
Abstract
Background:
Physicians’ lack of comfort and skill in communicating about hospice care results in deficits and delays in hospice referrals. Preclinical exposure to hospice may lay a foundation to improve medical students’ knowledge and comfort with hospice care.
Objective:
To understand how preclinical medical student (MS)-2s respond both educationally and emotionally to a required hospice care experience (HCE).
Design:
Accompanied by hospice clinicians, MS-2s spent 3 hours seeing inpatient or home hospice patients followed by a 1-hour debriefing. Students submitted written reflections to e-mailed educational and emotional prompts.
Setting/patients:
Two hundred and two MS-2s from 2 academic cohorts completed the HCE at 1 of 2 hospice sites.
Measurements:
Written reflective responses were analyzed qualitatively, where salient themes extracted and responses were coded.
Results:
Ninety-two students submitted 175 responses to Prompt #1 (educational impact) and 85 students entered 85 responses to prompt #2 (emotional impact) of the HCE. Eleven themes were identified for prompt #1, most frequently focusing on hospice services and goals and hospice providers’ attitudes and skills. Prompt #2 elicited a diverse spectrum of emotional responses, spanning positive and negative emotions. Most often, students reported “no specified emotional reaction,” “sad/depressed,” “difficult /challenging,” “heartened/encouraged,” and “mixed emotions.”
Conclusion:
In an HCE, preclinical students reported learning core aspects of hospice care and experiencing a broad spectrum of emotional responses. These findings may assist educators in the planning of HCEs for preclinical students, including debriefing sessions with skilled clinicians and opportunities for triggered reflection.
Introduction
Significant gaps persist in the care provided to patients and their families near the end of life (EoL). 1 Despite national improvements to increase the availability of hospice services, underutilization of timely hospice care remains an important contributor to deficits in EoL care. 1 –4 Medical school graduates, residents, and practicing physicians continue to report a lack of comfort and skill in communicating effectively with patients about goals of care and the range of treatment options for life-limiting disease, including hospice referral. 5 –11 Physicians’ discomfort or lack of skill in communicating effectively with patients and their families about hospice likely contributes to inadequate or delayed hospice referrals.
With mandates from the Liaison Committee on Medical Education 12 and recommendations from palliative medicine educators, 13 –15 the past decade has seen substantial growth in the inclusion of palliative and EoL care education in medical school curricula. 15 –17 Undergraduate palliative care education varies widely in extent and pedagogic approaches. 15 –17 Some medical schools report effective experiential learning through interactions with terminally ill patients 15,16,18 –20 and hospice experiences in the clinical years of medical school. 21 –23 In addition to discrete, immersion learning experiences, educators stress the importance of longitudinal, integrated approaches to palliative care curricula extending over the 4 years of medical school. 10,24 Only 2 published investigators have reported implementation of longitudinal, integrated 4-year curricula, 25,26 although the effects of the early year experiences in these programs have not been evaluated.
Analyses of students’ reflections on their experiences during the clinical years with terminally ill and dying patients reveal that these can be emotionally powerful and at times distressing experiences for which students do not feel well prepared. 19,27,28 In a study of preclinical students who were asked to predict their reactions to the deaths of future patients, many reported anticipating negative emotions such as fear, frustration, guilt, and self-doubt. 11 Enhanced preclinical education in palliative and terminal care may lay a foundation, which would improve students’ preparedness for subsequent experiences in the clinical years. Most preclinical palliative care education does not include direct patient contact, and concern has been raised about whether preclinical students are developmentally and emotionally prepared for experiences with terminal patients. 5 However, Wechter et al 29 found that a required hospice observational experience resulted in positive effects on MS-1s’ attitudes toward caring for the terminally ill. In addition, several investigators have reported positive findings for preclinical elective hospice experiences for small numbers of students. 30 –32
We previously described the development and evaluation of a longitudinal, integrated 4-year medical school curriculum in palliative and EoL care which aims to align learning objectives and teaching strategies with the developmental stage of the learners. 25 Our approach emphasized experiential learning, including in the preclinical years as well as student self-reflection and interprofessional learning. 25,33 The focus of this report is an in-depth evaluation of the second-year hospice care experience (HCE) component of our curriculum. Our goal was to explore through an in-depth thematic analysis of written student reflections how preclinical MS-2s respond both educationally and emotionally to a required HCE.
Methods
Study Design
During the fall semesters of 2 academic years in 2013 to 2014 and 2014 to 2015, all MS-2s at our school participated in a mandatory 3-hour HCE as part of a weekly clinical skills clerkship course. Prior to the HCE, all students participated in a required 2-hour “Introduction to EoL Care Workshop” in the first year of medical school. The goal of this first-year workshop was for students to recognize that physicians in all specialties need to acquire basic competencies and comfort in EoL care to provide patients and families comprehensive high-quality care. Students also had basic patient interview and relationship-building training in the clinical skills clerkship course as well as weekly tutored clinical exposures with patients to practice history taking and physical examination. Some students had additional clinical exposure through extracurricular activities such as volunteering to be a “patient buddy” to a child with serious illness through the pediatric interest group or providing company to patients in a chemotherapy infusion center through the palliative care scholars interest group. A minority of students participated in the “healer’s art” elective in their first year of school, which included facilitated sessions on grief and loss.
In the HCE, groups of 3 to 4 students spent 3 hours at an inpatient hospice facility or on outpatient home hospice care visits at private residential homes, assisted living facilities, or skilled nursing facilities. The students were accompanied and guided by a physician, advanced practice registered nurse, or registered nurse specializing in hospice medicine. To prepare for the HCE, students were encouraged to read 2 pertinent articles concerning palliative and hospice care available on the Yale School of Medicine’s Palliative and End-of-Life Care Education website. 34 Upon arrival at the preassigned HCE site, the on-site facilitator provided a brief introduction about the specific site and then students were divided into groups of 3 to 4 to accompany an assigned hospice clinician for visits with 1 to 2 hospice patients and/or their families. Following the patient visits, the hospice clinician conducted a 1-hour debriefing session to discuss the students’ observations and experiences and to address any questions. We encouraged the clinicians facilitating the debriefing sessions to provide empathic support and further explore the challenges and impressions that students shared from their visits with the hospice patients and their families. These facilitators also received training on the learning objectives of the HCE and how this experience fits into the overall curriculum.
The HCE learning objectives for the students were as follows: learn the key elements of assessment of patients at the EoL, including physical symptoms as well as psychosocial and spiritual aspects of terminal illness; compare and contrast the elements of history taking and physical examination for patients seeking palliative care and those seeking curative therapies without palliation; and reflect on the professional and personal challenges of caring for patients at the EoL.
On the evening, the HCE was completed, students received an e-mail invitation with an embedded web link to a Qualtrics survey (Qualtrics, December 2015, Provo, UT, USA) with the following 2 prompts: Name 1 to 2 things you learned about hospice care you want to be sure to remember when you start your clinical work. Briefly describe your emotional reaction to seeing a terminally ill patient at hospice.
Students voluntarily submitted anonymous free-text responses to these 2 prompts.
Setting
The MS-2s participated in the HCE at 1 of the 2 not-for-profit hospices, each with inpatient units and extensive home hospice care service programs. One site has 12 inpatient beds with an average daily home care census of 75 patients; the other site has 52 inpatient beds and an average daily home care census of >350 patients.
Study Sample and Analysis of Students’ Reflection Responses
We collected demographic characteristics of the MS-2s who participated in the HCE from the school’s Office of Student Affairs. The students’ survey responses were recorded electronically on Qualtrics and were subsequently imported to Microsoft Excel (2010) for analysis. Given the exploratory nature of the study, inductive coding was used to categorize similar themes to develop a coding key. 35 Two authors (C.T. and M.E.) independently read all the responses and identified recurring themes. Each reader performed this independent review without prespecified thematic structures; rather, it was an iterative process that involved multiple of readings of the students’ responses to denote, compare, and consolidate themes that surfaced. The same 2 authors then convened to jointly devise the coding keys for each prompt. The coding keys were then applied independently by the 2 authors to code all of the responses. More than 1 code was allowed for each response. All 3 authors then met to settle any coding variances.
Participation in the study was voluntary, individual respondents were anonymous, and responses were not linked to any personal identifiers. The study was granted a waiver from the school’s human investigation committee (Protocol # 1602017145, 45 CFR 46.101(b)(4)).
Results
The characteristics of the 202 students (each class size was 101) who participated in the HCE are shown in Table 1. Ninety-two students (response rate 46%) provided responses to our e-mailed prompts with responses from 39 students in 2013 to 2014 and 53 students in 2014 to 2015 (Table 2). For prompt #1 (educational response), 92 students entered a total of 175 responses, averaging 1.9 responses per student, and 183 coded labels were applied. For prompt #2 (emotional reaction), 85 students entered a total of 85 responses and 124 coded labels were applied. For both prompts #1 and #2, each response was allowed to receive more than 1 coding label.
Characteristics of MS-2s in the 2013 to 2014 and 2014 to 2015 Academic Years (n = 202) Participants in Hospice Care Experience.
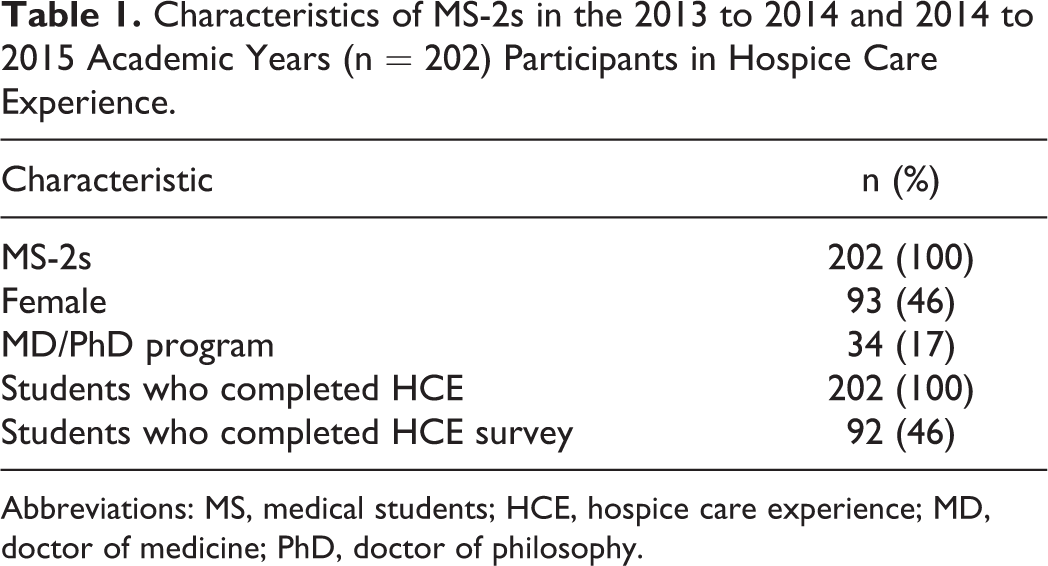
Abbreviations: MS, medical students; HCE, hospice care experience; MD, doctor of medicine; PhD, doctor of philosophy.
MS-2s responses to the Hospice Clinical Experience Evaluation Prompts in the 2013 to 2014 and 2014 to 2015 Academic Years.a
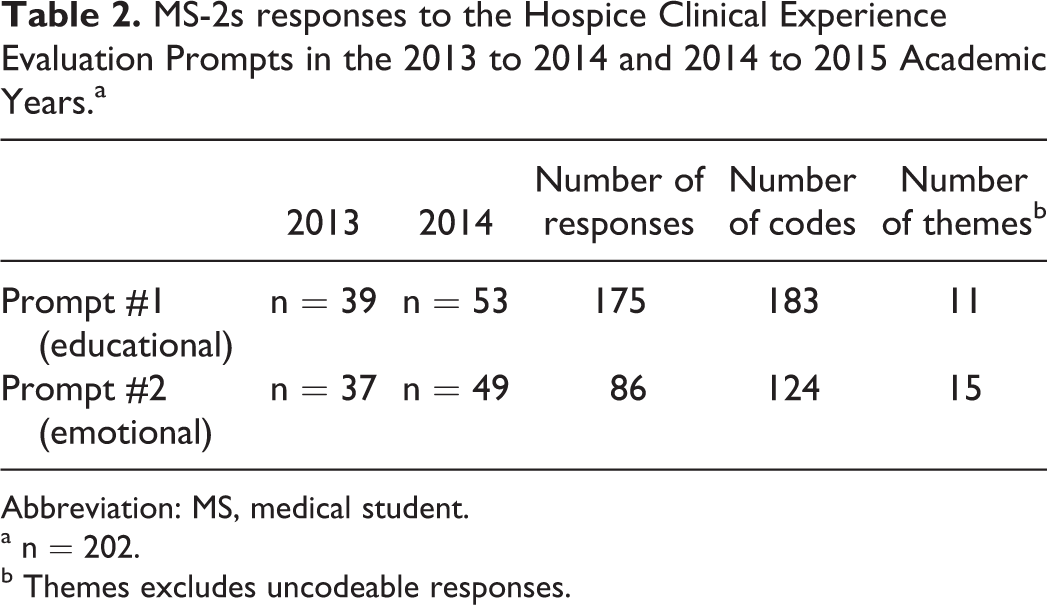
Abbreviation: MS, medical student.
a n = 202.
b Themes excludes uncodeable responses.
For prompt #1, 11 thematic codes were identified (Figure 1). Apart from these, there were 3 uncodeable responses. Seven of the 11 codes occurred with a frequency of ≥10 times and accounted for about 86% (157 of 183) of the coded responses (Figure 1). The 3 most frequent coded themes for “lessons learned” were (1) hospice eligibility, services, and options (n = 33); (2) hospice care goals, philosophy, and outcomes (n = 28); and (3) provider knowledge, skills, and attitudes about hospice care (n = 24). Illustrative examples of student entries for each of the frequently occurring codes for prompt #1 are shown in Table 3.
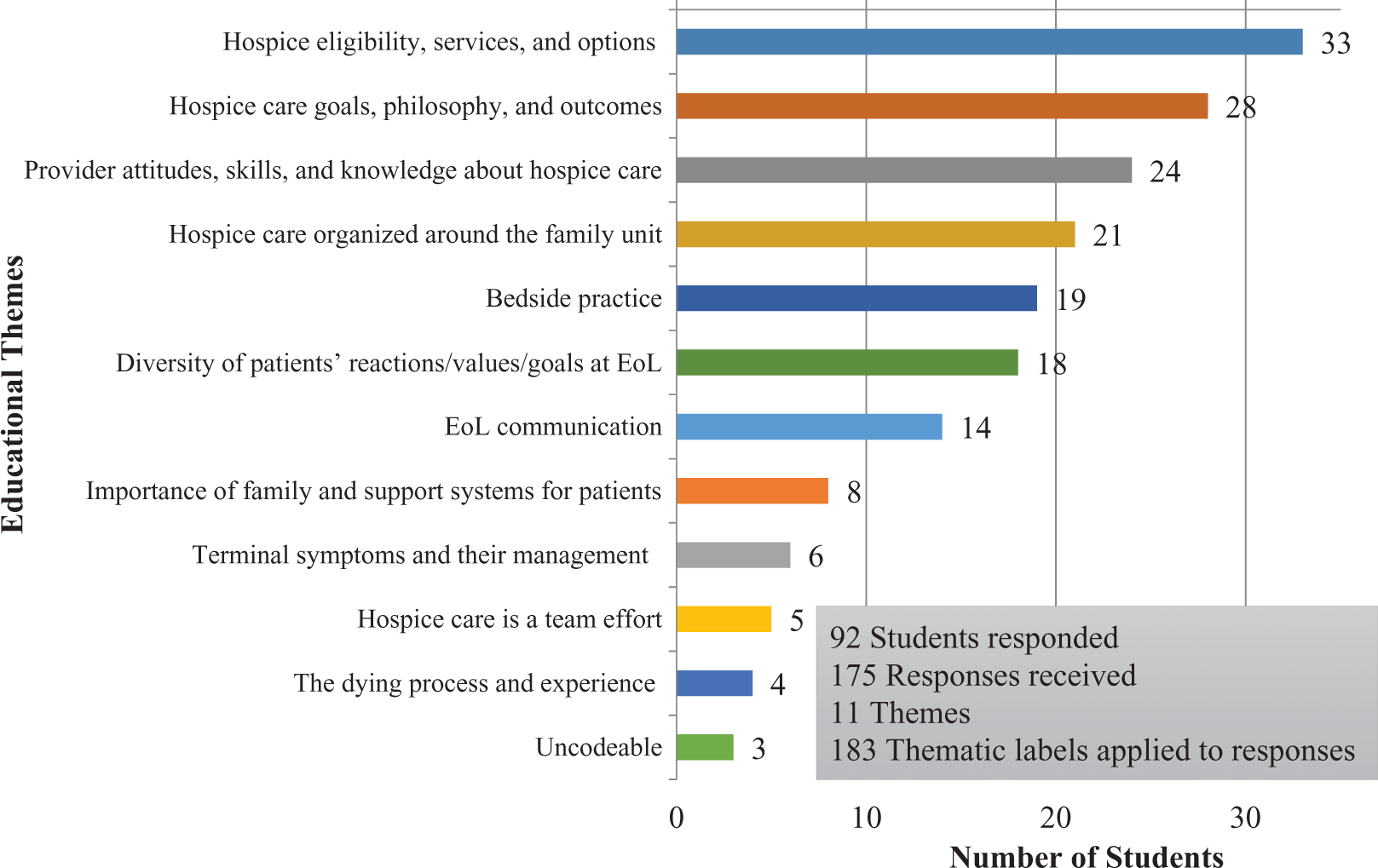
Eleven themes for educational responses emerged from the 175 responses submitted by 92 students (n), averaging 1.9 responses per student. The top 3 themes were “hospice eligibility, services, and options” (36%, n = 33), “hospice care goals, philosophy, and outcomes” (30%, n = 28), and “provider attitudes, skills, and knowledge about hospice care” (26%, n = 24). One hundred eighty-three coded labels were applied, with some responses receiving more than 1 label.
Illustrative Examples of MS2 Responses to Prompt #1 “Name 1-2 things you Learned About Hospice Care You Want to be Sure to Remember when you Start Your Clinical Work,” by Themes.

Abbreviation: MS, medical student.
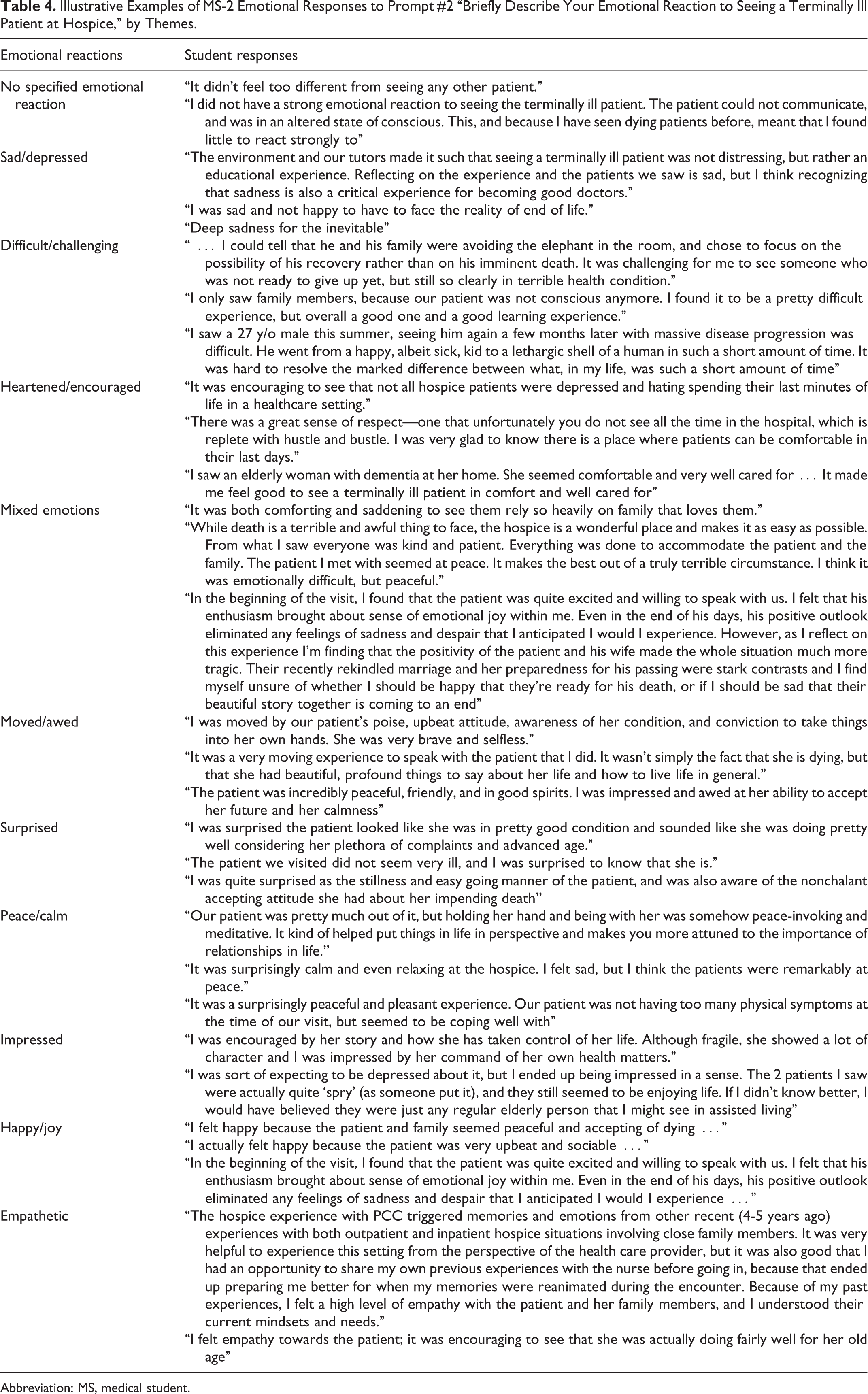
For prompt #2, 15 thematic codes were identified (Figure 2). Apart from these, 3 responses were uncodeable. Six of the 15 themes occurred with a frequency of ≥10 and accounted for about 69% (86 of 124) of the coded responses (Figure 2). The 3 most frequent coded themes for emotional reactions were (1) no specified emotional reaction (n = 26); (2) sad/depressed (n = 17); and (3) difficult/challenging, heartened/encouraged, mixed emotions (each occurring with an equal frequency of n = 11). Among the codes with lower frequencies, emotions in the positive realm (peace/calm; impressed; happy/joy; total n = 14) had a greater frequency compared to those in the negative realm (anxious/nervous; troubled; afraid/scared; total n = 6). Illustrative examples of student entries for each of the frequently occurring codes for prompt #2 are shown in Table 4.
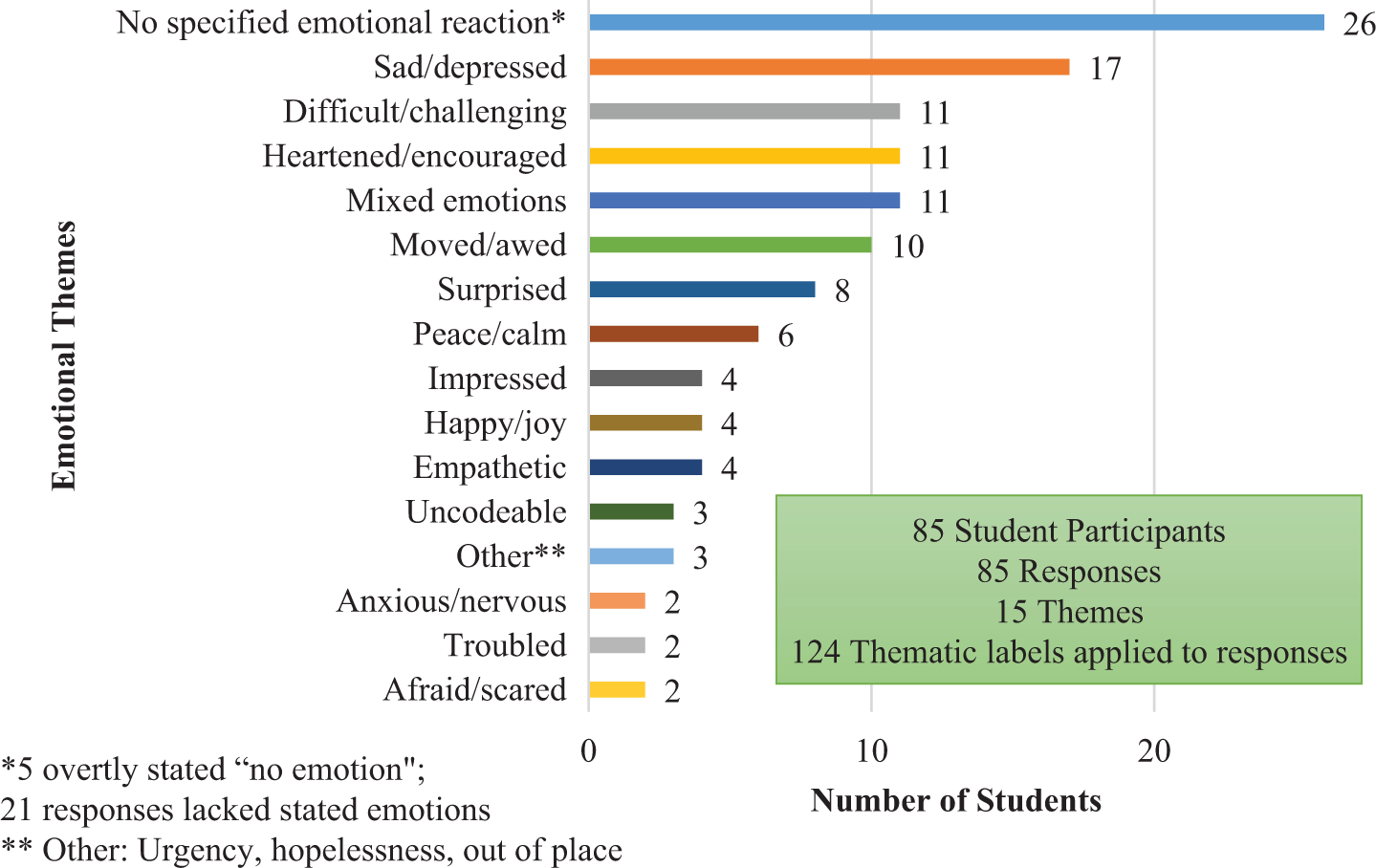
Fifteen emotional reactions emerged from the 85 responses submitted by 85 students (n). The majority of students reported no specified emotional reaction (30%, n = 26), followed by “sad/depressed” (20%, n = 17), “difficult/challenging” (13%, n = 11), “heartened/encouraged” (13%, n = 11), and “mixed emotions” (13%, n = 11). One hundred twenty-four coded labels were applied, with some responses receiving more than 1 label.
Illustrative Examples of MS-2 Emotional Responses to Prompt #2 “Briefly Describe Your Emotional Reaction to Seeing a Terminally Ill Patient at Hospice,” by Themes.
Abbreviation: MS, medical student.
Discussion
To our knowledge, ours is the first study to report on both the educational and the emotional responses of preclinical MS-2s to a required HCE. Our in-depth thematic analysis of students’ prompted written reflections elucidated a range of the educational and emotional responses to an early hospice exposure. We found that a required, time-limited HCE facilitated by a hospice clinician was a feasible and impactful learning opportunity for preclinical students.
Regarding the learning impact of the HCE, a majority of students reported learning core aspects of hospice services, goals, and care. A variety of other self-reported learning points were defined, including aspects of bedside practice, diversity of patients’ response to dying, EoL communication, the importance of family, and the management of terminal symptoms.
Students reported a broad spectrum of emotional reactions, in both the positive and the negative realms as well as mixed emotional responses to seeing terminally ill patients. Notably, positive types of emotional reactions exceeded negative types, and if one considers the responses in the categories of “sad/depressed” and “difficult/challenging” to be expected and appropriate, only a small minority of coded responses (6 of 124) reported negative emotional reactions (anxious/nervous; troubled; and afraid/scared) which would be of more concern to educators. Debriefing opportunities with experienced hospice clinicians were deliberately built into the experience to facilitate discussion and processing of students’ emotional reactions.
One striking finding in this analysis was that despite the explicit instructions in prompt #2 to report on their emotional reactions to seeing a terminally ill patient, nearly one-third of students (26 of 85) either reported overtly that they had no specified emotional reaction (5 students) or we found that their responses lacked any emotional content (21 students). We speculate that this may reflect that rather few occasions exist in the curriculum prior to the HCE when students are triggered to reflect on their own emotions. However, we acknowledge that further investigation is warranted to understand what factors may underlie this observation and what triggers are adequate for students’ self-reflection.
Our analysis of students’ educational and emotional responses complements the findings of previous studies. Wechter et al 29 found that a program where MS-1s directly observed EoL care had positive effects on the students’ attitudes toward the care of dying persons. Our study’s findings also showed some thematic similarities with previous studies of hospice-based electives which included preclinical students. For example, Mott et al 32 reported on the thematic content of MS-1s’ reflective essays written after volunteering with assigned hospice patients. These essays showed 5 salient themes: perceptions of hospice patients, personal feelings and reactions, amazement at normalcy of dying at home, impact of witnessing death and dying, and ideas for improving the EoL care curriculum. Shunkwiler et al 36 found that MS1-4s who elected to participate in volunteer training followed by hospice patient visits reported increased comfort levels of being with and talking to patients at the EoL.
The spectrum of emotional reactions to seeing terminally ill patients in our study stands in contrast to a study of preclinical students’ anticipated affective responses to the death of a future patient. 12 These anticipated responses often included fear, frustration, guilt, and sadness. 12 Our study found that observing actual hospice patients elicited positive, negative, and mixed emotions. A preclinical observational program allows students to interact with hospice patients in a “nonclinical” capacity, without concerns of having to focus on clinical management as in the later years of training. An early HCE may alter students’ preconceptions about caring for the terminally ill and thereby enhance their engagement with these patients during their clinical years. In this way, an early HCE that exposes students to hospice care and facilitates reflection on their emotional responses may help to mitigate students’ feelings of lack of preparedness for the difficult emotional reactions they experience when caring for dying patients in the clinical years. 19,37,38 Similarly, by equipping students with an understanding of the goals and benefits of hospice care, an early HCE may “inoculate” them against the negative effects of challenging EoL cases in future clinical rotations. We have anecdotally observed students who completed the HCE take the lead in suggesting the option of hospice care for terminally ill inpatients to their ward team.
The HCE contains many of the features promoted in optimal palliative care education: It is required, integrated, supervised, experiential, and dedicates time for debriefing and self-reflection. Reflective learning may enhance students’ development of professionalism 39 –41 and is particularly relevant for preparing students for competency in palliative and EoL care. 10,15,24 Emotion influences reflection itself: When emotion is the object of reflection, it can foster self-awareness in the learner. 42 Enhancing self-awareness contributes to improving skills in challenging clinical communication 43 and developing mindful practice, which can reduce the risk of burnout. 44
Limitations
Although we analyzed 260 responses from 85 students, the reflection response rate was <50%, so we would take caution when generalizing the findings to all MS-2s. In addition, we are unable to ascertain whether a specific hospice site or clinician influenced the thematic content of the students’ reflections. Nonetheless, we found consistency of educational and emotional themes to prior studies of hospice educational interventions. 29,32,36
Conclusion
An early HCE can introduce preclinical medical students to the core aspects of hospice care and philosophy. Students demonstrated a wide spectrum of emotional responses when spending time in the presence of terminally ill patients. These results provide support for introducing an HCE in the preclinical years and can aid educators in anticipating the spectrum of students’ educational and emotional reactions to an early HCE. We believe debriefing opportunities combined with self-reflection are important components of any experiential, learner-centered palliative or EoL curriculum. This type of early HCE may help prepare students for EoL care experiences in the clinical years by promoting the acquisition of more comfort with and knowledge about hospice care.
Footnotes
Acknowledgments
The authors thank Dr. W. Scott Long, Dr. Joseph F. Andrews, and all the clinicians and administrators at The Connecticut Hospice; Dr. William H. Zeidler and all the clinicians and administrators at the Middlesex Hospital Hospice and Palliative Care Program; the Yale Medical Students; and Dr. Margaret Bia, former director of Clinical Skills at Yale School of Medicine.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Alexandra K. Munroe Fund, Yale School of Medicine.