
Abstract
Context:
Pain management (PM) has not been routinely incorporated into HIV/AIDS care and treatment in resource-constrained settings.
Objectives:
We describe training for multidisciplinary teams tasked with integrating care management into HIV clinics to address pain for persons living with HIV in Nigeria.
Methods:
Education on PM was provided to mixed-disciplinary teams including didactic and iterative sessions following home and hospital visits. Participants identified challenges and performed group problem solving.
Results:
HIV trainers identified barriers to introducing PM reflecting views of the patient, providers, culture, and the health environment. Implementation strategies included (1) building upon existing relationships; (2) preliminary advocacy; (3) attention to staff needs; and (4) structured data review.
Conclusion:
Implementing PM in Nigerian HIV clinics requires recognition of cultural beliefs.
Introduction
Since 2001, new infections from the HIV have declined by 25% worldwide, yet an estimated 23.5 million people remain infected in sub-Saharan Africa representing 69% of the global HIV burden. 1 In all, 60% to 90% of persons living with HIV (PLWH) disease regardless of stage of illness or degree of viral control 2 –4 have been documented to have pain. It is frequently underdiagnosed and consequently unmanaged. 5 Moderate to severe pain intensity negatively impacts daily function and overall quality of life. 6,7 The expression of pain is subjective, reflecting personal and cultural attitudes of both providers and patients, thus impacting accurate interpretation and clinical management. 8,9 Unmanaged pain, a major global health care problem, 10 may result from disease progression, side effects of disease management, or be caused by unrelated problems in both adults and children. 11 –13
Guidelines for HIV management promoted by the World Health Organization (WHO) are public health measures that do not address individual care management. Clinical management strategies can be systematically applied once existing local challenges are clarified. 21 Faced with limited health resources, diverse languages, and embedded cultural beliefs, African HIV clinics are yet to focus upon patient-level problems requiring complex communication skills. 14,15,23 Yet pain management (PM) strategies were introduced almost 40 years ago when the WHO recognized a nominal need in resource-constrained countries to address the control of cancer pain, despite the lack of availability of advanced disease management modalities. 16
The “analgesic ladder” was proposed as a mechanism for approaching PM 17 and efforts to improve access to opioids for PM. A 2001 study in West Africa documented only 18% of surveyed physicians being aware of this “by-the-clock” dosing algorithm recommended for pain control. 18 The African Palliative Care Association, supported by multiple international hospice and palliative care (PC) organizations, facilitated pain advocacy workshops for teams from 17 African countries to stimulate improved regulations that might inhibit the medicinal use of opioids. 19 The WHO advanced these efforts by developing online courses for improving international opioid access and use (www.painpolicy.wisc.edu). Despite availability of effective training materials, PM remains inaccessible in many settings because of poor access to medications. Effective PC reflects an interdisciplinary team assessment to improve survival and quality of life in both patients with cancer and patients with HIV when pain and other symptoms are addressed. 20,21 Teaching methods for introducing PM must differ from those traditionally used for the basic sciences as the personal experience of the learner may impact the ability to learn. Published core competencies for teaching PM cite 3 critical elements: (1) necessity for interprofessional education relative to the multidimensional nature of pain itself; (2) methods for pain assessment and measurement; and (3) clinical skills needed for the management of pain. 22 Addressing this range of issues can be time consuming but omitting the clarification of cultural complexity may inhibit future success in symptom control. 20
This article describes an iterative training intervention, in Nigeria where cultural acknowledgement of the existence of pain may be a primary barrier to full implementation of PM for PLWH. This training was made possible by the US President’s Emergency Plan for AIDS Relief (PEPFAR) now operating in over 30 countries worldwide and aimed to introduce HIV care and treatment strategies to change the course of the epidemic in countries without uniform access to antiretroviral therapy (ART). Since initial implementation activity, strengthening of health infrastructure has become a major focus.
Methods
Setting
Nigeria is located in Western Africa covering 120 000 square miles (about the size of New Mexico) with an HIV prevalence of 3.7% to 4.7%. The most populated African country with over 5 basic languages and up to 364 dialects being spoken across a major land mass is a multicultural society based on tribal divisions that will be referred to in this article. True understanding of cultural attitudes would require stringent surveys targeting all ethnic and religious groups. This article represents in-depth discussions with a mixed-discipline group of HIV care and treatment technical assistance experts with 6 to 7 years experience in implementation of ART in rural faith-based clinic settings in southern Nigeria.
Within the context of implementation of HIV care and treatment in underresourced countries, we introduced PM as an implementing partner (IP) of the US PEPFAR program. 23 The stated goal of this IP was to promote durable viral suppression in each person initiating ART. The IP employed multidisciplinary clinical mentoring to enroll 500 000 PLWH in care and support activities across 240 treatment sites where more than 240 000 people initiated ART in 7 African and 2 Caribbean countries. Local clinical training teams were mentored to introduce care and treatment issues across the continuum of HIV illness. The training model used was a typical train-the-trainer approach followed by on-site clinical mentoring at care delivery sites. Guiding principles included (1) use of a patient- and family-focused approach that included home or community visits to reinforce adherence; (2) introduction of chronic, rather than acute, care delivery with continuity across the continuum of illness; (3) implementation of a sound laboratory infrastructure; and (4) the ongoing use of data to develop and improve care delivery. Individual quality of life was the promoted goal.
Within the IP program in Nigeria, 12 rural clinics provided ART to 6603 individuals in 2010, with a representative sample having a measured viral suppression rate of 85% after patients had been using ART for 9 to 15 months. 24 These sites received targeted education relative to adult and pediatric ART management that included an operational approach to delivery of clinical services, laboratory support, data collection and management, and care and support issues for individual patients and staff.
Resource-constrained settings may offer additional challenges to PM including (1) diverse cultures with potential conflict among persons of different ethnic origin; (2) significant poverty limiting access to effective treatments; and (3) traditional, hierarchical behaviors perpetuating top-down provision of care with expectations of physician-only leadership. Despite having initiated community-based treatment adherence methods, bias remains that medical issues are the purview of physicians. Task shifting is being used to share the burden of care across disciplines in many African settings but it does not, in practice, offer an interdisciplinary experience. 25
Interprofessional Education
“Care and support” is the term employed by the US government to represent the palliative approach. 25 To introduce care and support topics within this context, local program managers appointed a central focal team to be mentored as leaders for future activities. Care for patients was 1 of the 4 targeted funding strategies with PC defined as care needed by those as yet to receive ART or in need of linkage with other services. 26 In the Nigerian program, following a 5-day general introduction to the palliative approach to care, the IP program managers selected to introduce 3 specific topics regionally. To evaluate potential challenges to integration, “PM,” “mental health issues,” or “end-of-life care” were introduced in each of the 3 internal regions.
An external international educational team with 2 physicians, 1 nurse, and 1 social worker (community-based treatment supporter), all experienced in PM for patients with HIV in the African context, provided the training. One physician was a pain specialist from a different geographic region of Nigeria. In a 5-day capacity-building workshop, the training team reviewed prepared case presentations and participated in small group, home, and hospital visits for patients experiencing pain. Didactic PM presentations utilized this shared experience for discussion. Identification of diverse cultural beliefs regarding the experience of pain in Nigeria occurred throughout the teaching sessions. After the workshop, the focal and regional teams developed a pilot initiative. The Results section describes the educational experience and insights gained through the process.
Following a 1-week, program-wide introduction to palliative concepts for selected HIV trainers, 18 mixed cadre staff members were chosen to participate in a 1-week iterative workshop on PM. This geographic team included 6 physicians, 6 nurses, 3 community-based treatment supporters, 2 laboratory technicians, and 1 psychologist without prior PM training. There are at least 5 major languages spoken in Nigeria with Igbo being the primary language spoken throughout the South East Region where this training took place. Participants in the workshop spoke Igbo (15), Edo (1), Igala (1), and Yoruba (1), reflecting the general population of this region. In general, participants had little prior exposure to assessing and managing psychosocial problems in the medical setting. All participants spoke English.
Standardization of Clinical Material
To assure that learners share exposure to clinical material, we made multidisciplinary home and hospital visits to patients with identified pain problems. In all, 6- to 7-member teams visited the home of 2 patients while a third team participated in a family meeting with a hospitalized patient. During 1 home visit, participants were exposed to extreme poverty and in the other 2 patient encounters, the targeted patient had abandonment as a result of HIV stigma. These exposures raised emotional reactions in learners who are beyond the scope of this document. In this article, we describe the process and outcomes of a workshop meant to enable the introduction of PM for PLWH in 1 region in Nigeria that may have application in other resource-constrained settings.
Qualitative Interventions
The iterative educational intervention incorporated diverse training approaches to identify information and formulate the conclusions reached. An exhaustive survey of Nigerian culture was beyond the scope of this training. The principle author of this article served as primary facilitator. The local pain expert presented didactic material. The international training team met with the local focal team daily to review response to material to plan and modulate the next day’s activities. This interaction between instructors and students was at the core of the qualitative information collection and formulation of conclusions. Learners acted as experts in local culture and as interrogators of concepts presented in class. Observations offered in this article arose during focused discussion with participants. The authors refined these observations through a discursive process that included the preparation of this article.
Results
Prior to the workshop, multiprofessional training teams were assigned to geographical regions but tasks remained largely discipline specific. Goals of the workshop included (1) to review the HIV care and support continuum of illness as a framework for understanding patient needs throughout the illness; (2) to observe current PM approaches, through the eyes of the selected professional learners, using case discussions, chart reviews at visited sites, and home, clinic, or hospital visits with patients experiencing pain; (3) to conduct small group discussions regarding PM by discipline and as multidisciplinary groups; (4) to review with the focal team daily proceedings to improve and target next day activities; (5) to integrate care for care providers as one mechanism for sustaining the current workforce; and (6) to clarify next steps for the focal team. This iterative workshop introduced concepts to participants not routinely considered in HIV care delivery: (1) need for appreciation of the patient’s living circumstance as having an impact upon patient behaviors relative to adherence and long-term outcomes; (2) the concept of “total pain,” an existential appreciation that the experience of a symptom may be significantly influenced by issues not directly related to the problem; and (3) clarification of the contribution of health workers of diverse cadres for expanded understanding of patient needs.
For members of this training team, the workshop represented a first experience of working as an interdisciplinary team. Table 1 documents potential plans for integration of PM by discipline-specific teams. After reviewing local clinic charts, learners found that current intake forms did not identify pain as an HIV problem. Headache was recorded as an indicator of infection but not interpreted as a pain problem. Sensitization to pain as a problem, use of discipline-specific severity assessment methods, and describing availability of medications for PM were considered essential next steps before introducing clinical skills. During the PC training, learners demonstrated a high degree of personal loss relative to the HIV/AIDS epidemic that could impact their professional development in PM.
Challenges to Introducing Pain Management in HIV Treatment Sites.
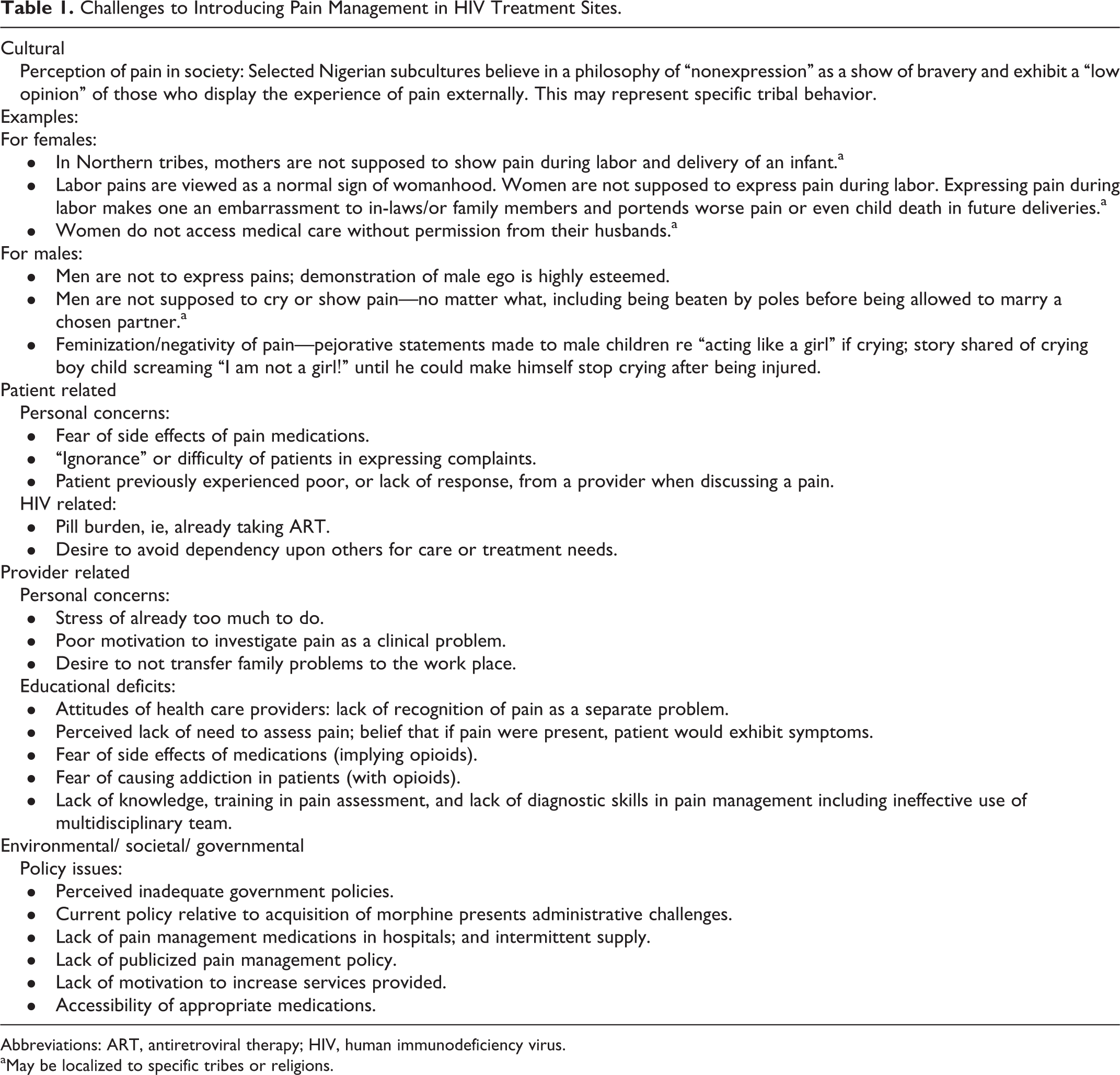
Abbreviations: ART, antiretroviral therapy; HIV, human immunodeficiency virus.
aMay be localized to specific tribes or religions.
The full interdisciplinary team identified barriers to implementation of PM as a routine component in HIV management in 1 southeastern region of Nigeria in 3 areas: (1) differences in professional training that produce discipline specific rather than interdisciplinary approaches to patient care (Table 2); (2) the impact of poverty and lack of resources including uniform access to pain medications (Table 3); and (3) cultural beliefs and practices that discourage both patients and providers from admitting to the presence of pain (Table 1). Discipline-specific health teams preferred different pain assessment tools and approaches for introduction of PM. These HIV trainers identified 64 barriers across 4 categories to introducing PM into routine HIV care and treatment. During the workshop, they participated in collective problem solving and identified low-cost mechanisms for introducing PM.
Discipline-Specific Integration of Pain Management With ART Care and Treatment.
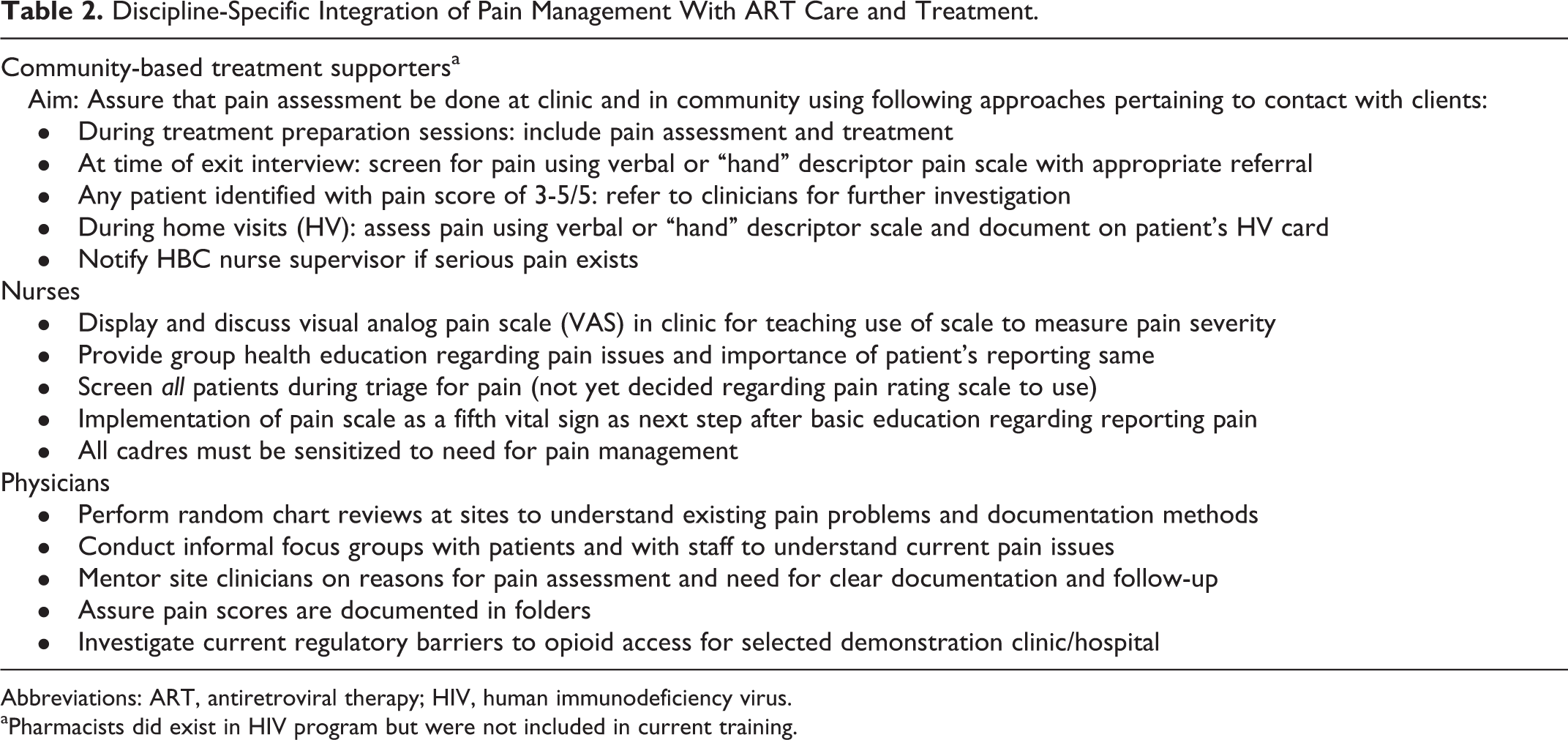
Abbreviations: ART, antiretroviral therapy; HIV, human immunodeficiency virus.
aPharmacists did exist in HIV program but were not included in current training.
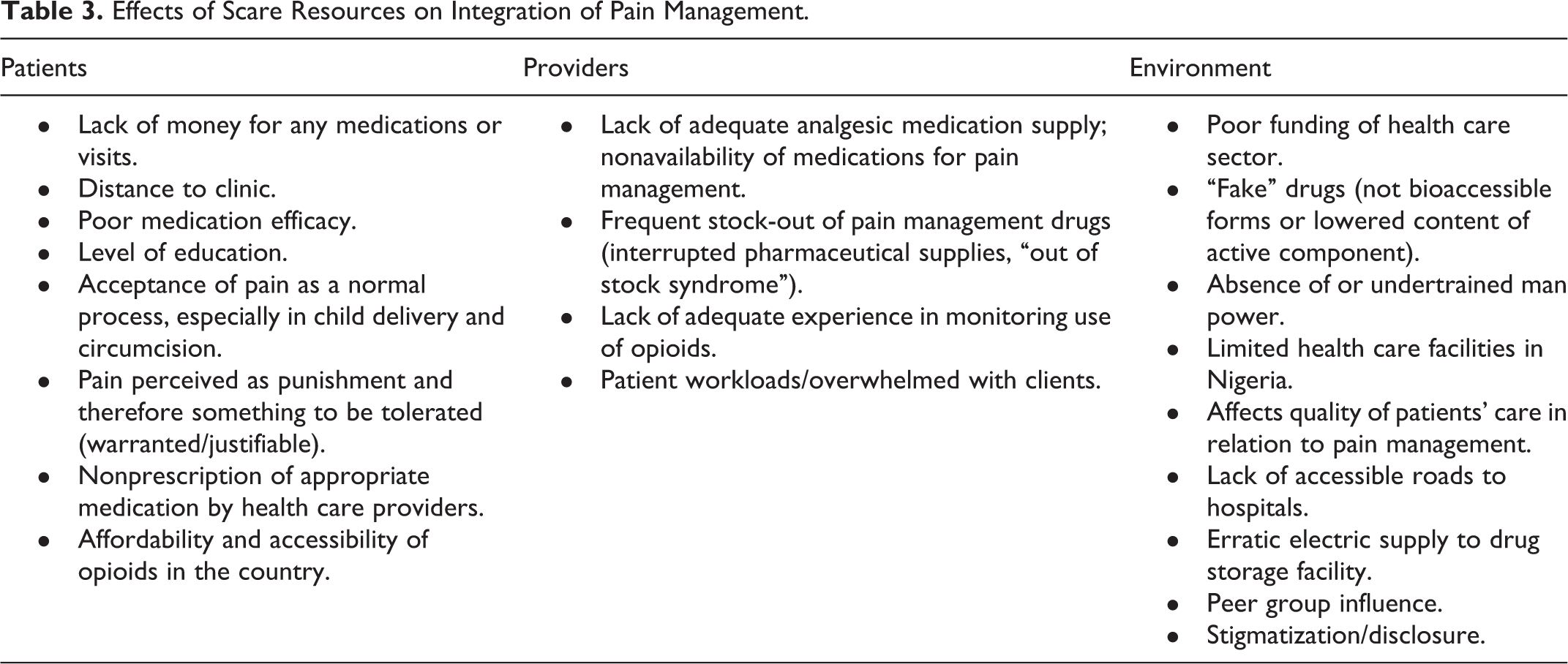
Effects of Scare Resources on Integration of Pain Management.
Potential Challenges to Integrating PC With HIV Care and Treatment
Under funded clinical care and poverty
During the workshop, group discussion revealed that participants perceive that poverty itself limits the potential for high-quality health care delivery (see Table 2). Poverty was identified as an overarching barrier to the introduction of new areas of clinical intervention in by those who participated in the training. Health care is underfunded and staff members perceive external limitations such as erratic electricity supply and poor roads to oppose optimal health care delivery. Staffing vacancies and lack of advanced clinical training are apparent in the workforce. Uneven production controls or lack of availability of medications is the norm. Providers are overwhelmed by the daily workload 27 and have little experience with focusing upon pain itself as a problem to be managed. Opioids are believed by many providers to be confined to teaching institutions. Workers are accustomed to working around these issues.
Poverty observed in the living conditions of the patients was also identified as a challenge to PM. Patients cannot afford to purchase medications and pain has evolved to be accepted as a normal part of living. Poverty is closely associated with persistent stigma surrounding HIV disease. Economic, educational, and social differences between the health workers and their patients became a significant issue during the training, revealed most acutely during home visits.
Cultural barriers
There is a widespread cultural belief in stoicism, which maintains an external demonstration of strength without display of emotion as the desired behavior for both men and women. The statement “to show pain is to demonstrate weakness” seems pervasive in some Nigerian tribal beliefs and practices as represented in this workshop regardless of actual tribe of origin. Facial expressions are expected to remain controlled or “nonexpressive.” Crying or outward expressions of pain are not acceptable and children learn this from an early age.
Patient and provider concerns
Prior to these mentored visits, providers believed that patients would resist taking pain medications because of their existing HIV “pill burden.” Patients were observed not to express feelings during clinical interactions and trainers believed that they may have had a prior negative experience with a provider leaving them reluctant to discuss their symptoms. Observed provider-related barriers to recognition and management of pain included noting that health workers have limited time with individual patients and seem uninterested, or not motivated, to understand patient problems. The trainers attributed this to lack of knowledge about PM and a fear of precipitating addiction, or diversion, of medication. Trainers noted that providers routinely failed to solicit patient input with regard to the patient’s experience of the pain.
Discussion
Nearly 40 years have passed since PM was identified as a critical intervention for persons with life-threatening illness yet individuals have lack of implementation of basic strategies. 28 Within diverse African countries, stigma relative to HIV disease itself and a reluctance to recognize the impact of pain as a problem combine to represent potent barriers to implementation of effective PM. Where multiple languages and religions may obscure the outward expression of pain experienced by any individual, cultural beliefs and practices must be clarified and systematically addressed to achieve effective PM for persons with HIV disease in resource-constrained settings.
Cultural issues related to self-sufficiency and stoicism in Nigerian cultures may inhibit members of specific cultures from acknowledging that pain exists resulting in inadequate training and implementation of services. In Nigeria, beyond literature cited in obstetrics and dentistry, little exists relative to the pain experience of nonsurgical patients. Although ethnicity and perception of pain have been addressed, no clear patterns have been documented. 30 One convenience sample from an HIV clinic in the middle belt of Nigeria documented 79 persons with pain but noted that patients may be “resigned to fate and believed that pain is part of the symptom complex” resulting in an underreporting of pain. 30 Another recent report addresses screening for mental health issues such as depression and alcohol use but fails to evaluate pain as a symptom. 31
The training described in this article integrated tribal beliefs and practices (culture) into educational considerations for introducing complex clinical topics; palliative medicine as a discipline addresses many of these topics including PM, mental health issues, and end-of-life care chosen by the Nigerian management team as necessary to be addressed in delivery of HIV care and treatment. Despite recent documentation to the contrary, 29 a poorly funded health sector does significantly impact the ability to introduce alternative clinical practices such as clinical teamwork, identification of staff bias in care delivery, and availability of time for full interview for patients with psychosocial or spiritual factors that influence medication adherence or other health behaviors. Learners in resource-constrained settings may not have appropriate experience or context for incorporating such skills.
Direct observation as experienced with on-site mentoring is 1 method for introducing these skills. The educational exercise demonstrated that patients with HIV disease experience unrecognized pain. It may be critical to understand the range of existing cultural beliefs and what efforts are needed for addressing them prior to introduction of widespread PM. Staff members need ongoing mentoring to assure that observations accurately reflect patient problems; measurement tools are used correctly; and documentation is effective. Team care, often believed to be too costly in resource-constrained settings, deserves an on-site evaluation when introducing complex clinical skills.
Management of pain depends upon (1) awareness that this widely experienced symptom warrants clinical attention; (2) serial educational efforts targeting concerns of each cadre of health worker and consumers; and (3) assurance of an effective supply of relevant medications, including opioids, for control of moderate to severe pain. Health workers in resource-limited settings must address concrete issues of access, affordability of medications, and strong beliefs by providers that addressing pain may not be relevant within the culture. 30 Fear of precipitating addiction or serious side effects of opioids (ie, “opioidphobia”) must be addressed. But it is first critical to appreciate individual, tribal, or cultural beliefs underpinning a societal need for adamant denial of pain as suffering is to be tolerated as a form of punishment. Introducing concepts that require complex communication requires more time than anticipated. Clarification of culture is critical to integration of new concepts. Learners need experienced mentors willing to participate in the discussion.
The major limitation of this program is lack of evaluation or consideration of outcomes. Challenges to implementation of PM in 1 resource-constrained setting originate from patients, health delivery staff, and the environment. Further study is needed to clarify cultural challenges to identification and management of pain in Nigeria. Successful interprofessional education requires that each discipline clarify its unique contribution prior to developing a team approach. Failure to attend to emotional or cultural aspects of care management can manifest as lack of knowledge or experience, professional fears of unintended outcomes, and cultural endorsement of behaviors that refute the problem being addressed.
Conclusions
Pain continues to be a significant stressor for PLWH/AIDS, regardless of stage of illness or access to care and treatment. 27 Personal concerns and educational deficits of health staff were not unlike obstacles identified in western countries since the 1970s when recognition and management of pain became a priority in the United States and other developed countries. 28 Where capacity building regarding health delivery must take precedence over care delivery for individual patients, PM has not been a focus of care delivery. Introduction of PM may evoke barriers ranging from lack of recognition of the problem through need for technical skills building and regulatory adjustments assuring opioid availability and accessibility. Significant barriers exist related to acknowledgement of pain as an actual problem and implementation of management strategies.
Footnotes
Acknowledgments
We thank the patients and staff of clinics in Nigeria for sharing their continued experience in living with HIV/AIDS.
Authors’ Note
This article was first presented as poster #A05-126 at the 32nd Annual Scientific Meeting of the American Pain Society, May 10, 2013, New Orleans, LA, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was made possible through grants from the US Office of Global AIDS Coordinator under the President’s Emergency Plan for AIDS Relief (PEPFAR) in resource-constrained settings and with the US Health Resources and Services Administration (HRSA) and the Centers for Disease Control (CDC).