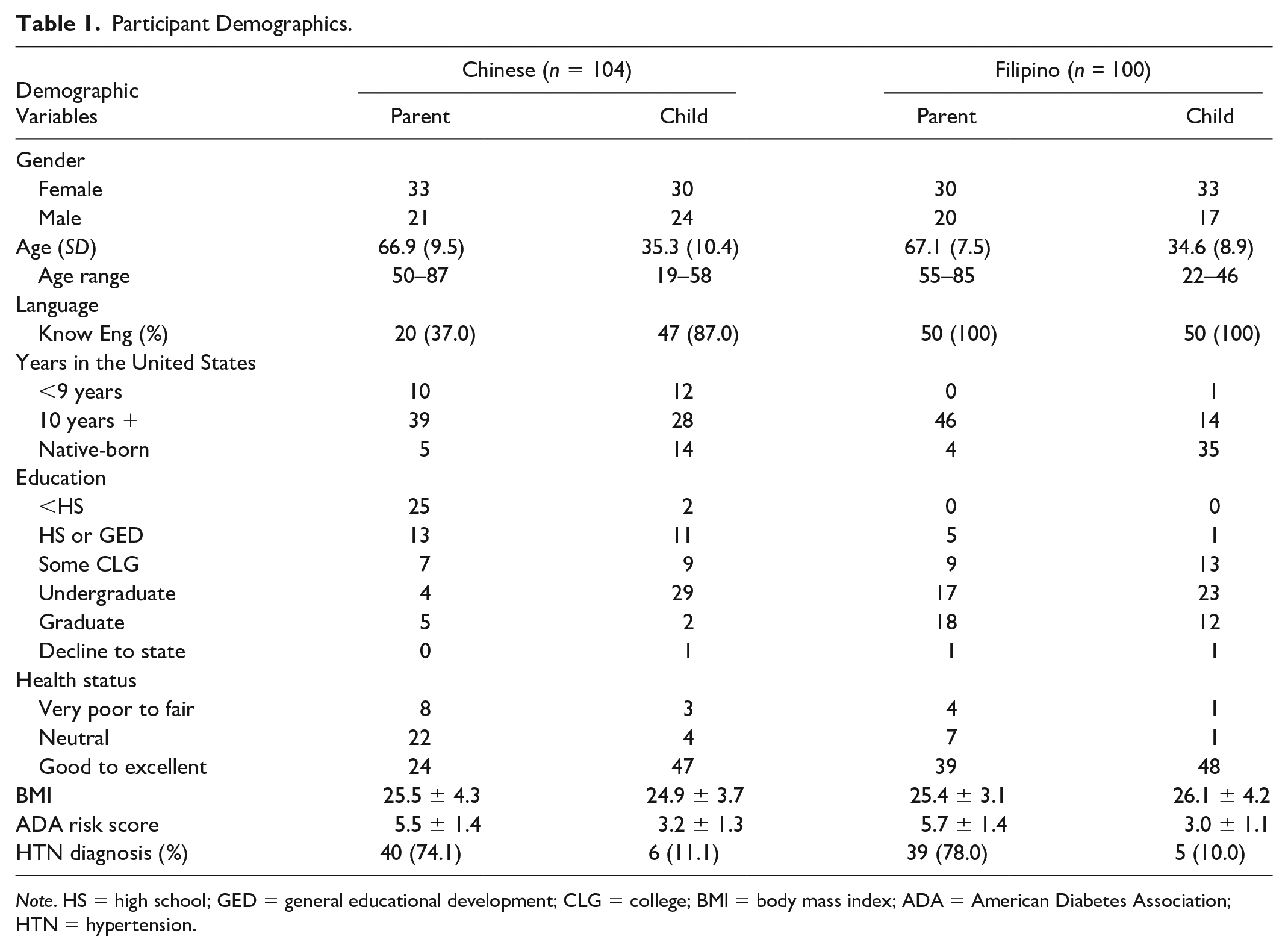
Note. HS = high school; GED = general educational development; CLG = college; BMI = body mass index; ADA = American Diabetes Association; HTN = hypertension.
Diabetes Knowledge Scores
Filipino parents’ DKQ scores averaged 2.05 points higher than those of Chinese parents. The independent sample t-tests revealed significant differences between Chinese and Filipino parents, t(102) = −2.91, p < .004, 95% CI [−3.45, −0.65], with a small standardized effect size of −0.23. This suggests that although the difference is probably not due to chance, the practical difference in DKQ scores between Filipino and Chinese parents is relatively small. Although Chinese adult children scored 0.53 points higher than Filipino adult children, this difference was not statistically significant.
Predictors of Diabetes Knowledge
Multiple linear regression analysis identified four significant predictors of DKQ scores across all participants (N = 208): participant role (parent vs. child), age, English proficiency, and self-rated health status, F(10, 197) = 3.22, p < .001, R2 = .14. Subgroup analyses showed that age and health status were significant predictors for parents, while no predictors were found for Chinese or Filipino adult children, F (9, 93) = 0.97, p < .468, R2 = .09. Table 2 summarizes regression coefficients by group.
Predictors of DKQ Scores by Group: Results From Multiple Linear Regression Analyses.
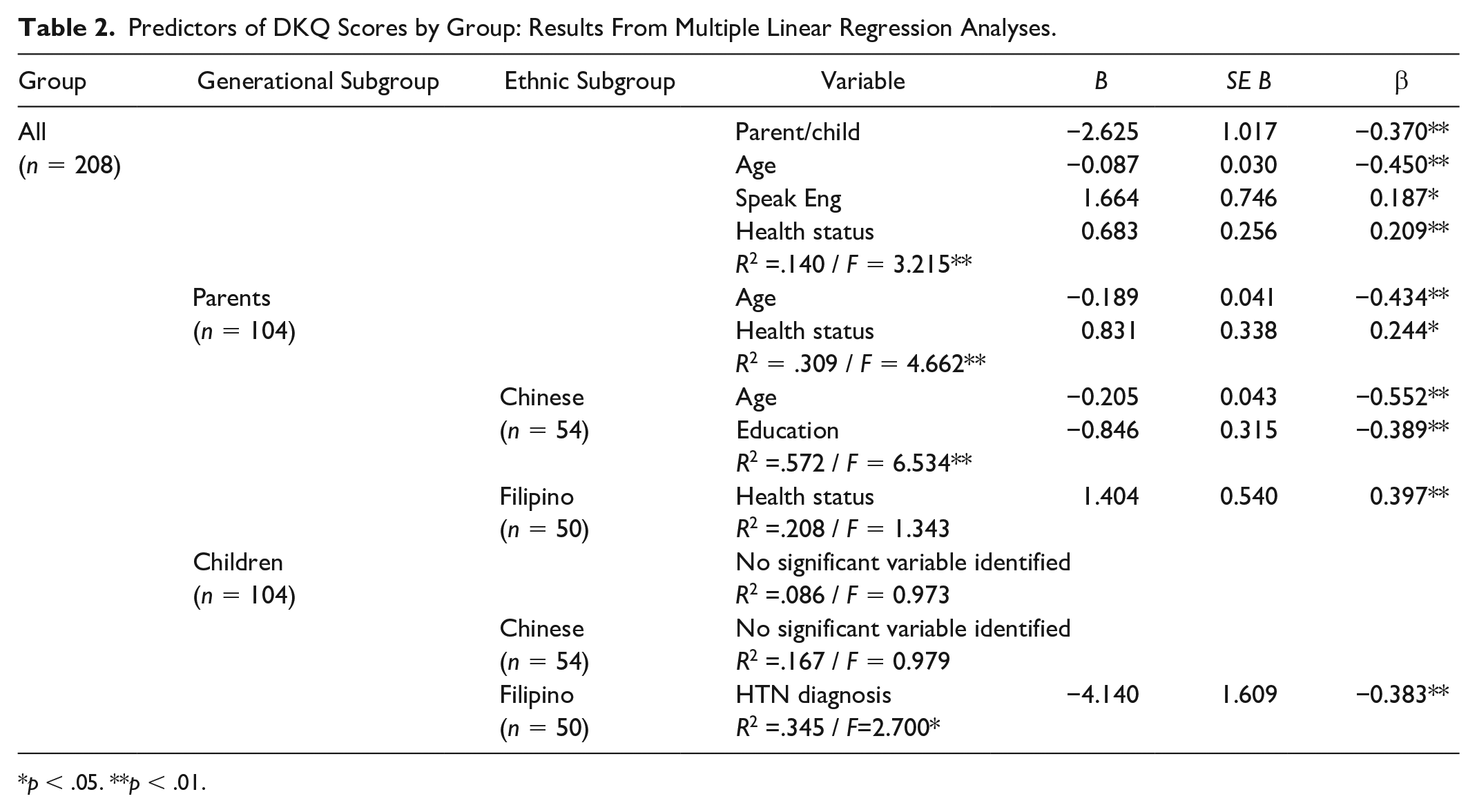
p < .05. **p < .01.
Item-Level Knowledge Gaps
Table 3 lists DKQ items with the lowest accuracy rates across all subgroups. Overall, accuracy was lowest among Chinese parents (23.6%) and highest among Filipino parents (32.2%). Common gaps included awareness of hereditary diabetes risk, knowledge about toenail care, and symptoms like poor circulation and slow healing.
DKQ Questions With Low Accuracy Rates (%).
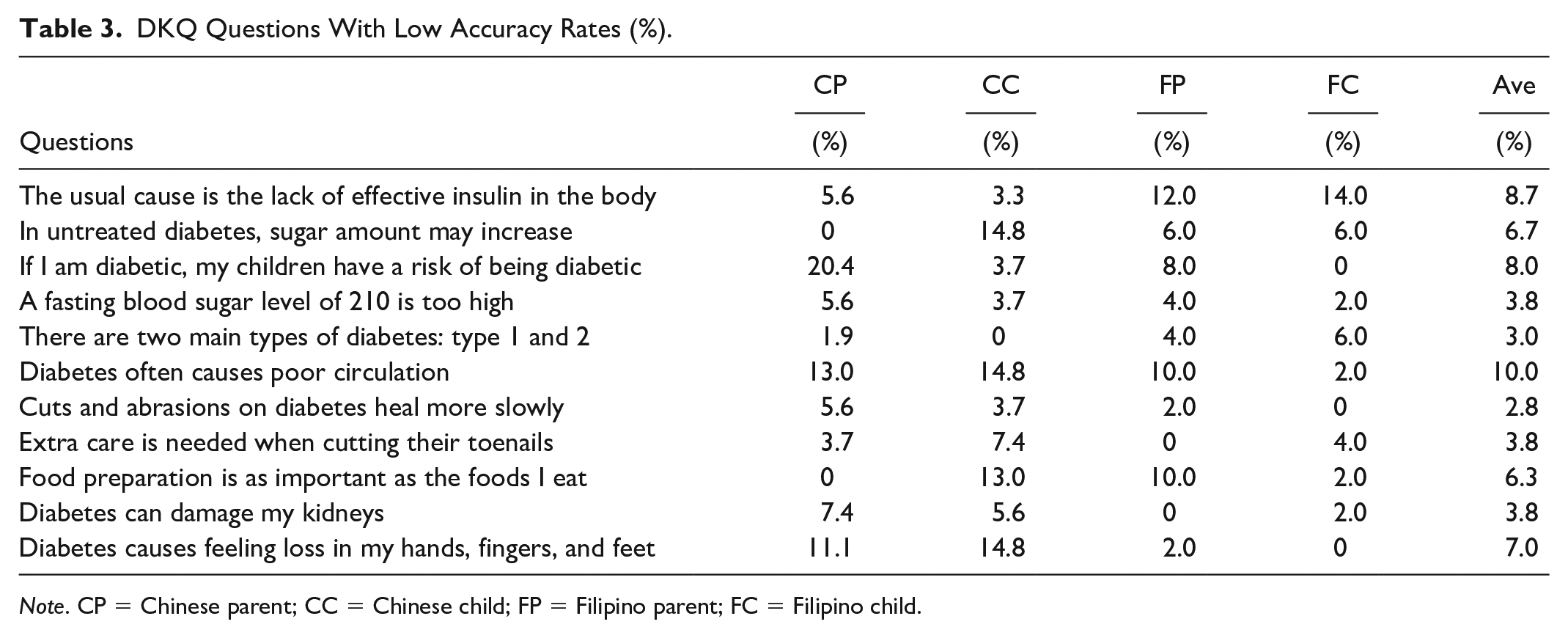
Note. CP = Chinese parent; CC = Chinese child; FP = Filipino parent; FC = Filipino child.
Family Support Differences
Independent t-tests using FSNST scores revealed three key differences between Chinese and Filipino adult children (Table 4):
Chinese adult children reported more frequent parental concerns about medication side effects (p < .001).
Filipino adult children reported feeling more overwhelmed by their parents’ health issues (p < .02).
Chinese adult children reported greater involvement in health care decision-making (p < .05).
Independent Sample t-Test for FSNST Score (p < .05) Between Filipino and Chinese Adult Children.
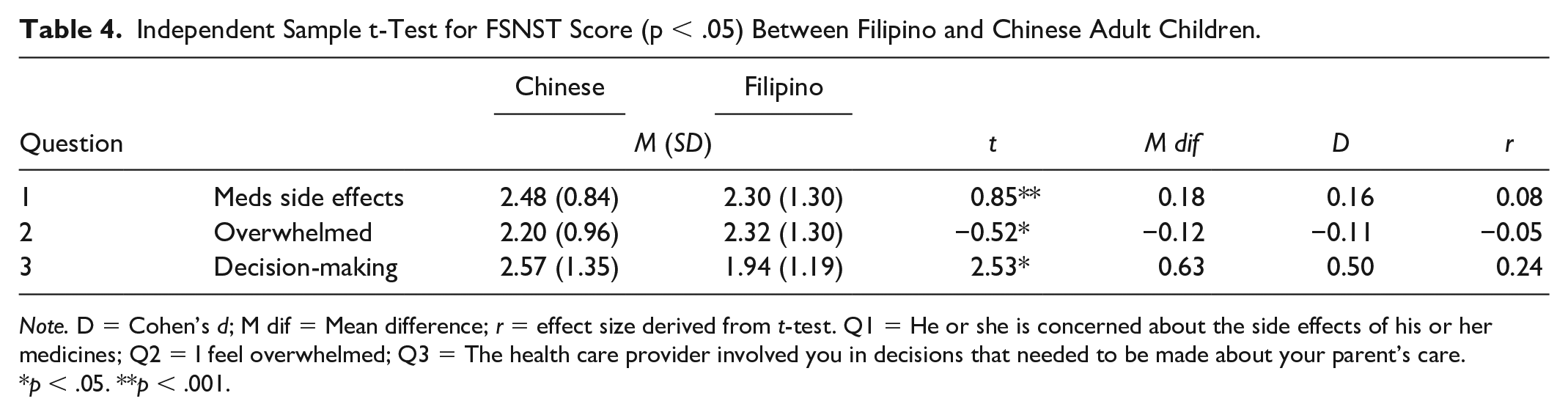
Note. D = Cohen’s d; M dif = Mean difference; r = effect size derived from t-test. Q1 = He or she is concerned about the side effects of his or her medicines; Q2 = I feel overwhelmed; Q3 = The health care provider involved you in decisions that needed to be made about your parent’s care.
p < .05. **p < .001.
Interaction Between Knowledge and Support
A two-way ANOVA revealed a statistically significant interaction between DKQ scores and ethnicity on FSNST scores, F(1, 97) = 4.22, p = .04. Simple main effects indicated that ethnicity influenced support scores. Among Filipino adult children, DKQ and FSNST scores were positively correlated, while Chinese adult children showed an inverse relationship (Figure 1).
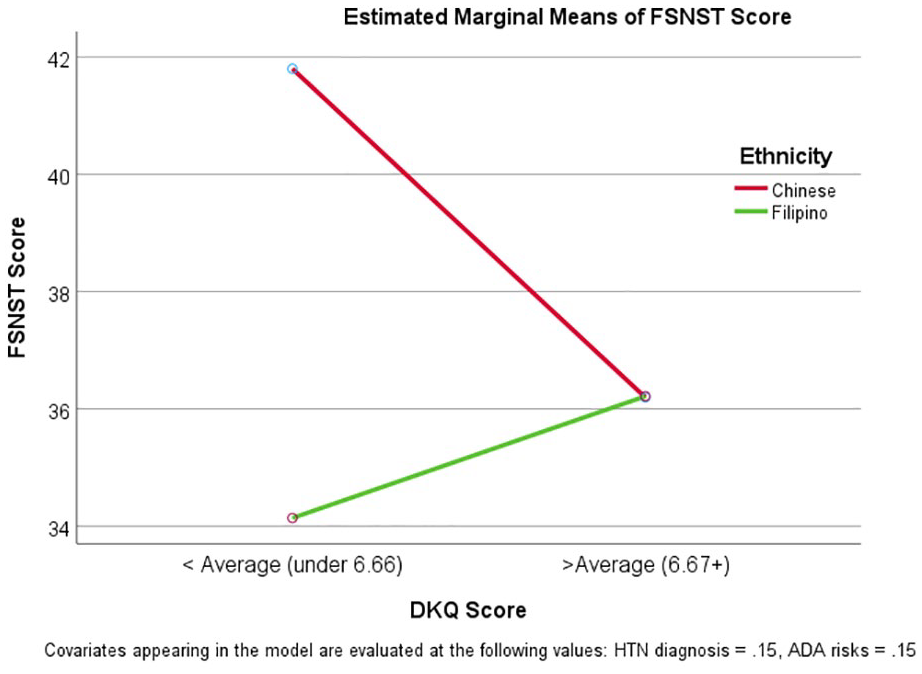
Means Plot of FSNST Score by DKQ and Ethnicity.
Discussion
This study examined diabetes knowledge and family support among Chinese and Filipino Americans, focusing on adult children’s roles and ethnic subgroup differences. Our findings have important implications for culturally tailored diabetes education and underscore the significance of family support in disease management. Overall, participants demonstrated lower diabetes knowledge compared with previous studies (Bukhsh et al., 2017; Garcia et al., 2001; Hu et al., 2013). Consistent with prior literature, our results confirm that family support in Asian American communities is shaped by deeply rooted cultural values, with subtle distinctions between subgroups (Choi et al., 2018; Yao, 2020). Older parents had lower diabetes knowledge scores than their adult children, aligning with research showing that knowledge declines with age (Rupel et al., 2021).
These findings can be interpreted through the lens of Family Systems Theory, which emphasizes the interconnectedness of family members and how individual behaviors, such as health knowledge or stress, ripple across the family unit. For example, the inverse relationship observed between diabetes knowledge and family support among Chinese adult children may reflect a redistribution of roles based on cultural caregiving expectations, as outlined by the theory. Similarly, Leininger’s Culture Care Diversity (Leininger, 1991) and Universality Theory support interpreting culturally specific caregiving roles, communication norms, and beliefs about medical interventions. This framework underscores the need for culturally congruent care that aligns with values such as filial piety and tiwala, both of which influence the degree and type of support family members provide.
Education level is a commonly cited predictor of diabetes knowledge (Bukhsh et al., 2019; Kassahun et al., 2016). In our sample, Chinese parents had lower DKQ scores, likely influenced by limited English proficiency and lower educational attainment. These barriers may hinder access to up-to-date, culturally appropriate diabetes education (Li-Geng et al., 2020). Since patients with lower health literacy often struggle with disease management, materials should be written at a fifth-grade reading level and include visuals (Hersh et al., 2015). Education was a significant predictor only among Chinese parents, possibly because Filipino parents already had uniformly high educational levels. Although most Filipino parents rated their health positively and had high educational attainment, their DKQ scores did not exceed expectations, possibly due to overconfidence or unaddressed gaps in practical knowledge. Duration of diabetes may also influence knowledge levels; those with longer illness experience tend to benefit from repeated exposure to diabetes education (Beck et al., 2015).
Adult Children’s Diabetes Knowledge and Family Support
Among Filipino adult children, our findings suggest that higher diabetes knowledge (as reflected in DKQ scores) is positively associated with greater family support involvement. This pattern may be explained through the cultural lens of tiwala, a deeply rooted Filipino value that embodies trust, reliance, belief, and confidence in others and in oneself. More than a transactional form of trust, tiwala reflects an unspoken mutual understanding, where support is given without the need for explicit proof, explanation, or verbal affirmation (Turalba-Khalil, 2024). In the context of caregiving, tiwala encourages adult children to assume supportive roles confidently, trusting their own health knowledge and their responsibility to care for elders. This aligns with our finding that Filipino adult children with higher diabetes knowledge felt more comfortable providing care. Tiwala thus serves as a cultural bridge, linking confidence in health knowledge to emotional readiness and kinship-driven caregiving, reinforcing the strength of intergenerational support systems in Filipino families.
Chinese adult children reported more concern about medication side effects, an observation likely influenced by cultural preferences for traditional or herbal remedies, which are often viewed as more natural and less harmful than Western pharmaceuticals (Fang, 2019; Lu & Lu, 2014). Despite exhibiting higher levels of family support, these participants did not score higher on the DKQ, revealing an inverse relationship between knowledge and support. This pattern may be explained by the cultural construct of filial piety (孝顺), a Confucian-rooted value system that emphasizes obedience, reverence, and care for one’s elders. In many Chinese families, caregiving is viewed as a moral obligation rather than a specialized skill. Filial piety does not necessarily require technical health knowledge. Rather, it demands presence, loyalty, and deference to parental needs, often enacted through action rather than questioning. In this context, high levels of support may reflect duty-bound behavior rather than informed health advocacy. Language barriers and limited access to culturally adapted materials likely further constrain diabetes-specific knowledge, highlighting a gap that culturally concordant interventions must address.
Cultural Challenges in Dietary Management
Standard diabetes dietary recommendations often conflict with cultural food practices. Chinese participants struggled with modifying staple foods like rice, which symbolize prosperity and social cohesion (Marton, 2014; Sunarti et al., 2022). In Chinese culture, preparing and sharing food is a demonstration of care and unity (Wang et al., 2020). Adhering to a diabetic diet, which entails not maintaining traditional eating habits with family, can disrupt these practices and hinder their understanding of nutrition (Li-Geng et al., 2020). Likewise, Filipino culture is rooted in the belief that sharing reflects caring, highlighting love, generosity, and hospitality through food offerings among family and friends. This tradition fosters and enhances connections, creating a sense of community, as meals are often shared in a family-style setting (Busebaia et al., 2023; Lopez-Thismon, 2019). Nevertheless, traditional Filipino cuisine tends to be high in fat and sugar, with sugary drinks being popular. It is essential to address these factors when managing the dietary needs of diabetic patients (Maglalang et al., 2017); having family support, along with a clear understanding of type 2 diabetes, can be extremely beneficial.
Implications for Future Transcultural Nursing
Our findings support the need for culturally tailored diabetes education that integrates family roles and cultural beliefs. For Asian Americans, diabetes education should go beyond focusing solely on individual behavior to include shared decision-making and collective health norms.
Limitations
This study has a few limitations. First, approximately 20% of participants declined to report their income, limiting our ability to assess socioeconomic factors as predictors of diabetes knowledge. In addition, we did not collect information on participants’ health insurance status, which could be a significant factor in understanding health care access and diabetes outcomes. Prior research suggests that a lack of insurance may be associated with the earlier onset of diabetes, particularly among individuals with obesity. Finally, the study’s subgroup analyses were based on relatively small samples (n = 50 per group), which may reduce the generalizability of the findings. Future research should incorporate more robust sampling and include variables such as income, occupation, and insurance coverage to better understand the structural determinants of diabetes knowledge and support.
Conclusion
This dyadic study offers culturally grounded insights into how diabetes knowledge and family support differ between Chinese and Filipino American families. Our findings highlight the distinct ways in which cultural values, such as filial piety in Chinese and tiwala in Filipino families, shape caregiving behaviors, emotional burden, and the relationship between knowledge and support. While tiwala fosters caregiving confidence and comfort in Filipino adult children, filial piety may promote caregiving as a moral duty, even in the absence of detailed health knowledge. These culturally embedded frameworks underscore the need to move beyond individualistic models of diabetes education.
For transcultural nurses and educators, these findings emphasize the importance of assessing family involvement, cultural norms, language proficiency, and acculturation levels when designing diabetes interventions. Culturally tailored education, delivered by ethnically concordant staff and supported by linguistically appropriate materials, can bridge knowledge gaps and empower family members, particularly adult children who serve as critical caregivers. Practical implications include integrating family-centered and culturally responsive strategies into diabetes self-management education, with particular attention to high-risk Asian American subgroups such as women aged 45 and over with prediabetes.
Footnotes
Acknowledgements
We extend our sincere gratitude to all participants for their time and invaluable contribution to advancing our understanding of type 2 diabetes management in Chinese and Filipino American families. We acknowledge the exceptional efforts of our CARE-T2D research team members—Carissa Villanueva, Liz Lu, RN, and Katrina Yuen, RN—whose dedication was instrumental in our successful recruitment process. Our deepest appreciation goes to Diana Lau, RN, PhD, for her extensive outreach to the Chinese community; Vilma Mila, RN, for her expert service as Tagalog/Ilocano interpreter; and Yu-Ruo Wang, RN, for her meticulous expertise in the translation and validation of Chinese study materials.
Author Contributions
TD: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing-original draft, Writing-review & editing. SB: Conceptualization, Data curation, Formal analysis, Methodology, Software, Validation, Visualization, Writing-original draft, Writing-review & editing. HP: Data curation, Investigation, Software. MLB: Conceptualization, Investigation, Supervision, Visualization, Writing-review & editing. MSB: Conceptualization, Data curation, Investigation, Methodology, Visualization, Writing-review & editing. GY: Conceptualization, Data curation, Funding acquisition, Investigation, Resources, Software, Supervision, Visualization, Writing-review & editing.
Data Availability
Due to the nature of this research, participants of this study did not agree for their data to be shared publicly, so supporting data is not available.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research received funding from San Francisco Building Infrastructure Leading to Diversity (SF-BUILD), NIH Grant Number UL1GM118985.
Ethical Considerations
This study received institutional review board approval from San Francisco State University, CA, USA (November 2017/No. X17-73).
Consent to Participants
Written informed consent was obtained from all participants in this study. Consent forms were provided either through our secure online survey platform or on paper, based on each participant’s preference. Participants were fully informed about the study’s purpose, procedures, potential risks and benefits, and their right to withdraw at any time without consequences. All participant information was treated with strict confidentiality, with data stored securely in password-protected files accessible only to authorized research team members. To protect participants’ privacy, all identifiable information was removed during data analysis and reporting, ensuring complete anonymity.