
Abstract
Introduction:
Resident physicians provide the most physician care to intensive care unit (ICU) patients. The body of literature about residents’ palliative and end-of-life care (PC/EOLC) experiences in the ICU is limited. To our knowledge, this is the first study to assess resident physicians in multiple specialties regarding PC/EOLC in the ICU.
Methods:
A Web-based survey was developed and administered to all resident physicians in a single academic institution who had completed at least 1 dedicated ICU rotation.
Results:
Residents reported moderate comfort in dealing with end-of-life (EOL) issues and felt somewhat prepared to care for critically ill patients at the EOL. Feedback should be provided to residents regarding their PC/EOLC skills, and education should be tailored to residents rotating in the ICU.
Keywords
Introduction
With rapid advances in medical technology, intensive care unit (ICU) use has increased in the recent years. Mortality rates in the ICUs range from 5% to 40%, 1 and more than 20% of deaths—or approximately 540 000 annually—in the United States occur in the ICUs. 2 Do-not-resuscitate orders are increasing, 3 and ICU deaths increasingly involve withholding or withdrawing of life-sustaining therapies. 4 –6 The ICU physicians must provide compassionate care to dying patients and their families to aid in the transition of goals from cure to comfort.
Palliative and end-of-life care (PC/EOLC) in the ICU is thus a growing need. Palliative care is important for symptom management when death is not imminent and becomes indispensable at the end-of-life (EOL). Early and frequent discussions about prognosis and uncertainty are important factors in communication with families about critically ill patients. 7,8 Thus, the initial ICU encounter is an optimal time to initiate discussion about prognosis and possible EOL issues. In teaching hospitals, the initial physician encounter in the ICU is often with house staff such as residents or interns. House staff should be skilled and comfortable in the delivery of PC/EOLC.
Although some studies have been undertaken on PC/EOLC education in trainees, it is a field in need of further study. The PC/EOLC education has been studied in residents in single specialties, 9 –14 all showing improvement in residents’ skills following educational interventions. Surveys indicate that American medical school graduates have low self-perceived comfort with EOL communication and that experience with dying patients contributed more strongly to perceived comfort and skill than classroom teaching. 15 In critical care education, a single-center PC curriculum was designed and implemented for critical care fellows. The program included small group sessions, didactic sessions, and a PC rotation; it led to improvement in both knowledge and attitude. 1 However, PC/EOLC education has not been compared among multiple specialties in the ICU, where educational opportunities may abound.
Overall, PC/EOLC education is an important component of medical training for residents in many disciplines and should not be neglected in the ICU. In teaching hospitals with a wide range of residency programs and specialty ICUs, the PC/EOLC experiences are likely to vary greatly. 16 The purpose of this study was to assess the opinions, attitudes, and experiences of residents regarding PC/EOLC education during their ICU training. To our knowledge, this is the first study to simultaneously assess resident physicians in multiple specialties related to PC/EOLC in the ICU. We hoped to better understand (1) how residents perceive the importance of and need for PC/EOLC education in the ICU, (2) how they rate current PC/EOLC education in the ICU, and (3) how receptive they are to curricular reform.
Methods
Literature review for surveys on PC/EOLC, medical education, and ICU experiences revealed no validated instruments. Survey questions were developed with the assistance of experienced survey designers using previous studies as a guide. 17,18 The study population included all current residents in a single academic medical center who had completed at least 1 month-long dedicated adult ICU rotation in the past 2 years, which included all residents in internal medicine, anesthesia, neurology, and general surgery. The survey was approved by the institutional review board and administered in the last month of the academic year to maximize available patients. A Web-based survey tool (Survey Monkey) was used, and invitations to participate were distributed via e-mail. Although the survey was open, weekly e-mail reminders were sent through the survey tool to participants who had not yet responded. Responses were collected anonymously. Data analysis was performed using the SAS software program. The Likert-type questions were grouped to create 4 composite measures of opinions and attitudes related to (1) family meetings, (2) technical skill in PC/EOLC, (3) prior training in PC/EOLC, and (4) education on PC/EOLC. Initial analysis examined reliability, central tendency, and variability for the 4 composite measures and for the total measure. Stepwise multivariate regression analysis was conducted to examine whether physician demographic data or physician EOL experience was associated with the 4 composite measures. The criterion for variables to enter the stepwise regression model was significance at the 0.05 level; all variables retained in the model were significant at the 0.10 level.
Results
End-of-Life-Care Experiences of Residents
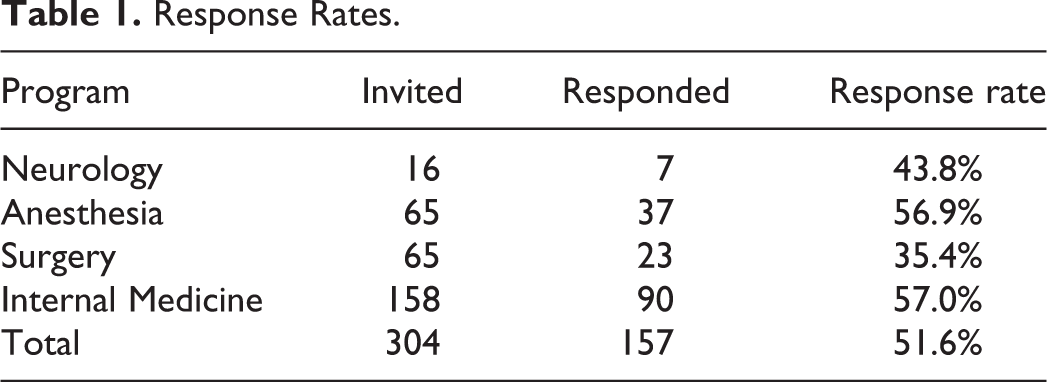
Of the 304 surveys distributed, 162 were returned for a response rate of 53.3%; 5 surveys had missing data resulting in an analytic sample of 157. Response rates were highest for residents in anesthesia and internal medicine (Table 1). Backgrounds and experiences of the respondents varied broadly (Table 2; Figure 1). Most (80%) residents agreed or strongly agreed that the most deaths they have been involved in during residency occurred in the ICU.
Response Rates.
Demographic Data for Respondents.a
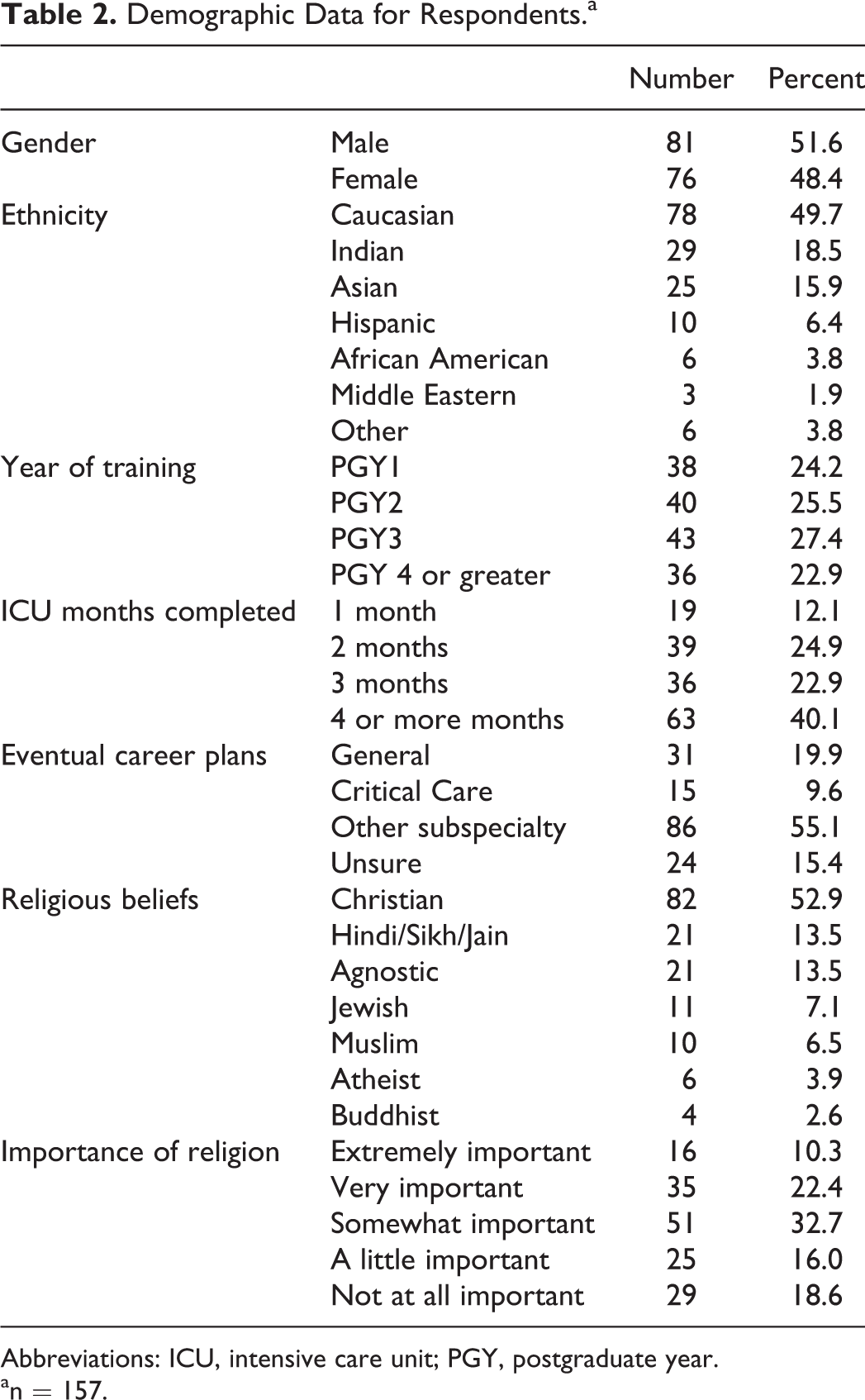
Abbreviations: ICU, intensive care unit; PGY, postgraduate year.
an = 157.
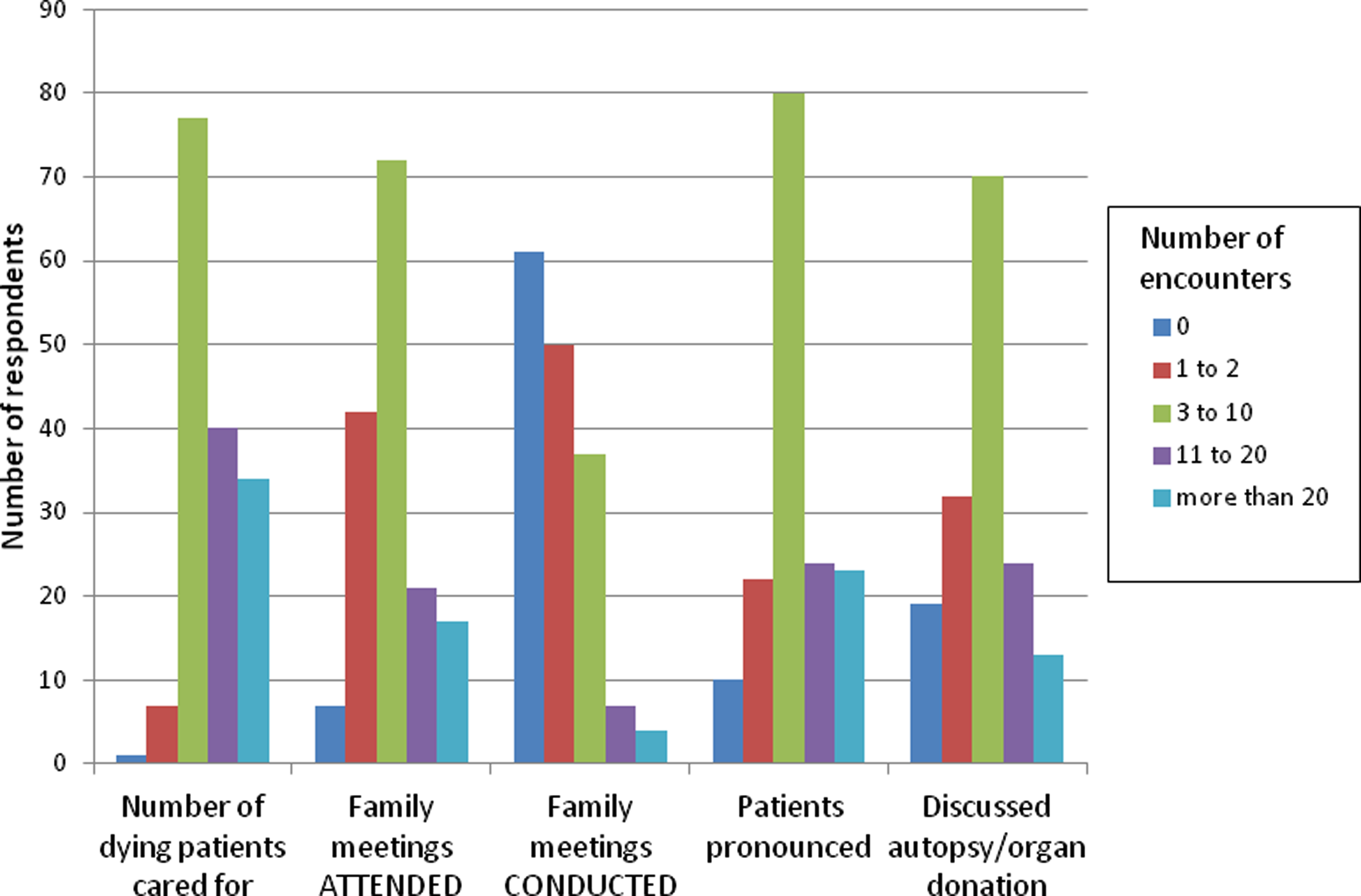
End-of-life care experience of residents.
Subgroup analyses using chi-square tests were performed by type of residency program on EOL experiences of the residents. Neurology residents were excluded in subgroup analyses due to small sample size. More residents in internal medicine and surgery had encountered greater than 20 EOL cases than their counterparts in anesthesia (Figure 2). Chi-square analyses showed that compared with their counterparts in anesthesia and surgery programs, residents in internal medicine had more experience in all tested facets of death and dying. When comparing Internal Medicine residents to all other residents, chi-square analyses showed that internal medicine residents had significantly more encounters in family meetings, pronouncing death, and requesting autopsy. Chi-square analyses comparing year of training and number of dedicated ICU rotations showed a trend toward both being associated with greater number of encounters with death and dying.
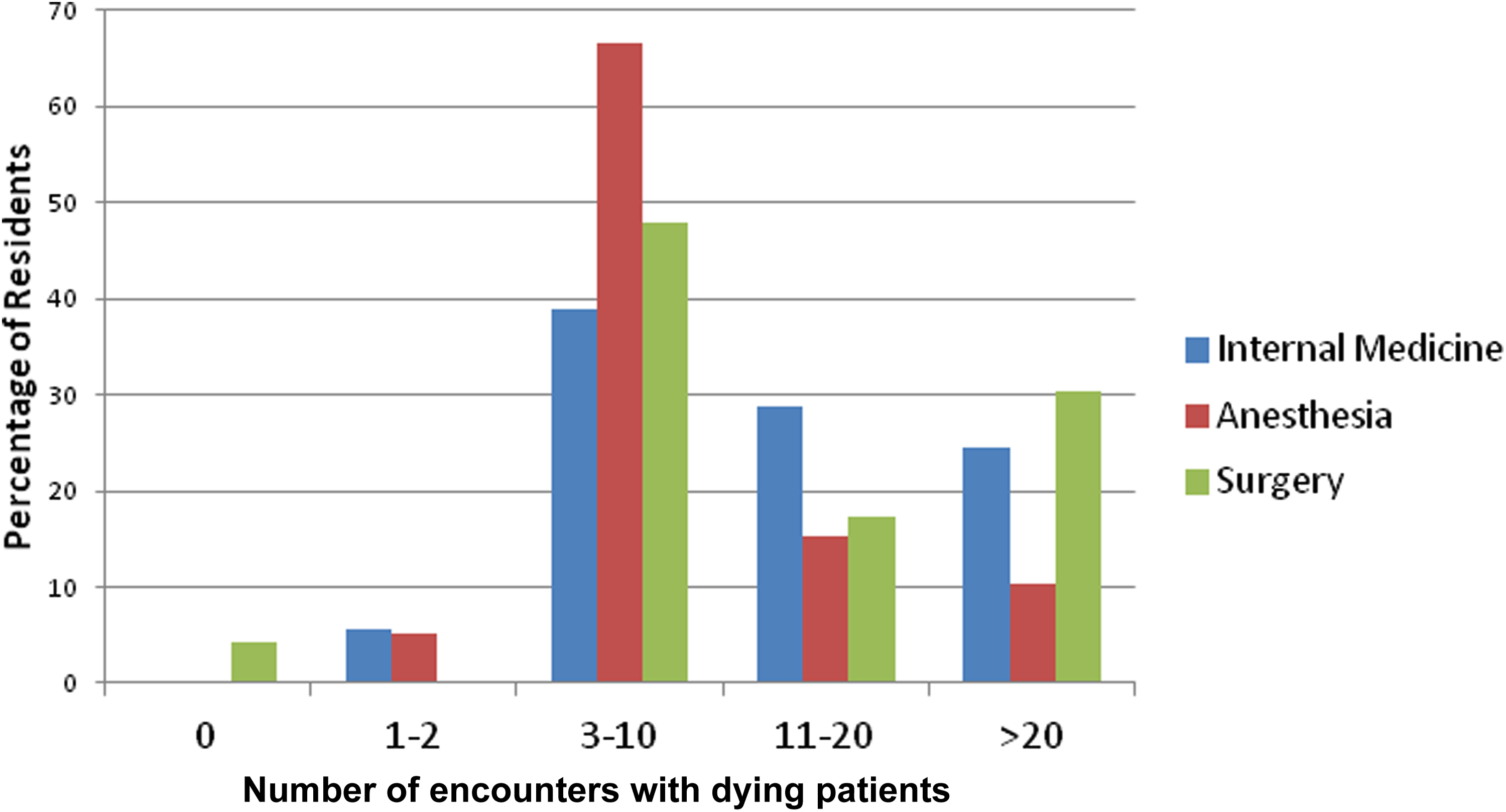
For how many dying patients have you been involved with provision of care?
Residents’ Opinions and Attitudes Toward PC/EOLC
Questions in the opinions/attitudes section are shown in Table 3 with the mean Likert-type response and standard deviation along with the grouping for composite measure analysis. Overall, residents felt somewhat prepared to care for critically ill patients at the EOL (Table 3, Question 19). Average responses for the composite measures were slightly above the mid-point indicating residents were only moderately comfortable dealing with EOL issues and with the training they received. Cronbach α values ranged from .42 to .71 (Table 4) indicating moderate internal consistency reliability for the questions in the composite measures and for the total measure.
Likert Scale Responses to Questions.a
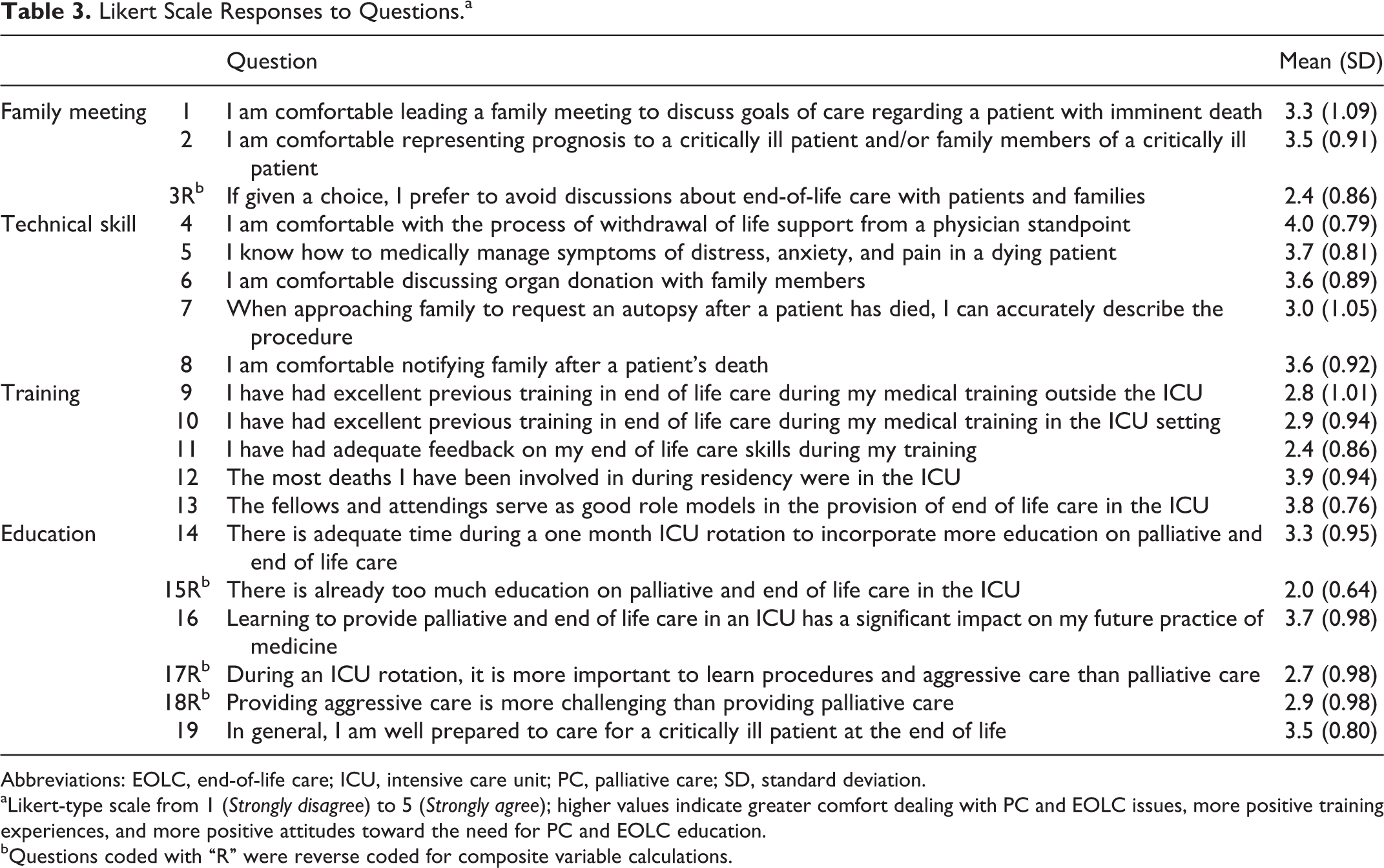
Abbreviations: EOLC, end-of-life care; ICU, intensive care unit; PC, palliative care; SD, standard deviation.
aLikert-type scale from 1 (Strongly disagree) to 5 (Strongly agree); higher values indicate greater comfort dealing with PC and EOLC issues, more positive training experiences, and more positive attitudes toward the need for PC and EOLC education.
bQuestions coded with “R” were reverse coded for composite variable calculations.
Opinions/Attitudes of Residents Toward PC and EOLC Issues.a
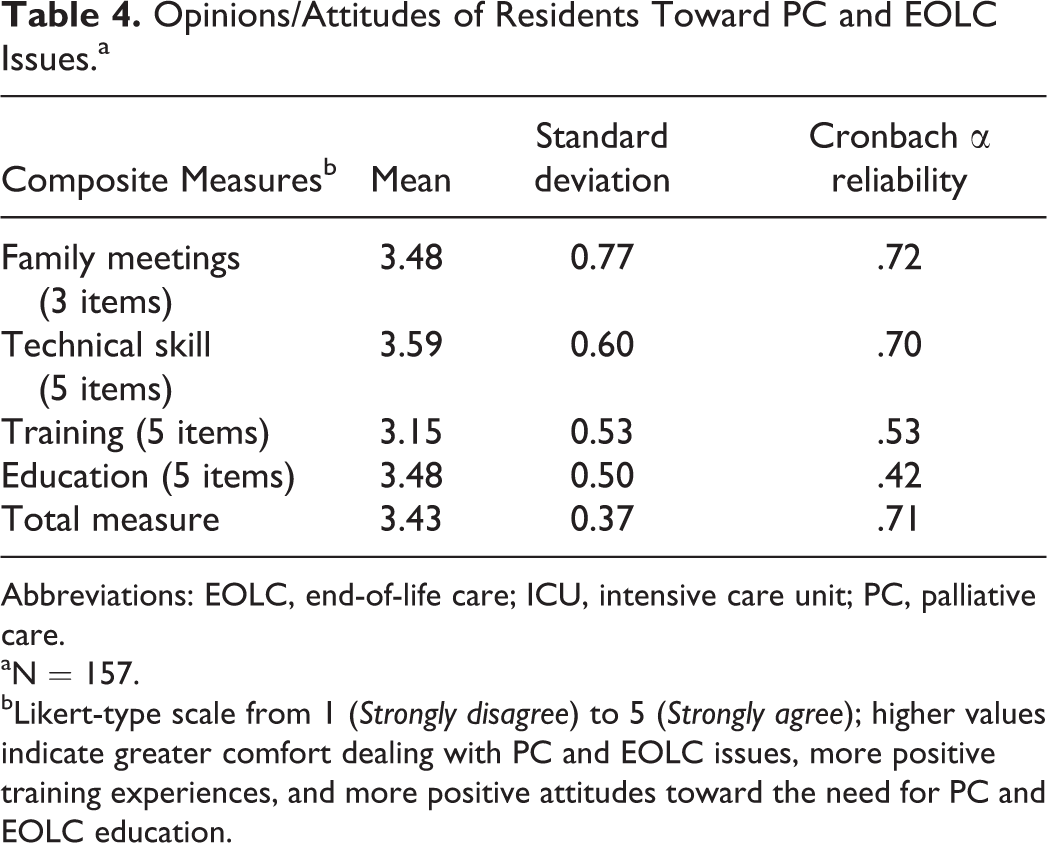
Abbreviations: EOLC, end-of-life care; ICU, intensive care unit; PC, palliative care.
aN = 157.
bLikert-type scale from 1 (Strongly disagree) to 5 (Strongly agree); higher values indicate greater comfort dealing with PC and EOLC issues, more positive training experiences, and more positive attitudes toward the need for PC and EOLC education.
In step 1 of regression analysis, we examined the effect of gender and ethnicity on the 4 composite measures and on the total measure. Female residents had more positive views than male residents toward PC/EOLC education in an ICU setting (estimate = 0.23; P value = .004). Otherwise, gender and ethnicity were not significant predictors of any of the measures. In step 2, we retained gender and ethnicity and added the physician demographic variables (type of residency training, religion, importance of religion, and number of ICU months completed) using forward stepwise selection. In step 3, we examined the effect of physician EOL encounters (Figure 1) on the 4 composite measures and on the total measure. Results of steps 2 and 3 are reported for each outcome separately.
Comfort With Family Meetings
In step 2, residency program and ICU months completed were significant predictors of comfort with family meetings. Anesthesia residents were significantly less comfortable with family meetings than internal medicine residents, and residents with only 1 month of ICU experience were significantly less comfortable than residents with 4 or more months of ICU experience. In step 3, all 5 variables reflecting physician EOL experiences were significantly positively associated with comfort in family meetings. However, only 1 variable (number of family meetings conducted) was retained in the final stepwise model (Table 5). Residency program and ICU months completed were also retained, and the amount of variance explained increased from 14% in step 2 to 31% in step 3.
Results of Stepwise Multivariate Regression Analysis for Composite and Total Measures of Opinions and Attitudes Toward PC/EOLC.a
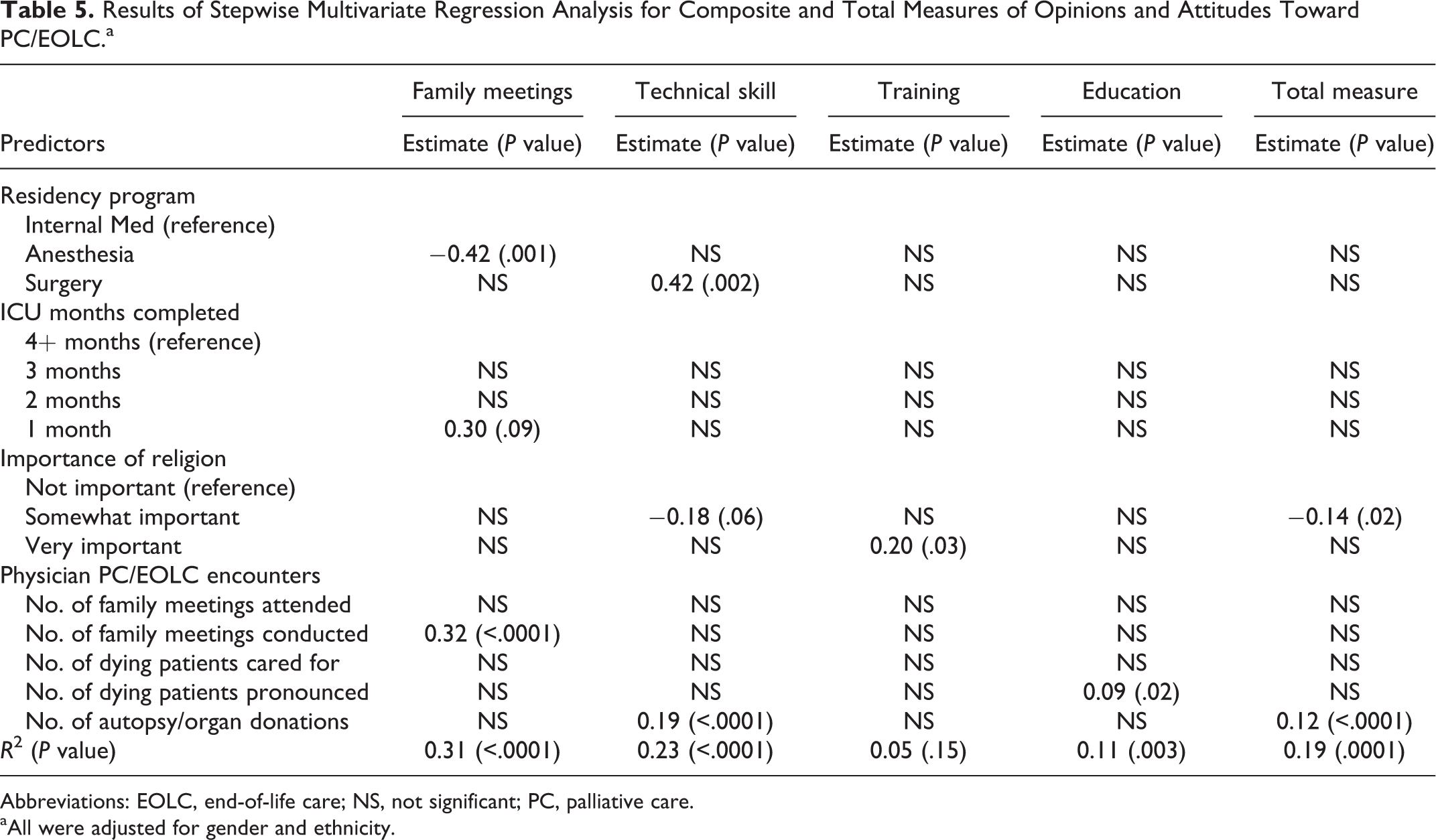
Abbreviations: EOLC, end-of-life care; NS, not significant; PC, palliative care.
aAll were adjusted for gender and ethnicity.
Technical Skill
In step 2, residency program and importance of religion were significant predictors of technical skill. Surgery residents had a significantly higher perception of their technical skill than internal medicine residents. Residents who described their religion as “somewhat important” had significantly lower scores in technical skill than residents who described their religion as “not important.” In step 3, all 5 variables reflecting physician EOL experiences were significantly positively associated with technical skill. However, only 1 variable (number of times approached family about autopsy/organ donation) was retained in the final stepwise model (Table 5). Residency program and importance of religion were also retained, and the amount of variance explained increased from 12% in step 2 to 23% in step 3.
Quality of Training
In step 2, the only significant predictor of quality of training was importance of religion. Residents who described their religion as “very important” rated the quality of their training more highly than residents who described their religion as “not important.” In step 3, none of the 5 variables reflecting EOL experiences of physician were significantly associated with quality of training. The final model (Table 5) retained only importance of religion as a predictor and accounted for only 5% of the variance in the outcome. However, the overall model had a nonsignificant P value of .15.
Education on PC/EOLC
In step 2, none of the physician demographic variables was significantly associated with education on PC/EOLC. The only significant predictor was gender, with females having significantly more positive views about the importance of education on PC/EOLC in the ICU setting compared to males (estimate = 0.23; P value = .004). In step 3, the only significant predictor among the 5 physician EOL experience variables was the number of dying patients pronounced (Table 5). Residents who had pronounced more dying patients had significantly more positive views about the importance of education on PC/EOLC in the ICU setting. Gender remained significant in the final model, and the amount of variance explained increased from 8% in step 2 to 11% in step 3.
Total Measure
In step 2, ICU months completed and importance of religion were significant predictors of scores on the total measure. Residents with fewer months of ICU experience had significantly more negative opinions and attitudes toward PC/EOLC in the ICU setting. Residents who described their religion as “somewhat important” had significantly more negative opinions and attitudes than residents who described their religion as “not important.” In step 3, all 5 variables reflecting EOL experiences of physician were significantly positively associated with opinions and attitudes toward PC/EOLC in the ICU setting. However, only 1 variable (number of times approached family about autopsy/organ donation) was retained in the final stepwise model (Table 5). The ICU months completed became nonsignificant when physician experience variables were included in the model, but importance of religion was retained in the final model and the amount of variance explained increased from 9% in step 2 to 19% in step 3.
Discussion
Palliative care/EOLC education is an important part of the educational experience for residents in multiple specialties. Given the large number of deaths in the ICUs, the ICU is an optimal place to teach PC/EOLC. 14 We evaluated resident education in PC/EOLC in the ICU for residents in 4 specialties. Our study confirms that residents have a broad range of experiences in critical care and palliative care. Overall, residents demonstrated moderate comfort with PC/EOLC issues with trends toward improvement with greater experience.
It is not surprising that internal medicine residents had more experience with death and dying compared to residents in anesthesia or surgery as shown in the chi-square analysis. For anesthesiologists, the patient relationship is often confined to the perioperative period, and a longer term relationship is less likely to develop. 19 Surgeons often will not operate on patients who are at high risk of dying because the risk of surgery may be greater than the potential benefit. The surgeon–patient relationship is often focused more on the technical aspects of surgery rather than a longer term interpersonal relationship. Thus PC/EOLC issues tend to be reflected back to internists. 20,21
Graduate medical education has traditionally followed a preceptor or apprenticeship model, whereby resident physicians gain skills through progressive experience. 22 Multiple factors such as number of encounters, months of ICU rotation, or years of residency training could all reflect increased experience. In the regression analysis, domains of family meeting and technical skill showed association between more months of ICU rotations and more comfort. Thus, in addition to encouraging role modeling of PC/EOLC skills and improving PC/EOLC education at all stages of training, increasing PC/EOLC encounters should be recommended to residents to help them increase their comfort and skill through experience.
Regression analyses also showed statistical significance of gender and importance of religion. That females have more positive attitudes toward EOLC education may reflect innate or culturally developed differences between men and women. Independent of religious background, residents who described themselves as “more religious” rated the quality of training as higher than their less religious counterparts. Approaches of physicians to religious and spiritual matters during the clinical encounter have been shown to vary with their own religious and spiritual characteristics. 23 Religion and spirituality are very important in the patient and family experience of EOLC, 24 and further exploration of providers’ religiosity in the setting of ICU EOLC could be useful.
This study shows that residents claimed an interest in learning more about palliative care in the intensive care setting. Although residents rated their faculty as good mentors, they did not feel they received adequate feedback. Indeed, the 3 lowest mean Likert-type scores were all classified within the training composite measure, more specifically related to prior EOLC education and feedback in EOLC skills (Table 3, Questions 9-11). It has been previously noted that trainees perceive inadequate feedback in their EOLC skills. 25 Providing helpful and constructive feedback in clinical education is a complex skill that requires honing on the part of the teachers. Educating critical care faculty and fellows on good feedback techniques could better equip them to guide residents as they learn about PC/EOLC issues. 26
Limitations of this study include small sample size and uneven group sizes, making it more difficult to compare data between groups of residents. Generalization to other institutions cannot be made from this single-center study. The survey, while modeled on prior surveys, has not been previously studied. Bias such as recall bias may lead to those who more recently completed an ICU or PC rotation reporting more of such experiences. The aim of this study was primarily to assess opinions and attitudes, which show trainees perceptions and interests. However, a limitation of self-report is that one cannot gauge whether physicians accurately report their skill level, which would require more objective data.
Conclusion
Providing good PC/EOLC is increasingly important in the provision of good critical care. The ICU is thus a suitable setting to educate residents about PC/EOLC. Overall, residents express interest in learning more about PC/EOLC. They show increased comfort in delivering PC/EOLC as they gain experience but feel that faculty feedback is inadequate. Efforts should be made to increase PC/EOLC teaching throughout the medical education system and to provide feedback to residents on their PC/EOLC skills in the ICU. Future directions could include educating critical care faculty in providing feedback to residents and creating a specialized ICU PC/EOLC education module, ideally with objective studies to measure effectiveness.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.