
Abstract
Objective:
To clarify how highly active hospital palliative care teams can provide efficient and effective care regardless of the lack of full-time palliative care physicians.
Methods:
Semistructured focus group interviews were conducted, and content analysis was performed.
Results:
A total of 7 physicians and 6 nurses participated. We extracted 209 codes from the transcripts and organized them into 3 themes and 21 categories, which were classified as follows: (1) tips for managing palliative care teams efficiently and effectively (7 categories); (2) ways of acquiring specialist palliative care expertise (9 categories); and (3) ways of treating symptoms that are difficult to alleviate (5 categories).
Conclusions:
The findings of this study can be used as a nautical chart of hospital-based palliative care team (HPCT) without full-time PC physician. Full-time nurses who have high management and coordination abilities play a central role in resource-limited HPCTs.
Introduction
In the 1990s, palliative care consultation teams were established to provide palliative care services in Western countries. During the past 20 years, the number of hospital-based palliative care teams (HPCTs), which are multidisciplinary teams aiming to maximize the quality of life for patients and their families facing the problems associated with life-threatening illness, has greatly increased in various countries, including the United Kingdom, the United States, Canada, and Australia; in all cases, these teams play important roles in the health care system. 1 –4 Various systematic reviews 5 and randomized controlled trials 6,7 have also reported the efficacy of HPCTs. The activities and efficacy of HPCTs have also been studied in Japan, 8,9 where they are expected to play an even more important role in the future.
In 2007, the Cancer Control Act and the Basic Plan to Promote Cancer Control Programs were enacted in Japan, addressing palliative care as one of the major issues in improving cancer care. This program required all government-designated cancer care hospitals (DCCHs) to organize HPCTs within each institute (397 hospitals, as of April 2014). 10 In 2008, the HPCT requirement for DCCHs was revised as follows: (1) members of the HPCT must include full-time palliative care physicians, psychiatrists, nurses, and pharmacists; (2) a palliative care outpatient clinic must be offered; (3) HPCT conferences must be held more than once a week; (4) information about the HPCT must be provided to patients and their families; (5) hospital-discharge support must be provided to inpatients; and (6) palliative care consultations must be provided to community health-care providers.
In 2012, Nakazawa and colleagues revealed that the mean annual number of consultations conducted by an HPCT was 73 per hospital and that the HPCTs with full-time palliative care physicians performed significantly more consultations than HPCTs without full-time palliative care physicians. 11 However, because of an underdeveloped postgraduate training structure, only 83 palliative care specialists are registered in Japan, 12 which is not enough to fill all the positions required by the HPCTs. In fact, only half of all DCCHs are able to place a full-time physician in their HPCT. 13,14 The Japanese Society for Palliative Medicine reported that even at facilities without full-time palliative care physicians, some highly active HPCTs received more than 150 consultations each year, 15 but the study did not investigate the methods required to manage an HPCT effectively.
It is therefore important to investigate how HPCTs can be managed effectively even without the full-time commitment of a palliative care physician. The present study thus aimed to clarify (1) tips for managing HPCTs efficiently and effectively, (2) how to improve and maintain professional competency in the HPCT, and (3) how to manage the relief of difficulties among highly active HPCTs without full-time palliative care physicians.
Methods
Study Design
The present study was a qualitative study using semistructured focus group interviews. This interview method can be used to investigate points of commonality and differences in the specific opinions of participants who have predefined shared characteristics. Our research team consisted of 6 researchers with experience in qualitative research.
Participants
The participants comprised physicians and nurses from HPCTs in the 397 DCCHs nationwide that met the following requirements: (1) no full-time palliative care physicians on staff and (2) more than 150 palliative care consultations annually. The participating facilities were recruited by explaining the study objectives in a letter, sent out using one of the largest mailing lists in Japan for doctors, nurses, and pharmacists who specialize in palliative care. Using snowball sampling of the facilities that offered to participate, we identified 7 facilities that met the requirements and selected 7 physicians and 6 nurses for participation in the study. AS sent an explanation of the study via e-mail and confirmed the participants’ willingness to participate in the study (see Ethical considerations given subsequently).
Data Collection
We considered that it would be appropriate to set up focus groups with 6 to 8 participants each to allow individuals to speak freely and in concrete terms about the activities of their HPCTs. 16 The first focus group interview was conducted on participants from 3 HPCTs (3 physicians and 3 nurses), and the second focus group interview was conducted on participants from 4 HPCTs (4 physicians and 3 nurses). Interviews lasted 2 hours each and were conducted in February 2014 in a conference room in Tokyo by a researcher (AS) who is a full-time physician in an HPCT at a DCCH. The interview guide was created based on the results of earlier discussions among the researchers. The semistructured interviews covered the following points: (1) the background of the participants with regard to the HPCTs in which they practiced; (2) tips for managing an HPCT efficiently and effectively; (3) how an HPCT can improve and maintain professional competency; and (4) how to manage the relief of difficult symptoms. On the day of the interview, participants were given an explanation of the present study, and the interviews were started after we received their written consent (see Ethical considerations given subsequently). Interviews were recorded with a voice recorder, and another researcher took field notes while AS conducted the interviews. Data saturation was confirmed between the researchers.
Data Analysis
Transcripts of the interviews were created from the recorded content and field notes. The transcripts were provided to the participants who confirmed and revised them. Next, the content was analyzed on the basis of the method outlined by Krippendorff. 17 First, transcripts were divided into units of semantic content, and all expressions and contents related to managing HPCTs were extracted. Next, units with similar expressions and semantic contents were classified into groups, summarized so that the semantic content was not lost and codified. Codes were grouped according to similarity and subcategories were created. Subcategories were then classified and categories were created. Content analysis was conducted independently by 2 researchers (AS and MK), after which discussions were conducted with 2 other researchers (NY and TY) who were not involved in the analytical process. Revisions were made until all 4 researchers agreed. YK supervised confirmation of whether subcategories and categories were appropriate. Hereafter, codes are signified by “ ”, subcategories by [], and categories by < >.
Ethical Considerations
The present study was conducted in accordance with the Declaration of Helsinki and ethical guidelines with regard to clinical research. The study plan was approved by the Ethics Committee at Kobe University Graduate School of Medicine.
Results
Participants
There were 13 participants in the study (7 physicians [6 males and 1 female] and 6 nurses [1 male and 5 females]). The mean number of years of clinical experience among the participants was 19 (range, 10-26 years), and the mean length of time practicing in an HPCT was 2.9 years (range, 1-6 years). The main specialties of the physicians were surgery (3 physicians), internal medicine (3 physicians), and radiology (1 physician). All 6 nurses were full-time HPCT nurses. Among the study participants, the mean number of annual HPCT consultations was 202 (range, 150-280). We extracted 209 codes from the transcripts and organized them into 3 themes.
Themes
Theme 1: Tips for managing HPCTs efficiently and effectively
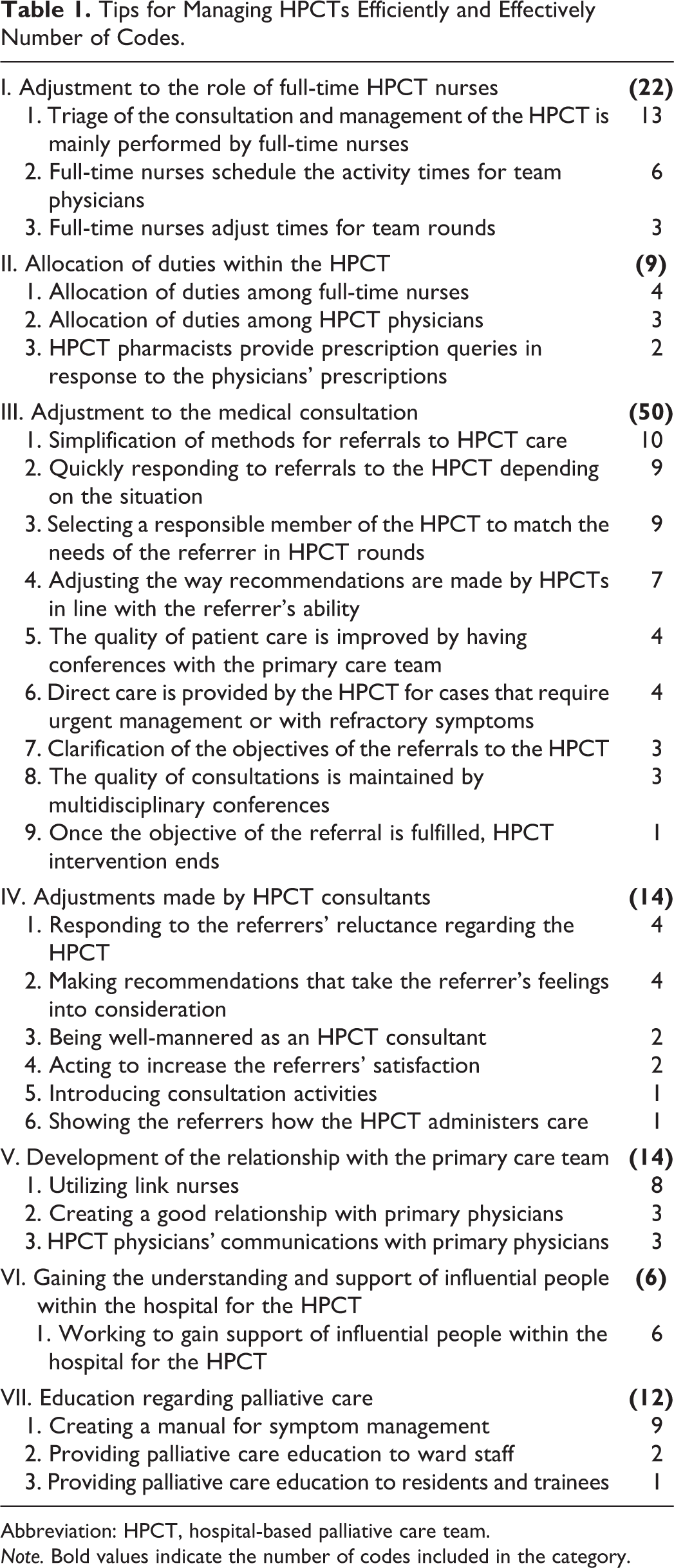
We extracted 127 codes and organized them into 28 subcategories on the basis of similarity. Subcategories were then organized into 7 categories as follows: <adjustment to the role of full-time HPCT nurses>, <allocation of duties within the HPCT>, <adjustment to the medical consultation>, <adjustments made by HPCT consultants>, <development of the relationship with the primary care team>, <gaining the understanding and support of influential people within the hospital for the HPCT>, and <education regarding palliative care> (Table 1).
Tips for Managing HPCTs Efficiently and Effectively Number of Codes.
Abbreviation: HPCT, hospital-based palliative care team. Note. Bold values indicate the number of codes included in the category.
Adjustment to the role of full-time HPCT nurses
This category included 3 subcategories and 22 codes. Participants indicated the importance of full-time nurses and noted that team management was typically conducted by full-time nurses. These opinions suggested the subcategories of [triage of the consultation and management of the HPCT is mainly performed by full-time nurses], [full-time nurses schedule the activity times for team physicians], and [full-time nurses adjust times for team rounds].
Outpatient examinations are also basically conducted by a nurse, with me standing behind watching. I think the nurse plays a key role. (D3)
Allocation of duties within the HPCT
This category included 3 subcategories and 9 codes. The subcategories included [allocation of duties among full-time nurses] and [allocation of duties among HPCT physicians], where participants noted that duties were allocated among multiple HPCT physicians. Because HPCT pharmacists were responsible for prescription recommendations, we added the subcategory of [HPCT pharmacists provide prescription queries in response to the physicians’ prescriptions].
Even if I am not in attendance, a list of the patients I am following up with palliative care appears on the electronic medical records. I continually add notes to these medical records, for example, “thoroughly check patients who exhibit dramatic changes in condition.” For patients who require only a check of their medical records, I just have staff quickly check them. (D2)
Adjustment to the medical consultation
This category included 9 subcategories and 50 codes. Adjustments to HPCT rounds included [quickly responding to referrals to the HPCT depending on the situation] and [selecting a responsible member of the HPCT to match the needs of the referrer in HPCT rounds]. For referrals to HPCT care, we added the subcategories of [simplification of methods for referrals to HPCT care] and [clarification of the objectives of the referrals to the HPCT]. With regard to HPCT recommendations, participants raised several issues, including [adjusting the way recommendations are made by HPCTs in line with the referrer’s ability] and [direct care is provided by the HPCT for cases that require urgent management or with refractory symptoms]. Participants suggested methods for guaranteeing the quality of HPCT consultations, including multidisciplinary conferences, resulting in the subcategories of [improving quality of patient care by having conferences with the primary care team] and [the quality of consultations is maintained by multidisciplinary conferences]. The point that [once the objective of the referral is fulfilled, HPCT intervention ends] indicated that intervention was provided only to patients who required it.
For patients who require care quickly, I go there first in the morning, consult with a physician, and quickly write the recommendation and try my best to respond to the problem that day, as quickly as possible. (N3)
Adjustments made by HPCT consultants
This category, focusing on other HPCT members, such as the palliative care doctors and specialist nurses, included 6 subcategories and 14 codes. Considerations given to staff requesting referrals, such as primary physicians and ward nurses, included [responding to the referrers’ reluctance regarding the HPCT], [making recommendations that take the referrer’s feelings into consideration], and [acting to increase the referrers’ satisfaction]. The idea of clarifying HPCT interventions was raised in the subcategory of [showing the referrers how the HPCT administers care]. From the physicians’ comments, we added [being well-mannered as an HPCT consultant] and [introducing consultation activities].
Being called at any time by anybody from anywhere means that you need to be happy that patients have called you. If I am called, I go as quickly as possible. (D2)
Development of the relationship with the primary care team
This category included 3 subcategories and 14 codes. With regard to relationships with the HPCT nurses, we extracted the idea of [utilizing link nurses].
I get the impression that communication between physicians goes a lot more smoothly. However, the more I cooperate with primary physicians, the more I feel that they start to trust me, making communication become gradually easier. (N5)
To address the HPCT members’ relationships with primary physicians, we added [HPCT physicians’ communicating with primary physicians] and [creating a good relationship with primary physicians].
Gaining the understanding and support of influential people within the hospital for the HPCT
This category included 1 subcategory and 6 codes. To foster and promote understanding of the HPCT within the hospital organization, we added the idea of [working to gain support of influential people within the hospital for the HPCT]. Some opinions were raised regarding the importance of gaining stakeholder support including “we have the cooperation of the nursing department” and “the head of the hospital supports us by attending conferences and coming with us on rounds.”
The head of the hospital attends our conferences every week and comes with us on rounds even when there are many people in attendance, which is really of assistance. The head has offered us full support for various initiatives that we have set in place, and this has really helped. (D4)
Education regarding palliative care
This category included 3 subcategories and 12 codes. Participants suggested that relationships with the primary care team improved when education was provided to them, and these opinions were captured in the subcategories of [providing palliative care education to ward staff] and [providing palliative care education to residents and trainees]. The HPCT recommendations were also simplified by [creating a manual for symptom management].
The manual itself was uploaded into the electronic medical records. Users can check on each item for easing symptoms, and the screen with this information appears. However, it would also be good if instructions for the easing of symptoms could be copied and pasted into the manual. (N6)
Theme 2: Ways of acquiring specialist palliative care expertise
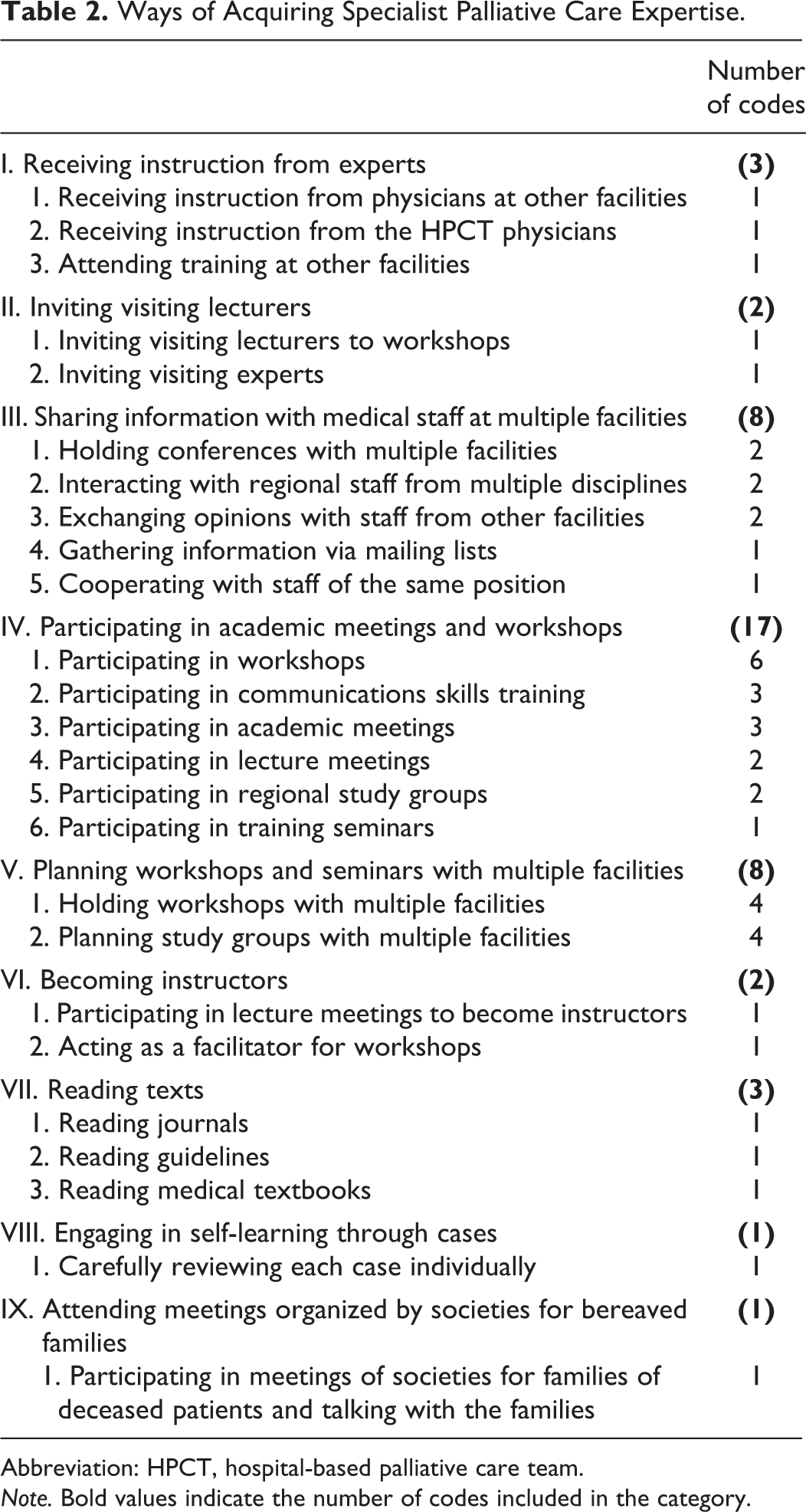
We extracted 45 codes and organized them into 25 subcategories on the basis of similarities. Subcategories were then organized into 9 categories: <receiving instruction from experts>, <inviting visiting lecturers>, <sharing information with medical staff at multiple facilities>, <participating in academic meetings and workshops>, <planning workshops and seminars with multiple facilities>, <becoming instructors>, <reading texts>, <engaging in self-learning through cases>, and <attending meetings organized by societies for bereaved families> (Table 2).
Ways of Acquiring Specialist Palliative Care Expertise.
Abbreviation: HPCT, hospital-based palliative care team. Note. Bold values indicate the number of codes included in the category.
In the category of <receiving instruction from experts>, participants suggested that instruction should be received by the HPCT not only from physicians, but also from palliative care experts from other facilities. In addition, participants stated that knowledge could be acquired by inviting experts to in-hospital workshops as a chance to implement <inviting visiting lecturers>. In the category of <sharing information with medical staff at multiple facilities>, participants suggested that [holding conferences with multiple facilities] presented opportunities for [interacting with regional staff from multiple disciplines]. Apart from conferences, opportunities for the exchange of opinions with medical staff from other facilities included [gathering information via mailing lists]. <Participating in academic meetings and workshops> was also suggested as a means of acquiring knowledge. Other participants suggested that, in addition to participating in academic meetings and workshops, <planning workshops and seminars with multiple facilities> and <becoming instructors> further increased opportunities to improve one’s expertise. For acquiring knowledge, in addition to <reading texts> such as academic journals, medical textbooks, and guidelines, some participants emphasized the importance of clinical experience by [carefully reviewing each case individually] and making new observations by <attending meetings organized by societies for bereaved families>.
Theme 3: Ways of treating symptoms that are difficult to alleviate
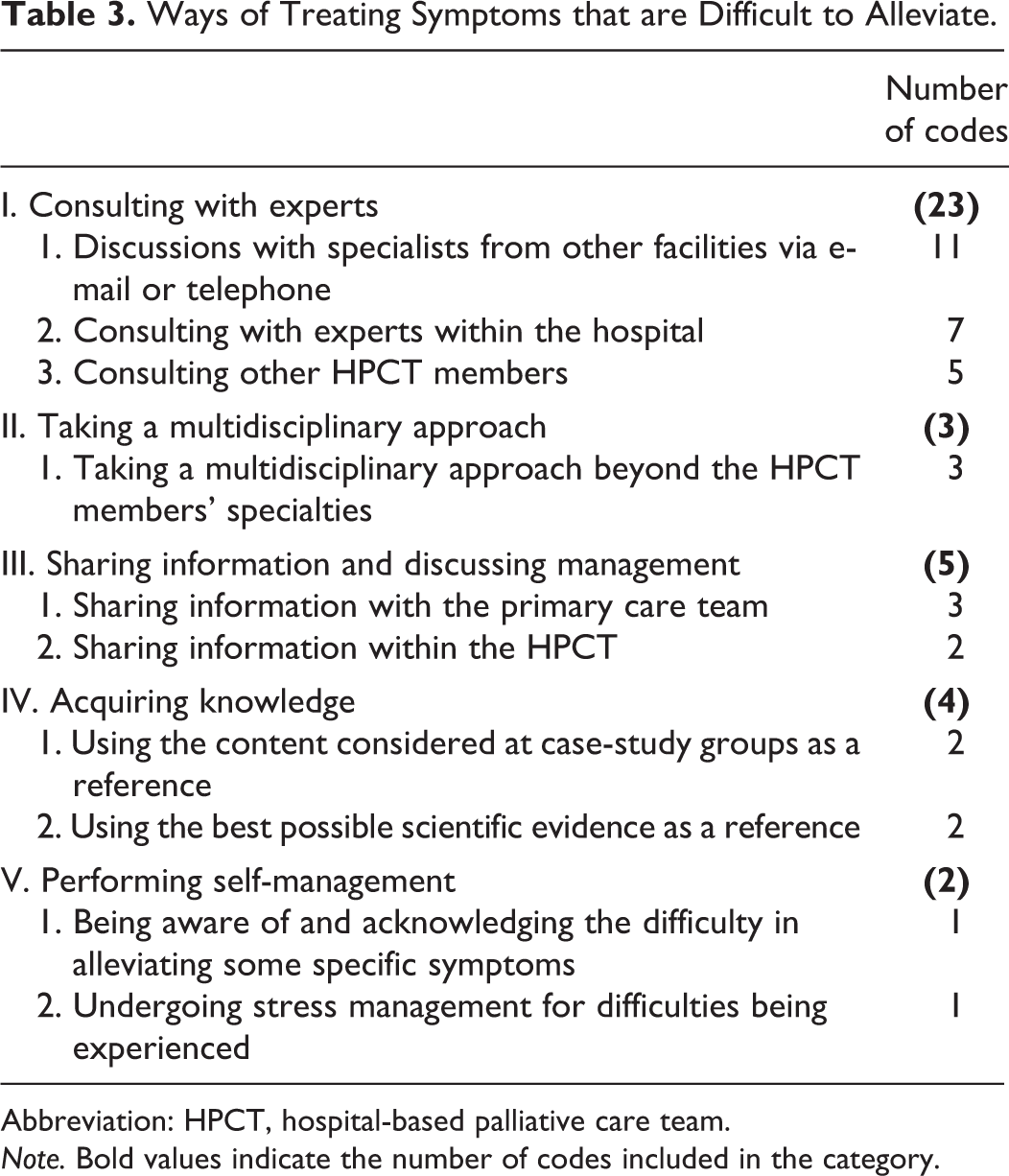
We extracted 37 codes and organized them into 10 subcategories on the basis of similarities. Subcategories were then organized into 5 categories, namely, <consulting with experts>, <taking a multidisciplinary approach>, <sharing information and discussing management>, <acquiring knowledge>, and <performing self-management> (Table 3).
Ways of Treating Symptoms that are Difficult to Alleviate.
Abbreviation: HPCT, hospital-based palliative care team. Note. Bold values indicate the number of codes included in the category.
<Consulting with experts> involved not only [consulting with experts within the hospital] and [consulting other HPCT members] but participants also cited the utility of having [discussions with specialists from other facilities via e-mail or telephone]. Some participants recommended that [taking a multidisciplinary approach beyond the HPCT members’ specialties] allowed testing of approaches that differed from those used in the HPCT (eg, involving a physiotherapist). Participants recommended that the difficulty of alleviating symptoms could be examined not just by [sharing information within the HPCT] but also by [sharing information with the primary care team]. The importance of stress management for staff members was raised in the subcategories of [being aware of and acknowledging the difficulty in alleviating some specific symptoms] and [undergoing stress management for difficulties being experienced]. The category of <acquiring knowledge> included the subcategories of [using the content considered at case-study groups as a reference] and [using the best possible scientific evidence as a reference].
Discussion
The present study is the first report to clarify how efficiently and effectively highly active HPCTs are engaging in consultation activities despite having no full-time palliative care physicians. The findings of this study can be used as a nautical chart of HPCT management when HPCTs have no full-time physician.
This study shows some methods that are used by HPCTs that experience a high number of referrals to conduct activities efficiently and effectively, and we believe that the information presented here can also be used as a “best practice” document for managing HPCTs.
The most important finding is that full-time nurses play a central role in managing HPCTs. Because HPCT staff often held other posts concurrently, they were unable to secure enough time for HPCT activities and had a heavy burden of duties. Therefore, to address this issue, full-time nurses managed the activity times of physicians and other HPCT members and adjusted HPCT rounds and conference times. Results showed that full-time nurses have high management and coordination abilities and play the most important role in HPCTs.
The second important finding concerned the relationship between the referrers (including primary physicians and ward nurses) and the HPCT. Methods used during consultations included simplifying the referral process and adjusting the recommendation style to meet the needs of primary physicians and ward nurses. These types of adjustments are consistent with those outlined in a report on advanced HPCTs in Japan 18 and a report regarding medical consultations overseas. 19 –22 We propose that there are several features of the “commandments” suggested by Goldman and colleagues in 1983, 19 such as an emphasis on verbal communications, being succinct, and establishing the urgency of the consultation, that are relevant for HPCTs today. 21 These methods are similarly important in HPCTs with insufficient staff.
The present study has a number of limitations. First, this study targeted only HPCTs at DCCHs and may not reflect the opinions of HPCTs at non-DCCHs. Second, we surveyed only HPCT members who are physicians and nurses and did not include pharmacists. Therefore, the results may be biased and our findings may not be universally applicable. Third, bias may have been introduced by the fact that the researcher who conducted the interviews (AS) is acquainted with some of the participants. Finally, because the interviews were not conducted individually, we cannot attach a level of importance to each extracted item by, for example, recording how many participants thought a certain category was important. Therefore, the results of this study cannot be used to determine priority items that could be addressed to efficiently manage HPCTs. We hope that a future questionnaire, based on these results, can be used to conduct quantitative research using a larger sample.
Conclusion
The present study clarified the methods currently used to effectively manage palliative care consultation teams despite the lack of full-time physicians. We believe that these findings, which outline methods used to acquire specialist palliative care expertise and to treat pain that is difficult to alleviate, form an important aid for providers so they can improve not only the care of patients with cancer and quality of life for these patients and their families but also education for medical staff specializing in palliative care.
Footnotes
Acknowledgments
The authors express their deep gratitude to the physicians and nurses who participated in this study. We also thank nurse Kanako Otagaki and pharmacist Takeshi Ioroi for their assistance in creating the field notes.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Grant-in-Aid for Scientific Research from the Ministry of Health, Labour and Welfare in 2013.