
Abstract
Objective:
Dialectical Behavior Therapy (DBT) is regarded as a highly effective treatment for suicide, yet no study to date has examined how DBT can help suicidal individuals with co-occurring internalizing and externalizing symptoms. Our study aimed to investigate DBT outcomes in suicidal youth and young adults with varying levels of internalizing and externalizing symptoms and the potential effectiveness of a DBT partial hospital program (PHP) on this population.
Method:
Data come from 117 adolescents and young adults (Mage = 17.82; 66% cisgender female; 83% White) who participated in a short-term, intensive DBT PHP. Regression-based moderation analyses with simple slopes assessed associations between self-reported suicidality, internalizing and externalizing symptoms, and DBT PHP outcomes: mindfulness, emotion regulation, dysfunctional coping, interpersonal competence, and DBT skills use.
Results:
Suicidal youth with clinically significant externalizing behaviors had high levels of emotion dysregulation after four weeks of treatment; however, these patients improved across all DBT outcomes, having the greatest gains in interpersonal competence and DBT skills use. All patients demonstrated improvements across DBT target outcomes, regardless of symptom type and severity.
Conclusion:
Overall, findings support DBT as an effective transdiagnostic intervention. Clinicians should strive to prioritize and allocate particular clinical attention to emotion regulation skills for patients with acute externalizing presentations to foster more effective acquisition and generalization of emotion regulation skills.
Suicide is the second leading cause of death in adolescents and emerging adults ages 13–24 (Centers for Disease Control and Prevention, 2023). Adolescents and young adults with internalizing (e.g., sadness, withdrawal, somatic) or externalizing (e.g., aggression, conduct problems) symptoms are more likely to attempt and die by suicide than individuals without these mental health symptoms (Soto‐Sanz et al., 2019). However, individuals with suicidal ideation (SI) and externalizing behaviors are more likely to attempt suicide compared with individuals with SI and no externalizing symptoms, who may be more likely to contemplate suicide without making an attempt (Witte et al., 2018). The effectiveness of Dialectical Behavior Therapy (DBT; Linehan, 1993), the gold standard treatment for suicide, is often assessed in individuals with internalizing disorders (e.g., depression, anxiety) and symptoms (e.g., feelings of emptiness, thwarted belongingness, burdensomeness), which can be directly linked to suicidality. Less is known about the efficacy of DBT for suicidal individuals with externalizing behaviors (e.g., aggression, conduct problems).
Prior research suggests that DBT can effectively reduce symptoms among suicidal youth with internalizing and externalizing presentations, with some evidence indicating greater improvement among individuals with externalizing behaviors (Adrian et al., 2019). Adrian and colleagues (Adrian et al., 2019) examined predictors of DBT treatment response in suicidal youth with internalizing and externalizing symptoms and found that youth with more externalizing behaviors at the start of treatment improved more than other groups posttreatment. Although this study assessed DBT response, the authors did not measure improvements in key DBT outcomes (mindfulness, interpersonal effectiveness, emotion regulation, and distress tolerance), which is essential as youth with internalizing disorders (e.g., depression; Visted et al., 2018) or externalizing behaviors (Bornstein et al., 2010; Cai et al., 2021; Eisenberg et al., 2001) struggle in these areas. No study to date has explored how DBT treatment outcomes vary in patients with co-occurring suicidality and internalizing or externalizing symptoms, which is essential considering the overlapping but distinct association between suicide and internalizing and externalizing symptoms (Soto‐Sanz et al., 2019).
The current study examined whether internalizing and externalizing symptoms moderated DBT treatment outcomes in suicidal youth to better understand how a 20-day DBT partial hospital program (PHP) can benefit this population. We were particularly interested in patients with externalizing behaviors given the unclear overlap with suicidality and the limited research on DBT effectiveness for these youth. Our first aim sought to examine DBT outcomes (i.e., mindfulness, interpersonal competence, emotion dysregulation, dysfunctional coping, and DBT skills use) in youth with varying levels of suicidality and internalizing and externalizing symptoms. We predicted that suicidal patients with either internalizing or externalizing symptoms would show persistent difficulties in key DBT outcomes after four weeks of treatment, with worse outcomes for youth with externalizing behaviors, as individuals with elevated externalizing symptoms may engage in distinct behaviors (e.g., impulsivity, substance use; Witte et al., 2018) that can potentially hinder progress in a short-term program.
The second aim sought to evaluate whether DBT outcomes improved over time for suicidal youth after accounting for their overall internalizing and externalizing symptoms. We hypothesized that suicidal patients with externalizing symptoms would show greater improvement than those with internalizing symptoms due to youth with more externalizing behaviors demonstrating greater treatment improvement than their counterparts (Adrian et al., 2019), though both groups were expected to improve across key DBT outcomes.
Materials and Methods
Participants
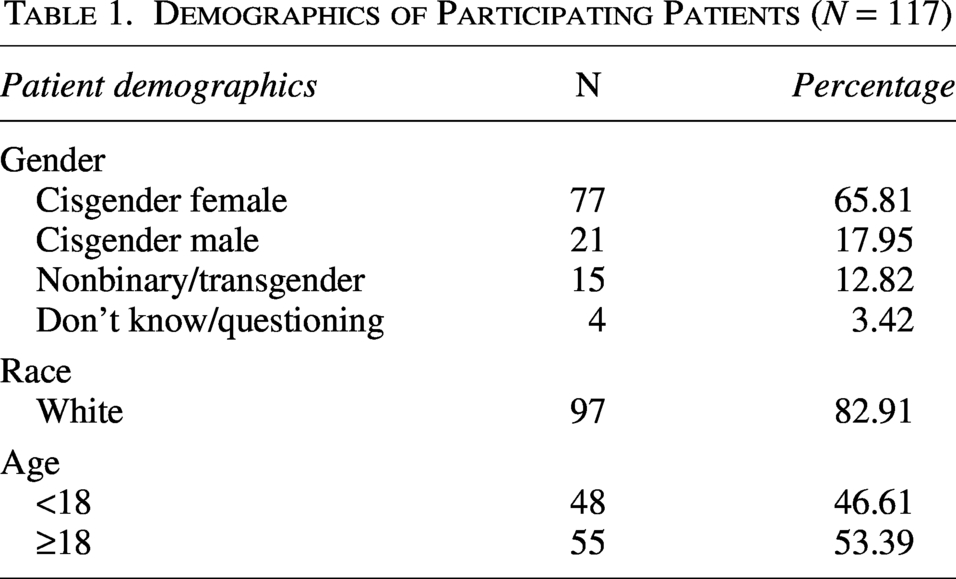
The sample included 117 adolescent and young adults (ages 13–24; M = 17.82; standard deviation = 2.42; 66% cisgender female; 83% White) who received DBT in a PHP from April 2022 to August 2024. Secondary data analyses assessed baseline self-reported suicidality, internalizing, and externalizing symptoms from a division-wide measurement-based care initiative, along with pre-post treatment outcomes. Additional demographics are provided in Table 1.
Demographics of Participating Patients (N = 117)
Treatment
This DBT PHP is housed in the adolescent and child division and admits both adolescents and transitional aged youth (ages 13–24). This adherent DBT program included the following four treatment components: individual therapy, group skills training, 24/7 on-call skills coaching, and the consultation team for therapists. The program ran from 8:30 am to 3:00 pm and included individual therapy twice a week, daily group therapy, weekly psychiatric consultation, and skills coaching available in person during program hours and by phone after hours. All participants, regardless of age, attended mandatory weekly family therapy with their primary caregivers. Caregivers had the option to attend a weekly parent skills group and utilize as-needed parent skills coaching.
Individual therapy was tailored to patients’ diary cards, which typically tracked target 1 (suicidal and self-harm) and target 3 (e.g., substance use, avoidance/isolation) urges and behaviors. The group therapy curriculum blended standard content and worksheets from the core DBT (i.e., mindfulness, interpersonal effectiveness, emotion regulation, and distress tolerance) and DBT-Adolescent (Rathus and Miller, 2002; i.e., Walking the Middle Path) modules. In addition, two Cognitive Behavioral Therapy/Exposure groups were offered. Group sessions were held hourly, and patients learned skills for mindfulness (e.g., fully being aware of internal and external experiences, staying present and non-judgmental), interpersonal effectiveness (e.g., building and maintaining relationships, setting limits), emotion regulation (e.g., accurately identifying and changing emotions, decreasing vulnerabilities to emotions), distress tolerance (e.g., tolerating unpleasant and intense emotions, minimizing suffering through acceptance), and Walking the Middle Path (e.g., dialectical thinking, dialectical dilemmas). Example worksheets and concepts included dialectical abstinence from the standard DBT module and Walking the Middle Path parent–child dialectical dilemmas from the DBT-A module.
Family sessions were conducted with the goal of improving patients’ home environment. Family therapy typically included psychoeducation on the biosocial model, parent–child dialectical dilemmas, behavioral reinforcement and management principles, and using double-chain and solution-focused analyses to assess and improve parent–child conflict. All patients were offered 24/7 phone coaching as a service, and phone coaching was guided by general behavioral reinforcement principles tailored to their developmental level (e.g., applying skills to request more independence for adolescents or to tolerate the home-to-college transition for young adults).
Procedure
Data come from a 4-week (20 clinical days) comprehensive DBT PHP (Tung et al., 2024) for adolescents and young adults (13–24) with emotion dysregulation and high-risk behaviors. Licensed staff clinicians screened participants for clinical appropriateness, motivation, and commitment to DBT. Participants were excluded from the DBT program if they were unwilling to remain safe (i.e., refusing to decrease self-harm or suicidal behaviors) throughout the duration of the program, had active psychosis, or a serious psychiatric disorder requiring medical monitoring (e.g., substance use, eating disorder). Despite these exclusions, the sample remained clinically acute, with 32.48% endorsing frequent suicidal thoughts in the three months prior to admission. Only participants who completed both routine admission and 4-week assessments (e.g., suicidality, internalizing, externalizing, DBT outcome measures) were included, and only first-time admission data were analyzed. Patients were also asked to complete a demographic questionnaire, which included questions about their sex, gender, sexual orientation, race, and age.
A certified Institutional Review Board (Tung et al., 2024) authorized the use of these data for research and program evaluation. The study was deemed exempt, and the requirement for informed consent was waived by the board. Despite the informed consent waiver, participants provided informed consent for participation in a study from which the present data were derived.
Measures
Mental health symptoms
Suicidal Thoughts and Behaviors
The Suicidal Behaviors Questionnaire (SBQ; Linehan, 1981) is a 23-item self-report measure assessing SI, suicide attempts, self-harm, and future suicide risk. Items are rated on 5-point (0–4) or 3-point (0–2) Likert scales, with higher scores indicating greater suicidality, and were recoded following Linehan’s instructions (0 = 0, 1 = 2, 2 = 4; Behavioral Research and Therapy Clinics, 2025). The SBQ demonstrated good overall test–retest reliability, internal consistency, and construct validity (current sample: α = 0.93; Pistorello et al., 2012).
Internalizing and Externalizing Symptoms
Internalizing (anxious/depressed, withdrawn/depressed, somatic complaints) and externalizing (rule-breaking, aggressive behavior) symptoms were captured using the Achenbach System of Empirically Based Assessments (ASEBA; Achenbach and Rescorla, 2014; Rescorla, 2004), including the youth (Youth Self-Report; YSR) and adult (Adult Self-Report; ASR). T-scores higher than 60 and 70 suggest “at-risk” and “clinically significant” challenges, respectively. The ASEBA is a widely used measure of adolescent and adult general psychological functioning with well-established reliability and internal consistency (Achenbach et al., 2017).
DBT outcomes
Mindfulness
The Five Facet Mindfulness Questionnaire (FFMQ; Baer et al., 2006) is a 39-item questionnaire used to capture self-reported awareness and ability to observe and describe emotions on a 5-point Likert scale with reverse-coded items so that higher scores captured more mindfulness. The FFMQ had strong internal consistency (current sample: α = 0.91) and external construct and criterion validity elsewhere (Christopher et al., 2012).
Interpersonal Competence
The Adolescent Interpersonal Competence (Buhrmester, 1990) contained 15 items assessing self-reported competence navigating self-disclosure, emotional support, conflict management, and assertion on a scale of 0 (“Very bad at this”) to 3 “(Very good at this”), with higher scores indicating stronger interpersonal competence. This measure is reliable (Chow et al., 2013) and has good internal consistency in the current sample (α = 0.84).
Emotion Dysregulation
The Difficulties in Emotion Regulation Scale (DERS; Gratz and Roemer, 2004) contained 36 items capturing self-reported emotion regulation difficulties on a 5-point Likert scale from 1 (“Almost never”) to 5 (“Almost always”), with higher scores indicating more difficulties regulating emotions. The DERS had strong internal consistency in the current sample (α = 0.95) and test–retest reliability (Gratz and Roemer, 2004).
Dysfunctional Coping and DBT Skills Use
The Dysfunctional Coping Subscale (DCS; 21 items) and DBT Skills Subscale (DSS; 38 items) of the Ways of Coping Checklist (WCCL; Neacsiu et al., 2010) assessed dysfunctional coping and DBT skills use, respectively. Items were rated on a 4-point Likert scale from 0 (“Never used”) to 3 (“Regularly used”), with higher scores indicating greater dysfunctional coping or DBT skills use. The DCS targets distress tolerance, a core DBT outcome. This measure is validated and reliable (Neacsiu et al., 2010) and demonstrated good internal consistency in the current sample (DCS: α = 0.87; DSS: α = 0.91).
Data analysis
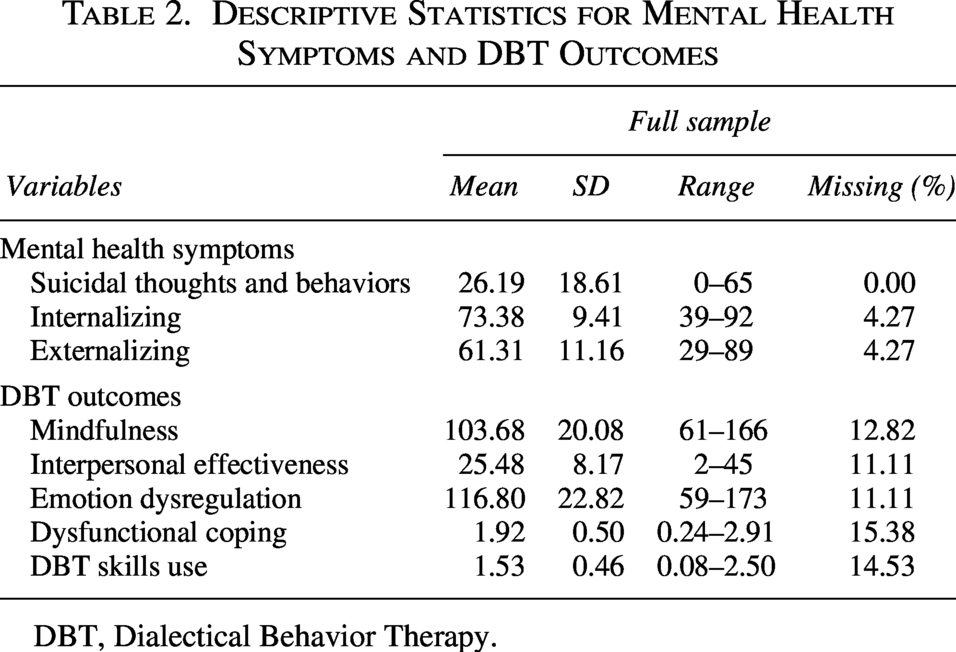
Descriptive statistics were tabulated for demographic information, suicidality, internalizing and externalizing symptoms, and DBT outcome variables (see Table 2). We addressed our primary research aims by using multiple regression in Mplus version 8 using robust full-information maximum likelihood estimation. As part of model estimation, we estimated the means of model predictors. This estimation approach accommodates assumptions associated with nonnormality and missing data. Nine percent of data were missing across predictor and outcome variables, and no variables had more than 16% missing data. According to Graham (Graham, 2009), one of the best predictors of an outcome is the same variable at another time point, which was included in each model (i.e., baseline DBT target outcomes).
Descriptive Statistics for Mental Health Symptoms and DBT Outcomes
DBT, Dialectical Behavior Therapy.
For our first aim, we had two models—one included suicidality and the ASEBA internalizing composite scale, and the other included suicidality and the ASEBA externalizing composite scale. The indicators (i.e., suicidality), moderators (i.e., internalizing and externalizing variables), and interaction terms were entered as predictor variables in both the internalizing and externalizing models. The continuous indicators and moderators were grand mean-centered. Interaction terms were created by multiplying each centered indicator variable with each centered moderator (e.g., Suicidality*Internalizing, Suicidality*Externalizing). In all models, we controlled for age and baseline DBT outcomes. Each DBT outcome was evaluated in separate models, resulting in 10 total models that examined internalizing and externalizing symptoms for each of the five outcomes.
To explore the statistically significant interaction effects, we estimated simple slopes. The interactions were probed by estimating the conditional effects of suicidality on outcomes at three levels of a priori importance on the ASEBA measures (t-scores of 50, 60, and 70, corresponding to normal, at-risk, and clinical levels of impairment, respectively). Given the a priori nature of these hypotheses, we report results based on unadjusted p-values. As a conservative approach that provides information about potential false positives, we also evaluated these moderation-based hypotheses after using the Benjamini-Hochberg procedure to control for the false discovery rate (FDR; Benjamini and Hochberg, 1995). We included all (30) simple slope estimates in our FDR analysis. For our second aim, we assessed changes in DBT outcomes over time by subtracting the model-estimated score (after four weeks of treatment—on the 20th clinical day) associated with specific covariate levels from the sample average at admission. We calculated effect sizes following recommendations by Morris and DeShon (Morris and DeShon, 2002).
Results
Aim 1: Main and interaction effects of mental health symptoms
In both internalizing and externalizing models, suicidality was positively associated with emotion dysregulation (internalizing: b = 3.00, p = 0.02; externalizing: b = 2.96, p = 0.02) and dysfunctional coping (internalizing: b = 0.06, p = 0.05; externalizing: b = 0.06, p = 0.02) after four weeks of treatment, but not with mindfulness or interpersonal effectiveness. Internalizing behaviors positively predicted DBT skills use (b = 0.01, p = 0.004). There were no other significant associations between internalizing or externalizing symptoms and mindfulness, interpersonal competence, emotion dysregulation, or dysfunctional coping. Age was not a significant predictor of mindfulness, interpersonal competence, emotion dysregulation, dysfunctional coping, or DBT skills use in either of the internalizing or externalizing models.
There was an interaction between suicidality and externalizing behaviors (see Fig. 1). The interactions were probed by testing the conditional effects of suicidality at three levels (t-scores of 50, 60, and 70, which correspond to normal, at-risk, and clinically elevated levels of symptoms, respectively) of internalizing and externalizing symptoms. For externalizing behaviors, the positive association between suicidality and emotion dysregulation was stronger for youth with at-risk (b = 2.69, p = 0.03) and clinically elevated (b = 4.73, p = 0.001) levels of externalizing behaviors. In addition, there was a positive association between suicidality and dysfunctional coping for youth with at-risk (b = 0.06, p = 0.02) and clinically elevated (b = 0.10, p = 0.01) levels of externalizing behaviors. And finally, suicidality negatively predicted mindfulness for youth with clinically elevated (b = −2.19, p = 0.05) externalizing symptoms. Of note, the overall omnibus interaction between suicidality and dysfunctional coping, as well as mindfulness, was not significant. This indicates that while our a priori hypothesized levels of interaction were statistically significant, when the interaction was assessed at several other levels of the moderator, no significant moderation was observed. Internalizing symptoms showed omnibus moderation of the link between suicidality and dysfunctional coping (b = 0.01, p = 0.04), but simple slope tests for all a priori points of interest were nonsignificant (t-scores of 50, 60, and 70). Additional details are denoted in Table 3. There were no other significant interactions for the mindfulness, interpersonal effectiveness, or DBT skills use outcomes for the internalizing or externalizing models. After adjusting the significance test of moderation-based hypotheses using FDR procedures, only the association between suicidality and emotion dysregulation for youth with clinically elevated externalizing behaviors remained significant.
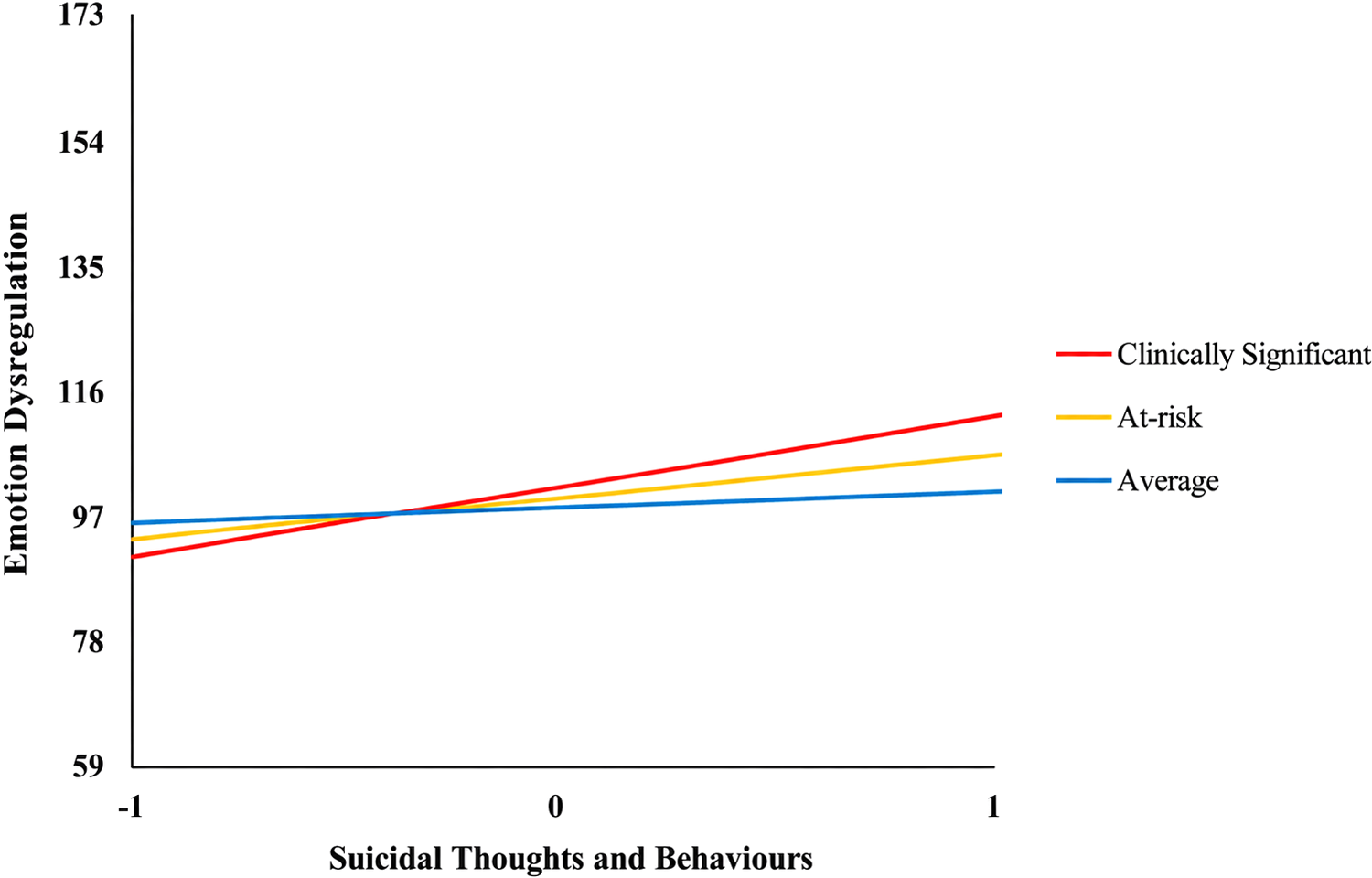
The Association between suicidality and emotion dysregulation by externalizing behaviors.
Main and Interaction Effects of Mental Health Symptoms on DBT Outcomes
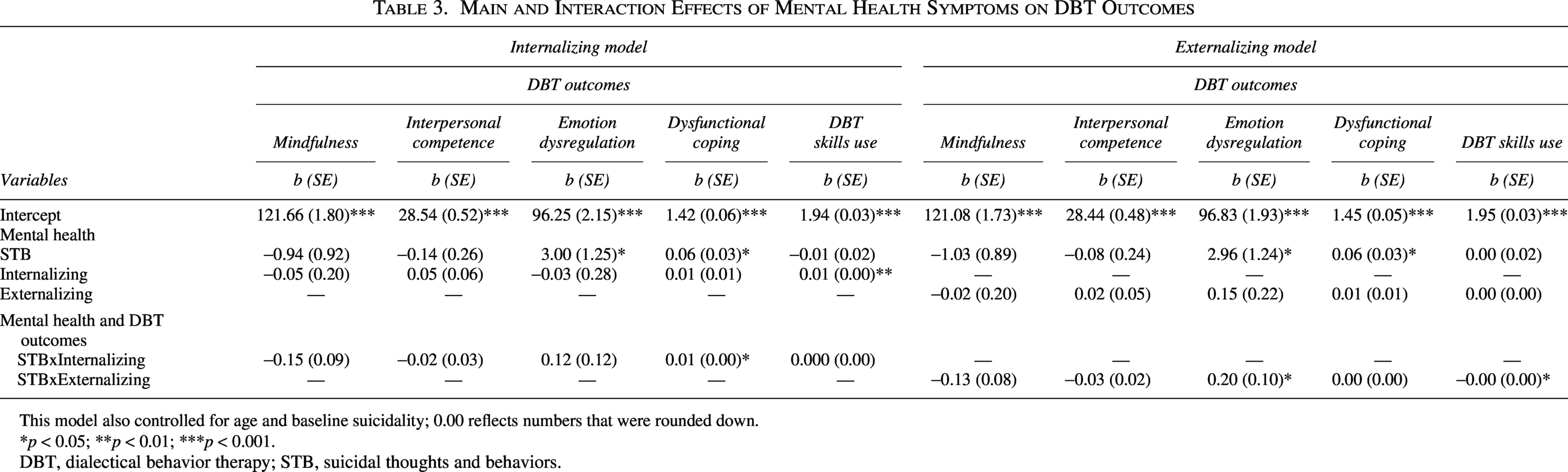
This model also controlled for age and baseline suicidality; 0.00 reflects numbers that were rounded down.
*p < 0.05; **p < 0.01; ***p < 0.001.
DBT, dialectical behavior therapy; STB, suicidal thoughts and behaviors.
Aim 2: DBT change scores as a function of pretreatment internalizing and externalizing symptoms
On average, at intake, patients reported having low-to-moderate suicidal thoughts and behaviors (M = 26.19; 0–65), clinically elevated internalizing symptoms (M = 73.38), and at-risk externalizing symptoms (M = 61.31). In terms of DBT outcomes, patients had elevated levels of emotion dysregulation (M = 116.80; 36–180), moderate to elevated levels of dysfunctional coping (M = 1.92; 0–3), moderate levels of interpersonal competence (M = 25.48; 2–45), and higher mindfulness (M = 103.68; 39–195) at admission. Additional descriptive statistics are in Table 2.
When comparing pre-post DBT outcomes for patients with varying levels of internalizing and externalizing symptoms, patients across all acuity levels (i.e., average, at-risk, clinically significant) demonstrated improvements in all DBT outcomes. Patients with average internalizing symptoms had the greatest improvement in dysfunctional coping (b = 0.63; d = 1.29) and mindfulness (b = −19.03; d = −0.95), and those with clinically significant internalizing symptoms had the greatest improvements in interpersonal effectiveness (b = −2.90; d = −0.35), emotion dysregulation (b = 20.43; d = 0.90), and DBT skills use (b = −0.38; d = −0.82). Patients with average externalizing symptoms had the greatest improvement in emotion dysregulation (b = 21.70; d = 0.95), dysfunctional coping (b = 0.53; d = 1.08), and mindfulness (b = −18.91; d = −0.94), whereas patients with clinically significant externalizing symptoms had the greatest improvements in interpersonal effectiveness (b = −3.09; d = −0.38) and DBT skills use (b = −0.44; d = −0.96).
Discussion
This is the first study to assess DBT outcomes in suicidal adolescents and young adults with comorbid internalizing and externalizing symptoms who are participating in a short-term, intensive, DBT PHP, which is further contextualized in Tung et al. (2024). We found several associations among suicidal youth with internalizing and externalizing symptoms; however, after post hoc correction, only suicidal youth with clinically significant externalizing behaviors had elevated emotion dysregulation after four weeks of treatment. Patients also improved across all DBT outcomes, regardless of their symptom severity.
Main effects of mental health symptoms
In both internalizing and externalizing models, suicidality was associated with higher emotion dysregulation and dysfunctional coping, suggesting suicidal youth may have continued emotion regulation and adaptive coping difficulties after four weeks of treatment. Researchers have found a positive and indirect link between suicidality and emotion regulation (Turton et al., 2021) and dysfunctional coping (Anestis et al., 2013). Our results demonstrate that patients higher in suicidality may continue having difficulties managing negative affect despite short-term treatment gains, suggesting they may benefit from ongoing therapy. Inconsistent with the literature, suicidality at admission was not associated with worse mindfulness, interpersonal competence, or DBT skills use after four weeks of treatment despite evidence linking higher suicidality to greater mindfulness difficulties (Aguiar et al., 2022), interpersonal challenges (e.g., thwarted belongingness, perceived burdensomeness; Chu et al., 2017), and lower skills use (Probst et al., 2018). This may suggest that suicidality alone may not sufficiently predict these DBT outcomes and that a combination of factors (e.g., experiential avoidance, thwarted belongingness and perceived burdensomeness, co-occurring symptoms) can better explain these associations.
Interestingly, internalizing symptoms at admission positively predicted DBT skills use after four weeks of treatment, such that patients with higher internalizing symptoms at admission were more likely to use DBT skills to cope after four weeks of treatment. Research has shown that patients with more acute mental health symptoms at admission have worse treatment outcomes (Nuernberg et al., 2016). However, this DBT PHP teaches skills that aim to directly target mood and affect, which may especially appeal to patients with internalizing symptoms who may have immediate mood changes, which incentivizes them to continue utilizing the skills. There were no other associations between internalizing or externalizing symptoms and DBT outcomes.
Interaction effects of mental health symptoms
Of note, the only interaction finding that was significant after post hoc correction was between suicidality and externalizing behaviors for youth with clinically significant symptoms. For this reason, we place the most emphasis on this finding, and we interpret the remaining findings with more caution.
Externalizing symptoms
Suicidality was associated with higher emotion dysregulation in patients with clinically significant externalizing behaviors, while a similar but nonsignificant pattern was observed in the at-risk group after post hoc correction. In line with the literature, this suggests that suicidal patients with more acute externalizing presentations had higher emotion dysregulation after four weeks of treatment (Clapham and Brausch, 2024). Suicidal youth with acute externalizing behaviors may remain dysregulated and struggle to replace habitual coping strategies (e.g., substance use) with DBT skills after a short-term program.
Although there was not an omnibus interaction between suicidality and externalizing behaviors when predicting dysfunctional coping and mindfulness, we found interactions at a priori hypothesized levels of externalizing symptoms. This pattern may reflect low statistical power and the small, subgroup-specific nature of real-world moderation effects, which can be difficult to detect across an entire sample. Suicidality was positively associated with dysfunctional coping for patients with at-risk and clinically significant levels of externalizing behaviors, meaning suicidal patients with more acute externalizing presentations had higher dysfunctional coping after four weeks of treatment. Dysfunctional coping has been linked with suicidality for individuals with externalizing behaviors (i.e., substance abuse; Anestis et al., 2013), such that individuals with suicidality (Kyron et al., 2022) and externalizing symptoms (Daughters et al., 2013) are less likely to cope with distress effectively. Patients who have more difficulty tolerating affective states may cope with distress through oppositionality, defiance, and conduct problems (e.g., delinquency and reward-seeking behaviors; Daughters et al., 2013). In addition, suicidal patients with more acute externalizing behaviors may also have difficulties with impulse control, especially when distressed (Meehan et al., 2013), which can make them less likely to use the adaptive coping skills that require impulse control and regulation.
Moreover, suicidality was negatively linked with mindfulness for youth with clinically significant externalizing symptoms, indicating that suicidal patients with more externalizing behaviors demonstrated decreases in mindfulness after four weeks of treatment. Youth with externalizing symptoms may have difficulty controlling their attention, potentially making it difficult for them to concentrate on the group content, stay on task, and control their behavioral responses (Samarghandi et al., 2019), especially when distressed (Meehan et al., 2013). Furthermore, patients with the most severe externalizing symptoms may continue having difficulty recognizing internal cues of distress, often done through mindfulness, which can be a potential barrier to applying new coping skills, such as those taught at the PHP.
Internalizing symptoms
The results suggest suicidality interacted with internalizing symptoms when predicting dysfunctional coping after four weeks of treatment but not at any of the identified points of interest of internalizing symptoms. These results may indicate that interactions between suicidality and internalizing symptoms occur at levels outside of the selected thresholds (t-scores of 50, 60, and 70). Dysfunctional coping is linked to suicidality in anxious youth, with anxiety uniquely predicting SI beyond coping, suggesting that higher levels of internalizing symptoms may be linked with greater suicidality and, potentially, more dysfunctional coping in individuals with anxiety (O’Neil Rodriguez and Kendall, 2014). This study also supports the idea that distress tolerance (which we measured via dysfunctional coping) underlies the internalizing construct (Eaton et al., 2011), suggesting a strong overlap between difficulties coping with distressing situations and internalizing symptoms. There were no other interactions for the other DBT outcomes, suggesting no differences in mindfulness, emotion regulation, interpersonal competence, or DBT skills use for suicidal patients with varying levels of internalizing symptoms. These nonsignificant findings indicate that there may be more meaningful predictors (e.g., emotion regulation) of these DBT outcomes (e.g., interpersonal competence; Baer et al., 2022) outside of comorbid internalizing symptoms or that the interaction between suicidality and internalizing symptoms may be a better predictor of future suicidality (Piqueras et al., 2019), which we did not assess.
DBT outcomes by mental health symptoms for suicidal youth
Expanding on our knowledge that this PHP improves DBT outcomes in adolescents and young adults (Tung et al., 2024), these results demonstrate that this PHP is also helpful in targeting all DBT outcomes for suicidal patients with varying levels of internalizing and externalizing presentations. When examining program outcomes, there was an increase in mindfulness, interpersonal competence, and DBT skills use and a decrease in emotion dysregulation and dysfunctional coping for suicidal patients with average, at-risk, and clinically significant internalizing and externalizing symptoms.
In particular, suicidal patients with average levels of internalizing or externalizing symptoms demonstrated the greatest improvements in dysfunctional coping and mindfulness, and suicidal patients with clinically significant internalizing or externalizing symptoms demonstrated the greatest improvements in interpersonal effectiveness and DBT skills use. Suicidal patients with fewer acute symptoms may have less difficulty learning and applying skills requiring focus (i.e., mindfulness) and help them tolerate intense negative affect (i.e., adaptive coping skills), as milder symptoms may allow for better cognitive functioning (Beaujean et al., 2013) that can help them focus and regulate. Whereas suicidal patients with more acute symptoms may benefit from more structured and skills-focused programs, as they may struggle with greater skills deficit (e.g., problem-solving; Xu et al., 2023) compared with groups with less severe symptoms. Furthermore, patients with clinically significant symptoms may especially benefit from content and skills focused on navigating interpersonal relationships (i.e., interpersonal effectiveness skills), an area that may be particularly relevant in adolescence and young adulthood. Interpersonal conflict may be especially beneficial for suicidal patients with acute symptoms to navigate effectively, as internalizing symptoms (e.g., social anxiety and depression) and externalizing behaviors (e.g., aggression, substance abuse) can place one at more risk and make one more sensitive and reactive to conflict (Johnson et al., 2013).
Finally, suicidal patients with average externalizing symptoms and clinically significant internalizing symptoms had the greatest improvements in emotion dysregulation. Patients with milder externalizing behaviors may apply emotion regulation skills more easily than those with acute symptoms, as evidenced by our interaction findings.
Limitations and future directions
While there are several strengths of this study, such as our unique sample and treatment setting, these aspects of the study also present limitations, as they qualify the generalizability of our results to a specific group of people and setting. For example, our sample was predominantly White and affluent, which may influence internalizing and externalizing presentations. Patients of higher socioeconomic status have unique stressors (e.g., parental pressures of perfectionism; Lyman and Luthar, 2014) that may influence their emotional and behavioral difficulties and the type of support and resources used to address their symptoms, which may contrast to those available to marginalized individuals. Future studies should examine how DBT outcomes vary by the observed internalizing and externalizing constructs for suicidal youth who identify as low-income and/or Black, Indigenous, and People Of Color. In addition, there were no specific inclusion or exclusion criteria to be enrolled in this study, as all patients admitted into the DBT PHP were eligible to participate. This said, external factors, such as motivation and commitment, could have potentially influenced their program outcomes. However, it is important to note that motivation and commitment to improving were a requirement for admission and to remain in the program. Furthermore, we did not have a distress tolerance measure, which is a DBT outcome, and instead utilized dysfunctional coping to represent an aspect of distress tolerance. We used the WCCL (Neacsiu et al., 2010), used by Marsha Linehan, to assess whether individuals resort to dysfunctional coping due to an inability to tolerate distress effectively. Coping can indicate how people manage distress; therefore, maladaptive coping may have the potential to reflect distress tolerance difficulties. However, there are scales that directly capture distress tolerance (e.g., Distress Tolerance Scale; Simons and Gaher, 2005), which should be considered to better understand how comorbid suicidality and internalizing and externalizing outcomes relate to this core DBT target outcome. A person-centered clustering approach may provide a more holistic representation of their symptomology and treatment progress, whereas we framed our hypotheses in terms of individual variables. Moreover, this study did not account for the presence of attention-deficit/hyperactivity disorder (ADHD) symptoms, which may affect patients’ ability to learn DBT skills. Although programming was adapted for individuals with executive functioning difficulties, future research should control for ADHD and other neurodevelopmental disorders. Finally, this PHP did not formally collect information on factors that could influence treatment outcomes, including illness duration, treatment attendance, skills practice, or family involvement, which should be accounted for in future studies.
Conclusions
Our results indicate that suicidal patients with higher externalizing behaviors demonstrated greater emotion dysregulation after four weeks of DBT in this PHP. Despite this, all patients demonstrated improvements across the target DBT outcomes, suggesting patients with elevated symptoms can benefit from spending more time in this intensive DBT program and can help identify and guide the specific DBT skills targeted during sessions. For example, clinicians should monitor and prioritize emotion and behavioral regulation skills for youth with acute externalizing behaviors, as they may be at higher risk for persistent emotion and behavioral regulation difficulties even during short-term DBT. Youth with high externalizing symptoms may benefit from additional coaching or behavioral strategies beyond standard DBT. It is especially important to involve caregivers and other providers (e.g., school staff) to help reinforce DBT skills in multiple settings (e.g., home, school, community), as patients with acute externalizing symptoms can benefit from a systems-approach, even after attending a short-term program, like this DBT PHP, to optimize their skills in these domains.
In sum, our findings suggest that this DBT program can be effective across different symptom profiles, which supports its use as a transdiagnostic intervention and can allow clinicians to focus on core skills (e.g., emotion regulation) rather than diagnosis-specific protocols, especially for patients with acute externalizing symptoms who may need additional clinical support and attention.
Availability of Data and Materials
Datasets used in this study may be accessed upon request.
Footnotes
Author Disclosure Statement
The authors have no known conflicts of interest to disclose.