
Abstract
A hospice and palliative care (PC) bed was created in 2006, located within a quiet area of our intensive care unit, in order to admit terminally ill patients sent to the emergency department (ED) for end-of-life care. We retrospectively analyze the records of the 342 terminally ill patients sent to the ED from 2007 to 2011. Among them, 176 (51.5%) were admitted to our hospice and PC bed, where 114 died. Besides, 99 (28.9%) of them died on stretchers in the ED. Our intervention led to a significant decrease in the number of terminally ill patients dying on stretchers in the ED. It also allowed both patients and families to have access to a more suitable environment.
Introduction
Since the year 2000, a constant increase in the number of emergency department (ED) admissions for end-of-life care has been reported in the international literature. 1 –6 This has been particularly well reported for patients with cancer or aged patients in several countries such as United States, Canada, Australia, and France. 6 –12 Despite both the development of palliative care (PC) consults in ED and the increasing number of hospice and PC beds in acute care departments, reports also show that patients with cancer and aged patients spend a considerable time in ED before being transferred to an inpatient unit or to a PC bed, which may not be immediately available. 13,14 Finally, patients and family caregivers, as well as most emergency clinicians and nurses, agree that the ED is neither a convenient place to receive adapted palliative and hospice care nor a decent place to die. 11,12,15,16
In 2002, we reported 8 that 35% of the adult patients dying on stretchers in the ED of our university hospital were at the terminal stage of a cancer or of a neurological, cardiac, or respiratory chronic disease. We estimated that these deaths occurred in unacceptable conditions, due to the inappropriate environment of the ED for end-of-life care and to the lack of skills in palliative and hospice care of the ED staff. In December 2006, we obtained from the health national authorities the agreement to settle within our intensive care unit (ICU) a palliative and hospice care bed specifically dedicated to the ED. Our purpose was to improve the quality of both PC and the end-of-life conditions of patients at the terminal stage of a chronic disease sent to the ED. We report here on the first 5 years of this experience.
Settings and Methods
The ED of our French university Hospital receives 41 600 admissions per year. The inpatient Palliative Care Unit (PCU) includes 19 beds, distributed in several units. The main PCU (8 beds) is located 6 miles away from the main building of the hospital and thus from the ED. Our adult ICU is closely linked with the adult ED. It includes 16 beds, receives 1100 admissions per year, and is managed by 5 intensivists. In December 2006, the ICU obtained the agreement for 365 annual days of PC dedicated to ED patients at the terminal stage of a chronic disease, who could not be sent to the PCU because of a lack of available beds within a reasonable delay. No additional physical bed was created in the ICU, and PC was given without additional staff. Palliative care was provided by intensivists, with the constant support of the PCU team. An inward formation in PC was organized for the paramedical staff of the ICU. Moreover, a university graduation for PC was obtained by some nurses of the staff. Part-time physiotherapists, dieteticians, and psychologists, who already belonged to the staff of the ICU, were asked to participate in the PC. The PC bed was located in a comfortable room, at a quiet end of the department. In 2009, a private room—including a bedroom and a bathroom—was created for the families within the nonmedical area of the ICU, and a permanent access to the patient was organized for close family members, relatives, and officers of religious cults.
In order to evaluate the effectiveness of our intervention, in terms of reduction in the rate of terminally ill patients dying on stretchers in the ED, we made a retrospective analysis of our PC activity, from January 1, 2007, to December 31, 2011. For this purpose, we included all the patients admitted during this period to the ED, presenting either at the terminal stage of a chronic disease or with an acute lethal condition occurring in the context of a terminal chronic disease. Identification of the population of the study was performed from the institutional database of diagnosis coding (Programme de Médicalisation du Système d’Information) of our institution. In accordance with French legal recommendations on biomedical research, this retrospective study was exempt of necessity of approval by the local institutional review board, as it was neither causing any privacy violation nor leading to any intervention or treatment modification, for the patients included. A strict accordance to the Helsinki Declaration guidelines was observed by the authors. Patients at a terminal stage of an acute lethal condition without the context of an underlying terminal chronic disease were not included in the study. The records of all terminally ill patients, admitted from the ED to the ICU for PC, were reviewed. The terminal stage of a chronic disease was identified through medical evidence, in patients having a known and advanced chronic lethal disease, with no possibility of curative treatment and presenting with 1 or more major organ failure. For each patient, the confirmation of the terminal stage of the chronic disease was obtained by the consultation of at least 2 physicians, among whom the patient’s regular practitioner, or the specialist in charge of the chronic disease. The following data were extracted: age, sex, usual place of residence, type of chronic pathology, modalities of former care (active or palliative), knowledge (for patient and relatives) about the terminal stage, Palliative Performance Score (PPS) on admission, type of person referring the patient to the ED, cause of admission and type of care requested, length of stay in the ED, consultation of the physicians in charge of the chronic pathology, modalities of care in the ED and in the ICU, outcome, and stay mean duration in ICU. In parallel, we analyzed the outcome of the terminally ill patients admitted to the ED, who could not be admitted to the ICU for PC.
Results
During the study period, 5720 patients were admitted to the ICU and 208 155 to the ED. A total of 342 terminally ill patients were admitted to the ED; among them, 67 (19.6%) were transferred to the PCU, 99 (28.9%) died on stretchers in the ED, and 176 (51.5%) were admitted to the ICU PC bed (Figure 1).
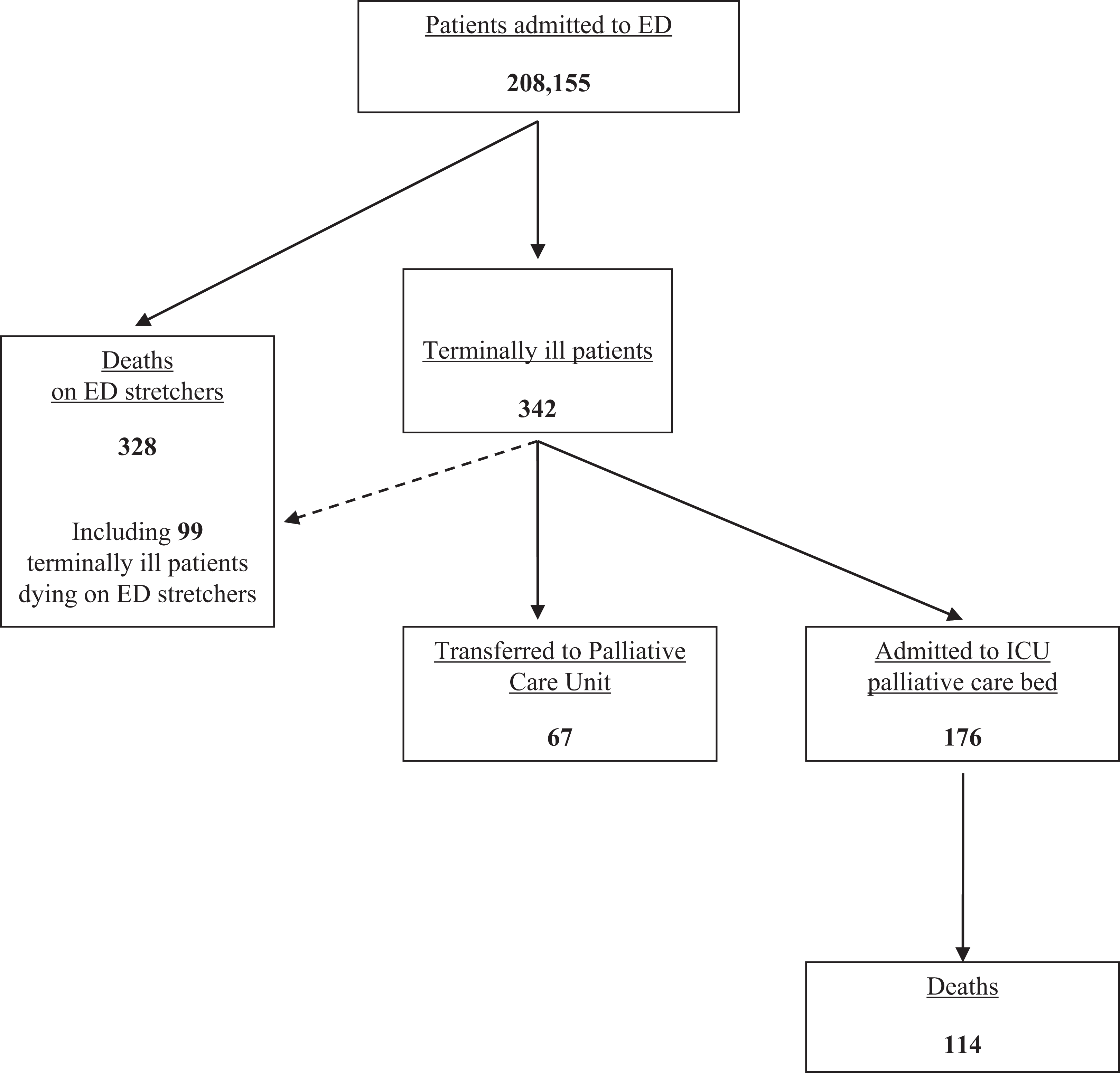
Outcome of the terminally ill patients admitted to emergency department (ED).
The main characteristics of the 176 patients admitted to the ICU for PC are displayed in Table 1. Mean age was 72 years, sex ratio 103 male–73 female; and mean PPS on admission was 39.5 (PPS 10-30: 80 patients [45.4%], PPS 40-50: 70 patients [39.8%], PPS 60-70: 22 patients [12.5%], PPS 80-100: 4 patients [2.3%]). The advice of the regular practitioner or of the specialist in charge of the chronic disease was obtained before admission for 74.4% (131 of 176) of patients and for 100% within 24 hours of admission to the ICU. During the time spent in the ED before admission to the ICU, inappropriate life-prolonging procedures were initiated in 29.5% (52 of 176) of patients. Analgesic medications were prescribed in 100% of patients and initiated in 41.5%; anxiolytic medications were prescribed in 84.7%. The mean length of stay of these patients in the ICU was 5.3 days, and 64.8% (114 of 176) of them died within a mean delay of 2.7 days.
Main Characteristics of the Patients Admitted to ICU Palliative Care Bed.
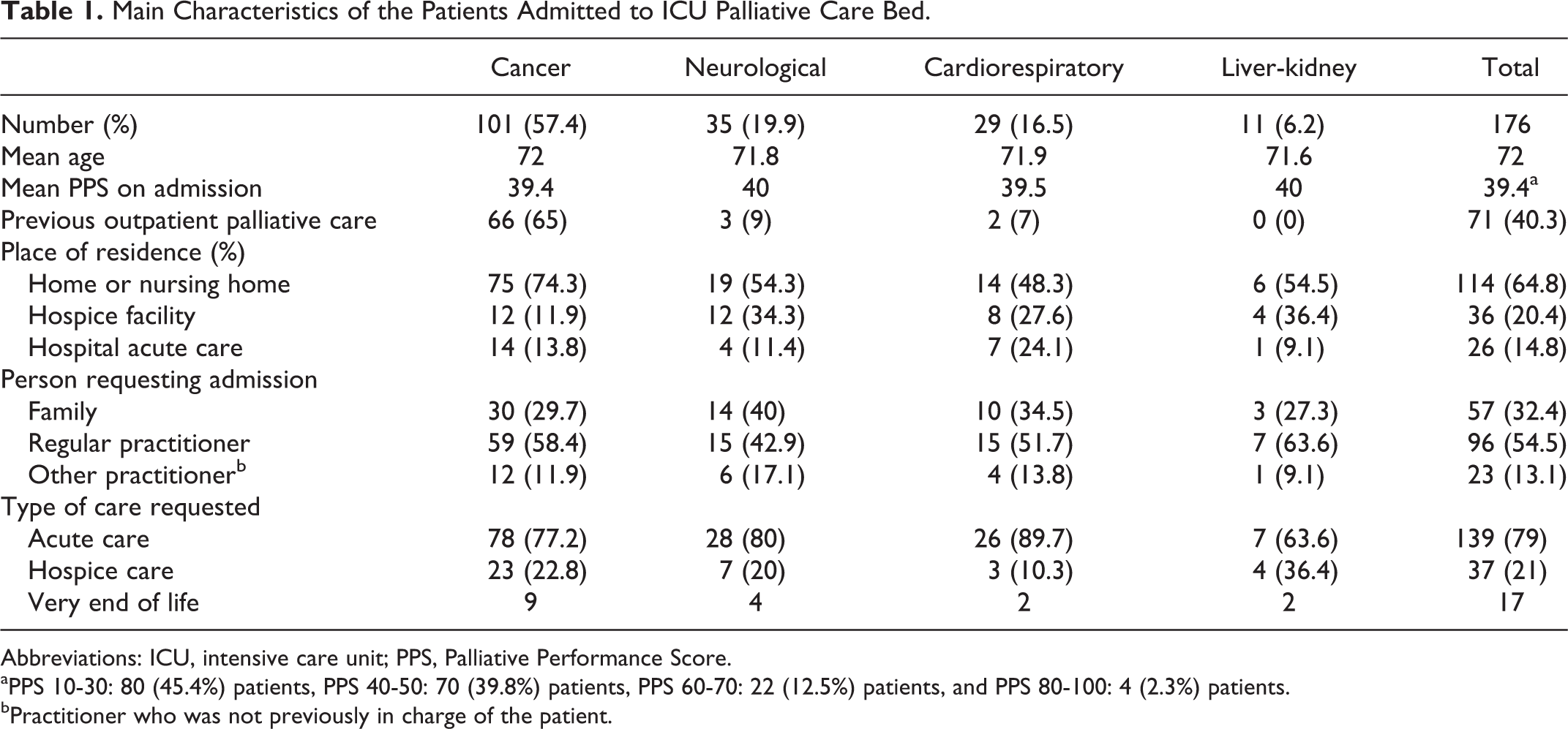
Abbreviations: ICU, intensive care unit; PPS, Palliative Performance Score.
aPPS 10-30: 80 (45.4%) patients, PPS 40-50: 70 (39.8%) patients, PPS 60-70: 22 (12.5%) patients, and PPS 80-100: 4 (2.3%) patients.
bPractitioner who was not previously in charge of the patient.
Concerning the outcome, 64.8% (114 of 176) of patients admitted to the ICU for PC died, 14.2% (25 of 176) were subsequently transferred to the PCU and 11.4% (20 of 176) to the medical departments previously in charge of their chronic disease. Seventeen (9.6%) patients were finally discharged back home or to their previous nursing/hospice facility. Since its creation in 2009, the family room was occupied with a rate of 50%.
Discussion
Despite large programs of public health, developing palliative, and hospice facilities, these structures are underutilized 1 and more and more patients are sent to ED at the end of their life. 2 –7,11,12 As soon as 2002, we reported 8 that 35% of patients dying on stretchers in the ED of our university hospital were at the terminal stage of an incurable disease, and we raised concerns upon the respect of dignity of these dying patients. We decided to create a specific device, night and day closely connected with the ED, in order to give these patients specific palliative and hospice care and to respect the intimacy of both patients and families. As our purpose was to reduce the number and rate of terminally ill patients dying on stretchers in the ED, we consider that our intervention was successful. Indeed, among all the patients who died within the ED during this 5-year period, the rate of those sent to the ED after months or years of an incurable disease decreased from 35% in 2002 to 30.2% (99 of 328). Moreover, 51.5% (176 of 342) of the terminally ill patients admitted to the ED during this period were transferred to the ICU PC bed, where they received adapted hospice care and where their families and relatives were welcomed in a more decent way. We can also reasonably imagine that, without our intervention, the 114 terminally ill patients initially sent to the ED and who died in the ICU would probably have died in the ED; thus, the rate of terminally ill patients dying on stretchers would have been as high as 48.2% (99 + 114/328 + 114). Even if this type of organization may differ from an ED to an another, we believe that PC beds dedicated to ED must at least (1) be assigned essentially to end-of-life care of terminal ill patients, (2) be located very closely to the ED, to avoid both delayed transfer and long duration of transportation, (3) be located in a silent and comfortable area, (4) be able to admit patients round the clock, 7 days/wk, (5) be able to give appropriate palliative and hospice care, with staff trained for this activity, and (6) be equipped or connected with hosting facilities for patients’ relatives. Moreover, as the number of terminally ill patients who died on stretchers in the ED remained as high as 99, we believe that the number of PC beds dedicated to each ED has to be adapted with the ED activity.
Finally, it may be interesting to evaluate in future studies whether such devices improve the feelings of patients and families, as well as those of ED nurses and clinicians, and whether it decreases the time spent by these terminally ill patients on ED stretchers.
Conclusion
A palliative and hospice care bed specifically devoted to the ED allowed a significant decrease in the number and rate of terminally ill patients dying on stretchers in the ED. It also probably bought a substantial benefit, in terms of quality of both care and environment, to these patients and to their families.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.