
Abstract
This study examined how child disability status relates to attachment in adoptive families. Using cross-sectional survey data from 4,002 adoptive parents in the United States, we compared parent-reported attachment for children with and without identified disabilities. Using multiple regression analyses, the study investigated the association between child disability and attachment while controlling for child demographics and adoption-related factors. Across all disability categories, parents reported significantly lower attachment when their child had a disability. Older age at adoptive placement, adoptions from foster care or intercountry adoptions, and a prior relationship with the child were also associated with lower attachment, whereas receiving post-adoption services predicted stronger attachment. Findings underscore the importance of early, disability-informed adoption-competent supports to promote secure attachment.
Introduction
Adoption provides children with a family when their original parents are unable to care for them or choose not to be their parents. According to recent estimates, in a given year in the United States, close to 47,000 children join families through adoption from foster care, approximately 25,000 join families via private domestic adoption, and just over 1,000 children join families via international adoption (Children’s Bureau, 2025; Drumm et al., 2025). The literature consistently shows the centrality of permanency, which adoption offers, on child well-being. For example, children who transition from foster care or institutionalized care to an adoptive family report better developmental or adult outcomes compared to those who remain in non-permanent settings (Juffer & van IJzendoorn, 2007; Lindner & Hanlon, 2024). Similarly, nationally representative surveys of adoptive parents provide strong evidence on the benefits of permanency that most adopted children exhibit positive health, social, and educational outcomes, even among those with early adversities (Vandivere et al., 2009). These findings affirm that adoption can be a vital means for children to achieve positive well-being outcomes.
While adoptive families are typically a nurturing and healthy environment for children, they often experience challenges related to bonding and attachment (van den Dries et al., 2009). Attachment theory posits that children form bonds with their primary caregivers (usually their parents) based on early childhood experiences, as well as other developmental and environmental factors (Ainsworth et al., 1971; Bowlby, 1988). For adoptive families, these factors can be complicated due to children’s histories of loss, experiences of abuse or neglect, institutionalization, or the experience of having multiple, unpredictable caregivers (Escobar et al., 2014; Turner et al., 2019). A child’s disability can further present challenges in forming attachment between the child and parents (Alexander et al., 2024; Tesson et al., 2022). Therefore, assessing the level of attachment an adoptee with a disability forms with their adoptive parents is an essential component of adoption practice and post-adoption support, allowing practitioners to understand how they can meet this critical need for the children and families they work with.
Adopted Children With Special Needs
A disability is defined as a condition that prevents individuals from fully performing certain activities or engaging in their communities or environments (Centers for Disease Control and Prevention [CDC], 2025). Disabilities thus include physical, sensory, intellectual, developmental, and mental/psychiatric conditions that limit individuals’ activity and interaction (CDC, 2025). When an adopted child has a disability or condition, they are considered to have special needs and thus may be eligible for financial subsidies, depending on the type of adoption and other eligibility criteria. (Child Welfare Information Gateway [CWIG], 2023). In the field of adoption, there is no universal definition of “special needs.” States operationalize this term differently within the federal framework outlined in Title IV-E of the Social Security Act (2025), which requires a determination that the child cannot safely return home, and that it will be difficult to place the child without additional support due to factors such as age, ethnicity, sibling status, and/or medical condition. However, this only applies to domestic adoptions, primarily those from the public child welfare system (CWIG, 2023; Social Security Act, 2025).
Currently, an accurate estimate of adopted children with special health care needs or disabilities appears to be unavailable, even though existing literature indicates that a significant proportion of adoptions involve children with special health care needs or disabilities. For example, Vandivere et al.’s (2009) study estimated that 39% of adopted children had special health care needs, while the comparable percentage was 19% for the general child population. For intercountry adoptions, while the overall numbers of adoptions are decreasing, the percentage of adoptees with an identified medical special need has increased, with more than half being children with disabilities since 2014 (Hanlon & Quade, 2022).
Children with disabilities are more likely to experience adjustment issues after adoption (Hill & Moore, 2015; Raby & Dozier, 2019). Research shows that the risk of adoption failure is higher for children with disabilities, particularly for those with emotional and behavioral difficulties, with adoptive parents experiencing significant emotional, financial, and parenting challenges (Good, 2016). However, families who have adopted children with special health care needs generally perceive their adoption experience as positive (Glidden, 2000; Haugaard et al., 2000; McKlindon et al., 2011) even though they may experience difficulty in the parent–child relationship (McKlindon et al., 2011). This is particularly true when adoptive families are well informed of children’s condition in advance (Mozzi & Nuernberg, 2016).
While prior literature has documented the positives and challenges experienced by adoptive families of children with disabilities, there is still little known about their strengths, needs, and challenges. Furthermore, these families are often left without support and hit extra roadblocks when trying to get services (Haugaard et al., 2000; Hill & Moore, 2015). They also report that available post-adoption services are too limited, and that these services need to be more flexible, responsive, and ongoing (Haugaard et al., 2000; Hill & Moore, 2015). In particular, many adoptive parents want to have practical services for their child’s school, community life, health needs, and behavior (Hill & Moore, 2015), which connect directly to how attachment unfolds after adoption.
Parent–Child Attachment in Adoptive Families
Attachment theory provides a helpful framework for understanding the relationships formed through adoption. Attachment relationships have been studied by social scientists, demonstrating that adoptive families can form secure attachments despite a lack of genetic relationship and past adverse experiences, allowing for a deeper understanding of attachment relationships over time (Raby & Dozier, 2019; van den Dries et al., 2009). Most adopted children form healthy attachments over time, but the amount of time varies depending on their prior adverse experiences (Carlson, 2014; Raby & Dozier, 2019; van den Dries et al., 2009). In addition, a child’s age at adoption has a significant influence on their attachment relationship with adoptive parents. While children adopted under 12 months exhibit comparable attachment relationships, those adopted at an older age are less securely attached, compared to their non-adopted peers (van den Dries et al., 2009). While adopted children overall develop secure attachments with their adoptive parents over time, they may continue to show disorganized attachment patterns where they have inconsistent or conflicting behaviors in stressful situations (Carlson et al., 2014; van den Dries et al., 2009). This illustrates the longer-term effect of early childhood adversity (Dozier & Rutter, 2008).
Given the dynamic and plastic nature of attachment processes (Bowlby, 1988), there have been efforts to develop and deliver attachment-based interventions for adoptive families. Prior studies found that these interventions were effective in increasing positive parenting behaviors and children’s psychosocial adjustment in adoptive families. However, their impact on children’s attachment security and patterns was not conclusive (Dalgaard et al., 2022; Harris-Waller et al., 2018; Ní Chobhthaigh & Duffy, 2019; O’Dell et al., 2015), which may suggest the complexity of attachment processes that require long-term, persistent efforts. Furthermore, there are very few, if any, prior studies that investigated the effectiveness of attachment-based interventions for adoptive families of children with disabilities. The limited existing literature on interventions for adopted children with disabilities and their adoptive parents mainly focused on child behavioral health and functioning, and parenting stress as primary outcomes (Purrington et al., 2025; Zarnegar et al., 2016).
Similarly, current literature on child–parent attachment for adoptive families of children with disabilities is sparse. At the same time, there is evidence that children’s disabilities or special needs may increase the risks of insecure or disorganized attachment (Alexander et al., 2024; Howe, 2006). Limited literature reports mixed findings on the relationship between child disabilities and parent–child relationships. Some studies (Hill & Moore, 2015; Tan et al., 2015) reported that adoptive families of children with special needs or disabilities experience lower quality parent–child relationships, while other studies (Howe, 2006; Reilly & Platz, 2003) found no significant effect of children’s special needs or disability on parent–child relationships. Furthermore, the types of disabilities appear to influence adoptive families’ experiences. Families who adopt children with developmental or intellectual disabilities often report good satisfaction and steady adjustment. On the contrary, many adoptive parents of children with emotional or behavioral challenges report that they felt less prepared and less attached to their children (Egbert & Lamont, 2004; Hill & Moore, 2015).
Despite the growing proportion of adoptions that involve special needs (Hanlon & Quade, 2022), there is limited scholarship regarding how disability status influences the parent–child attachment relationship within the context of adoptive families. This study seeks to address that gap by examining the relationship between disability status and attachment, while also considering the adopted child’s demography and other adoption-related factors such as child age and gender, adoption type, prior adoption history, and receipt of post-adoption support.
Method
Study Sample and Data Collection Methods
The study used data that the National Council for Adoption (NCFA) collected for their Profiles in Adoption surveys of adoptive parents, adoptees, and birth parents (Hanlon & Quade, 2022), and this study specifically used the survey data collected from adoptive parents in August 2021. NCFA invited adoptive parents to participate in an online survey, sharing and posting the link to the survey questionnaire via email, listserv invitations, and social media. They also asked their stakeholders and other contacts in the adoption community to share the study information with adoptive parents. Both adoptive parents from the same family were allowed to participate in the survey, and they were asked to retrospectively reflect on their experience and adopted children’s from their perspectives. When respondents had multiple adopted children, they were asked to respond by focusing on the most recent adoption for certain questions. This study focused on information relating to adopted children’s disabilities and attachment. Among those who had completed the survey and wished to enter a raffle for a gift card, 150 were randomly selected and offered a $25 Amazon gift card as a token of appreciation for their time and input.
Using this non-probability sampling method, a total of 4,212 adoptive parents were recruited and completed the online survey. Of the initial responses from these adoptive parents, 4,208 provided a valid response on the study’s dependent variable, attachment. An additional 133 cases were excluded from this study, as they involved adoption types other than private domestic, intercountry, or foster care adoptions (n = 108) or lacked information on child gender (n = 25). The study further excluded 73 cases that were responses from the second parent of an adoptive family, ensuring that the same child was counted only once. This resulted in a final sample size of 4,002 cases. The study was approved by the Institutional Review Board of The Catholic University of America.
Variables and Measures
The independent variable of the study is the adopted child’s disability, and the study investigated its association with the child’s attachment. The study also included control variables in its analytic model. They were child age and gender; the match between child and adoptive parents’ race, types of adoption, child’s relationship to adopted parents before adoption, history of prior adoption, number of children at home, and receipt of post-adoption services.
Attachment
The questionnaire used items from the Attachment and Bonding Observation Checklists (Fahlberg, 2012) to measure the child’s attachment to adoptive parents. The Checklists were originally developed to support professionals in assessing a child’s attachment and bonding with primary caregivers, and it has four versions tailored for different age groups of children (birth to 1 year, 1–5 years, grade school years, and adolescents). The questionnaire selected and used 10 items from three versions (birth to 1 year, 1–5 years, and grade school years). A version corresponding to the adopted child’s age at the time they were placed in adoptive homes was displayed for each respondent, and responding adoptive parents were asked to mark their answer, reflecting on the first 6 months after the child’s adoption. The mean score of adoptive parents’ responses on the 10 items was calculated and used in the study. Cronbach’s alpha was .91 for the items on infants (birth to 1 year) and children aged 1 to 5 years, and .89 for the items on grade-school-age children in this study.
Child Disability
Within the context of adoption, special needs are often defined broadly as a factor or condition that may make it challenging to find an adoptive family for a child. It thus includes not only a child’s disability but also other characteristics such as age, racial/ethnic background, and risks of a disability (CWIG, 2010; Social Security Act, 2025). In the original survey used for this study, special needs referred to a child’s diagnosed disability or other special health care needs that could affect the child’s functioning. This includes physical and developmental disabilities/conditions, and other health conditions. Specifically, the survey presented 13 conditions with an Other option for a question on a child’s special needs, and respondents were allowed to select multiple conditions. In this study, we grouped 14 options into four categories, in consultation with an expert, so that the analytic model did not have too many variables: (a) general medical conditions, (b) hearing and vision impairment, (c) neurodevelopmental conditions, and (d) other special conditions. General medical conditions included blood conditions, congenital heart conditions, infectious disease, craniofacial special needs, orthopedic conditions, urogenital conditions, and chromosome disorder. Two conditions, hearing impairment and visual impairment, were put into the category of hearing and vision impairment. Neurodevelopmental conditions included autism spectrum disorder, cognitive impairment, neurological conditions, and in utero substance exposure. An Other option was renamed as other special conditions. Four separate variables were created for each group of conditions, and a value of “1” was assigned if a child was identified to have any of the conditions listed within the group. If respondents did not report any conditions for a child, a value of “0” was assigned.
Control Variables
Respondents were asked to report their adopted child’s chronological age at the time the child was placed in their family, as well as the child’s gender. Three response options were provided for child gender, including male, female, and prefer not to answer. As noted previously, cases with no information on child gender, including those marked with the prefer not to answer option, were excluded from the final sample due to their low frequency (n = 25). The survey asked whether the child’s race was the same as that of the adoptive parents. If the child and adoptive parents were of the same race, it was coded as “1.” If they are of different races, it was coded as “0.”
The questionnaire included an item inquiring about the types of adoption, with five options provided: private domestic, intercountry, adoption from foster care, embryo, and other. The study only included private domestic, intercountry, and foster care adoptions, and private domestic adoption was used as the reference group. Respondents were asked whether they were the child’s relatives by blood and marriage and whether the child had a history of prior adoption. Both items had response options of Yes (coded as “1”) and No (coded as “0”).
Additional items considered for this study included the number of children at home at the time of adoption and receipt of post-adoption services. The number of children was measured as a continuous variable, and adoptive parents were asked to report the number of children in their response. For the receipt of post-adoption services, respondents were asked whether they were able to receive the supportive post-adoption services they needed. It had three response options: Yes, No, and Not Applicable. Those who had marked Yes served as the reference group.
Data Analytic Methods
Descriptive statistics were used to illustrate the characteristics of adopted children. The study performed bivariate analyses, including t-test, correlational analysis, and Welch’s analysis of variance (ANOVA) test, to investigate the association between the dependent variable and the independent and control variables. The primary analytical methods employed in the study were hierarchical regression analyses, which were conducted using three models. The first model (Model I) only included child disability as a predictor and examined its association with a child’s attachment to adoptive parents. Child demographic variables (i.e., child age and gender and the match between child and adoptive parents’ race) were added to the second model (Model II) to investigate whether the effect of child disability, if any, would hold. The last model (Model III) included adoption-related variables, such as types of adoption, history of prior adoption, child’s prior relation to adoptive parents, number of children at home, and receipt of post-adoption services, and examined whether the association between child disability and attachment would change. An additional analysis was conducted where the number of conditions, rather than the presence/absence of given conditions, was used for child disability variables. The results showed a significant association between the number of conditions and attachment scores, where lower attachment scores were reported for children with more conditions. Since the results of the overall model were similar between the two analyses, we only reported the findings of the analytic model where each category of disability had dichotomous response options.
Results
Characteristics of Adopted Children
Table 1 presents study findings on adopted children’s demography. The mean age of adopted children in this study was 2.0 years (SD = 3.35), ranging from 0 to 18 years. Adopted children’s gender was evenly distributed between males and females (50.5% vs. 49.5%). Close to 60% of children (56.7%) were identified to be of the same race as their adoptive parents. In the study, approximately half of the children (n = 2,019, 50.4%) were reported to have one or more disabilities or conditions. Neurodevelopmental conditions were most frequently reported (32.5%), followed by general medical conditions (16.0%). Among neurodevelopmental conditions, in utero substance exposure was the most prevalent (n = 888, 22.2%), while cognitive impairment was the second most common (n = 339, 8.5%).
Adoptive Child Demography (N = 4,002).
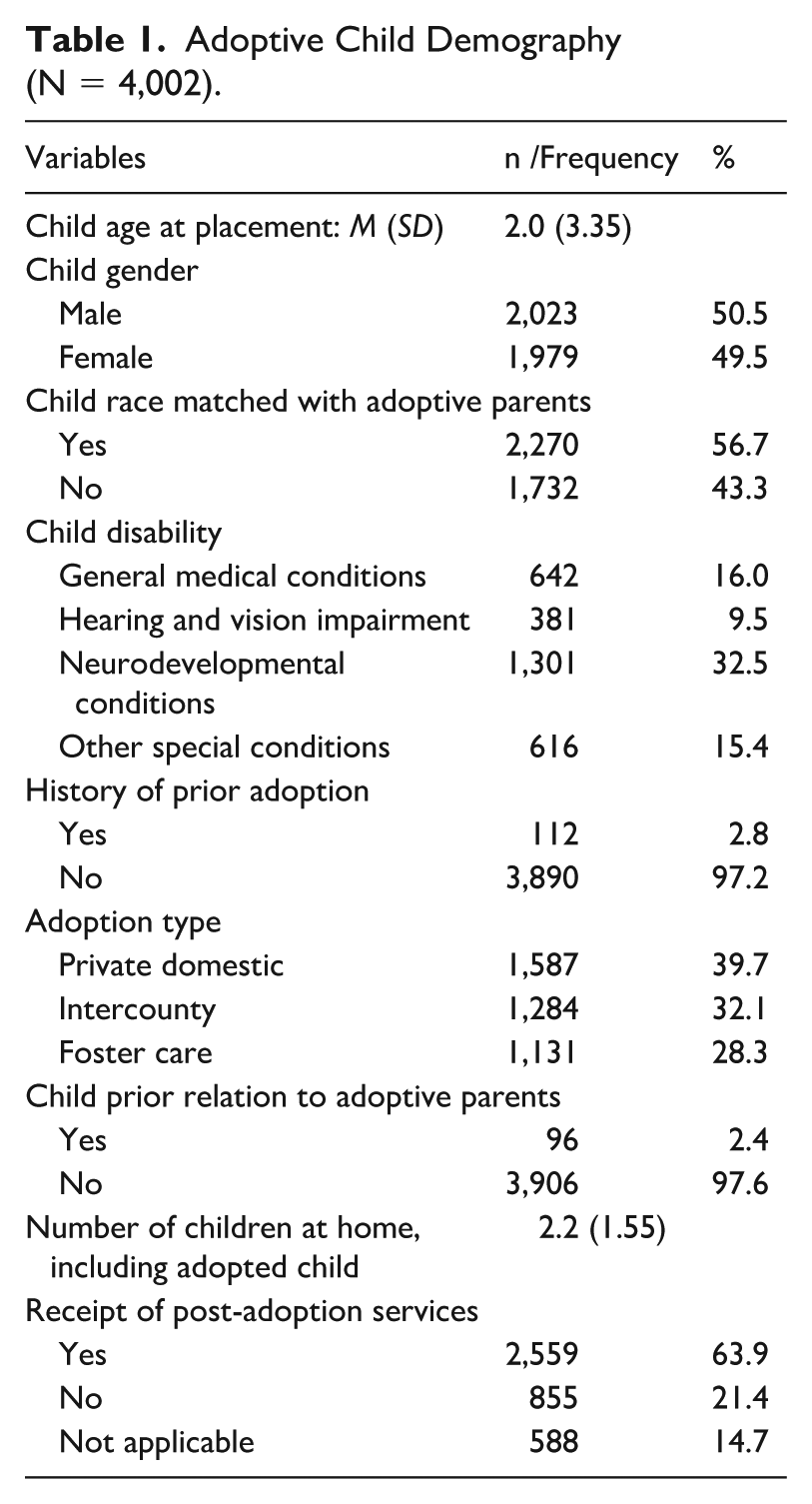
Most adopted children did not have a prior history of adoption (97.2%) and did not have a relationship with their adopted parents before adoption (97.6%). All three types of adoption (i.e., private domestic, intercountry, and foster care adoption) were well represented in the study, with private domestic adoption being the largest group (39.7%). Adoptive families had about two children (SD = 1.55) on average at home, including adopted children, and the number of children at home ranged from 1 to 10. Over 60% of respondents (63.9%) reported that they had received post-adoption services they had needed for their adopted children.
Results of Bivariate Analyses
The results of bivariate analyses showed a significant association between the child’s disability and attachment scores (Table 2). Regardless of disability types, significantly lower attachment scores were reported for children with disabilities than those without disabilities. For example, the mean attachment score was 3.9 (SD = .98) for children with neurodevelopmental conditions, while it was 4.3 (SD = .76) for those without such conditions (p < .001).
Bivariate Analysis on Child Attachment to Adoptive Parents.
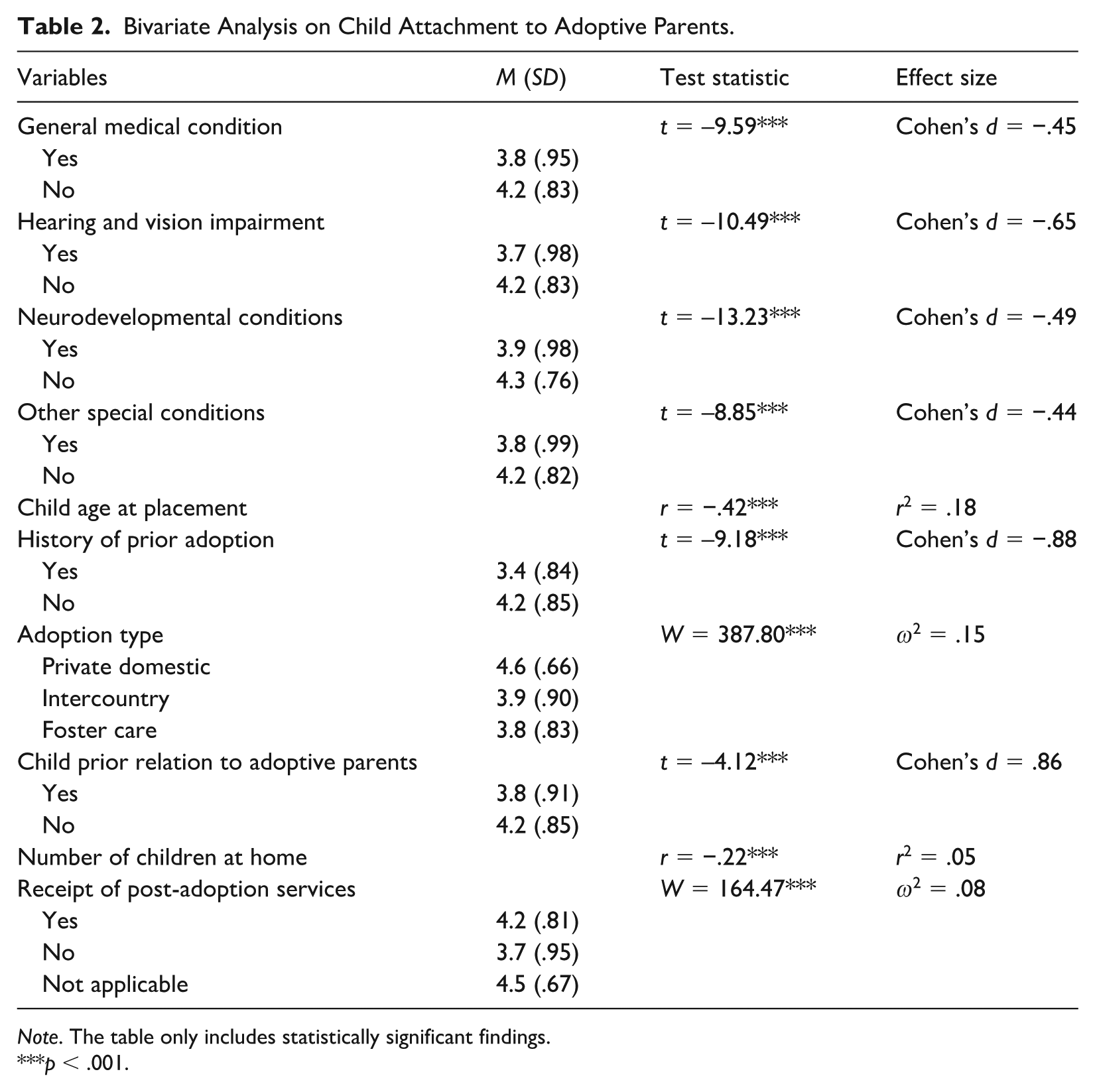
Note. The table only includes statistically significant findings.
p < .001.
In addition to child disability, most control variables were found to have a significant relationship with attachment scores (Table 2). For example, significantly higher attachment scores were reported for children who were adopted at a younger age, as well as for those who had no history of prior adoption, compared with those who were adopted at an older age and who had experienced prior adoptions (p < .001 for both). Adoption type, a child’s prior relation to adoptive parents, number of children at home, and receipt of post-adoption services were also significantly associated with attachment scores. For example, Games-Howell post hoc test shows that significantly higher attachment scores were reported for children adopted through private domestic adoption compared with those through intercountry and foster care adoption (p < .001). The difference between children adopted through intercountry and foster care adoption was also statistically significant (p < .01). The results of another Games-Howell post hoc test report that attachment scores were significantly higher for children who did not need post-adoption services compared to those who did or did not receive post-adoption services (p < .001 for both). Among those who would need post-adoption services, children who had received such services had significantly higher attachment scores than those who had not (p < .001). It is notable that children who had a prior relationship with adoptive parents reported significantly lower attachment scores than those who did not (p < .001).
The only control variables that were not significantly associated with attachment scores were child gender (t(4,000) = 1.04, p = .30) and the match between child and adoptive parents’ race (t(4,000) = −.65, p = .52). For example, the mean attachment scores were 4.1 (SD = .84) for males and 4.2 (SD = .88) for females, and this difference was not statistically significant.
Results of Regression Analyses
Consistent with the findings of bivariate analyses, the results of regression analyses showed lower levels of attachment for children with disabilities (Table 3). This was true for all four types of disabilities. For example, in Model I, which only included child disabilities as a predictor, children with neurodevelopmental conditions were reported to experience lower levels of attachment with their adoptive parents compared to those without these conditions (B = −.32, p < .001). The significant effects of child disabilities held even after additional variables were added to the model (Models II and III).
Regression Analysis on Child Attachment to Adoptive Parents.
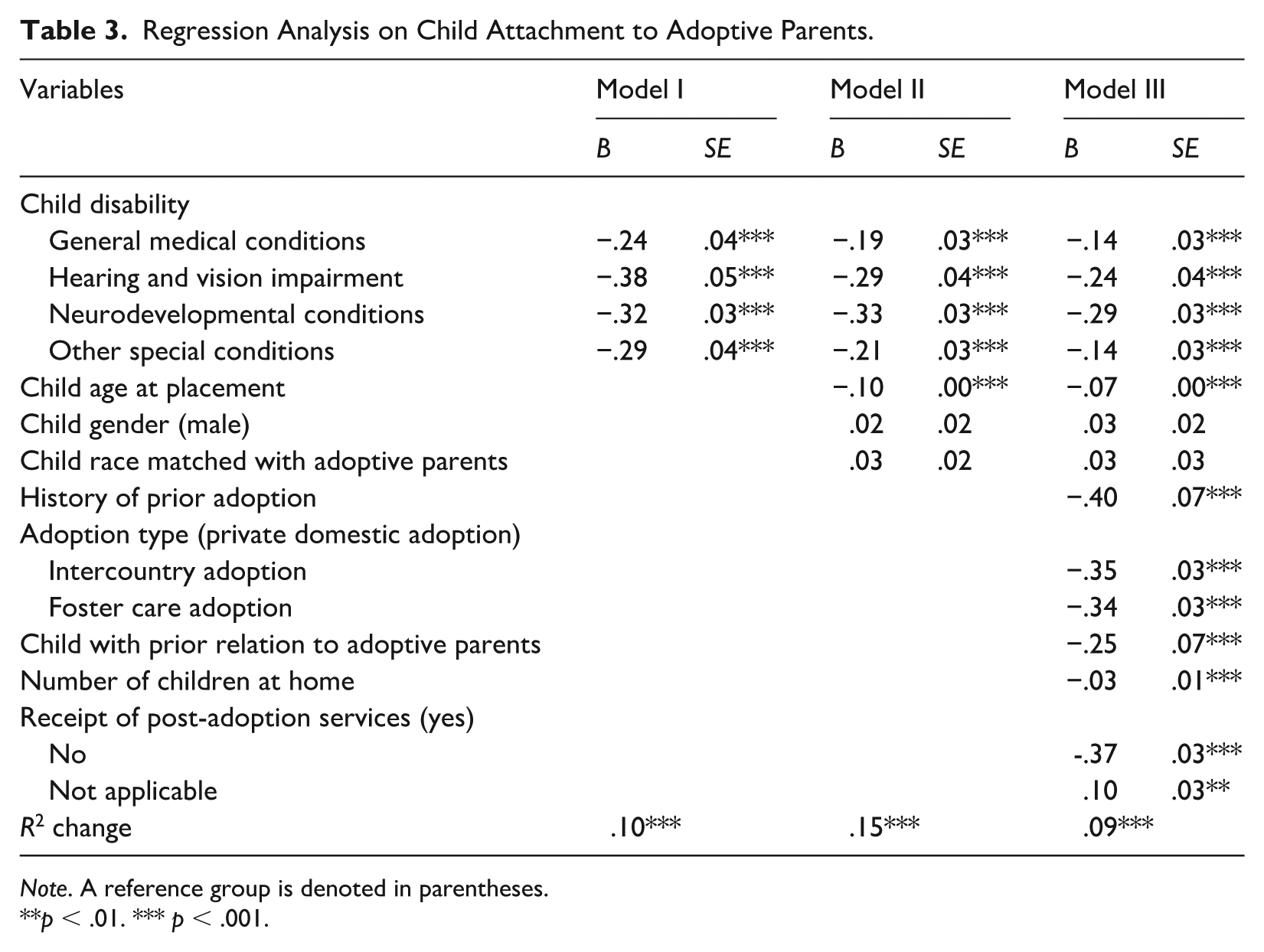
Note. A reference group is denoted in parentheses.
p < .01. *** p < .001.
While all three models reported a significant association between child disabilities and attachment, it was noted that additional variables in Models II and III significantly improved the models’ explanatory power. Four types of child disabilities explained 10% of the variance in attachment (p < .001, Model I). The addition of child demographic variables explained another 15% of the variance in attachment (p < .001, Model II). Similarly, the explanatory power of Model III got significantly larger as adoption-related variables were added (△R2 = .09, p < .001, Model III).
Specifically, child age at the time of placement was found to be a significant predictor for child attachment to adoptive parents. The results showed that children who were placed in their adoptive homes at a younger age were more likely to experience higher levels of attachment (B = −.10, p < .001, Model II). In contrast, child gender and match between child and adoptive parents’ race did not have a significant effect on the attachment variable (p = .43 and .18, respectively, Model II).
The variables added in Model III were all found to be significantly associated with child attachment to adoptive parents. For example, adoptive parents whose children had a prior history of adoption reported lower levels of attachment compared to those whose children did not (B = −.40, p < .001, Model III). Higher levels of attachment were reported for children who were adopted through private domestic adoption than those through intercountry and foster care adoption (p < .001, Model III). It was noted that lower levels of attachment were reported for children who had had a relationship with adoptive parents before adoption (B = −.25, p < .001, Model III).
Discussion
This study adds new, practice-relevant evidence about how disability status relates to attachment in adoptive households, while accounting for child demographics and other adoption-related factors. The study found that across all disability categories, adoptive parents reported lower attachment scores when their adopted child had an identified disability. This finding held even after controlling for selected demographic and adoption-related factors. The attachment scores were very similar for children with and without disabilities, regardless of disability types.
In addition to a child’s disability, the study findings show a significant association between a few demographic and adoption-related factors and attachment. It is clear that age matters where the study reported its inverse relationship to attachment (i.e., younger age at the time of adoption is associated with higher attachment scores). The number of children in the home was significantly and inversely associated with attachment, suggesting that family composition is an important consideration, likely due to parental bandwidth for bonding and ensuring a child’s needs are met. Adoption types matter as well, with families formed through private domestic adoption forming higher attachment than other adoption types. Children who had a pre-adoption relationship with their adoptive parents showed lower attachment scores, even when other child and adoption factors were held constant; this counterintuitive finding is likely due to complex pre-adoption dynamics and warrants further research. Finally, a history of a prior adoption was linked to lower attachment.
Taken together, it is clear that child-level needs and the child’s environment/context shape attachment in the post-adoption period. Post-adoption services also matter, as families who reported not needing services had the highest attachment scores; among those who perceived a need, receiving services was associated with higher levels of attachment than not receiving them. Interpreted together, post-adoption needs indicate a higher level of complexity, and access helps mitigate it — making a strong case for routine screening of attachment and easy-to-access pathways to evidence-based attachment-focused supports. It is noteworthy that neither gender differences nor children being of a different race from their adoptive parents showed statistically significant differences in attachment. These null findings suggest that modifiable factors (e.g., age at the time of adoption and post-adoption service access) are more salient for strengthening or harming attachment than immutable demographics.
These findings align with and extend the current literature reviewed. Prior syntheses show that adoption, on average, improves children’s relational security compared with remaining in non-permanent settings, especially for children placed for adoption at younger ages (Palacios et al., 2019; van den Dries et al., 2009). At the same time, adoptees as a group can show elevated risk for disorganized attachment when compared to the general population, with improvement but not full catch-up after their adoptive placement (Carlson et al., 2014; van IJzendoorn & Juffer, 2006). Prior literature also reports that children with disabilities experience difficulty in developing a secure attachment with their caregivers (Alexander et al., 2024). This study’s finding that disability is associated with lower attachment in adoptive families fits the broader picture that early adversity further complicates the pathway to secure attachment. It is possible that a parent’s focus on a child’s medically complex needs may detract from attention to bonding and relational connectedness (Alexander et al., 2024; Tesson et al., 2022). The findings of this study that the attachment scores were similar for children with disabilities regardless of disability types are somewhat inconsistent with prior literature.
The differences found by type of adoption also merit attention. Compared with private domestic adoption, families formed via intercountry adoption or foster care adoption reported lower attachment. This is likely due to circumstances and child and family characteristics that lead to different types of adoptions. Private domestic adoption is more likely to involve the adoption of infants or young children (Ishizawa & Kubo, 2013), and children adopted through international or foster care adoptions are more likely to experience pre-placement maltreatment, multiple caregivers, and other adversities before adoption (Vandivere et al., 2009).
Implications for Practice, Policy, and Future Research
Practitioners can utilize this knowledge to set more effective expectations for prospective adoptive parents regarding their role in promoting healthy attachment from the outset of the adoptive placement. These findings support targeted post-adoption support strategies providing attachment-focused parental coaching and ongoing screening of the parent–child attachment dyad, especially for families of children with disabilities. Access to robust post-adoption support is often dependent on policymakers recognizing the importance of these resources and ensuring they are available to families after an adoption. Systems should fund attachment-focused support as a preventive measure to avoid larger and more intensive interventions in the future.
Because certain demographic characteristics (i.e., child gender and racial match) were not associated with attachment, resource allocation should prioritize clinical complexity and service need rather than fixed traits. Child welfare service providers can implement post-adoption support plans to track attachment scores and, when warranted, to provide attachment-focused interventions where they are most needed. Beyond individual case planning, practitioners should prioritize the routine linkage of adoptive families to adoption-competent, attachment-focused mental health supports early in the placement, or even pre-placement. Practitioners can normalize help-seeking, screen periodically for attachment-related issues, and build referral networks to help their clients continue receiving support from specialized professionals.
Younger age at placement is consistently associated with stronger early attachment, so time-to-placement should be treated as a core quality metric by child welfare providers and policymakers. Currently, there is considerable variation among states regarding timelines for children to achieve permanency (Font, 2023). Future research can draw comparisons of attachment outcomes for children in different state systems based on their time outside a permanent family. The U.S. Department of State’s (2025) annual reports to Congress indicate that intercountry adoption process timelines have dramatically increased in recent years, which may warrant policymakers and practitioners to find faster pathways for children to leave residential/orphanage care and join permanent families.
Future researchers are encouraged to follow families longitudinally beyond 6 months and could incorporate multiple measures of attachment, beyond just parental reporting. There are likely mediating factors that impact attachment, especially regarding parenting styles and access to post-adoption supports/services. Research utilizing these variables may help tease out more specific action steps for new adoptive parents. Furthermore, the study found that attachment scores were similar regardless of child disability types, which was somewhat different from prior studies where adoptive families of children with emotional and behavioral challenges might experience more difficulty in parent–child relationship compared to families that have children with developmental of intellectual disabilities (Egbert & Lamont, 2004; Hill & Moore, 2015). Future studies should further explore the diversity of adoptive families’ experiences, depending on the presence and types of a child’s disability.
Limitations
Several limitations should be considered alongside our findings. First, the data are parent-reported and thus do not represent those who were adopted. In addition, the data were collected via a non-probability sample recruited through adoption-related organizations; this method may result in an overrepresented sample of adoptive families who remain connected to their adoption agency or other adoption-related organizations. The generalizability of the study findings may be further limited as the families that adopted older children were underrepresented in the study.
Another limitation comes from the conceptualization and measurements of variables used in the study. Attachment was measured using an adapted checklist of items, focusing on the first six months after the adoptive placement. Parental reporting was done retrospectively and may have lacked accuracy. In addition, the study conceptualized special needs as a child’s disability or other special health care needs that could affect the child’s functioning. Different findings may be produced if disabilities or special needs were to be conceptualized and categorized differently. Furthermore, the study did not consider the diversity within each type of adoption. For example, it did not distinguish kinship and non-kinship placements within foster care adoption: while the study included a child’s prior relation to adoptive parents as a covariate, it would not fully capture the differences between kinship and non-kinship placements within the context of foster care adoption.
It should also be acknowledged that the study would have had different results if its analytic models had included additional variables. For example, information on birth order or sibling position within the adoptive family was not available and was thus not included in the study. Given its association with family dynamics and attachment-related process (Salmon, 2003; Shanahan et al., 2007), its inclusion in the study might have led to different results. Furthermore, the use of a cross-sectional design limits the ability to make causal inferences. Future research could employ multi-informant or observational measures, along with longitudinal follow-up and quasi-experimental designs.
Conclusion
Adoption remains a critical pathway of intervention in the lives of children in need of a permanent family. While often resulting in positive well-being outcomes, this study highlights specific types of adoptions at higher risk for slower or less-healthy attachment: Children with identified special needs or disabilities, those placed at older ages, and those placed via intercountry adoption or for adoption from foster care. Practitioners informed of this can seek to increase support for adoptive families in these categories to promote secure attachment relationships.
Footnotes
Disposition editor: Cristina Mogro-Wilson
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.