
Abstract
Purpose:
To describe parents’ perspectives of health care provider actions that helped or did not around the time of infant/child’s intensive care unit (ICU) death. Semistructured interviews with 63 parents (Black, White, and Hispanic) 7 months post infant/child death were audio-recorded, transcribed, analyzed, and themes identified.
Findings:
What helped most: compassionate, sensitive staff; understandable explanations of infant’s/child’s condition; experienced, competent nurses; providers did everything to help infant/child; and parents’ involvement in care decisions. What did not help: insensitive, nonsupportive staff; conflict between providers and parents; communication problems around the death; inexperienced nurses and doctors; parents not understanding child’s disease, care, complications.
Conclusions:
Compassionate, sensitive staff and understandable explanations of children’s conditions were most helpful; insensitive, nonsupportive staff least helpful by gender, racial group, or care setting. Conflict between providers and parents was most problematic for minority parents and mothers.
Keywords
Introduction
Approximately 25 000 children (birth to 19 years) die annually in hospitals in this country, most in neonatal intensive care units (NICUs) and pediatric intensive care units (PICUs).1,2 Death of a child is devastating for parents and grandparents and is felt by all members of the family. 3 Parents whose child has a chronic or terminal illness experience their child’s declining condition and the emotions that accompany an impending great loss. For others their child’s unexpected death evokes an immediate sense of unreality and great pain. Grief experienced by parents is personal and unique, involving a range of emotions including anger, pain, guilt, loneliness, anxiety, and emptiness. 4 Both NICU and PICU environments with their fast pace, high-technology equipment, high noise levels, and frequent emergencies are frightening and add to parents’ anxiety.5,6 When parents have no existing relationship with the hospital or live at some distance, the pain, loss, and sense of bewilderment can be worse. 7 And the use of pediatric palliative care to help both the child and the family is often used late or only after the child’s death. 8
What health care providers do around the time of a child’s death is important for families attempting to cope with a devastating life event and can have an effect on parents that lasts for decades.9,10 The primary aim of this study was to describe parents’ perspectives of what health care providers did that helped or did not help around the time of their infant’s/child’s death. A secondary aim was to examine differences by parent gender, race, and care setting (NICU or PICU).
Parent Experiences
Parents report a variety of responses during their child’s hospitalization including feeling lost in the hospital environment, bewildered by the many types of staff, yet wanting support and ready access to staff, honest and complete information, and trust in physicians to do all they could to save the child’s life.6,10 –13 Conflicting information among physicians was stressful for parents. Parents value nonjudgmental care, empathy, prayer, and bereavement support. 14 In other studies, parents report the importance of a consistent group of caregivers who have better communication with the family and continuity of care and the opportunity to have memories (eg, to bathe and hold the child) and memory keepsakes (handprints, locks of hair).14,15 A number of studies report lack of adequate palliative and hospice care.16,17
Decisions needed around the time of the child’s death, including resuscitation and autopsy, are especially stressful for parents.18,19 Some parents want clear explanations and written summaries of options before making a decision; some wish to be present during resuscitation; and when withdrawal of life support is necessary, some appreciate choosing the time and place to stop the ventilator. Most parents wanted to hold or be with their child before the death. 18 At the time of death, respect for the child’s body and compliance with the families’ wishes on autopsy and funeral arrangements are important to mothers but are not always understood by health care professionals, which hinders parent coping. 13 After the death, parents often feel lost and abandoned by health care providers and want to continue the relationship with hospital staff. 20 Parents perceive the lack of visiting by hospital staff during the palliative stage, lack of attendance at children’s funerals, and lack of telephone calls as disappointing and hurtful.4,21
Differences by Gender and Race/Ethnicity
Admission of an infant or child to an NICU or PICU frequently creates high parental anxiety5,22 that may be compounded by language and cultural differences. This holds if parents speak a language different from that of health care providers, where there are insufficient translators, or where the cultural norms for decisions on care are group decisions rather than individual decisions.17,23 African Americans may hold mistrust of the health care system, especially regarding advanced directives and end-of-life care, and both African Americans and Mexican Americans verbalize a preference for decision making as a family.24,25 Research by Doty and Ives 26 found that Hispanic families report more difficulty than non-Hispanic families in understanding non-Hispanic physicians, regardless of language. Other research found physicians ignore more comments from Spanish speakers than English speakers. 27 In addition, members of minority cultures may be passive with authority figures and fearful in medical situations. 23
A number of studies have demonstrated that infant and child death affects women more than men, resulting in more traumatization, general symptomatology, posttraumatic stress disorder (PTSD) symptoms and intense, and longer lasting grief symptoms.28 –35 In a sample of 35 married couples, Schwab 36 found that, compared to fathers, mothers experience more hurt, depression, anger, guilt, confusion, somatic problems, and preoccupation with the child’s death and are less able to control their expressions of emotion. However, 1 study found that fathers’ anxiety and depression scores increase from 1 to 6 months after the death but mothers’ scores do not. 31 Fathers of deceased children with disabilities feel that they grieve differently, but not less, than their wives. 37 Cordell and Thomas 38 also found differences in grieving between mothers and fathers; men’s responses are consistent with their perceptions of how men should behave.
Despite the changing demographic makeup of the United States, research on racial/cultural differences and similarities in parents’ perspectives of health care provider actions around the time of the child’s death is very limited. Most studies consist of primarily or exclusively White samples of women with few studies including more than 20% non White participants 17 and men. Most have small sample sizes4,6,13,21 and have been conducted with differing lengths of time since the child’s death, requiring parents to recall events that happened up to 10 years ago. 13 Other studies have a wide range of infant/child ages at the time of death, including parents who experience death of a newborn and death of a 20-year-old child, sometimes in the same study. Parents recruited from parent support groups and advertisements, 18 especially those who lost a child many years earlier, are likely to be systematically different than parents recruited from a hospital setting soon after the child’s death. Comparisons between families whose infant died in an NICU and those whose infant/child died in the PICU have not been reported. This study was designed to address these knowledge gaps.
Methods
The qualitative data reported here are from a longitudinal mixed methods study examining parents’ health and functioning following the ICU death of a child. The study was approved by the institutional review boards (IRBs) of the University and each study site. Parents (White non-Hispanic, Black non-Hispanic, Hispanic/Latino) who had lost a child in the NICU or PICU were recruited from 4 hospitals in South Florida and from death records from the Florida Department of Health’s Office of Vital Statistics. One hospital was a free standing children’s hospital, 3 were comprehensive referral hospitals with NICU and PICU units. Families were identified by clinician coinvestigators at each study site. A letter was sent to each family (in Spanish and English) describing the study. Research assistants (RAs) then called the families, screened for inclusion and exclusion criteria, described the study to them in Spanish or English, answered parents’ questions, obtained verbal consent, and scheduled the first interview where written consent was obtained. All parents were able to understand spoken English or Spanish, had a singleton pregnancy, a neonate who lived for more than 2 hours in the NICU, or a deceased child 18 years of age or younger who lived at least 2 hours in the PICU. Exclusion criteria were a multiple gestation pregnancy with a deceased newborn, the child living in a foster home before hospitalization and whose injury was suspected to be due to child abuse to eliminate extreme family conditions, and death of a parent in the illness/injury event, such as motor vehicle crashes, because the surviving parent would be dealing with the death of a spouse and a child simultaneously. Quantitative data were collected at 1, 3, 6, and 13 months post death. Qualitative data were collected from 63 parents at 7 and 13 months post death using semistructured interviews. At the 7-month interviews, parents were asked for their perspective on the events around the time of their child’s death.
Procedure
Using a standardized protocol with core questions and probes (Table 1), the 63 semistructured 7-month post death parent interviews were conducted in English and/or Spanish by health professional students with advanced clinical degrees. The semistructured interviews were developed based on the purpose of the study, the literature, our own clinical expertise in this area, and in discussion with the 2 study consultants. One consultant is an internationally known medical sociologist whose expertise is in qualitative methods and families with chronically ill children. The second consultant is a nationally known nurse scientist whose area of expertise is grief in parents of deceased children, qualitative methods, and instrument development. The interview questions and format were further reviewed by each of our clinical site coordinators for face validity, understandability, and level of language. Seven months after the death was chosen for interviews since it was a month after the 6-month milestone of the death. The investigators wanted the parents’ views after they had reflected on their experience to identify aspects of the experience that were truly important to them. In addition, this timing prevented contamination of the 6-month quantitative interviews for this subsample.
Interview Questions.
The interviewers were trained in study interview methods and supervised to maintain interview integrity across parent participants. Interviews were conducted in the parents’ homes at a time convenient for the parent/parents and were conducted separately in another room when both parents participated. Interviews, which took 1.5 to 2 hours, were audio-recorded and transcribed verbatim in the language of the interview. Transcripts were compared to audio-recordings for transcription accuracy by English- and Spanish-speaking PhD and master’s students in health disciplines. Corrected transcripts were entered into Atlas.ti for analysis. To develop initial codes, an inductive approach to thematization was used on an initial 6 transcripts by the investigators and 6 PhD students with relevant clinical expertise. Using themes derived from this initial inductive analysis and their operational definitions, 2 English speakers and 2 Spanish speakers coded the interviews. All coders were graduate students in health care disciplines and fluent in the language they were coding. All transcripts were coded independently by 2 coders and compared. The English speakers and the Spanish speakers also discussed their coding to maintain consistency across languages. Any inconsistency in coding was reviewed and discussed by the 2-coder team until they reached consensus. Texts that included discussion of “health care providers” (nurses, physicians, psychologists, social workers, physical therapists, etc) were then analyzed for subthemes following the same process described above. The number of parent responses within each subtheme was tallied and compared by parent gender, race/ethnicity, and setting in which the child died (NICU or PICU; see Tables 2 and 3).
What Helped Most.
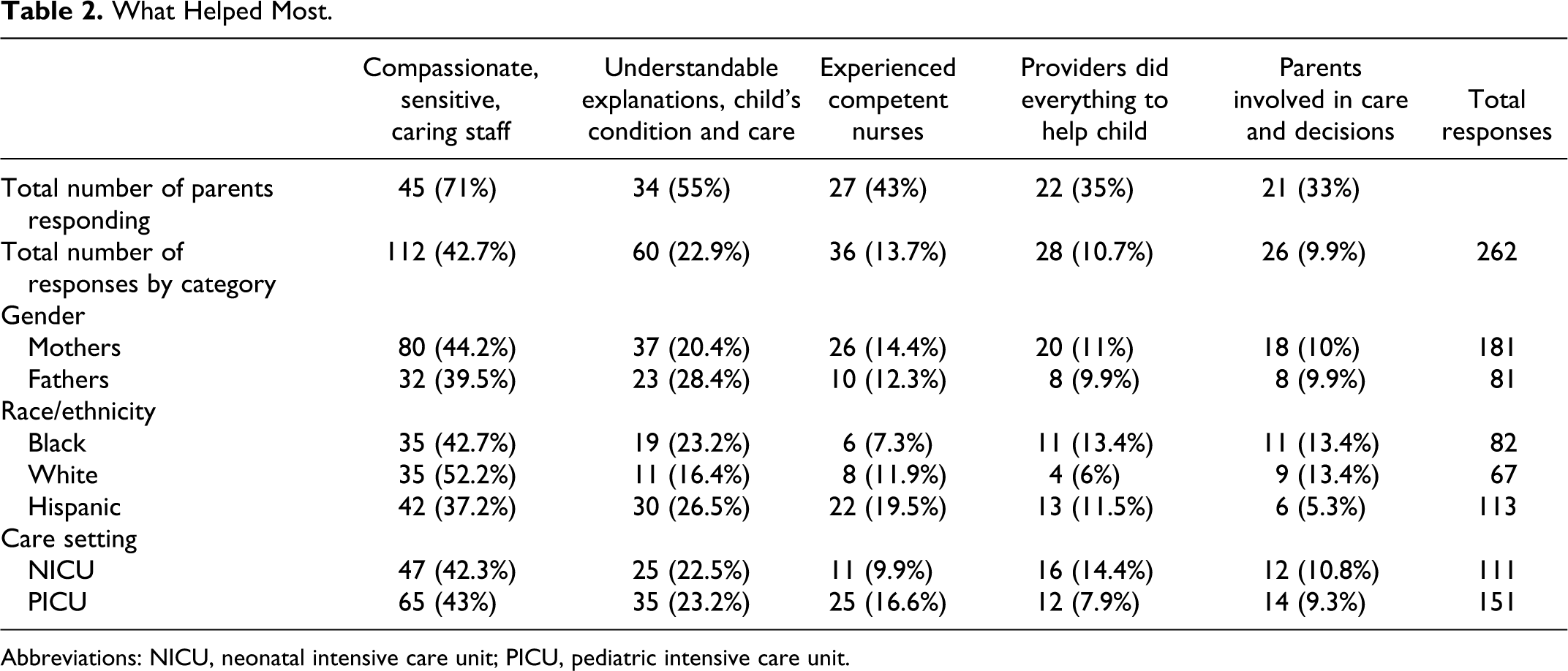
Abbreviations: NICU, neonatal intensive care unit; PICU, pediatric intensive care unit.
What Did Not Help.
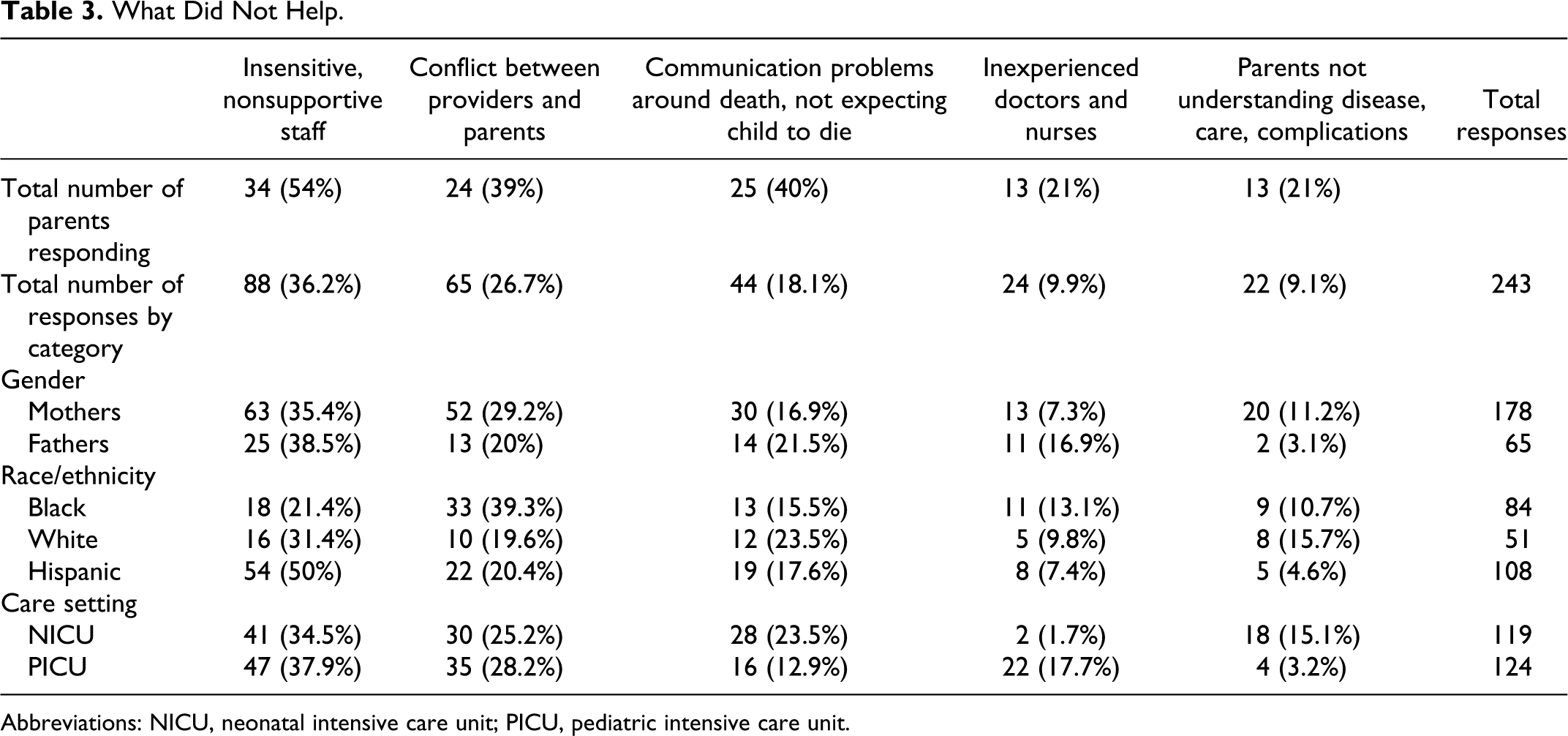
Abbreviations: NICU, neonatal intensive care unit; PICU, pediatric intensive care unit.
Results
Current Study Sample
This subgroup, a convenience sample of the first 63 parents (with 22 NICU infant deaths and 25 PICU child deaths) willing to participate in the qualitative data collection, did not differ in characteristics from those in the larger sample. Interviews conducted from November 2007 to September 2010 were done with 46 English-speaking parents (35 mothers and 11 fathers) and 17 Spanish-speaking parents (9 mothers and 8 fathers). Parents’ mean age was 35.1 years (SD = 9.03); 33% were Black, 27% White, and 40% Hispanic; most were married (65%); 49% had incomes above $25 000; 33% had some college or technical school; 37% were college graduates; and 35% had no other living children. Major causes of child death were congenital anomalies (25.5%), prematurity (23.4%), head trauma (14.9%), and chromosomal abnormalities (10.6%). Mean age at death was 43.4 months (SD = 66.23). Sixty-two (98.4%) of the 63 parents identified health care provider actions they perceived as helpful, while 51 (81%) of the 63 parents identified provider actions that were not helpful.
What Helped Most
Themes, rank ordered, regarding what helped most were compassionate, sensitive, caring staff; understandable explanations regarding infant’s/child’s condition; experienced, competent nurses; perceptions that providers did everything to help the infant/child; and parents’ involvement in care and decisions (Table 2). Mothers had more responses about what helped most than fathers, however mothers’ and fathers’ responses were similar in the percentage of responses by category. In all 3 racial/ethnic groups and for PICU and NICU parents, the categories of “compassionate caring staff” and “understandable explanations regarding the child’s condition and care” had the highest number of responses, indicating these actions by health care providers helped the most. Of the 5 categories, Black parents had their lowest response as “experienced competent nurses,” while for Hispanic parents this category had the third highest number of responses. For Hispanic parents, the lowest number of responses was in “parents involved in the child’s care and decisions.” White parents had the lowest number of responses in the category of “providers did everything they could to help their child.” The category of “experienced competent nurses” had the third greatest number of responses by PICU parents, while this category received the least for NICU parents.
Compassionate, sensitive, caring staff
Provider actions perceived as caring and compassionate included nurses and doctors who cared for the child almost as if he or she was their own and when the child was nearing death called the parents to be with the child and have the opportunity to hold the child before the passing. At the time of the death and immediately afterward, staff that cried and/or prayed with the parents, went to the child’s funeral, and telephoned the parents after the death were perceived as caring, sensitive, and compassionate. For some parents, the memory/keepsake box was perceived as a caring gesture. Her care leading up to her death was awesome.—They were very understanding to our needs.—They were in tune with what we wanted and they let us do what we wanted.—They gave us our privacy—but they checked on us to see that we were ok.—The doctor actually came to our daughter’s funeral. The ones that helped us through and made a difference—were the ones that—will remain in our hearts.—The ones who took that extra couple of minutes to talk to us, or you know tried to help us—believe that there was hope—and then when things showed what they were—they told us in a compassionate way—and I think that separates the good nurse from the bad nurse and the good doctor from the bad doctor—those that can cry with you, those that feel for you—but they still have their head on straight.
Understandable explanations regarding the infant’s/child’s condition
This category included health care providers being patient with parents’ questions, providing explanations in the language and at a level they understood, and providing explanations more than once. Questions received by the staff—very positive—sometimes probably frustrating because we drove them nuts with the details.—Our background is not in medicine. The neurologist spent hours with us showing us CAT scans, explaining what it all means and we felt it was our responsibility to really understand what was going on with her—and the diagnosis was very complex —the outcome unclear. We were educated enough to really understand it for the most part—and I think it was well received by the medical staff. The 2 young nurses really took the time explaining everything to me—what was going on. They are in the medical profession—you know, it’s easier for them to understand certain things but you know, you explain something to me I might forget it in a few minutes or you can explain it to me right now, this moment—5 minutes after, [when] I have to explain it to my mom—I’m like—what’s that again? You don’t really fully grasp it until you hear it a few times.
Experienced, competent nurses
Parents perceived and valued nurses who worked with confidence in caring for their child, nurses who cared for the child over time and knew the child’s needs and routines, and nurses who parents trusted to care for their child while they were not at the bedside. They felt they could go home confident that the child was being well cared for by nurses familiar with his or her care and who would call and tell them if the child’s condition had changed. None of the nurses gave our family members and our friends any headaches. They were always seeing if she was comfortable and that she wasn’t in any pain—bringing her anything she wanted—if she wanted a certain movie—if she wanted ice cream—you know things she can softly eat—just I mean, just comforting us—telling us—“you guys are doing great”—just uplifting us—ah man,—can’t say better words about those nurses. I couldn’t have asked for better.—Those nurses were so good to her.—They took such good care of her. Every time we called, they answered. They didn’t get mad that we called so many times.—They understood that—that we were so far away that we couldn’t really get to see her much and they didn’t care that we were staying there until like 3 o’clock in the morning.—They didn’t let it bother them.
Perceptions that providers did everything to help the infant/child
Provider activities contributing to these perceptions included trying the range of treatment options for the child, keeping the child comfortable, and explaining any remaining treatment options to the parents. They tried, they tried.—There was nothing I could tell you that they didn’t do.—They tried cause if they wouldn’t try he would have passed away that same day.—So I know they tried. There was a doctor who was really trying to make me come to terms that she’s dying—and that there is nothing they can do. He suggested things like getting a footprint, holding her. He did his best to try to help a bad situation because there is no easy way of doing it. He really supported me. I felt he felt my pain as a parent so that helped at the end when they asked me to let her go—to stop CPR—that really helped me to make a decision that they did do everything possible.
Parents’ involvement in care and decisions
Parents were very vocal regarding being involved in their child’s care and decisions about care. Keeping parents up to date on the child’s condition, changes in treatments and the child’s condition, and shared decisions on the timing and removal of life support were very important. When they got a code blue everyone was there—giving him CPR. The doctors, nurses, everybody was there—and they said if we wanted them to—they would stop doing that—that he was going to go—and they needed to know what to do.—We didn’t want him to suffer anymore.—We told the doctor—to stop—and he gave us the opportunity to say goodbye to him. We would have a meeting with the doctors, nurses, everybody.—They would tell us exactly how they were gonna do this, why they were gonna do this, do you approve—do you want to do something different?
What Did Not Help
Themes, rank ordered, on what did not help were insensitive, nonsupportive staff; conflict between providers and parents; communication problems around the death including not expecting to be told their child would die; inexperienced, unknowledgeable nurses and doctors; and parents not understanding the child’s disease, care, and complications (Table 3). For mothers and fathers, White parents, Hispanic parents, and both PICU and NICU parents, the category of “insensitive, nonsupportive staff” received the highest number of responses, indicating actions least helpful to parents. For Black parents, “conflict between providers and parents” was the least helpful followed by “insensitive, nonsupportive staff.” There were other notable differences in responses by racial/ethnic group. The second least helpful category for White parents was “communication problems around the death” and for Hispanic parents, “conflicts between providers and parents.” Both PICU parents and NICU parents indicated that “conflicts between providers and parents” was the second least helpful provider action.
Insensitive, nonsupportive staff
Parents perceived provider actions as insensitive and unsupportive when they were abrupt, when they were perceived as being cold and insensitive to the parent’s situation, and when they laughed and joked outside the dying child’s room. He said—“well I explained to you.”—He got agitated with me when I questioned him.—He said, “I explained to you there’s no hope and there’s no brain activity. Yes we can do another test to see if there’s anything that has happened but I am telling you it’s kind of useless what we are doing here.” He seemed to get disgusted with me and he walked away. The night before she died, the nurse kicked me out of the room and told me I was doing more damage to her—because I was holding her and touching her. She said I shouldn’t stimulate her and she took her away from me—she took my last night that I had with my daughter away.
Conflict between providers and parents
Conflict between parents and providers occurred in several areas: aspects of care, aggressive treatment versus not, and pressure to end life support, sign autopsy or organ donor papers, and make funeral arrangements. Conflicts arose when providers imposed their own views on these critical decisions that had to be made. Conflicts also arose when providers insisted on following orders or standard procedures rather than listening to parents who knew the child’s care routine. He wanted to trach her and I refused to trach her. I told him “you prove to me why she needs to be trached and I will [allow you to] trach her, but if you cannot prove to me that she needs to be trached, then she won’t be trached”—and he says to me—“well you need to educate yourself, you’re stupid.” He told me there are 6 people working on him, “what do you want”—he kind of led me to believe that it was too much—people working on him. “I have 6 nurses on him and we can’t work fast enough”—and then he mentioned organ donation—when I just found out my son had an accident. At that point I was basically very angry with the doctor because I am thinking is [my son] gonna get less quality care because they want his organs.
Communication problems around the death including not expecting to be told the child would die
Providers’ declarations that the child would die were perceived as not helpful by many parents. For some parents the child’s death was unexpected, while for others it was not expected at this time. For many parents the manner of communicating the information was perceived as unhelpful in their time of crisis. They did not talk to me about a “do not resuscitate” order.—We didn’t talk about that at all. When she started to crash they asked me to leave the room—and I flipped out. When they invited me back in, they told me she had more brain damage—and asked me if I wanted them to discontinue life support.—That had not been something they had ever asked me or talked to me about—and I felt—really kind of—I mean, I couldn’t make a decision in that—in that moment.—I mean, she is laying right in front of me dying.—So I really wished they had talked to me about that beforehand.—I was alone.—I didn’t know my husband’s answer to that.—It was a big decision—with no notice. I think the NICU doctor came in and told everyone he wasn’t breathing and he was having seizures—and I honestly don’t even remember what happened. I was in complete shock. I didn’t understand why everyone else was crying. I didn’t understand what the doctor was saying. I didn’t understand how it can go from being like a 90% chance of surviving to your child’s not gonna make it anymore.
Inexperienced, unknowledgeable nurses and doctors
Nurses and physicians were perceived as inexperienced and not knowledgeable about the child’s diagnosis or care and treatment when they were not familiar with the diagnosis, symptoms, and course; not competent using equipment needed for the child’s care; and demonstrated only beginning knowledge and skills that parents had not expected from providers of a dying child. The doctor was asking about the family history. He was asking him [husband]—and he said, “the only thing that runs in our family is asthma.” They wasn’t asking me [mother with preeclampsia] so I told them—the only thing that runs in our family is high blood pressure. My parents were with my daughter at the hospital so my husband and I could leave and take showers and stuff.—She was on the dialysis machine. The nurse that came on when my parents were there—one of the machines got messed up—and the nurse didn’t know what to do. My mom asked what was going on—and the nurse was abrupt and didn’t want to answer my mom’s questions—and my mom got upset—and so did I. I felt nervous even being around [this nurse]. There was a situation when the dialysis machine was stopping.—This was a huge issue for us. She just didn’t seem like she knew what she was doing. I later spoke to the nursing director just about what happened—and found out she was a “traveling nurse.”
Parents not understanding the disease, care, complications
Many parents did not understand providers’ explanations of the child’s care and condition due to language that was unfamiliar or not at their level and complications that were unexpected and not explained. I kept asking them—what are the results to that—nobody tells me anything—the EEGs—no one ever completely—fully explained them to me.—they are like,—“Well they’re like the other one.”—So I’m like, ok good—cause I don’t understand the other one either. He was just so small and he wasn’t moving.—He’s incredibly little—like a doll. They took him—and I figure they are going to clean him up and put him, you know—whatever they do—and this lady looks at me and she says to me—“ah do you want us to resuscitate him?”—and I’m looking at her like, are you out of your mind?—What do you mean?—What do you mean—do I want your to—and I say—“You need to NOW.”—She asked me 3 or 4 times and I’m screaming—and I’m seeing the time passing by—and I don’t hear him crying.—Why isn’t he crying? She just kept on asking me and she says to me, “he can have cerebral palsy, he may not walk, he may not talk, he may not play, he may not be a normal kid—do you want me to”—and I answered and I turned around and told her to go to—. They took him and I didn’t see him anymore.
Discussion
Some findings from this study regarding the need for compassionate, caring staff 14 and understandable explanations of the child’s condition and prognosis 10 are consistent with the findings of others. Moreover, findings regarding insensitive staff and conflicts on care or ending life support13,18,19 are also consistent with those reported previously. Comparisons of parent responses by gender, racial/ethnic group, and care setting in this study add to the knowledge in this area.
In examining parent responses by gender, similar proportions of mothers and fathers agreed on categories of what helped most (Table 2), and the category of “insensitive, nonsupportive staff” (Table 3). Responses then differed. Mothers had more responses regarding “conflict between providers and parents” and “not understanding the child’s disease, care and complications” than fathers (Table 3). Mothers likely were with the children more in the ICU and assumed more of their care than fathers, thus accounting for the responses in these categories. If mothers were in the ICU more often, they likely encountered comments from providers aimed at decisions that parents made, which were not consistent with what providers wanted. Sometimes these conflicts result from a mismatch in the parents’ and the provider’s priorities. Parents often are focused on comfort issues—positioning of the child, having a toy or other prized possession nearby, modesty measures—while providers are focused on measures to support the child’s vital signs and functions. Mothers may also have seen more care changes that occurred with little or no explanation or one that was confusing. Fathers expressed more concern about “inexperienced doctors and nurses” and “communication problems” than mothers. This may have been because fathers interacted less frequently with staff while mothers had developed a relationship with the staff, observed provider skills and developed more trusting relationships than fathers. Communication with parents is a major concern in studies of parents with children in ICUs.22,39 Major stressors of changes in the parenting role, child suffering, and potential death increase anxiety and decrease parents’ ability to absorb information provided to them. A potential disparity in time on the unit and fathers’ need to gain information from mothers based on her understanding of the child’s care and prognosis may help to explain fathers’ greater concerns around “communication problems.” Differences in the responses of mothers and fathers to health care provider actions may also be due to differences in cultural expectations of parenting and gender roles.
In all 3 racial/ethnic groups, “compassionate caring staff” and “understandable explanations regarding the child’s condition and care” were perceived as provider actions that were most helpful to parents around the time of their child’s death. For Hispanic parents, the category of “experienced competent nurses” was perceived as the third most helpful, while for Black parents it was perceived as the least. In other studies, nurses are considered to be more involved during the dying process than other family members or friends and have been described as “skillful, compassionate strangers.” 40 Some parents in this study referred to nurses as “family.” This may be due in part to their providing care for critically ill children around the clock for days to weeks to months in the ICU. Nurses are also reportedly viewed as more emotionally supportive than physicians. 41 For both Hispanic parents and Black parents responses in the category of “parents involved in the care and decisions” received the least or next to the least number of responses. Previous research indicates members of minority cultures tend to be passive with authority figures and fearful in medical situations. 23 Hispanic Americans are reported to rely more heavily on physician judgment 42 which may also have contributed to these findings. For White parents, the category of “providers did everything they could to help their child” received the lowest responses of the 5 “what helped” categories. This may be a reflection of a reportedly greater level of comfort in agreeing to limit care, ending the child’s pain and suffering. 43
Although the rankings differed, parents in all 3 racial/ethnic groups found “insensitive, nonsupportive staff,” “conflicts between providers and parents,” and “communication problems around the death,” as the 3 categories of provider actions that were most problematic for them around the time of the child’s death (Table 3). For Hispanic parents “insensitive, nonsupportive staff” was most problematic, accounting for 50%of their total responses followed by “conflicts between providers and parents.” These findings may be due to language differences between parents and providers, lack of translators, or cultural differences between parents and providers. 17 Studies indicate that Hispanics and Blacks prefer decisions about care and end of life be made by the family as a group, while Whites prefer autonomy in decision making. 44 In addition, Blacks believe in a “higher power” and “miracles” and prefer more aggressive treatment rather than giving up and ending life support. 44 As Bullock’s 44 research found, Black adults noted that “those who believe” do not “hasten death” through the use of advance directives and hospice care plans. For Black parents in this study, “conflicts between providers and parents” were most problematic, perhaps reflecting differences in belief systems, decision making, and distrust with the health care system and physicians and preference for more aggressive treatment. Both Hispanic parents and Black parents had the fewest comments categorized as “not understanding the child’s disease, care and condition.” This was especially evident with Hispanic parents where responses in this category were less than 5% of the total 108 responses. These parents may have felt they had a sufficient understanding of their child’s condition and care but were in conflict with care and treatments suggested or carried out by providers. White parents responded least about “inexperienced doctors and nurses.”
Both PICU and NICU parents’ responses indicated that “compassionate caring staff” and “understandable explanations regarding the child’s condition and care” were most helpful. Parents of children who died in the PICU had the third greatest number of responses in the category of “experienced competent nurses,” while this category had the fewest responses from NICU parents. This may have been because their children were in these units for longer periods of time or episodically over time where parents and nurses who provided care for their children over 24 hours developed trust relationships. For NICU parents, this category received the least number of their responses perhaps because of shorter hospital stays, being overwhelmed by the ICU environment with its, noise, emergencies, and little time to develop relationships with nursing and other health care staff.
Both PICU and NICU parents’ responses indicated that “insensitive, nonsupportive staff” and “conflicts between providers and parents” were most problematic. For NICU parents, “communication problems” were the third most problematic category, perhaps reflecting their sudden overwhelming situation, high anxiety, lack of time to absorb what was happening, and to develop communication patterns with staff. For PICU parents “inexperienced doctors and nurses” ranked third and “not understanding the child’s disease, care and complications” had the least responses. For these parents, their child may have been ill for some time, allowing the parents to become knowledgeable in the child’s care and condition and be more concerned with inexperienced providers who were not familiar with the diversity of diagnoses and developmental levels of the children in the PICU.
Less than 1% of children with life-threatening illnesses receive hospice care, 17 with studies indicating that minority children are less likely than White children to receive hospice care. 41 Findings from this study with a 73% minority sample reinforce the need for a better understanding and earlier use of a palliative care team. While the study’s major clinical recruitment sites had palliative care teams, only 2 of the 63 parents mentioned palliative care or hospice care during their interviews. Palliative care was mentioned by 1 parent who wanted her son enrolled in a palliative care study being conducted in another state, but it did not work out. Similarly, hospice was mentioned by a parent who began to realize the parents were losing the battle for their child’s life. The mother indicated that hearing about hospice care was helpful in facing the life limiting stage of the child’s condition. Other than these 2 instances, palliative and hospice care that potentially could have helped the children and their families earlier in the child’s course, was absent from the conversations regarding health care providers’ actions around the time of the infant’s/child’s death. Perhaps as Docherty and team 45 found, the challenges of identifying the dying point, making the transition to palliative care, and turning care over to an outside palliative care team played a role for providers in this study. The prospect of relinquishing hope for a cure and attending to the terminal phase of life may be too difficult for many clinicians and parents.
Clinical Implications
In this study as in others, “compassionate caring staff” and “understandable explanations regarding the child’s condition and care” are provider actions viewed as most helpful to parents around the time of their child’s death. Providers are perceived as competent and caring when they show compassion for the child and sensitivity to the parents’ feelings and circumstances. This includes making the child as comfortable as possible; visiting the child and parents during the ICU stay; comforting them with a hug, a smile, a beverage; not removing hope until it is clear there is no other course; and honestly communicating that to parents in language and at a level they can understand. At the time of death, it is important for providers to help parents with arrangements that need to be made. After the child’s death, continued contact with parents by telephone or attending the child’s funeral is important in parents not feeling abandoned. These actions are important in parents’ coping with the child’s death, as well as in their perceptions of the success of the hospital’s services and the effectiveness of individual providers.
Parents need “understandable explanations regarding the child’s condition and care.” Providers need to find out what parents know and want to know. Timing of requests for “do not resuscitate” (DNR) status, organ donation, and autopsy is important. Parents need enough time to understand and take in the child’s critical condition and think about it before dealing with DNR and organ donation requests. In this study, for minority parents (Hispanic and Black) and for mothers, “conflicts between parents and providers” regarding care and aggressive treatment or not presented extremely stressful situations. For some parents, the child’s death will be unexpected due to a sudden unexpected deterioration in the child’s condition or a parent’s inability to hear and accept the providers’ message of impending death. Religion and culture often play a part in conflicts where parents view the child as a “gift from God” to be taken care of no matter the child’s condition or prognosis, a belief often at odds with providers. Other parents view the reason for a child’s life, the extensive care needed, and subsequent death as serving to bring the members of the family closer. Whatever the source of the conflict, providers must be open to the beliefs, values, and decision making used by the parents and families. This includes understanding that while parents from 1 racial/ethnic group may tend to respond in one way, individual differences within these groups are often as diverse as differences between groups.
By gender, racial/ethnic group, and care setting, “insensitive, nonsupportive staff” was perceived as most unhelpful in this study. Parents perceived some providers as cold and insensitive or less than knowledgeable about the child’s condition. Some health care providers have great discomfort talking to parents about a child’s impending death. This may be especially difficult for ICU providers whose whole focus is on rescuing children from life-threatening conditions. Research of Lawrence 46 indicated that sudden and unexpected infant death was one of the most stressful events faced by staff. Levetown, 23 in a review of communication problems, provides helpful approaches for providers talking with parents in NICU and PICU settings. Parents’ perceptions about unknowledgeable staff hold import for staffing decisions in ICUs. Traveling or float nurses, for example, who are not knowledgeable about the child’s condition or competent in ICU care, would be better assigned to general floor areas. Cross-training for some staff from acute care units would be a better solution to an ICU that needs more nurses due to a higher than usual acuity or unexpected staff absences.
Earlier use of hospice and palliative care can help families and dying children as well as staff. For parents, learning about palliative and hospice care from providers is a beginning. While White parents are known to use these services more than minority parents, research also indicates that when there is equal insurance coverage for hospice services the disparity in use by racial/ethnic group is resolved. 43 Greater provider reimbursement for these services could also make them more readily available.
Parents also express understanding of the stress providers face daily in caring for dying newborns and children. In this study parents asked, “How do you deal with this job every day—seeing parents and [their] kids that are going to die” or “Sometimes I feel worse for the nurse than I did for myself of what I put her through.—I don’t care how hard you are—and how they put up with it,—it still bothers at the end of the day.” Others commented, “I don’t know how they do it.—Anybody works at ICU that’s an incredible type of human being to do that—beyond my understanding of how anybody could go home and live watching all the illnesses and the deaths.—On the other hand, you see people live and that gives you the reward I suppose.” While these comments might not have been heard around the time of the child’s death, perhaps this perspective came with time and distance some 7 months away from the situation.
Providing care daily for dying children and their parents is stressful and difficult for health care providers. Controlling emotions, developing distance, reverting to hospital policies and procedures, joking and laughing in another geographical area and intellectualizing the child’s condition are health care providers’ methods of coping with the situation. And coping mechanisms are essential for the staff’s continued functioning. However, parents may easily perceive this coping as staff becoming desensitized, not caring for their child and themselves, not listening to them, and giving up on their child. Good communication between parents and providers can help with these perceptions. Other potential aids include availability of stress counseling for staff, bereavement-debriefing sessions 47 and upbeat social events that celebrate staff successes. Another may be periodic staff development programs using actual case studies and role playing that involve all members of the health care team. Such approaches may serve to help and support providers who are then able to better help parents faced with the death of a child.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Institute of Nursing Research, NIH, R01 NR009120