
Abstract
Kin caregivers provide support to millions of children in the United States when their biological parents are unable. Despite their critical role, kin caregivers often lack financial, medical, legal, housing, and support resources. These inequities are exacerbated in rural areas. The Wyoming/Montana Kinship Navigator Program was designed to improve outcomes for caregivers and children with a rural, solution-focused, enhanced case-management model. This evaluation protocol includes a quasi-experimental design and propensity score matching for baseline equivalence. Outcomes include caregiver well-being, service access, and child permanency obtained through surveys and administrative records. Findings from this novel two-state evaluation partnership will support an evidence-base regarding rural kinship navigator models and will inform the Title IV-E Prevention Services Clearinghouse program review.
Introduction
According to the U.S. Census Bureau (2025), kin caregivers provide critical support to about 2.5 million children in the United States when their biological parents are unable to provide care. In rural states such as Wyoming and Montana, 3% of children are being raised in kinship care. Thus, 4,000 and 7,000 youth are living in kinship arrangements in Wyoming and Montana, respectively (Kids Count Data Book, 2025). Kinship care refers to situations in which a child is cared for full-time by relatives or adults with whom they have a family-like relationship (Child Welfare Information Gateway, 2025). Although most children in kinship care live with a grandparent (62.1%), a report produced by the United States Government Accountability Office showed that children in kinship care may also live with other relatives (24.8%) or with nonrelative fictive kin (13.1%; United States Government Accountability Office, 2020).
Regardless of the pathway into kinship care, placement with kin is typically preferred over foster care (Wheeler & Vollet, 2017), as it may provide stability and may help children maintain family connections (Riehl & Shuman, 2019). Kin caregivers also help to keep youth out of the overburdened foster care system (Washington et al., 2025). In fact, according to the U.S. Department of Health and Human Services, and as reported in the Kids Count Data Book (2025), since 2019, kin care programs have had a positive impact in reducing the number of children moving into the foster care system. Moreover, this family-like support is shown to be beneficial to child well-being (Bell & Romano, 2017; Bramlett et al., 2017), and kinship care arrangements have been associated with improved outcomes related to child behavior (Washington et al., 2018), mental health, well-being (Stewart et al., 2024), and child permanency (Bell & Romano, 2017) as compared to non-kin, out-of-home placement.
Because kinship caregivers are not always a part of the formal foster system, they may lack access to critical resources and services to support themselves or kin children in their care. For example, compared with their formal counterparts, informal kin caregivers are less likely to obtain support for financial, medical, and legal services, as well as support for childcare, respite, and housing assistance (Gleeson et al., 2009; Hernandez et al., 2014). Yet these kinship caregivers are known to experience more health challenges, poorer physical and mental health, higher caregiver stress, and may have lower educational attainment than traditional foster caregivers (Garcia et al., 2015). In addition, kinship families are more likely than non-kin foster families to experience economic challenges, live in poverty, experience food insecurity, and lack job stability (Lee et al., 2017). Despite these heightened needs, kinship families are less likely to seek or less able to access financial assistance or support services than non-kin caregivers. Insufficient financial resources rank as a top unmet need (Coleman & Wu, 2016; Schlatter et al., 2023).
Several programs have been developed to assist kinship caregivers in obtaining needed education, support, and resources to care for children who are not biologically their own. Although programs exist in varying geographic areas in the country (Forehand et al., 2024; Fowler et al., 2023; Littlewood et al., 2023; Preston, 2021a; Wheeler et al., 2020), few are developed to address the needs of rural families. The purpose of this manuscript is to describe a novel, two-state model to assist rural kinship caregivers as they navigate the process of providing care to kin children. The manuscript also describes the evaluation design and identifies key questions to be answered by the evaluation.
Literature Review
The Family First Prevention Services Act (FFPSA), enacted as part of Public Law (PL) 115-123 (FFPSA, 2018), amended Title IV-E to allow Title IV-E agencies to receive federal funding for programs that support both licensed and unlicensed kinship families in accessing resources (Lindell et al., 2020). Title IV-E agencies approved to operate kinship navigator programs may claim 50% Federal Financial Participation for allowable kinship navigator program administration and delivery. To qualify for reimbursement, states must employ program models that meet service criteria and have been tested, reviewed, and rated by the Title IV-E Prevention Services Clearinghouse as meeting promising, supported, or well-supported practice standards (Wilson et al., 2024). Although there were no approved kinship programs when the FFPSA went into effect, there are currently 14 Title IV-E state agencies approved to operate six Clearinghouse-rated evidence-based kinship navigator programs. As of 2025, the approved states and territories include Washington, Colorado, Ohio, Arizona, Florida, Nevada, Delaware, Iowa, Minnesota, Nebraska, South Carolina, Utah, Virginia, and Puerto Rico (Children’s Bureau, 2025).
Program Services in Approved Kinship Navigator Programs
To qualify for federal funding under the FFPSA, kinship navigator programs must meet the following service criteria as described in section 427(a)(1) of the Social Security Act: (a) they must coordinate with other state or local agencies who promote service coordination or referral services (e.g., 2-1-1 services, 3-1-1 information systems); (b) they should be planned and operated in consultation with kinship caregivers, youth raised in kinship care, and organizations that both represent caregivers’ interests and provide outreach to kinship families; (c) they must establish information and referral services that link kinship caregivers with relevant training and legal assistance; (d) they should provide outreach to kinship care families, including by establishing, distributing, and updating a kinship care website, or other relevant guides or outreach materials; and (e) they should promote partnerships between public and private agencies across sectors including schools, community-based or faith-based organizations, and relevant government agencies, to increase their knowledge of the needs of kinship families (“Social Security Act, 42 U.S.C. § 627(a)(1)(A)–(E),” 2018).
Although there is heterogeneity in program components, methodology of intervention design, evaluation approaches, and measured outcomes, many states show areas of overlap, and results for caregivers and youth are generally positive (Forehand et al., 2024; Fowler et al., 2023; Littlewood et al., 2020, 2021, 2023; Preston, 2021a, 2021b; Schmidt & Treinen, 2021; Wheeler et al., 2020). All programs integrate information and referral services into their program models, and most programs conduct needs assessments for individual families. In addition, several programs provide case management, peer support or support groups, caregiver education/training, or legal services (Arizona’s Children Association, 2017; Forehand et al., 2024; Littlewood et al., 2020, 2021, 2023; Preston, 2021a, 2021b; Wheeler et al., 2020). Some programs incorporate less common components such as the creation of a genogram and backup placement plan (Colorado; Forehand et al., 2024), a web-based resource to promote access and coordination (Florida; Littlewood et al., 2023), and mental health assessment and treatment (Ohio; Wheeler et al., 2020). Despite representation from several geographic regions of the United States and its territories, few, if any, have been developed to serve and incorporate rural populations into their respective kinship navigator programs.
Evaluation of Approved Kinship Navigator Programs
Per Title IV-E Prevention Services Clearinghouse standards of review, approved program evaluations have approved study designs (e.g., either used randomized control or quasi-experimental designs [QEDs] with comparison groups) (Forehand et al., 2024; Fowler et al., 2023; Littlewood et al., 2020; Preston, 2021a, 2021b; Schmidt & Treinen, 2021; Wheeler et al., 2020). Only one state specifically included rural as a demographic characteristic, with one of seven counties classified as rural (Forehand et al., 2024). Although not specifically, another state’s evaluation of 19 counties contained eight designated “nonmetro” as defined by the United States Department of Agriculture Economic Research Service (Fowler et al., 2023; U.S. Department of Agriculture [USDA], 2013). All other programs were evaluated in one or two “metro” designated counties. This makes it difficult to predict whether results observed in states with high urban representation would be replicated for kinship navigator programs that serve a majority rural population, and whether rural kin families may benefit from services tailored to their unique needs.
States with approved programs have produced evidence of benefit to both kin caregivers and children in their care. Overall, these evaluations have shown that kinship navigator programs are successful in connecting kin families to services (e.g., support groups and Temporary Assistance for Needy Families [TANF]-Child-Only benefits; Fowler et al., 2023; Littlewood et al., 2021; Preston, 2021a, 2021b). They have also resulted in positive caregiver well-being outcomes and high satisfaction across service types (Fowler et al., 2023; Littlewood et al., 2021). Kinship navigator programs have also promoted positive placement outcomes for youth in kinship care, as evidenced by shorter case episodes, lower likelihood to enter foster care, greater retention in kinship care until reunification with parents, less placement disruption, and less re-entry into the child welfare system than those in other types of services (e.g., services as usual; (Forehand et al., 2024; Littlewood et al., 2020; Preston, 2021a; Schmidt & Treinen, 2021; Wheeler et al., 2020). In contrast, outcomes for youth maltreatment were mixed, with one program finding similar rates between intervention and control, whereas another program showed the benefit of kinship navigator programs on maltreatment outcomes (Littlewood et al., 2020; Wheeler et al., 2020). Overall, the results of existing kinship navigator programs are promising. However, the limited rural representation within program evaluation samples indicates a need for further evaluation of kinship navigator programs delivered in rural states.
Rural Kinship Navigator Programs
Rural populations face some unique challenges for program delivery, evaluation standards, and kinship family environments. Although the U.S. Census Bureau does not formally define “rural” (United States Census Bureau, 2020), it refers to areas that are a great distance from urban resources and are of low population density compared with metropolitan areas (United States Department of Agriculture Economic Research Service, 2025). The low population density means rural area programs may struggle to obtain the sample sizes needed to generate adequately powered impact estimates, namely, statistical significance required for Title IV-E Prevention and Services Clearinghouse approval (Wilson et al., 2024). Both urban and rural contexts have been linked to challenges with distance to resources, time to access, and affordability of home and community-based resources for their residents (Siconolfi et al., 2019). Similarly, they have fewer high-paying, professional job opportunities, but rural communities face even more challenges in accessing health care with fewer primary care physicians or mental health providers per capita (Franco et al., 2021). Professionals in rural communities often have a multiplicity of roles, serving as a “jack of all trades,” potentially limiting the ability for the wide variety of direct, in-person services that might be found in more populated locations (Chisengantambu-Winters et al., 2024). In addition to provider limitations, rural families report challenges with access to social services, unemployment, limited housing access, and long travel times for work (Rodriguez & Grahame, 2017; Siconolfi et al., 2019). Despite these challenges, rural communities and particularly indigenous communities possess strengths such as strong social capital, which encourages family support, informal caregiving, and connection (Siconolfi et al., 2019; Yeung et al., 2021). Taken together, it is likely that rural families may benefit from a tailored, solution-focused approach to resource navigation to improve their outcomes.
The Wyoming/Montana Kinship Collaborative
Developing collaborative efforts between rural states to design, deliver, and evaluate kinship navigator models has the potential to strengthen evaluation design and increase the potential for a successful Prevention Services Clearinghouse review. The multi-state Rural Kinship Navigator Collaborative, which includes Wyoming, Montana, Vermont, and Maine, was established in 2022 with support and technical assistance from Casey Family Programs, Generations United, and the University of Washington School of Social Work. As neighboring states in the “top five” for most population residing in areas designated frontier and remote rural, Wyoming and Montana, specifically, decided to collaborate in parallel kinship navigator programs as a unique partnership designed to maximize capacity for rigorous program evaluation. Additional partners in each state served as evaluators, providing guidance and oversight to the collaborative program.
The Wyoming/Montana Kinship Navigator Program was designed as a 6-month, enhanced case-management model based on a solution-focused approach (Blundo & Simon, 2016). Solution-focused case management is a framework that emphasizes abilities, strengths, and individual goals rather than disability. Within this approach, kinship navigators identify caregiver goals, monitor progress, and coordinate with and refer to other agencies. The needs of kinship caregivers and children are placed at the center of all services. As shown in Figure 1, the program services include six components: (a) partnerships with kinship families and organizations including with stakeholder oversight committees (i.e., caregivers, youth, coalition leaders, and local kin organizations) to provide ongoing feedback; (b) outreach, information and referral, including assistance in accessing benefits as needed; (c) needs assessment and case management; (d) caregiver education; (e) peer support; and (f) urgent needs and concrete goods (see Figure 1). Each state uniquely housed navigators within existing outreach and referral programs. For example, Wyoming is housed within 2-1-1 services, and Montana is housed within Montana University Extension Services. The navigators delivering these services are all trained in the same solutions-focused tenets as well as in case-management techniques, caregiver education needs and resources, and legal/public benefits.
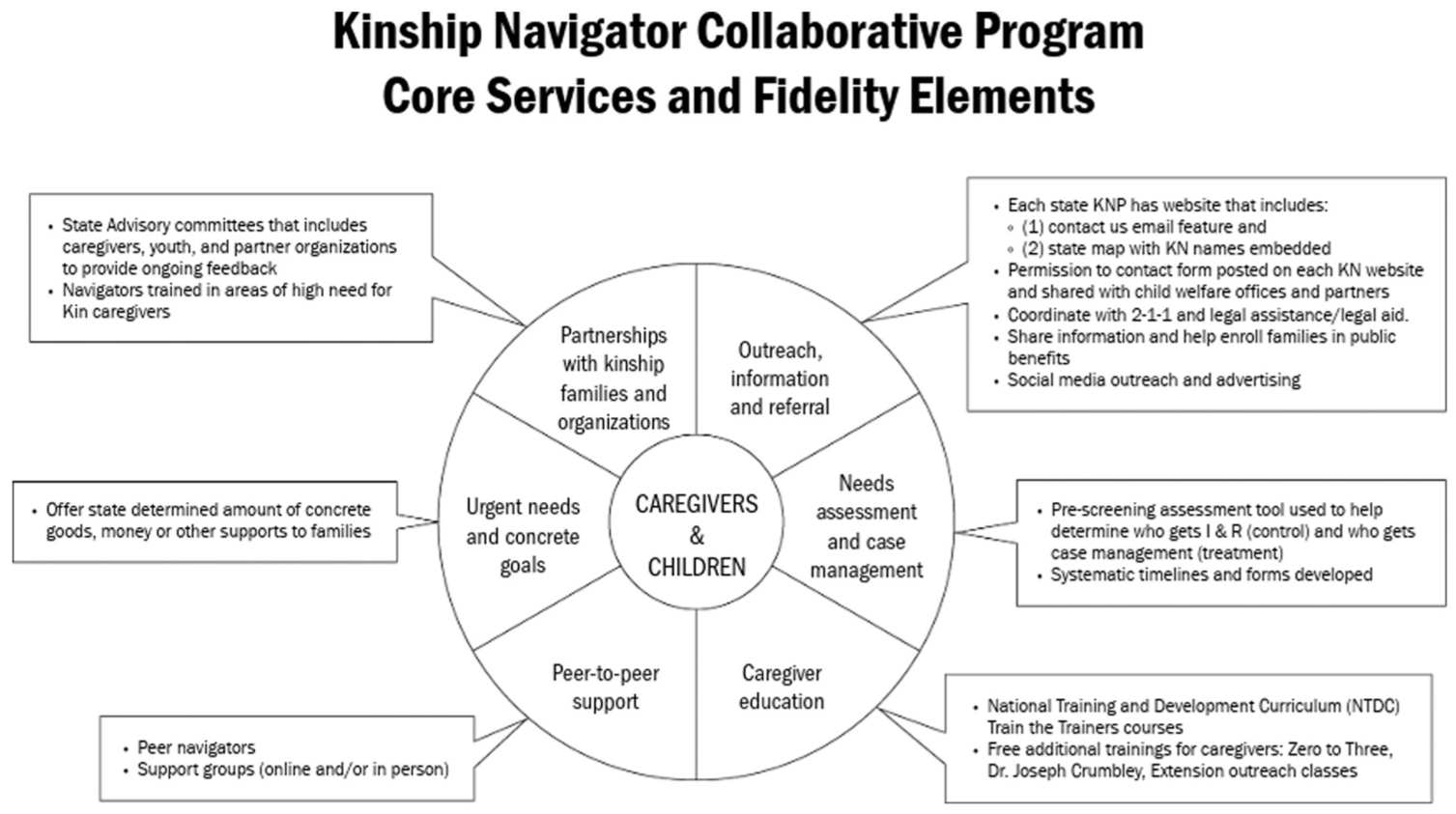
Core services of the Wyoming/Montana Kinship Navigator Program.
As part of the program model, navigators conduct family needs assessments with kin caregivers at the initial meeting or within 3 weeks of the initial meeting (Routh et al., 2024). Navigators use information from the assessment to set goals and provide solution-focused, enhanced case-management services and referrals. Goals are revisited and revised as needed, and assistance is provided to access services at 3 weeks, 3 months, and potentially, 6 months post-enrollment, depending on when cases close. Caregiver education and peer-support are also offered to all program enrollees. Specifically, the National Training and Development Curriculum (NTDC) for Foster and Adoptive Parents are offered to all kinship caregivers, including training related to accessing services; impacts of substance use; separation, grief, and loss; trauma-related behaviors; trauma-informed parenting; kinship parenting; building resilience; parenting diverse families; and cultural humility. Additional training is offered regarding parenting young children ages 0 to 3. Peer-to-peer kinship caregiver support groups are offered both online and in person, with localized or statewide representation depending on caregivers’ needs and interests. Finally, navigators can meet urgent needs and needs for concrete goods with one-time support.
Theory of Change
As previously noted, kinship caregivers often lack information and resources, not knowing what services are available to support them. This may include available services and benefits, access to legal assistance and financial resources, education about kinship caregiving issues, emotional and social support, and knowledge of how to navigate child welfare, educational supports, and social service systems. These challenges may lead to adverse consequences such as caregiver stress and placement instability. Ensuring child stability and well-being, along with kinship caregiver well-being can be further complicated by residing in rural and remote contexts.
The Wyoming/Montana Kinship Navigator Program aims to serve kin caregivers of children who would, but for the willingness of family or fictive kin, be placed in the nonrelative foster-care system in both metropolitan and non-metropolitan areas (e.g., rural and remote areas) as well as tribal lands. The Program employs trained navigators and partners with kin family serving stakeholders (e.g., community organizations, legal resources, schools, government agencies, etc.) to recruit, connect, and support kinship families across both frontier rural states. Navigators provide individualized supports to caregivers working across their complex rural systems through distance information and referral as well as enhanced-case management with individualized plans; peer support and education; advocacy and systems navigation (e.g., schools, courts); and regular follow-up connections. These activities serve to increase access to services and supports, individually tailor plans to meet unique needs, and connect families with localized resources. Through this model, caregiver stress should be reduced, which in turn is expected to improve longer-term caregiver well-being. Greater caregiver awareness and utilization of resources should also lead to an improved stability of placement for the kin child(ren).
Purpose of the Evaluation
This manuscript describes a protocol for the evaluation of a two-state partnership examining a shared kinship navigator model. The purpose of evaluating this program is to examine the feasibility, acceptability, and impact of the Wyoming/Montana Kinship Navigator Program model on outcomes for kinship caregivers and children. The primary questions answered in the current evaluation: (a) Do kinship caregivers who participate in the Wyoming/Montana Kinship Navigator Program model experience greater satisfaction with services, utilizations of services, and improvements in well-being as compared to caregivers who are enrolled in a minimal support program? and (b) Do children cared for by kinship caregivers who participate in the Wyoming/Montana Kinship Navigator Program model experience greater stability than do children enrolled in the comparison program (i.e., minimal support)? It is expected that, relative to the comparison group, caregivers in the intervention will engage in greater utilization of services and experience greater improvements in caregiver well-being than those in the comparison group. It is also expected that intervention will result in greater placement stability (i.e., permanency) for children in the intervention than in the comparison groups. These outcomes are each identified as important for measuring program impacts. The current evaluation protocol supports Wyoming’s and Montana’s mutual goal of developing a kinship navigator program that will be eligible for a clearinghouse approval rating that will allow them to be reimbursed through Title IV-E funding, thereby supporting the sustainability of the program within each state. Furthermore, the kinship navigator program described in this protocol is uniquely focused on caregivers and children in two states with large rural/frontier populations. Although prior initiatives have operated in geographically diverse areas and included some rural participants, they have not centered their implementation and evaluation on rural contexts, including service scarcity, transportation challenges, broadband limitations and other constraints. The program and evaluation partnership among these two rural states itself is also unique. By combining evaluation efforts, we expect to achieve a sufficiently large and diverse sample to conduct a rigorously powered evaluation. This effort will enhance generalizability to rural and frontier regions nationwide and will serve as a model for other low-density states seeking to conduct methodologically rigorous evaluations and advance rural best practices.
Method
Due to the rurality of both states, limited staffing, and extreme distances to remote or rural locations, it is not practical to use a robust randomized control trial where each family has an equal likelihood of receiving or not receiving intervention services. Therefore, the Wyoming/Montana Kinship Navigator Program evaluation study employs a QED to evaluate the relative impact of intervention and comparison conditions to improve outcomes among kinship caregiver families across both states. In this case, we are using a static group comparison design whereby intervention and comparison groups are compared on posttreatment outcomes. To ensure statistically similar samples, as defined by the Prevention Services Clearinghouse (Wilson et al., 2024), QEDs were employed where an intervention condition is compared with a comparison condition (i.e., counties), but the units (i.e., individuals in this intervention) are not randomly assigned to conditions. As the program delivery is parallel in both Wyoming and Montana, data for the two states will be combined to increase the sample size and, hence, power for detecting differences in outcomes between the groups. The study is estimated to take 4 years to complete. It is being conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Institutional Review Board of Montana State University. Given the program development and evaluative nature of the work, the University of Wyoming determined the project to be nonresearch. Although the University of Wyoming’s board deemed the evaluation, nonresearch procedures were conducted in accordance with the research protocol approved by Montana State University. Data sharing agreements will be implemented to facilitate the sharing of administrative data between each state’s social and health services departments, the program administrators, and evaluation teams.
The intervention is defined as solutions-oriented, enhanced case management, whereas comparison is defined as minimal intervention information and referral services. Given that most kinship caregivers are informal caregivers (Bramlett et al., 2017)—meaning they do not have an open child welfare case —and were already included in services offered by both states prior to program collaboration, we were unable to use child welfare services-as-usual as our comparison condition.
Participants
Kinship caregivers are eligible to enroll in the evaluation study if they meet the following criteria: (a) they identify as a current kin caregiver for one or more children younger than the age of 18, (b) they speak English or Spanish, and (c) they provide informed consent. Participants are excluded if they either have an open case with the Kinship Navigator Program at the start of the evaluation study or if they have had a previously closed case with no change to placement or housing. If participants are unable to be contacted or to enroll at the time of initial recruitment, they may be recontacted for potential enrollment with subsequent referrals or direct outreach to the Kinship Navigator Program.
Measures
Screening Measures
Sociodemographic data are collected about kin caregiver and child characteristics including caregiver age, sex, ethnicity and race, and self-reported socio-economic status (i.e., self-reported receipt of Supplemental Nutrition Assistance Program; SNAP), all assistance received to meet needs (e.g., child support, Women, Infants, and Children Special Supplemental Nutrition Program; Free or reduced school meals, Social Security Income), as well as age, date of birth, sex, and ethnicity and race of each child in kinship care. Administrative data will also be accessed to measure socio-economic status as indicated by receipt of means-tested public assistance: The SNAP provides monthly benefits that help low-income households buy the food that they need for good health. For most households, SNAP funds account for a portion of their food budgets. In this study, we examine SNAP status on the day prior to first contact with the program and enrollment. If the SNAP is received during the relevant period, then the measure has a response of “Recipient.” Otherwise, the measure has a response of “Not a Recipient” for baseline. In Wyoming, SNAP is managed by the Department of Family Services, whereas in Montana, these programs are managed by the Department of Public Health and Human Services, Human & Community Services Division. SNAP data will be used to contextualize the sample and to examine equivalence between those enrolled in the intervention and comparison conditions.
Needs for case management services are assessed using a 14-item pre-screening assessment that was developed for this study. Caregivers are asked about eight Basic (e.g., Do you have livable, safe housing? Are you getting adequate food for two meals a day for you and your kin child(ren)?) and six Situational Needs (e.g., Do you need legal services and information? Do you and your kin child(ren) have dependable transportation?). Caregivers responded “Yes” or “No” to each item. The number of Basic Needs and Situational Needs is summed, and total scores are calculated for each need domain. Higher scores reflect greater needs. The number of Basic and Situational needs is used to determine whether families in enhanced case-management counties qualify for enhanced case-management services.
Outcome Measures
Selection of outcome measures was guided by a balance between methodological rigor and practice feasibility within rural and frontier service contexts. The measures that were selected were determined to minimize administration time, eliminate licensing fees, and reduce the need for reliable broadband access, thereby enhancing their applicability across rural, frontier and under-resourced settings.
A Client Survey was developed for use with both intervention and comparison participants at case closure and 6-month post-closure follow-up time points. The survey, administered online, in person, or over the telephone, measures outcomes related to Child Permanency, Adult Well-Being, and Access to Services. Open-ended, qualitative questions were also developed and included in this study to assess satisfaction with the kinship navigator, the intervention program, and access to services.
Child Permanency is measured using two items: (a) “Is the child still at home?” (Y/N) and, (b) if “Y,” “Why did the child leave home?” Response options include “returned to birth parent,” “moved to foster care,” “moved to another kin caregiver,” “age 18 or older and left the home,” and “other.” At each assessment, the family is given a stability score (i.e., 1 = “stable,” 0 = “unstable”). Stability is indicated if the child remains in the home, if the child returns to a birth parent, or if the child turns 18 and leaves the home. Otherwise, the child’s situation is determined to be unstable.
Adult Well-Being is measured in both the intervention and comparison conditions and refers to the specific skills and capabilities adults need to navigate their worlds in healthy, positive ways and to provide for themselves and their kin children’s needs. For the purposes of this study, well-being is operationalized as mental or emotional health outcomes and is assessed with the following four questions which were derived from the Family Empowerment Questionnaire and determined to be relevant for kinship caregiver populations (Day et al., 2024; Man et al., 2003): (a) “I now feel that I am better able to cope with caring for the child I am raising than before I became involved in kinship care services and activities”; (b) “I do not feel as stressed out as I was before participating in kinship care services and activities”; (c) “I feel as if my overall health and sense of well-being has improved since participating in kinship care services and activities”; and (d) “I am enjoying life more now since participating in kinship care services and activities.” Each item is rated on a 7-point Likert-type scale from Strongly Disagree to Strongly Agree. The mean of the four items is calculated by the evaluation team to create a mean well-being score, with higher scores reflecting greater adult well-being. Face validity was based on the previously published nature of the measured items. This measure is used to study kinship navigator programs and was shown to have strong reliability (i.e., Cronbach’s alpha = .85; Day et al., 2024).
Access to services (i.e., a kinship caregivers’ ability to access services, or utilization of services to support the family’s financial, legal, social, educational, and/or health needs such as medical care, financial assistance, and social services; Wilson et al., 2024) is measured using an adapted version of the Family Needs Scale (Lee et al., 2016). Prior work (Routh et al., 2024) established the broad face validity of the adapted measure for use in a sample of kinship caregivers and established its reliability (i.e., Cronbach’s alpha = .91). Participants completing the measure are asked whether they have used a given resource in the 6 months prior to the assessment. Participants are asked to respond “Yes,” “No,” or “I did not need this.” If the answer is “Yes,” the participant is then prompted with a question, “Was the kinship navigator helpful in getting access to and/or using this service or resource?” Participants are instructed to answer “Yes,” “No,” or “I did not ask the Kinship Navigator for help with this.” Summary scores are created to reflect the total number of services accessed and the total number of services accessed due to the assistance of the navigator.
Administrative Outcomes Data
In addition to the Client Survey, outcomes data are also extracted from administrative records to assess Child-Permanency outcomes and access to services. The Adoption and Foster Care Analysis and Reporting System (AFCARS) data is case-level information on children from all 50 states formally in the foster or adoption system to track their housing placement. Specifically, this tracks “entry” for those beginning an out-of-home placement, “in foster care,” or “exit” within a fiscal year, with additional specifications for why they may have exited (e.g., return to parents, adoption, legally free). Data are gathered from the start of Kinship Program entry (i.e., baseline) to 6 months post closure. If the child has no noted entry (i.e., not formally in the AFCARS system) or remains “in foster care” with a kinship caregiver, then the measure will have a response of “stable placement.” If the child exits only once because they return to parents, age out, or are adopted by kinship caregivers, then the measure will reflect “stable placement.” If the child has multiple “entries” or “exits” within this timeframe or is removed from kinship caregivers for nonrelative caregivers, the measure will have a response of “unstable placement.” The National Child Abuse and Neglect Data System (NCANDS) will also be accessed to provide evidence of child permanency for informal kinship families. As with AFCARS, NCANDS data will be gathered from the start of kinship program entry to 6 months post closure. If the child has a record indicating a move from the kinship family to another family, then the measure will have a response of “unstable.” If there is no record of a move or if the child is in neither the NCANDS nor AFCARS systems, the measure will reflect “stable placement.” Although Child Safety is considered as an important outcome variable to collect from administrative records, it was ultimately not included due to the large portion of informal kinship families who are not tracked in the state administrative systems leading to likely too small of a sample to interpret (Day et al., 2024).
Access to services is also measured using TANF-Child-Only and SNAP service data. TANF-Child-Only aids needy families so that children may be cared for in their own home or the home of relatives. Child-Only cases arise when a parent or caretaker is ineligible to receive TANF assistance, but the child being cared for is eligible for the service and when a child is living with another related adult who is ineligible to receive TANF cash assistance. Both TANF-Child-Only and SNAP data are gathered in the period from 1 day prior to first contact with the program (i.e., baseline) to case closure and from baseline to 6 months post-closure. If services are received under either program during the relevant period, then the measure will have a response of “Recipient” for that service. Otherwise, the measure will have a response of “Not a Recipient.” These data will be compared with data from the intervention Family Needs Assessment and Client Survey data, where caregivers self-report current use of SNAP and TANF in their home.
Procedure
Program participants are recruited in similar ways in each state. Each state’s website includes a “contact us” email or hotline phone number for client self-recruitment in either group. Permission to contact forms to facilitate a warm hand-off were also provided through partner organizations for intervention clients, including childcare scholarship sites, school liaison personnel, Department of Family Services, Extension staff, 211, pediatrician offices, and district judges, through in-person presentations, distribution of referral forms, and flyers. The following considerations were used in the selection of intervention and comparison counties: (a) county participation in a pilot test of enhanced case management services, (b) proximity to an established kinship navigator, (c) county demographic characteristics, including rurality, geography, reservation communities, and (d) presence of kinship peer support groups. A greater number of comparison counties were selected than intervention counties due to differences in size and population density between comparison and intervention counties. Within Wyoming, the intervention was assigned to the following counties: Albany, Converse, Laramie, Natrona, Sheridan, and Sweetwater. In Montana, service was already being provided statewide, so counties were equally divided between intervention and comparison. Intervention counties included: Blaine, Carter, Cascade, Chouteau, Custer, Daniels, Dawson, Fallon, Garfield, Glacier, Granite, Hill, Lake, Liberty, McCone, Mineral, Missoula, Philips, Pondera, Powder River, Powell, Prairie, Ravalli, Richland, Roosevelt, Rosebud, Sheridan, Teton, Toole, Treasure, Valley, and Wibaux. All other counties in both states serve as comparison counties.
All caregivers may receive navigator services regardless of eligibility. Intervention caregivers are eligible to have data included in the analyses if they meet the following conditions: (a) they completed an intake and family needs assessment; (b) they completed a 3-month follow-up; (c) they completed a 6-month follow-up (unless the case closed at 3 months); (d) they were sent a Client Survey by their navigator at case closure; and (e) if the case reflected high fidelity to the model (i.e., at least 75% adherence to expected activities and time intervals). Comparison caregivers are eligible to have their data included in the analysis if they meet the following conditions: (a) they have contact with a navigator during the study period; (b) they are eligible for Kinship Navigator services at that point of contact (meaning they have a kinship child in the home), and (c) they do not move out of the service area before case closure.
Intervention Allocation
Allocation to intervention (i.e., enhanced case management) or the comparison condition (i.e., information and referral) occurs at the individual level and is determined by county of residence. Those from intervention counties who identify two basic needs (e.g., housing, health care) or one complex need (e.g., legal services) and who are interested in receiving case-management services are eligible to participate in the enhanced case management service.
Participants are assigned to the comparison condition if they reside in a designated comparison county; if they reside in an intervention county and do not qualify for case management; or if they reside in an intervention county, qualify for the intervention condition, are placed on the intervention waitlist, but due to Kinship Navigator Program capacity limitations, they self-select out of the enhanced case management services. After the closure of each case, participants may reach out for additional support if they have program-specific questions. Navigators only answer the specific question posed, in line with comparison group protocols.
Treatment Conditions
The intervention (i.e., Enhanced Case Management; Wyoming/Montana Kinship Navigator Program Model) comprises services and support within the Wyoming/Montana Kinship Navigator model. The program offered is similar for all participants in the condition. However, variation is permitted in the program may occur depending upon the results of the screening assessment for need. Enhanced case-management services within that model comprise a minimum of three solution-focused, enhanced case management visits with a trained Kinship Navigator. These visits include a baseline visit (i.e., approximately 60 minutes), as well as visits at 3 weeks and 3 months post-baseline (i.e., 30–45 minutes each). A 6-month post-baseline visit (i.e., 30–45 minutes) is also scheduled if participants remain in the program beyond the 3-month post-baseline visit. Navigators are also available for unlimited ad hoc contacts during the study period. During the 3-month post-baseline visit, navigators assess whether the child remains in the home. Needs and goals are also re-evaluated. If the child has left the home or goals are met, and no additional needs are present, the Kinship Navigator closes the case and initiates the post-intervention follow-up period. If the child remains in the home and goals are unmet or additional needs and goals are identified, the Kinship Navigator extends services and includes one additional visit at 6 months post-baseline. At the 6-month post-baseline visit, the participant’s goals are re-evaluated, and the case is closed. The method of contact for all visits is determined by the preference of the participant. All baseline visits take place either in person or by telephone. All follow-up visits include in-person, telephone, email, or text contact as determined by the preference of the participant. Participants are compensated for the completion of each assessment timepoint and receive $150 total for their participation.
Prior to the evaluation study, service-as-usual was information-and-referral-like services available throughout Montana and parts of Wyoming. Together, Montana and Wyoming programs refined comparison service protocols based on both states’ service-as-usual programs. Participants in the comparison condition (i.e., those from comparison counties) receive a consistent, minimal follow-up version of information and referral services (i.e., minimal support condition). This service includes receiving a standardized packet including resources and information (e.g., general state resources and contacts along with a county-specific form with additional resources; resource types include legal aid, self-care, Grandfamilies facts, financial and housing, food and nutrition). Participants can also initiate contact with the Kinship Navigators to request additional resources. Neither outreach for purposes of case management nor concrete goods are offered by Kinship Navigators to comparison service participants. Navigators are available for unlimited ad hoc contacts initiated by the participants. All comparison cases remain open until 4 to 6 weeks after the participant’s last contact with the Kinship Navigators. Once a 4- to 6-week period elapses, the case is closed, and follow-up evaluation processes are initiated. If the case remains open at the 6-month timepoint due to continued contact, the case is then automatically closed and follow-up processes initiated. All contact with participants in the comparison takes place by telephone, text, or email. Participants receive a total of $150 for completion of assessments throughout the study.
Participants who engage in the comparison condition are only eligible to receive enhanced case management in the following circumstances: (a) if their comparison case is closed, (b) if they reside in an intervention county, and (c) if they qualify for enhanced case-management services. In this circumstance, all information and referral data for the participant is deleted, a new case is opened with assignment to the intervention condition, and new data is collected. Otherwise, participants in the comparison condition cannot participate in enhanced case management later during the study period. All services offered to participants are documented in an electronic participant record management system and extracted for entry into SPSS for analysis of process, fidelity, and outcomes.
Statistical Analyses
The sample size for this study will include 250 caregivers total (125 per treatment arm). This is feasible based on each state’s prior work and the estimated prevalence of children in kinship care and caregivers providing care. We chose the sample size for this study using power calculations based on the odds ratios for improvement observed in another study of a kinship navigator program completed in Washington state (Day et al., 2024). The required sample size was estimated using G*Power 3.1 for a one-tailed test with α = .05, 80% power, an expected odds ratio based on existing evidence (Day et al., 2024) of 1.8 (e.g., Adult Well-being) to 3.0 or greater (e.g., services access, support group) and a baseline probability of .20 ranges from 103 to 387 participants.
SPSS will be used to calculate general descriptive statistics for program participants and will be used to perform statistical tests. Incomplete responses (i.e., less than 80% of the survey completed) will not be included in the analysis. Reasons for data missingness will be examined, and determined whether they are missing completely at random, missing at random, or not missing at random. Should it be determined that data are missing completely at random, or missing at random, multiple imputation will be conducted for intervention and comparison groups, respectively, in which all covariates in the imputation are included in the impact models and that include the outcome in the imputation. Findings will be presented for both imputed and non-imputed missing data sets. Multiple imputation will be used for those with 80% or greater of the survey responses completed, but with remaining missing data. Fidelity to protocol and assessment timepoints are calculated for each condition. Only cases with at least 75% adherence to protocol and assessment timepoints will be included in the analysis.
To ensure that any differences in outcomes between the intervention and comparison conditions are due to group assignment and not underlying demographic differences, we used propensity-score matching to establish the analytic sample (Shadish et al., 2006). Propensity score matching (PSM) was used to create dyads for comparison. A propensity score is the estimate of the likelihood that a given individual will be classified in a particular group, given a set of specified characteristics (Holmes, 2014). The goal of PSM is to compare intervention and comparison conditions on individuals who have similar likelihoods for receiving the intervention, given the specified characteristics. For our analysis, Caregiver Age, Caregiver Race/Ethnicity, and SNAP Benefit will be used. A composite score for matching participants between intervention and comparison groups will be computed using logistic regression with nearest neighbor matching, a ratio of 1, and the treatment group as the dependent variable. Cases are matched on the proximity of scores to each other (Gibson et al., 2019). The absolute standard mean difference and variance ratios of the demographic measures will be reported to understand the quality of the PSM and to determine baseline equivalence. To ensure that any differences in outcomes between the intervention and the comparison groups are due to group assignment and not underlying demographic differences, we will examine the equivalence of groups in each analytic sample at baseline. We will examine the child’s biological age at the time of enrollment as determined by birth year on a numerical scale, ethnicity and race of the responding caregiver and their child(ren), and socioeconomic status operationalized as SNAP participation as determined by administrative data at baseline. Equivalence will be assessed by examining baseline differences expressed in effect size units according to procedures outlined in guidance from the Prevention Services Clearinghouse (Wilson et al., 2024). Effect sizes less than 0.05 will be considered equivalent with no further need for adjustment in analysis, while variables will be included as covariates in the impact analysis for which baseline effect sizes are between 0.25 and 0.05 (Wilson et al., 2024). After establishing baseline equivalence between intervention and comparison conditions for the analytic sample, dichotomous variables will be evaluated for how likely it is that any observed difference between the intervention condition and control condition is due to change using a series of logistic regression analyses. These analyses will include necessary control variables. Effect size and statistical significance will be reported for any observed difference in outcomes for each dependent variable. Alpha will be set to p < .05. All results will be one-tailed, reflecting the expected superiority of the intervention relative to the comparison condition.
Discussion
Developing an evidence-base to secure permanent funding for kinship navigator programs is critical to the sustainability of these programs, particularly in rural states where access to services and supports may be limited. Literature supports the value of these programs for improving caregiver and child outcomes of families involved in kinship care, including child permanency, adult well-being, and access to services (Forehand et al., 2024; Fowler et al., 2023; Littlewood et al., 2020, 2021; Preston, 2021a; Schmidt & Treinen, 2021; Wheeler et al., 2020). By exploring the delivery and outcomes for rural states serving rural caregivers, we can further understand best practices to promote these outcomes for all. To date, there are a total of six unique kinship navigator programs with limited exploration of rural or remote families and service provision that have received a favorable rating from the Title IV-E Prevention Services Clearinghouse, the body developed in accordance with the FFPSA. This Wyoming/Montana Kinship Navigator Program model of distance delivery reaching across two frontier/rural states potentially reduces delivery burden to comparatively high-density kinship caregiver families with individualized, solutions-focused navigation. The model increases the long-term stability of both programs by standardizing core components, providing a clear program template for staff training, and ensuring equitable care for all Kinship caregivers across both states. If our study’s findings indicate enhanced-case management, underlying the Wyoming and Montana Kinship Navigator Program with enhanced-case management is more effective than a minimal support condition (i.e., Information & Referral and materials packets provided to caregivers), it could indicate that this program improves important outcomes for families in kinship care.
The development and methods of the Wyoming/Montana Kinship Navigator model are designed to optimally receive a rating of “supported.” Through combining data collection efforts and ensuring parallel programming, even across unique navigator providing organizations, we provide proof of concept and a training manual for specifically how other rural-located or rural-serving organizations can replicate these services to meet their kinship caregiver and youth needs. The enhanced-case management services can be offered at a distance and at intermittent timeframes to not overburden clients, but also allow for individualized goals, peer-connection and education, and connection to local specific resources to further meet their unique situations. The evaluation is largely integrated into the program delivery, providing an opportunity for fidelity to delivery and quality assurance to more deeply address the needs of kinship families at the time-of-service provision. By bridging the distance rural families face to understanding and accessing services and resources available to them, kinship families may ultimately improve caregiver well-being, family stability, and healthier children. Ultimately, this model increases the long-term stability of both programs by standardizing core components, providing a clear program template for staff training, and ensuring equitable care for all Kinship caregivers across both states.
In addition to providing evidence of the effectiveness of the Wyoming/Montana Kinship Navigator Program on measures of services access, caregiver well-being, and child permanency, this study may allow for the identification of individuals who are more likely to benefit from enhanced case management, compared with minimal support and vice-versa. Evidence may also be presented that suggests the relationship between individual characteristics and service use, child permanency, and caregiver well-being. Finally, this study will provide qualitative evidence regarding what is useful and what can be modified to improve satisfaction with both enhanced case management and minimal support strategies to support caregivers.
Limitations
Despite the potential impact, there are several limitations to our study. Although our design (e.g., quasi-experimental) is acceptable to the Title IV-E Prevention Services Clearinghouse (Wilson et al., 2024), it is not as strong as a fully randomized design where assignment to treatment condition occurs by chance. Therefore, it is possible that intervention and comparison conditions will differ on important variables of influence (e.g., socioeconomic status (SES)). Although PSM will help to address identified group differences, it is possible that unmeasured confounds may remain, thereby influencing findings. We were able to include a 6-month post-closure assessment period and will be able to detect the stability of our findings over a 6-month interval following the conclusion of each type of treatment. We recognize, however, that information about the durability of treatment effects beyond 6 months will be lacking. Finally, despite the strategies employed to cast a wide recruitment net within intervention and comparison counties, we realize that there is a substantial proportion of the eligible population who may not respond to opportunities for support. Although there is greater generalizability due to the many community-based organizations engaged in recruitment efforts, the results of our findings may not extend to those who did not elect to respond or to those who did not seek assistance. Methods employed, however, were deemed suitable for real-world tests of kinship navigator programs and reflect one of the very first investigations of a rural kinship navigator program conducted by way of a two-state partnership.
Implications for Research and Practice
Findings from the evaluation of the Wyoming/Montana Kinship Navigator Program have the potential to advance the evidence-based practice of rural kinship navigation, where current literature and evidence to guide practice are limited. The currently approved programs have many similarities to this program, but research-supported does not always align with the community context. For example, some programs require in-person home visits to provide services. Although in-home visits may be ideal for relationship building, it is not feasible with the capacity or distance within rural implementing states. Where geographic isolation, limited provider availability, and sparse resources shape caregiver need and the experience of kinship care, a multi-state partnership can provide additional capacity support for program and staff development that may not otherwise be feasible. Similarly, this process highlights opportunities for expanding and creatively considering how different organizations with similar missions might partner to provide services to meet a target audience. Results from this evaluation can guide service providers in other rural states in the selection of navigation programs that align with their programming capacity to meet the needs of rural kinship caregivers.
Testing a standardized, two-state program that is tailored for rural contexts will provide a replicable model for other rural areas in the United States to consider when program evaluation criteria necessitate larger sample sizes. The partnership between community outreach and research institutions provided an opportunity to conduct rigorous evaluation without overburdening delivery partners. The partnership communication ensured that the evaluation was streamlined for participants by having data collection inform programming and vice versa. It also exposed undergraduate and graduate students as new professionals in counseling, family and consumer sciences, gerontology, community health and more to program development, delivery, and the role of evaluation to inform practice. The methods outlined in this protocol may provide guidance to researchers planning investigations of other programs in the strategies for conducting rigorous evaluation in low-population areas, such as multi-state, multi-partner collaborations and data pooling.
Conclusion
Joint program development, delivery, and evaluation strategies outlined here can converge to support the capacity of low-population-density areas to qualify for Prevention Services Clearinghouse review. These methods support the potential for sustainability of kinship navigator programs in rural contexts as well as provide a road map for other outreach, resource, and referral programs with similar capacity challenges. Through understanding both participant and funder stakeholder needs, and by leveraging a collaborative approach, the Wyoming/Montana Kinship Navigator Program aims to demonstrate effective and sustainable outcomes, thereby qualifying as an evidence-based program according to the Title IV-E Prevention Services Clearinghouse standards and meeting the needs of the Title IV-E Prevention Services Act.
Footnotes
Acknowledgements
We thank Drs. Angelique Day and John Fowler, University of Washington, for their guidance with the program design and evaluation methodology for this two-state collaborative evaluation study. We thank Chandra Ortiz, Peyton Vining and the kinship navigator staff for guidance in the preparation of this manuscript.
Disposition editor: Cristina Mogro-Wilson
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported through external funding from the Montana Department of Health and Human Services, contract number HHS-CFSD-00000365DPHHS. This is funding from Montana State General Funds, in part, for the evaluation of the program outlined in this manuscript. Additional evaluator time and effort were supported through the Kinship Navigator Program evaluation efforts with Kinship Connections of Wyoming, funded by the Wyoming Department of Family Services, grant number 2301WYPKIN.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.