
Abstract
Introduction:
Artificial intelligence (AI) is increasingly influencing nursing and surgical care. Although AI-supported systems may improve efficiency, they also raise ethical and humanistic concerns, highlighting the importance of patient perspectives.
Methods:
An explanatory sequential mixed methods design was used. Quantitative data were collected from 312 postoperative surgical patients to assess knowledge and attitudes toward AI-supported care. Based on these results, 15 participants were selected for in-depth qualitative interviews using purposive sampling. Descriptive qualitative content analysis was applied, and the findings were integrated.
Results:
Patients’ attitudes toward AI were generally moderate and cautious. Most participants reported limited knowledge and perceived AI as a media-driven and abstract concept. Major concerns included loss of human touch, system errors, data security, and trust. AI was viewed as a supportive tool rather than a replacement for nursing care.
Discussion:
Acceptance of AI-supported nursing care is shaped by cultural values, trust, human-centered expectations, requiring empathy and professional oversight.
Keywords
Introduction
The increasing digitalization of health care services and the widespread adoption of artificial intelligence (AI)-based applications are transforming the planning, delivery, and evaluation of care processes (Bajwa et al., 2021). Clinical decision support systems, imaging analysis technologies, patient monitoring tools, and automated data evaluation systems support clinical decision-making, reduce workload, and improve care quality (Ferreira et al., 2025). The literature also emphasizes their potential benefits for patient safety and care outcomes (Dailah et al., 2024; Guo et al., 2025; Huter et al., 2020). Nursing practice, particularly surgical care, is directly affected by these developments. Nurses play a central role in patient safety, early complication detection, and individualized care throughout the surgical process (Guo et al., 2025; Huter et al., 2020). In this context, AI-supported systems may facilitate patient monitoring, clinical data analysis, and reduce nurses’ routine workload, thereby increasing time for direct patient care (Dailah et al., 2024; Guo et al., 2025).
From a transcultural nursing perspective, technological innovations are integrated into care within cultural, social, and ethical contexts that shape patients’ health beliefs, values, and expectations. Therefore, AI integration should not be considered only in terms of technical adequacy and clinical effectiveness. Ethical issues, patient privacy, data security, human control in decision-making, and the effects of AI on the humanistic aspects of care are increasingly debated (Dailah et al., 2024). Patient–nurse interaction, trust, empathy, and individualized attention remain fundamental components of surgical care and may be interpreted differently across sociocultural contexts (Ahadian et al., 2025; Dailah et al., 2024). Thus, understanding how AI affects these human dimensions and how patients make sense of such technologies is critical for patient-centered care.
Existing studies on AI in health care have largely focused on technical infrastructure, clinical outcomes, or health care professionals’ perspectives (Ahadian et al., 2025; Dailah et al., 2024; Guo et al., 2025; Hajiheydari et al., 2025; Huter et al., 2020; Molina-Mula & Gallo-Estrada, 2020). Although patient-focused research is increasing, the evidence remains fragmented. Current studies mostly report moderate acceptance of AI, alongside concerns about privacy, data security, and depersonalization of care (Dailah et al., 2024; Huter et al., 2020). Patients generally perceive AI as a supportive tool rather than a replacement for health care professionals, especially where human interaction is essential (Ahadian et al., 2025; Molina-Mula & Gallo-Estrada, 2020). Trust in AI is also associated with system transparency, professional supervision, and prior exposure to digital health technologies (Guo et al., 2025; Hajiheydari et al., 2025).
However, most studies have been conducted in non-surgical or general health care settings and have relied mainly on quantitative approaches. Studies directly examining surgical patients’ perceptions, attitudes, expectations, and concerns regarding AI-supported nursing care remain limited. In addition, culturally embedded meanings, norms, and values influencing patients’ interpretations of AI-supported care have received little attention. This gap highlights the need for mixed methods studies that combine measurable attitudes with qualitative insights to understand surgical patients’ perspectives within their lived experiences and sociocultural contexts.
Therefore, patient perceptions of AI in surgical care should be examined through both measurable attitudes and individual experiences within cultural and social contexts. This study evaluates surgical patients’ knowledge and attitudes toward AI and complements these findings with qualitative data on their experiences and perspectives. Accordingly, the study aims to determine surgical patients’ knowledge and attitudes toward AI-supported nursing care; explore their perceptions within personal and cultural contexts; identify concerns, expectations, and values influencing acceptance; and examine how cultural beliefs, trust, and expectations of human-centered care shape their experiences. The results may support the development of patient-centered, ethical, safe, and culturally congruent AI-supported nursing practices.
Methods
Study Design
This study adopted an explanatory sequential mixed methods design. Quantitative data were collected and analyzed in the first phase to identify general patterns in patients’ knowledge of AI and attitudes toward AI-supported health care applications. These findings then informed purposive sampling for the qualitative phase, ensuring the inclusion of participants with diverse perspectives and experiences (Mayoh & Onwuegbuzie, 2015).
The study was reported in accordance with STROBE for the quantitative phase and COREQ for the qualitative phase. In-depth individual interviews were conducted with selected participants, and descriptive qualitative content analysis was used to explore patients’ subjective experiences and the meanings they attributed to AI-supported practices in surgical care. This approach enabled an interpretative understanding of patients’ lived experiences within their sociocultural and clinical contexts.
Integration of quantitative and qualitative findings provided a comprehensive interpretation of patients’ engagement with AI-supported nursing care, particularly in relation to trust, ethical considerations, and the humanistic dimension of care, consistent with the explanatory sequential mixed methods design.
Ethical approval was obtained from the Osmaniye Korkut Ata University Ethics Committee (Decision No: 2025/22; Date: -May 23, 2025). Written informed consent was obtained from all participants, and the study was conducted in accordance with the Declaration of Helsinki, with confidentiality and anonymity ensured.
Participants and Settings
This study was conducted between June and November 2025 in the surgical clinics of a public hospital in Osmaniye with adult postoperative patients. In the quantitative phase, participants were recruited from patients aged ≥18 years who had undergone elective surgery, had no communication barriers, and voluntarily agreed to participate. Patients with cognitive or psychiatric conditions affecting communication or participation were excluded.
In the qualitative phase, purposive sampling was applied based on quantitative findings. Participants were selected from those who completed the quantitative phase and represented varying levels of AI knowledge and attitudes, allowing exploration of diverse perspectives on AI-supported surgical care.
The quantitative sample size was determined by power analysis with a 95% confidence level, 5% margin of error, and Cohen’s d = .30, yielding a minimum of 300 participants; 312 patients were included to account for potential data loss (Cohen, 2013). In the qualitative phase, in-depth interviews were conducted with 15 participants, and data collection continued until saturation was achieved. Participants were selected to ensure sociodemographic diversity and variation in experiences with artificial intelligence.
Procedure
During the quantitative phase, eligible postoperative patients were informed about the study by clinic nurses, while clinical decision-makers were excluded to prevent conflicts of interest. After receiving detailed information, participants provided written informed consent and completed the questionnaires in approximately 10 to 15 min. Questionnaires were checked for completeness, and participants could review missing responses or leave items unanswered.
In the qualitative phase, participants who consented to further contact were purposively selected based on quantitative findings to ensure variation in AI knowledge and attitudes. Interviews were conducted by the researcher, while data collection and analysis continued concurrently until saturation was reached. The overall process followed a sequential structure: quantitative findings guided participant selection for the qualitative phase, and qualitative data were analyzed iteratively. Methodological rigor was supported by consistent data collection procedures, documentation of research steps, and adherence to mixed methods research guidelines.
Quantitative Phase
Quantitative Data Collection
Demographic Information Form
This form included items assessing participants’ age, sex, educational level, occupation, perceived income status, chronic illness, and surgical history. Additional multiple-choice questions evaluated participants’ knowledge of artificial intelligence, willingness to use AI-supported care, perceived areas of benefit, and views on the role of artificial intelligence in nursing care. Data from this form were used to describe participants’ characteristics and contextualize attitudes toward AI-supported nursing care.
General Attitude Toward Artificial Intelligence in Healthcare Scale
Participants’ attitudes toward artificial intelligence in health care were assessed using the scale developed by Schepman and Rodway (2020) and adapted to the health care context by Kaya and İşci (2025). The scale consists of 20 items rated on a 7-point Likert-type scale (0 = “I have no opinion” to 6 = “Strongly agree”) and includes two subscales: Positive Attitude (12 items) and Negative Attitude (8 items). Negative Attitude items were reverse-coded prior to analysis. Total scores range from 0 to 120, with higher scores indicating more positive attitudes toward AI. The original study reported a Cronbach’s alpha of .89, and internal consistency in the present study was .85.
Quantitative Data Analysis
Quantitative data were analyzed using SPSS Statistics version 23.0. Descriptive statistics were presented as frequencies, percentages, means, and standard deviations. The normality of data distribution was assessed using the Kolmogorov–Smirnov test. When the assumption of normal distribution was met, independent samples t-tests were used for comparisons between two groups, and one-way analysis of variance (ANOVA) was applied for comparisons among three or more groups. For variables in which ANOVA revealed statistically significant differences, appropriate post hoc analyses were conducted to identify the sources of between-group differences. In all statistical analyses, a significance level of p < 0.05 was accepted.
Qualitative Phase
Qualitative Data Collection
Interviews were conducted face-to-face in a quiet and appropriate setting to ensure that participants could express themselves comfortably. Audio recordings were transcribed verbatim after the interviews and anonymized prior to analysis.
Qualitative Data Analysis
Qualitative data were analyzed using descriptive qualitative content analysis, following the core phases described by Braun and Clarke (2013). Interviews were audio-recorded, transcribed verbatim, and read repeatedly to ensure familiarity with the data. Meaningful statements were identified through open coding, and similar codes were grouped into subthemes and then organized under main themes.
Rigor and trustworthiness were enhanced through prolonged engagement with the data, repeated transcript readings, and independent coding by the researchers. Codes and themes were compared, and discrepancies were resolved by consensus. Dependability was supported by an audit trail, confirmability by direct participant quotations, and transferability by detailed descriptions of the study context and participant characteristics.
Data Integration
Quantitative and qualitative data were integrated in three stages. First, quantitative findings informed the qualitative phase, consistent with the “following a thread” approach in explanatory sequential mixed methods design. Second, both datasets were analyzed separately and compared through triangulation to identify convergences and divergences. Finally, iterative researcher discussions enabled a holistic interpretation of patients’ perceptions, trust, ethical concerns, and views on the humanistic dimension of AI-supported surgical care.
Results
Quantitative Phase
Participant Characteristics
A total of 312 surgical patients were included (52.6% female; mean age 50.71 ± 15.16 years). Most participants had limited knowledge of artificial intelligence (44.2%), although 57.1% had previously heard of it, with curiosity being the most common emotional response (32.1%). Attitudes toward artificial intelligence were generally moderate and cautious; 40.1% expressed negative views regarding its use during surgery, while 53.2% were undecided about AI-supported postoperative care. Major concerns included medication administration (68.9%) and reduced human touch (63.8%). Positive attitude scores were significantly higher among younger participants, males, individuals without chronic disease, those with higher education and active employment, and participants with greater knowledge of artificial intelligence (p < .01). In contrast, age was associated with increased negative attitudes. Perceived income, place of residence, previous surgery, and type of surgery were not associated with attitudes (Table 1).
Sociodemographic Characteristics of Participants and Comparison of Attitude Scores Toward Artificial Intelligence in Healthcare According to These Characteristics (n = 312).
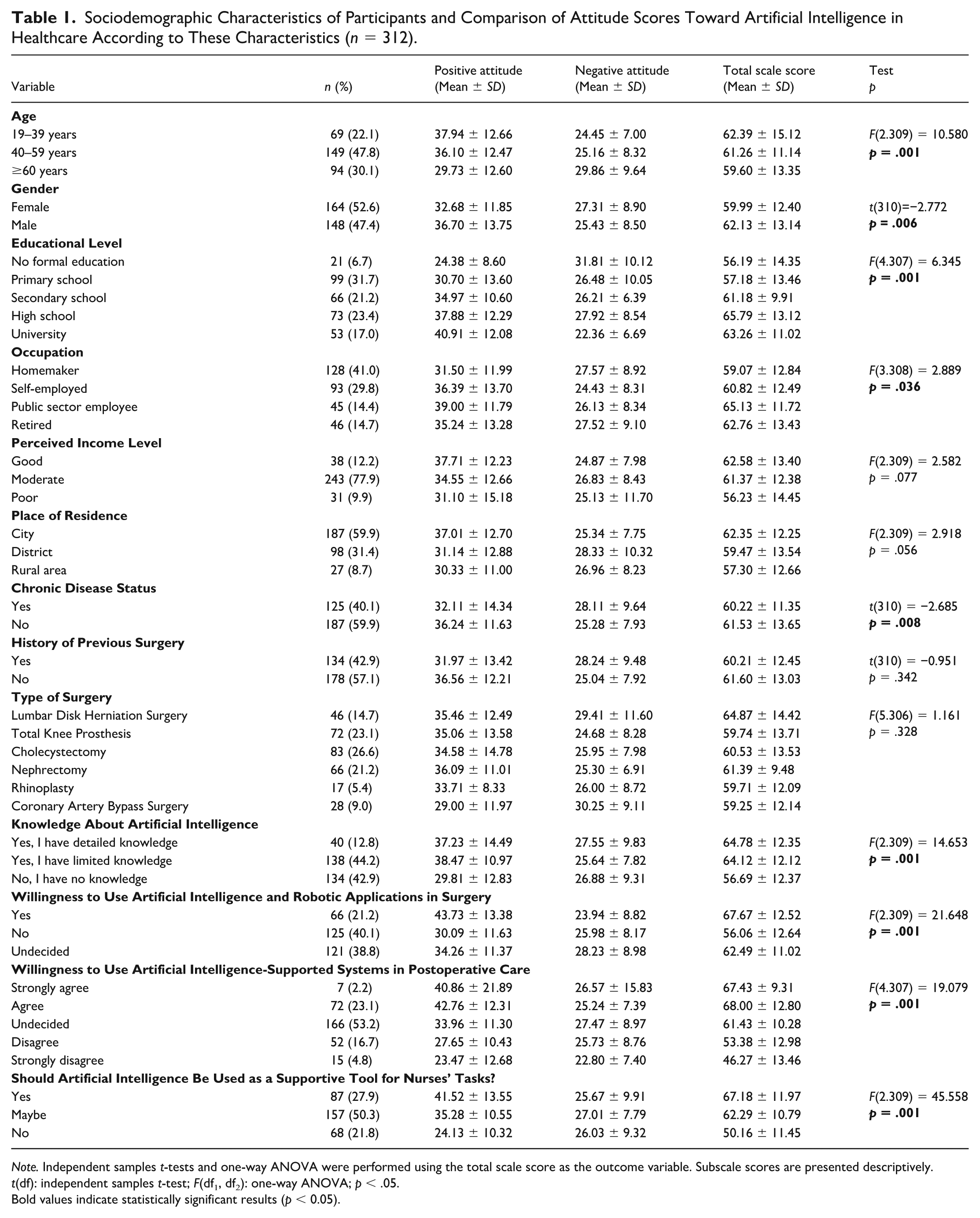
Note. Independent samples t-tests and one-way ANOVA were performed using the total scale score as the outcome variable. Subscale scores are presented descriptively.
t(df): independent samples t-test; F(df₁, df₂): one-way ANOVA; p < .05.
Bold values indicate statistically significant results (p < 0.05).
Participants’ scores on the Positive Attitude subscale of the General Attitude Toward Artificial Intelligence in Healthcare Scale ranged from 0 to 72, with a mean score of 34.58 ± 12.92. Scores on the Negative Attitude subscale ranged from 0 to 48, with a mean of 26.41 ± 8.75. The total scale score ranged from 27 to 102, and the mean total score was 61.00 ± 12.78 (Table 2).
Distribution of Subscale Scores of the General Attitude Toward Artificial Intelligence in Healthcare Scale (N = 312).

Qualitative Phase
Interviewee Characteristics
The qualitative sample consisted of 15 participants, the majority of whom were women (n = 8), with a mean age of 52.3 ± 14.8 years (range: 29–78). Most participants had secondary/high school education (n = 6) and were homemakers (n = 6). The majority reported no chronic disease (n = 9) and no previous surgical history (n = 8). Most participants had limited knowledge of artificial intelligence (n = 6), and attitudes toward artificial intelligence were evenly distributed across low, moderate, and high levels (n = 5 each).
Interview Findings
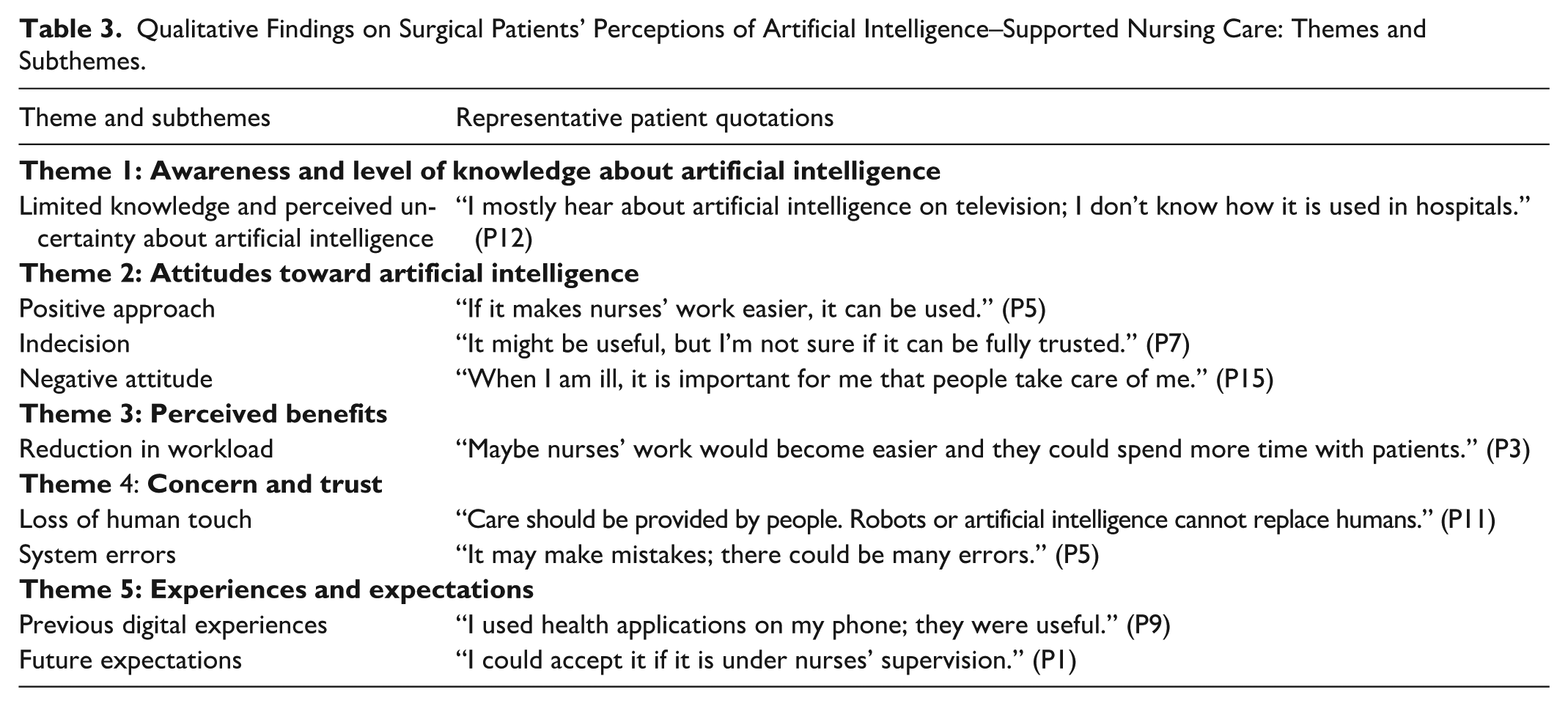
As a result of the qualitative analysis, five main themes were identified to explain participants’ perceptions and experiences related to artificial intelligence: (1) awareness and level of knowledge about artificial intelligence, (2) attitudes toward artificial intelligence, (3) perceived benefits, (4) concern and trust, and (5) experiences and expectations. These themes were developed based on similarities in content and recurring meaning patterns across participants’ narratives (see Table 3).
Qualitative Findings on Surgical Patients’ Perceptions of Artificial Intelligence–Supported Nursing Care: Themes and Subthemes.
Theme 1: Awareness and Level of Knowledge about Artificial Intelligence
Qualitative analysis identified awareness and level of knowledge about artificial intelligence as a main theme, reflecting how participants conceptualized AI. The subtheme limited knowledge and perceived uncertainty showed that participants encountered AI mainly through television, the internet, and news media but lacked clear understanding of its use in health care, particularly in surgical care and nursing. Many associated AI with robots and were uncertain about its role in patient care.
Representative participant statements illustrating this subtheme are presented below: I hear about artificial intelligence on television; they say it is used in many things, but I don’t know what it does in healthcare. Now even intelligence has become artificial. Everything is becoming artificial. (P3) I hear the name, but I don’t know how it is used during surgery or while caring for patients in the hospital. It must be a computer or a robot; I think that is artificial intelligence. (P7) It appears on television and the internet, but I don’t know if it really exists in hospitals or if it is actually being used. I couldn’t figure out what it would be used for in a hospital. Will robots take care of us? (P11)
Theme 2: Attitudes Toward Artificial Intelligence
Participants’ attitudes toward AI in health care varied considerably. Three subthemes were identified: positive approach, indecision, and negative attitude, reflecting diverse emotional and cognitive evaluations of artificial intelligence.
Some participants expressed a positive approach, believing that artificial intelligence could support the care process by reducing nurses’ workload: If it makes nurses’ work easier, it can be used. There are so many patients; maybe if nurses benefit from artificial intelligence, their work will become easier. After all, why does technology advance? To make things easier . . . And if it means we will receive better care, then it should be used. (P5)
However, some participants, while acknowledging the potential benefits of artificial intelligence, reported indecision regarding its reliability. This uncertainty was particularly associated with concerns about data security and perceived loss of control: It might be useful, but I don’t know if it can be trusted. Many banks or institutions cannot protect our information. Using artificial intelligence in hospitals might also lead to our data being used by others. (P7)
Participants expressing a negative attitude emphasized that human interaction and individualized attention are indispensable in the care process and voiced concerns that AI-supported applications might weaken these aspects. These views also encompassed broader anxieties and a sense of alienation related to technological advancement: When I am ill, I want people to take care of me. Everything is becoming machines—yes, things get easier, but it’s also frightening . . . They even say it will take over the world. (P15) When I am a patient, it is very important for someone to talk to me and show interest. Machines are frightening. Let them be used in other fields, but healthcare is different . . . Is this much technology really right? Where will it all lead? Will the next step be living in space? Sometimes this level of technology worries me. (P11)
Theme 3: Perceived Benefits
The qualitative analysis showed that perceived benefits was a prominent theme in participants’ evaluations of AI use in health care. The subtheme reduction in workload indicated that AI-supported applications could reduce nurses’ routine tasks and increase the time available for direct patient care.
It is noteworthy that perceived benefits were described indirectly through improvements in nursing care, rather than in terms of direct patient–technology interaction or personal experience.
Representative participant statements reflecting this subtheme are presented below: Maybe nurses’ work would become easier, and they could pay more attention to patients. But I don’t know which tasks of nurses it would actually do. (P3) If nurses’ workload is reduced, they can spend more time with us. Benefiting from technology is a good thing—why not? Artificial intelligence wouldn’t have emerged for nothing. We shouldn’t oppose every innovation. The world has changed; something new comes out every day. (P8)
Theme 4: Concern and Trust
Participants’ evaluations of AI in health care were dominated by trust-related concerns, reflecting cautious and conditional acceptance. Two subthemes, loss of human touch and system errors, captured these concerns. Participants emphasized the importance of human interaction and individualized attention, expressing concern that AI could weaken relational aspects of care. Although viewed as potentially supportive, AI was not considered a replacement for human presence, highlighting care as a relational and emotional process rather than a purely technical one: I speak in my own local way; robots wouldn’t understand that. Artificial intelligence cannot understand my problems. I need to talk to the people working here, tell them where I am in pain, talk to a human being. I may cry and need comfort. Artificial intelligence cannot comfort me. (P1) Care should be provided by people. Robots, artificial intelligence—none of these can replace humans. Everything shouldn’t become digital. It feels like everything is becoming artificial, as if emotions and thoughts no longer matter and everything is turning mechanical. (P11) When I am ill, I want someone to talk to me and show interest. Machines are frightening. Sometimes we share our problems and our lives with nurses. What would robots or artificial intelligence understand about my problems and feelings? (P13)
Some participants also drew attention to the possibility of errors in AI systems, noting that such errors could pose risks to patient safety. Concerns related to incorrect decision-making and technical failures were described as factors that undermine trust. These views reflect a clear reservation regarding the autonomous use of artificial intelligence in health care: Artificial intelligence can make mistakes; there may be many errors. Can it be trusted? After all, machines can break down—what happens if everything gets mixed up? If the electricity goes out, where is artificial intelligence then? Especially in healthcare, things should not be entrusted to machines. (P5) If there is an error and my medication is given to someone else or I receive someone else’s medication, that would be very bad. Humans also make mistakes, but what if a robot or computer breaks down, or if hackers interfere with the data? (P14)
Theme 5: Experiences and Expectations
Another prominent theme was experiences and expectations, with two subthemes: previous digital experiences and future expectations. This theme showed that participants’ past experiences with technology shaped their attitudes toward future AI use. Positive experiences with digital health applications appeared to foster a more open and accepting approach to AI-supported practices: I used applications on my phone for diabetes, such as nutrition tracking, daily water intake, and step counting, and they were useful. If artificial intelligence makes things easier like that, then it should be used. (P9) There is the e-Nabız application where I can see my test results. We also make appointments for examinations through the phone. These are useful applications. I also ask artificial intelligence questions about health—for example, whether there will be problems during surgery or whether there will be a lot of pain after surgery . . . (P14)
A substantial proportion of participants acknowledged that AI-supported applications may have a place in future health care services; however, they emphasized that such use should occur under the supervision of nurses and in a supportive role. The expectation that artificial intelligence should function as an assistive tool rather than a decision-maker was particularly prominent.
These findings suggest that artificial intelligence should be positioned as a tool that complements a human-centered approach in nursing care rather than replacing it: I could accept it if it is under the control of nurses—or at least very well monitored. Unsupervised use or machines working on their own would not be appropriate, especially in healthcare. But if it is supervised, it could be acceptable. (P1) They say robots perform surgeries now. Will artificial intelligence do it next? Technology has advanced a lot; if robots perform surgeries, then artificial intelligence can also be involved. Nurses may use it for patients as well. But everything should not be left entirely to devices. It can be used, of course, but its management and guidance should be carried out by doctors and nurses. (P13)
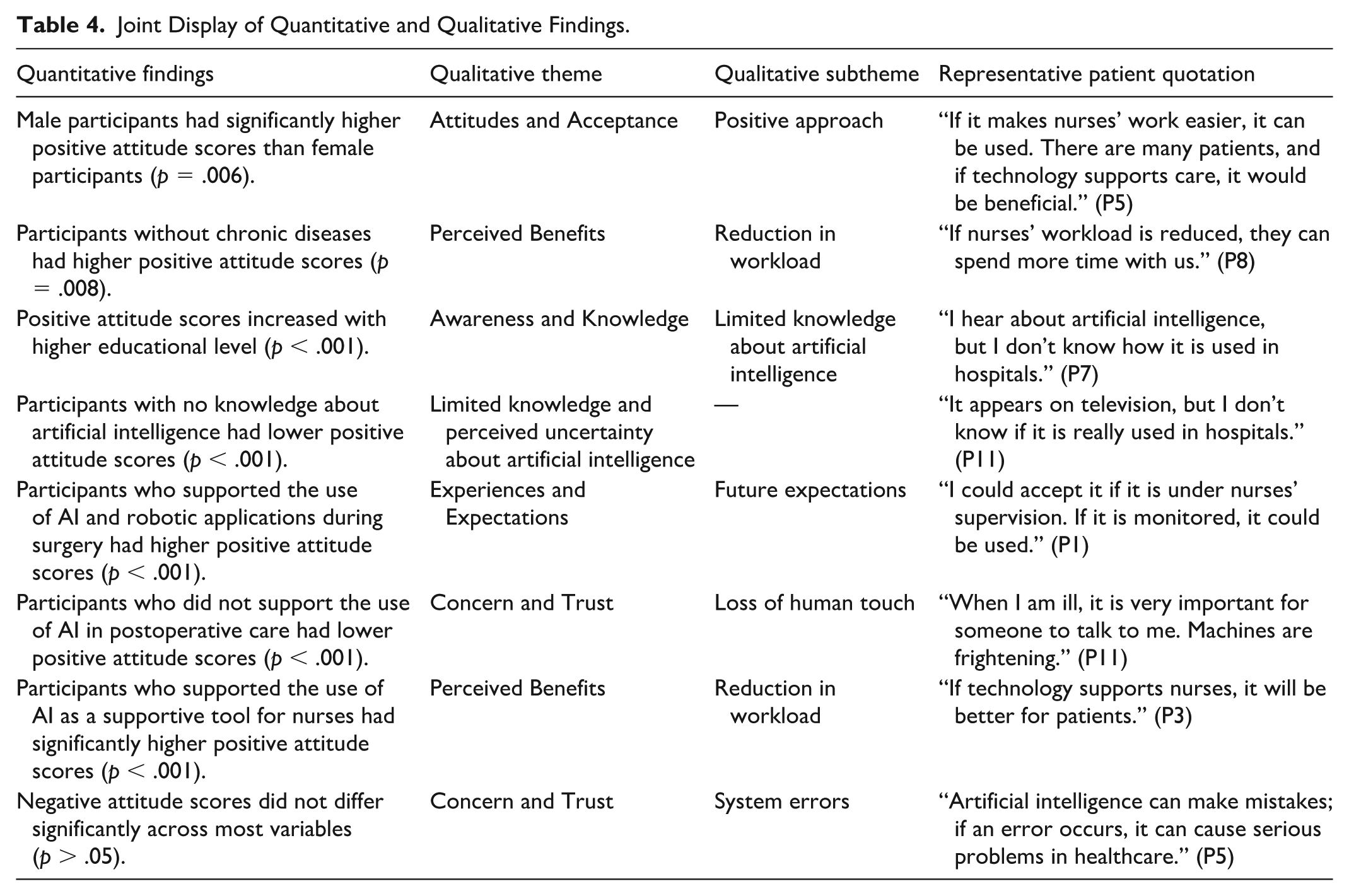
Table 4 was developed to facilitate the integrated interpretation of the findings of the mixed methods study by combining quantitative results with corresponding qualitative themes.
Joint Display of Quantitative and Qualitative Findings.
Discussion
This mixed methods study examined surgical patients’ attitudes toward artificial intelligence (AI)-supported nursing care through a transcultural and patient-centered lens. The findings showed that patients’ acceptance of AI was cautious and conditional, shaped by perceived technical benefits as well as cultural meanings, trust, and expectations regarding human-centered care. Quantitative findings indicated moderate overall attitudes, while qualitative findings showed that patients often perceived AI as a media-driven and abstract concept rather than a concrete part of health care delivery.
From a transcultural nursing perspective, patients’ interpretations of AI were closely related to culturally embedded values such as human interaction, empathy, and professional responsibility. Concerns about loss of human touch and system errors reflected not only technical concerns but also expectations about the relational nature of nursing care. In surgical settings, where patients are vulnerable and dependent on professional care, trust and patient–nurse interaction are particularly important (Osnat, 2025; Young et al., 2021). The expectation that AI should support rather than replace nurses highlights the continuing importance of human presence in care.
Limited knowledge and awareness were key factors shaping attitudes toward AI. Most participants encountered AI mainly through media sources, which contributed to uncertainty and ambiguous perceptions. Although participants expressed curiosity and interest, these were accompanied by concerns about safety, control, and reliability. Similar findings in other cultural contexts suggest that superficial exposure to AI may limit acceptance when not supported by meaningful explanations (Fritsch et al., 2022; Gundlack et al., 2025). Therefore, culturally sensitive communication strategies are needed to explain how AI works and how it aligns with patients’ values and expectations.
The moderate scores on the General Attitude Toward Artificial Intelligence in Healthcare Scale also reflected this ambivalence. Participants recognized potential benefits such as efficiency and workload reduction; however, ethical concerns, perceived risks, data security, and reduced human oversight limited stronger acceptance. Consistent with previous research, patient acceptance appears to depend on transparency, accountability, and professional control over AI systems (Faiyazuddin et al., 2025).
Sociodemographic differences further showed that AI perceptions are culturally and socially situated. Younger participants reported more positive attitudes, possibly due to greater exposure to digital technologies, whereas older individuals expressed stronger concerns about trust, familiarity, and interpersonal communication (Kaya & İşci, 2025; Fritsch et al., 2022). Higher education was associated with greater acceptance, potentially reflecting higher digital literacy, while lower education levels were linked to uncertainty and apprehension (Lee et al., 2022). Participants without chronic diseases were more positive, whereas those with chronic conditions were more cautious, possibly due to greater reliance on continuity and individualized care (Antes et al., 2021; Wang et al., 2023). Occupational status also influenced attitudes, while type of surgery did not, suggesting that broader cultural beliefs, trust, and ethical concerns may be more influential than specific clinical experiences (Longoni et al., 2019; Topol, 2019).
Although studies on patients’ perspectives toward AI are increasing, most have used quantitative designs or focused on general health care contexts. The present study extends previous research by showing that surgical patients’ acceptance of AI-supported nursing care is shaped not only by technological awareness but also by cultural, relational, and ethical meanings. Qualitative findings particularly highlighted the importance of human presence, empathy, and professional responsibility in surgical care.
These findings have implications for nursing education and future research. Nursing curricula should include AI literacy at undergraduate and postgraduate levels, addressing technical knowledge as well as ethics, patient safety, data security, and human-centered care. Simulation-based learning and case-based discussions may help nurses use AI-supported systems while preserving empathy and patient–nurse interaction.
Future studies should examine changes in patient attitudes as exposure to AI technologies increases and compare findings across different cultural contexts. Intervention studies evaluating educational strategies to improve patients’ knowledge, trust, and acceptance of AI may also support more effective implementation. Mixed methods approaches should continue to be used to capture both measurable attitudes and deeper experiential dimensions.
Overall, surgical patients perceived AI as a supportive tool rather than an autonomous agent. Enhancing patient education, ensuring transparency, and respecting cultural values related to human connection and professional oversight are essential for trust. From a transcultural nursing perspective, ethical and sustainable AI integration into surgical care requires alignment with patients’ cultural expectations, relational needs, and meanings attributed to nursing care.
Conclusion
This study indicates that surgical patients approach artificial intelligence-supported nursing care with cautious acceptance shaped by limited knowledge and strong ethical and humanistic concerns. While patients acknowledge the supportive potential of artificial intelligence, they emphasize the preservation of human touch, trust, and professional supervision. These findings suggest that culturally sensitive, transparent, and patient-centered approaches are essential for the ethical and sustainable integration of artificial intelligence into surgical nursing care.
Footnotes
Acknowledgements
We extend our sincere gratitude to all participants for their valuable contributions to this study.
Ethical Considerations
The study was started after an ethics committee approval was obtained from the Osmaniye Korkut Ata University Ethics Committee (Decision No: 2025/22; Date: May 23, 2025) and an institutional permission was granted from the institution where the study was conducted. All participants gave written informed consent before participating in the study.
Author Contributions
Songül Güngör (SG) and Gülseren Maraş Baydoğan (GMB) contributed to the conception and design of this study; SG collected the data of the study; SG performed the statistical analysis of the manuscript; Kezban Koraş Sözen (KKS); SG critically reviewed the manuscript and supervised the whole study process. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available due to the protection of personal data of participants but are available from the corresponding author on reasonable request.