
Abstract
Background:
As patients in hospice become increasingly dependent upon caregivers, physical therapy interventions can minimize the risk of injury to the patient or caregiver that may occur during transfers between surfaces.
Case Description:
A 68-year-old male hospice patient was referred to physical therapy for strengthening and transfer training after a fall that resulted in the patient remaining in bed for 5 weeks due to an increased fear of falling. Treatments focused on caregiver training for correct transfer techniques.
Outcome:
During 10 treatment sessions, the patient and caregiver became independent and safe with all transfers. Although the patient’s health declined, his risk for and fear of falling decreased. Confidence with transfers improved for the patient and caregiver.
Discussion:
Physical therapy “benefits were immeasurable” for the patient and caregiver by teaching them how to safely perform patient transfers with reduced risk of injury.
Introduction
The role of physical therapy in the hospice setting is not widely used. Physical therapy can assist with caregiver training on the use of equipment, proper body mechanics, fall prevention strategies, and maintaining balance. 1 In the hospice setting, clinical decision making for physical therapists needs to be patient centered. 2 Physical therapy in the hospice setting involves compensation and support, as opposed to the traditional restorative approach. Regardless of the precipitating factors, the patient usually declines in function, resulting in a skilled need for physical therapy intervention. Ongoing problem solving and support helps the family cope with the changing needs of the patient. 2 When physical therapy is used in the hospice setting, patients are more satisfied with their care and find their rehabilitation program more effective when the patient discusses the physical therapy program with their physical therapist. 3 Additionally, the more actively families participated in the rehabilitation, the more effective and satisfactory the program was to the patients and the more useful in overall patient care. Therapy has the potential to decrease the cost of hospice services as well as balance the utilization of team members. 4 Therapy empowers both the family and the patient, reduces anxiety, decreases injuries, and restores dignity.
Hospice’s focus of care is to maintain a person’s quality of life (QOL) and physical activity positively affects QOL. Within a population with incurable cancer and a short life expectancy, physical exercise improved emotional functioning and physical fatigue was reduced. 5 Patients with spinal cord compression, who receive rehabilitation, have increased satisfaction with life, less depression, and persistent decreases in pain, according to observational studies. 6 When therapy services are provided, the hospice goal of promoting safety, independence, meaning, and QOL is more attainable, despite the physical and mental decline expected. 7 The purpose of this case study is to highlight the importance of caregiver training by physical therapists, in the hospice setting, to optimize the safety, function, and QOL for the patient and the patient’s family.
Case Description
The patient was a 68-year-old male who was referred to physical therapy for transfer training. He lived with his wife of 16 years, who was his primary caregiver. Their home was a single-family residence with 2 steps into the home, and a full flight of steps to the basement. The patient had a history of obesity, diabetes with a 30-year history of bilateral lower extremity neuropathy, hypertension, hypothyroidism, and coronary artery disease with a prior open-heart surgery. The patient was diagnosed with congestive heart failure in 2010, when he was hospitalized as a result of a myocardial infarction. He was placed on 2.0 L of continuous oxygen via nasal cannula at that time.
In January 2011, the patient was admitted to the hospital for 4 days and was diagnosed with pulmonary fibrosis. He was discharged to home on 8.0 L oxygen and was informed there was nothing more the physicians could do for him. About a week later, hospice services were requested. The patient was taking 13 different medications. His wife was responsible for administering most medications and assisted with blood glucose testing. The patient was still able to administer his own insulin.
The patient was previously referred to physical therapy when he was first admitted to hospice services. At that time, he received instruction in safe ambulation with a front-wheeled walker and a home exercise program was initiated. Four physical therapy treatments were provided over the course of 3 weeks. When he was discharged from physical therapy the patient was walking short distances on level surfaces with supervision and the use of a wheeled walker.
A second referral for physical therapy was made 5 months later, for caregiver training with safe transfers and functional mobility, as tolerated. Approximately 5 to 6 weeks prior to the referral, the patient fell at home while walking. No injuries were sustained but he was unable to get up from the floor and into bed until almost an hour later with maximal assistance. The patient’s wife repeatedly attempted to assist him from the floor, but the patient required an hour to recover before he had enough energy. Since that time, he remained in bed, primarily due to his and his wife’s fear of the patient falling.
The patient’s wife had difficulty with transferring the patient from the hospital bed to the wheelchair or bedside commode. She perceived herself to be exerting more than 50% of the effort in transferring the patient and observed the patient leaning backward during the transfer process due to his fear of falling. Conversely, the patient perceived his wife to be pulling him during the transfer. Both the patient and his wife expressed fear while attempting transfers and both were fearful of the patient falling to the floor. While the patient was being transferred by his wife, he was unable to see his feet, which he stated was frightening. The patient’s wife was experiencing physical strain from lifting him multiple times a day. She was exhausted, had increased low back pain, and was unable to leave the home for any length of time despite receiving respite assistance 2 hours a week to go to the store. The patient’s wife had a history of osteoarthritis in her knees, lower spine and both hands. A medical recommendation was made for bilateral total knee arthroplasty, but the patient’s wife was unable to schedule these surgeries due to her obligations as primary caregiver.
The patient had not ambulated in 5 to 6 weeks. He was weak and tired of being confined to the hospital bed. He rated his current QOL as poor. He was unable to sit and use his computer. Basic bed to wheelchair transfers were extremely taxing, typically requiring the patient to utilize supplemental oxygen due to hypoxia. He was still on 8.0 L of oxygen.
Over the last year and a half, the patient’s weight decreased from 350 to 209 lbs. The weight loss initially began when he began taking testosterone 1 1/2 years previously. He lost his appetite, had more energy, and lost an average of 8 pounds a month for several months. Since he became ill 9 months ago, he lost an additional 60 to 70 more pounds due to lack of appetite. The patient’s mind was alert and oriented, but he was unable to tolerate much physical activity. He was unable to tolerate sitting for any length of time, due to lightheadedness and symptoms consistent with hypotension. Assistive aids included an oxygen concentrator, portable oxygen, hospital bed with overhead trapeze, wheeled walker, wheelchair, and a gait belt.
Quality of life declined significantly for both the patient and his wife since he had been unsafe to transfer or ambulate. When asked about specific goals for physical therapy, the patient’s wife wanted to be able to transfer the patient safely and confidently with the risk of falling minimized. The patient wanted to be able to walk to the outdoor patio, approximately 20 feet, and sit outside briefly.
Examination
At the time of the second physical therapy examination, the patient’s supine blood pressure = 95/60 mm Hg, heart rate = 92 bpm, and SpO2 = 94% on 8.0 L oxygen. He was 6’1” and 209 lbs. with a body mass index (BMI) of 27.6. There was no presence of lower extremity edema. His skin color was pale at rest and became almost white with activity. The patient’s overall range of motion was within functional limits. His lower extremity strength was grossly 3+/5 and bilateral upper extremity strength was grossly 4+/5. 8 He kept the head of the hospital bed elevated in order to breathe more easily.
The patient was able to transfer from recumbent to sitting with standby assistance and sat on the edge of the bed with his hands propped and contact guard assistance. He performed a sit-to-stand transfer with the use of a gait belt and a front-wheeled walker with minimal assistance. He was able to maneuver the walker and complete a stand pivot transfer to the wheelchair, with minimal assistance. The patient was fatigued and short of breath after this transfer, requiring him to sit in the wheelchair for 5 to 6 minutes and utilize supplemental oxygen, at 8.0 L via face mask, to recover. The patient’s physical symptoms were closely observed and monitored by the physical therapist for signs of hypoxia/hypotension. The patient was unable to ambulate at the time of the initial evaluation due to weakness and shortness of breath.
The patient’s balance was assessed with Tinetti Assessment Tool with a resulting score of 9/28, placing him in the high fall risk category. 9 He scored 62/64 on the Falls Efficacy Scale–International (FES-I), indicating a high fear of falling. 10 Both the patient and his wife were asked to rate their confidence in her ability to transfer him safely, using a bipolar scale of (−)3 to (+)3. He rated his confidence in her, at a (−)2 or (−)3. The patient’s wife rated her self-confidence in transferring the patient at (−)3. The patient reported no pain during the evaluation.
The body mechanics of both the caregiver and the patient were observed while the wife transferred the patient from the bed to the wheelchair and recorded with the use of video (Figure 1). During the transfer, her trunk was flexed forward, with lower extremities fully extended. She attempted to lift up the patient without the use of a gait belt or walker. The patient was unable to see his feet, which frightened him. His impaired sensation in his feet, as a result of diabetic neuropathy, compounded his fear of falling. The patient maintained his arm position, around his wife’s shoulders, with his legs visibly shaking as he attempted to complete his transfer to the wheelchair. After completing the transfer, the patient was pale, short of breath, and visibly fatigued. He required supplemental oxygen and several minutes of resting.
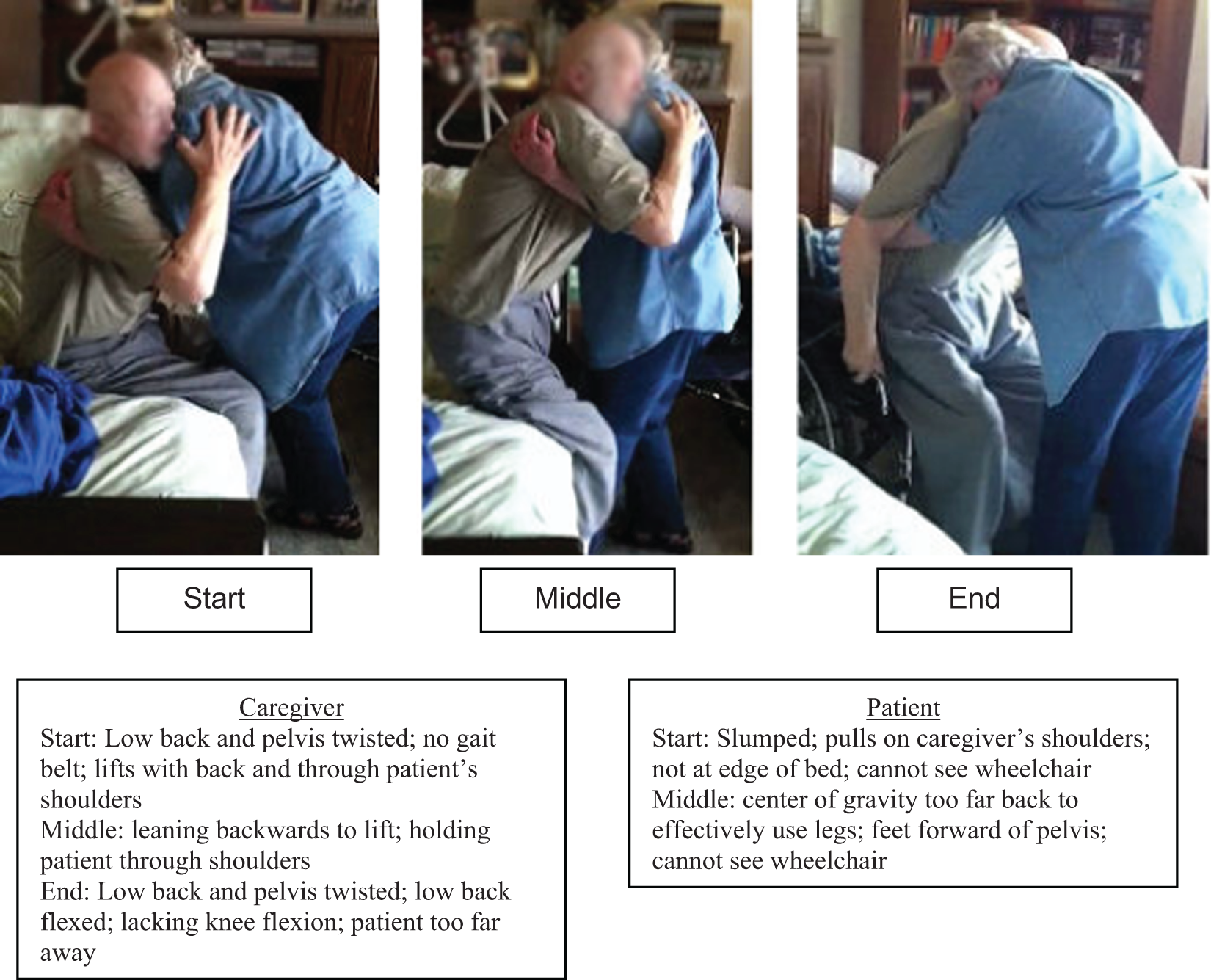
Images of the start, middle, and end of a transfer performed during the initial evaluation with a brief listing of incorrect transfer techniques by the patient and the caregiver.
Clinical Impression
Both the patient and the caregiver needed careful instruction in safe transfer training. The patient’s wife demonstrated poor body mechanics during the transfer process, and both parties were fearful of the patient falling. Her poor transfer technique was likely contributing to her low back symptoms. Both parties realized their transfer process was unsafe.
The emphasis of physical therapy was to address the needs of the patient and his wife, to improve their satisfaction and ability with meeting needs while expecting a consistent decline in ability. Treatment goals were (1) the caregiver was to safely transfer the patient using appropriate equipment and technique; (2) reduced risk and fear of falling using the Tinetti and FES-I (both the patient and caregiver); (3) the patient was to ambulate 20 feet, to the patio, with a walker and minimal assist; and (4) the patient would be independent with an updated home exercise program for strength and flexibility.
The prognosis for this patient was limited. This patient’s functional mobility and strength was expected to improve, although ultimately his overall decline was anticipated; however, his wife was expected to be independent with safe patient transfer techniques. The plan of care included physical therapy intervention twice a week for 2 weeks, then once a week for 4 weeks. Visit frequency was set at once a week after the initial 2 weeks to allow opportunity for the patient and his wife to implement what was instructed in therapy sessions and for the physical therapist to provide appropriate instruction as the patient and caregiver needs changed.
Interventions
Treatments consisted of caregiver training in proper transfer techniques for bed to wheelchair transfers and sit-to-stand transfers. Caregiver training also included the use of a gait belt and walker. Video recordings of caregiver and patient transfers were utilized to educate the caregiver on proper transfer techniques. No verbal cues were given to the caregiver to safely transfer the patient after treatment 4. The patient’s home exercise program, which was previously established, was reviewed and updated to address the patient’s current needs. Therapeutic exercises were included to improve bed mobility, transfers, and to prevent skin breakdown, as the patient tolerated. Gait training was implemented as appropriate and desired by the patient.
Outcomes
The patient received a total of 10 physical therapy treatments over 8 weeks. The initial goal of safety with transfers was achieved by the fifth visit. The remaining treatments were utilized for gait training, strengthening, reinforcement of correct transfers, and other specific goals the patient or caregiver had on the day of treatment. On visit #8, the patient’s balance and fear of falling was reassessed. The patient’s Tinetti balance score improved 9 points to 16/28 and the FES-I scored 61/64.
The patient and his wife’s confidence with transfers improved to (+)3, from (−)2 or (−)3, for both parties after this episode of physical therapy. The caregiver was fully independent and safe with all patient transfers (Figure 2). The patient’s strength and transfer sequence improved, requiring contact guard assistance, and occasionally minimal assistance, depending on the patient’s strength and ability at that moment. At the time of discharge from physical therapy, the patient ambulated 40 feet with contact guard assistance, gait belt, and use of the walker.
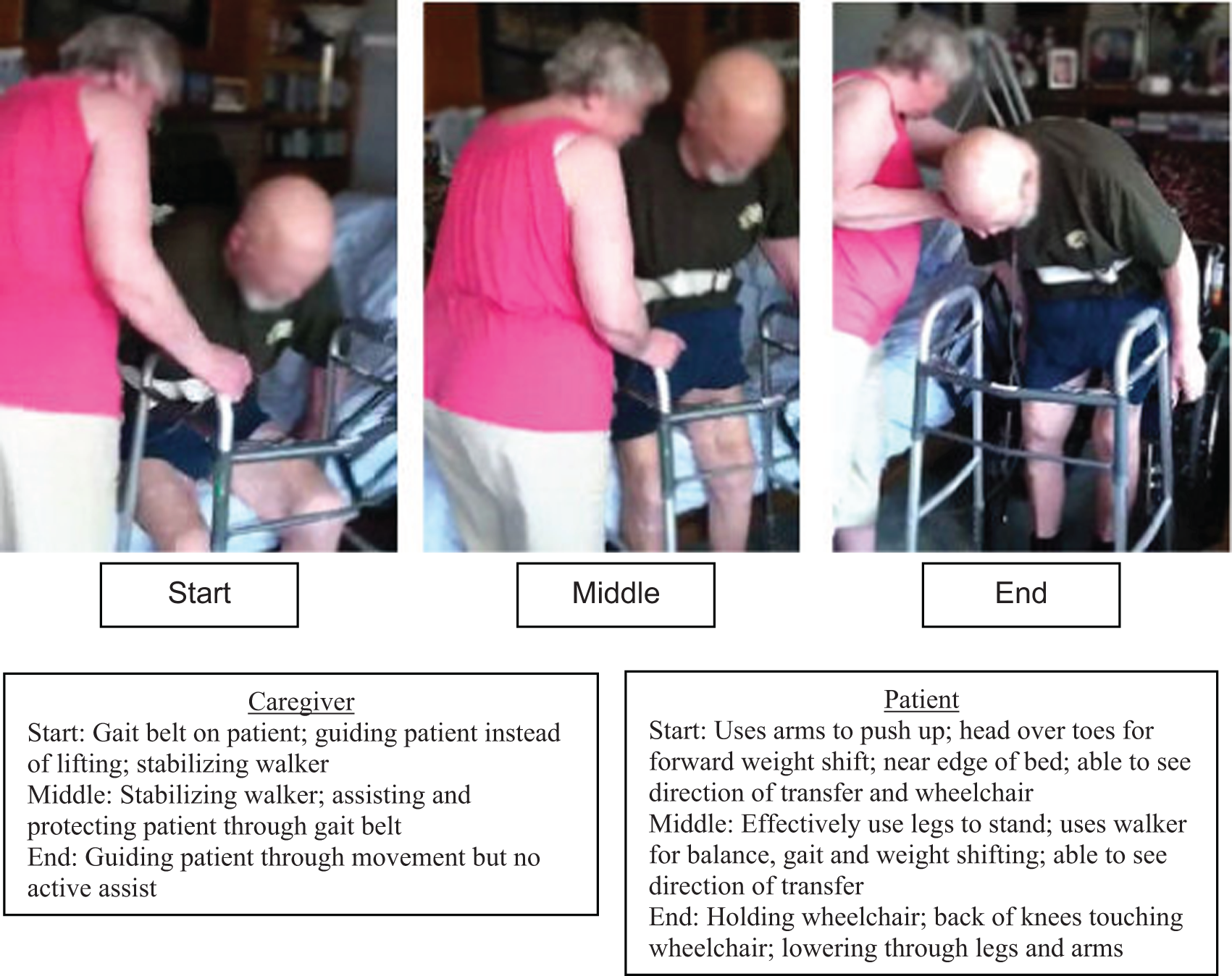
Images of the start, middle, and end of a transfer performed during the final treatment session with a brief listing of correct transfer techniques by the patient and the caregiver.
The McGill Quality of Life Questionnaire (MQOL) was provided for the patient to answer pre- and posttherapeutic intervention. 11 The patient’s MQOL score changed from 66 to 100 after therapeutic intervention was completed. The MQOL scores are calculated inversely, a higher score indicating the lower the QOL. 12 Although a minimal detectable change has not been established for the MQOL, an increase of 40 points does indicate the patient’s QOL decreased.
The caregiver’s assessment of her burden was evaluated with a caregiver strain questionnaire. 13 The caregiver strain index identifies a positive score of 7 or greater to be indicative of the need for further assessment to determine appropriate intervention. 14 Before therapy services, the patient’s wife rated her strain as a caregiver at 10/12. After physical therapy services, her score decreased to 9/12. Her response to the question regarding physical strain improved after physical therapy intervention. The patient’s wife was advised, by the physical therapist, to request a physical therapy referral when transferring the patient became more difficult. Further caregiver training may be indicated as the patient’s function declines and he becomes more dependent.
Patient Reported Benefits of Therapy
Both the caregiver and the patient expressed immense gratitude for the physical therapy provided. The caregiver stated the physical therapy “made all the difference” in how she moved the patient. “Without the physical therapy instruction, someone was going to get hurt. It took away the fear,” she reported.
The patient stated, “The benefits were immeasurable.” He had “more confidence” in his abilities, after physical therapy instruction and intervention.
Discussion
The purpose of this case study was to identify the skilled physical therapy services needed for a patient on hospice with a fear of falling. The skilled services of a physical therapist are often underutilized or overlooked in the hospice setting. Physical therapy was provided for this patient and caregiver, which focused on decreasing the risk of falls and safety during transfers. Although the patient’s general health declined, his risk for falls and fear of falling decreased, and his confidence with transfers improved. He improved in strength and functional mobility, safety for both the patient and caregiver improved, and the caregiver’s burden was greatly reduced. During this episode of care, the patient’s risk of falling was significantly reduced, with his Tinetti score improving from 9/28 to 16/28. 9 This is greater than the minimal detectable change of 5 points established for the Tinetti Balance and Gait Assessment. 15 The patient’s FES-I score improved by 1 point; however, the minimal detectable change for the FES-I has not been established.
As indicated by the MQOL, the patient’s QOL decreased. Upon discussion with the patient and the patient’s wife, they both concurred that the overall decline in QOL was likely due to his gradually increasing respiratory problems. Although his safety and functional mobility improved during this episode of physical therapy, the patient’s perception of his QOL declined. It is possible that the MQOL is not the most appropriate survey to identify improved QOL from a functional mobility perspective.
Physical therapy services assist to alleviate caregiver burden by training the caregiver how to safely assist the patient with bed mobility, transfers, and gait. Instruction in positioning of the bedridden patient can prevent skin breakdown. Physical therapy helps preserve the patient’s highest functional mobility by training both the patient and the patient’s caregiver. Physical therapists can make recommendations for necessary adaptive equipment to maximize patient safety in the home. Specific patient and caregiver concerns are addressed to help the patient maintain dignity and the highest QOL. Each hospice patient and caregiver has individual needs and the hospice team should carefully evaluate and address each situation appropriately to provide the highest level of care. Safety for both the patient and caregiver must not be overlooked or minimized.
Limitations
This was a single case study and cannot be extrapolated to all hospice patients. A simple measurement tool to rate the confidence of the patient and caregiver with transfers is needed for use in a home setting. All confidence scales related to functional activities rated self-confidence with tasks more advanced than household transfers. Consequently a simple bipolar scale was utilized to rate confidence with transfers.
The role of physical therapy in the hospice setting is still emerging. There is a need for more research in this area to educate the medical field, third-party payers, and the general public, on the immeasurable benefit that physical therapy can provide for individuals who are approaching the end of their lives. Additional outcome measures are needed to assist a hospice worker in rating functional ability and confidence levels for both the patient and the patient’s support system.
Conclusion
Although an individual’s condition may be terminal, every person deserves the highest QOL until the end. Physical therapists have a unique opportunity to improve the safety and QOL for both the patient and the caregiver at a very critical time. This case study is an example of how beneficial the skilled services of a physical therapist can be in the hospice setting for the patient and the caregiver.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.