
Abstract
Purpose:
Evidence has demonstrated the positive effects of music therapy on symptom management for palliative medicine patients. Previous studies have addressed patient needs, with limited discussion involving the relationship between interventions utilized to improve symptoms. The purpose of this study was to understand the impact of music therapy sessions; identify common music therapy goals and interventions and assess their effect; and investigate the effects of gender, age, and type of cancer on symptoms in patients who experienced music therapy.
Methods:
This was a retrospective study of data collected during music therapy sessions. Patients scored their symptoms (pain, anxiety, depression, shortness of breath, and mood) before and after sessions. Data collected from over 1500 patients included symptom evaluation, goals, interventions, music used, patient/family reactions, and narratives.
Results:
Among 293 patients who met all study inclusion criteria, significant improvement in pain, anxiety, depression, shortness of breath, mood, facial expression, and vocalization scores was noted. In addition, 96% of patients had positive responses to participating in music therapy. Vocal and emotional were the 2 most effective interventions in improving symptoms. All 5 patient-reported symptoms improved when the therapist focused on these symptoms as goals. Age, gender, and diagnosis had no impact on symptom improvement.
Conclusions:
This study demonstrated the importance of music therapy for addressing symptoms and behaviors of palliative medicine patients. Statistically and clinically significant effects were noted. The most effective interventions were identified. More research needs to be conducted to better understand the benefits of music therapy for palliative medicine patients.
Introduction
Music has been used in treating patients since biblical and ancient days of Plato, Hippocrates, and Alpharabius. 1 It was used by Native Americans to address mood, spirituality, emotional disturbances, neurological disorders, and unhealthy souls, and it was used from the Middle Ages through the 17th century for its preventative, curative, and psychological value. 1,2 More recently, it has been used by music therapists to help address patients’ social, physical, emotional, psychological, and spiritual needs. 3
Music therapy is an evidence-based practice in which board-certified music therapists (MT-BCs) work within a therapeutic relationship to address patients’ individualized goals. 4 Kordovan et al 5 found that music therapy was rather or very helpful in 68% of the patients on their inpatient palliative care unit and that those who died there indicated they drew strength from music therapy (P = .0007). Research has demonstrated the effectiveness of music therapy in addressing pain, fatigue, comfort, relaxation, and shortness of breath in palliative medicine patients. 2,3,6 –14 It has also addressed anxiety, depression, sadness, grief, hope, stress/distress, and mood. 2,3,6 –14
Music therapy has been used in palliative medicine to enhance quality of life; communication; coping; and expression of feelings such as fear, loneliness, anger, and isolation. 2,3,5 –15 Finally, it has been used to support patients and families during the actively dying process. 6,12 Any of these physical, social, psychological, emotional, and spiritual needs may be addressed by music therapists.
Music therapy interventions have included music-assisted imagery, instrument playing, music listening, choosing songs, music-assisted relaxation/imagery, singing, musical life review, song-writing, entrainment, lyric analysis, improvisation, and verbal processing. 2,5,8,9 These interventions can commonly be categorized as receptive, recreative, creative, or combined, and the patient’s participation level depends upon his or her level of energy and symptom management at the time of the session. 2,6,9
Gutgsell et al 9 used 1 intervention of live music paired with autogenic relaxation exercises guided by the MT-BC. Patients who regularly sang, previously played an instrument, previously participated in music therapy, or significantly felt music played a role in their lives appeared to benefit more from active music therapy; however, there was no significant correlation between any of these factors and the intervention that was chosen. 5
An active music therapy program has been in place since 1994 on the Harry R. Horvitz Center for Palliative Medicine at the Cleveland Clinic where music therapy is offered free of charge. A rich database has been collected since the beginning of the program with our past studies demonstrating that music therapy is effective in improving anxiety, depression, mood, pain, shortness of breath, facial expression, body movement, and verbalization. 7,8 However, the effects of patient characteristics, patient goals of music therapy, and music therapist interventions have not been studied in depth relative to these outcomes. This study was designed to address this gap.
The objectives of this study were (1) to describe patient characteristics, patient goals, and interventions used by the music therapist; (2) to assess the impact of music therapy sessions on outcomes; and (3) to identify which patient characteristics, goals, and interventions had an effect on outcomes. Patient-reported outcomes included changes in pain, depression, anxiety, shortness of breath, and mood before and after the music therapy session. Therapist-reported outcomes included changes in facial expression, body movement, and vocalization.
Methods
Participants
This study was approved, and a waiver of informed consent granted, by the institutional review board at The Cleveland Clinic. All procedures followed were in accordance with the Helsinki Declaration of 1964 and its later amendments or comparable ethical standards. 16 Patients included those admitted to the Horvitz Center and those followed by the Palliative Medicine consult service on other acute inpatient units at the Cleveland Clinic. This was a retrospective study of data obtained from music therapy sessions with these patients held between September 2000 and May 2012. These data can be accessed as necessary by the authors upon request. All palliative medicine patients were eligible to receive music therapy sessions. They could request it themselves or could be referred by physicians, nurses, social workers, physician assistants, chaplains, nursing assistants, music therapists, psychologists, and/or family members. Data collected was entered into a password-protected database on a secured drive on the hospital computer. During the data analysis stage, the data were downloaded into an Excel spreadsheet and deidentified in order to maintain patient anonymity and confidentiality.
Sessions/Procedures
One of the board-certified music therapists (MT-BCs) who worked on the palliative medicine unit conducted a music therapy session with individual palliative medicine patients and any family members present. More than 1 goal may have been addressed per session. A variety of interventions were used, with more than 1 being utilized in the majority of sessions. These interventions were consolidated into 6 main categories: music listening, verbal/cognitive participation (eg, music discussion, choices, songwriting, etc), vocal participation (eg, singing and humming), physical participation (eg, playing instrument, clapping, tapping foot, etc), verbal/emotional participation (verbal processing, musical life review, lyric analysis, etc), and music-assisted relaxation. Live, patient-preferred music was utilized in the majority of the sessions. Our experience and the literature have suggested that patient-preferred music has the best effect for patients. 15,17
Data Collected
Data collected on all patients who agreed to participate in music therapy was included in the music therapists’ clinical notes in the patients’ medical records and was documented in a computerized database on a secured drive utilizing FileMaker Pro (FileMaker, Inc, Santa Clara, CA, USA). 18 This clinical database was created prior to the implementation of electronic medical records. Data included the standardized music therapy assessment, elements of the standardized music therapy clinical note, patient-related information (Table 1), patient goals for the music therapy session, interventions used by the music therapist, symptom evaluations from the patient, behavioral evaluation from the music therapist, music used, patient and family member reactions, and narratives. Specifically, patient-related information included age, gender, diagnosis, reason for referral, and referral source. Symptom evaluations from the patient included pre- and postsession severity of pain, depression, anxiety, and shortness of breath, all of which were rated on a 0- to 10-point scale and mood which was rated on a 0- to 4-point scale based on the Rogers Happy/Sad Faces Assessment Tool. 19 The music therapist scored 3 behavior variables on a 0- to 3-point scale before, during, and after the music therapy session (facial expression, body movement, and vocalization) based on the Nursing Assessment of Pain Intensity 20 and the Riley Infant Pain Scale. 20 For all of these assessments, higher scores represent worse outcomes. The outcome measures were used in prior studies, but they have not yet been validated.
Patient and Music Therapy Characteristics.
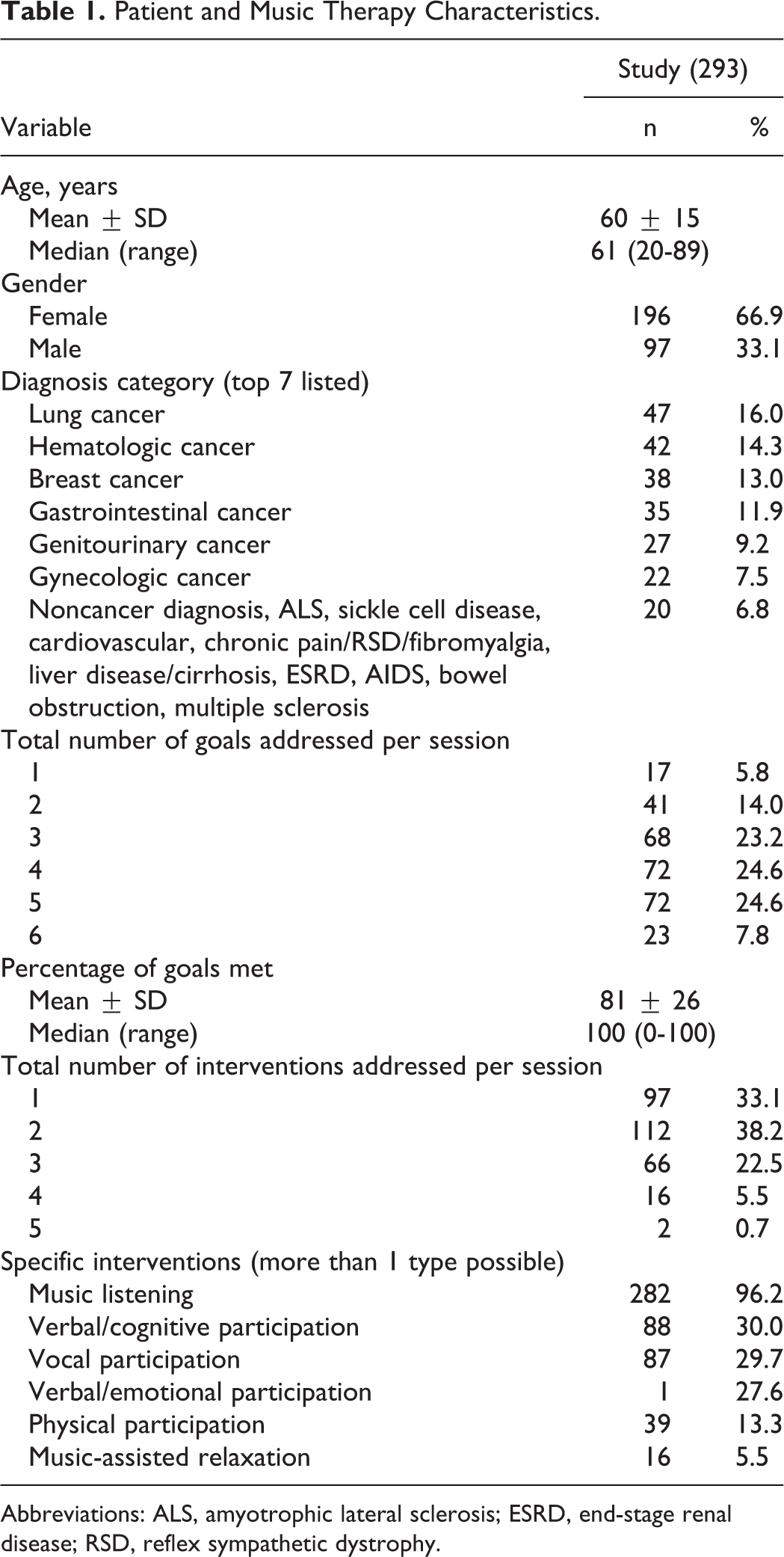
Abbreviations: ALS, amyotrophic lateral sclerosis; ESRD, end-stage renal disease; RSD, reflex sympathetic dystrophy.
Study Inclusion
The music therapy database contained 5970 music therapy sessions from 1570 patients. Inclusion criteria for this study consisted of patients being at least 18 years of age and having at least 1 patient-reported rating of pain, depression, anxiety, shortness of breath, or mood before and after the music therapy session. Only the first session with data was included in this study for patients who had more than 1 session. This inclusion resulted in a total of 547 patients. Among these, 293 patients had complete data on all primary outcomes measures and were included in the data analysis.
Statistical Considerations
Categorical variables are described using frequency counts and percentages and continuous variables using mean, standard deviation, median, minimum, and maximum. Limited demographic comparisons were made between 293 study patients and 254 who were excluded for incomplete outcome data to make sure there were no apparent exclusion biases and were found to be similar (P = .90 age, P = .55 gender, P = .67 diagnosis; results not otherwise shown). Changes in the 5 patient-reported outcomes and 3 therapist-reported outcomes before and after the music therapy session were compared using the paired t test. Multiple linear regression analysis was used to assess the effect of gender, age, type of cancer, goals, and interventions on the change in each of the 8 outcome scores. For the purpose of this analysis, diagnosis was categorized as cancer of not cancer, while goals and interventions were categorized as present or absent. Goals or interventions occurring in <5% of patients were not included in the analysis. Regression results are reported as the parameter estimate and P value to indicate if the parameter estimate differs from 0, where 0 represents no effect of the variable in question. Parameter estimates indicate the change in outcome score for each variable. Because higher scores represent worse outcomes, positive parameter estimates indicate that the outcome score worsened (increased) and negative estimates indicate that the score improved (decreased). Clinical relevance is a topic of much debate, and previous authors have determined that it depends on how severe the initial rating is, how much of a change occurs, and the patient’s perception of the change. 21,22 Therefore, we arbitrarily decided that a change of 2 points was considered to be clinically relevant on variables measured on a 10-point scale, and a change of 1 point was considered relevant on variables measured on a 4-point scale. As another way of summarizing outcome data, the 8 primary outcomes were described as the number and percentage of patients whose scores improved, stayed the same, or worsened and as the number and percentage with clinically relevant improvement. Basic data description was conducted with the tools built into FileMaker Pro. All other analyses were done with SAS software (SAS Institute, Inc, Cary, North Carolina). All statistical tests were 2 sided, and P < .05 was used to indicate statistical significance.
Results
Patients were primarily female (67%), with a median age of 61 years and a cancer diagnosis (93%; Table 1). The most common diagnoses were lung cancer (16%), hematologic cancers (14%), breast cancer (13%), and gastrointestinal cancer (12%). The top 5 referral sources included social workers (32%), physicians (18%), physician assistants (13%), patient availability (12%), and nurses (11%). In order of frequency the top 5 reasons for referral included enjoyment (23%), anxiety, (16%), pain (13%), depression (12%), and support (7%).
Of the 287 who identified their preferred style of music, 37 different styles were identified. The top 5 styles of music were gospel/religious (19%), various/any (16%), country western (11%), semiclassical/ classical (8%), and jazz/Frank Sinatra (8%). Other styles included rock various decades, musicals, and hip hop. In addition to the religious music mentioned earlier, Jehovah Witness and Jewish music were also utilized. Various ethnic music used included polkas, Irish, Native American, Brazilian, Spanish, and Filipino.
Twenty total goals were identified in all patients (Table 2), with individual patients having 1 to 6 goals (Table 1). The music therapist documented whether goals were met, but if unknown, they were considered to be unmet. One to 5 interventions were utilized per session, with at least 1 or 2 being utilized in 71% of sessions (Table 1).
Goals of Music Therapy (Ordered From Most to Least Common).a
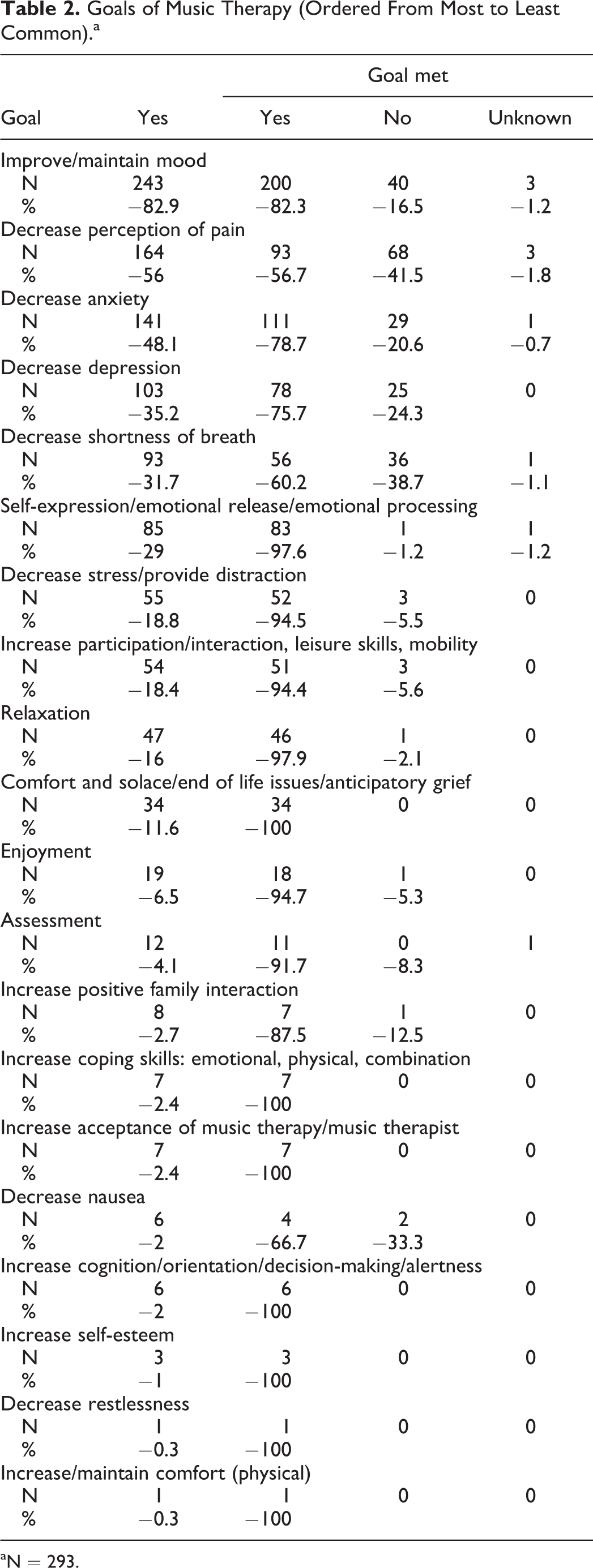
aN = 293.
There were statistically significant reductions (improvements) in pre- to postsession mean scores for all measurements except body movement (Table 3). However, the percentage of patients reaching the clinical significance threshold ranged from 0.7% (body movement) to 66.2% (mood; Table 4). Ninety-six percent of patients had a positive verbal response to the session, with the remaining 4% having an ambivalent or no verbal response.
Continuous Assessment of Score Changes.a
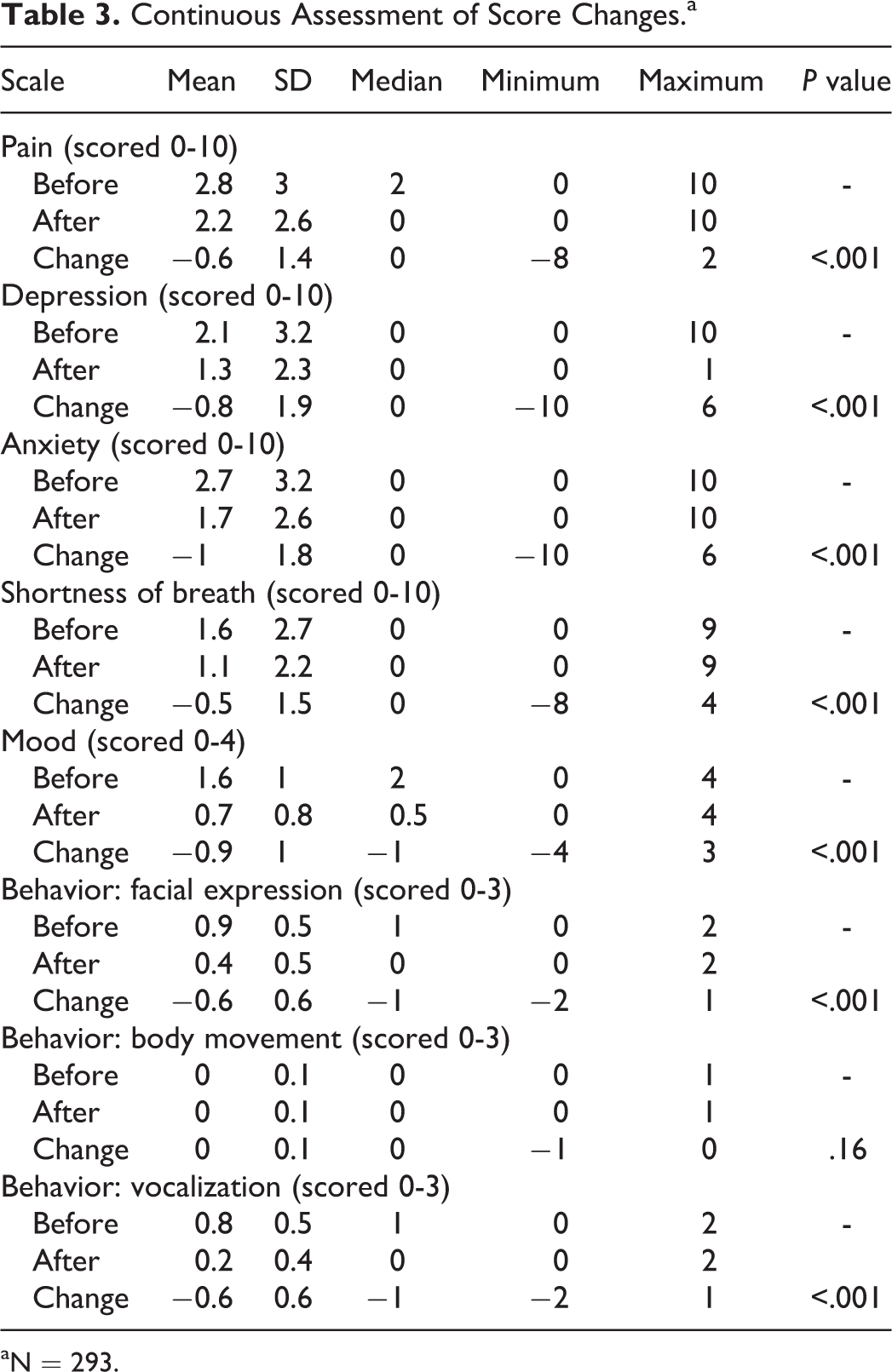
aN = 293.
Categorial Summary of Score Change.a
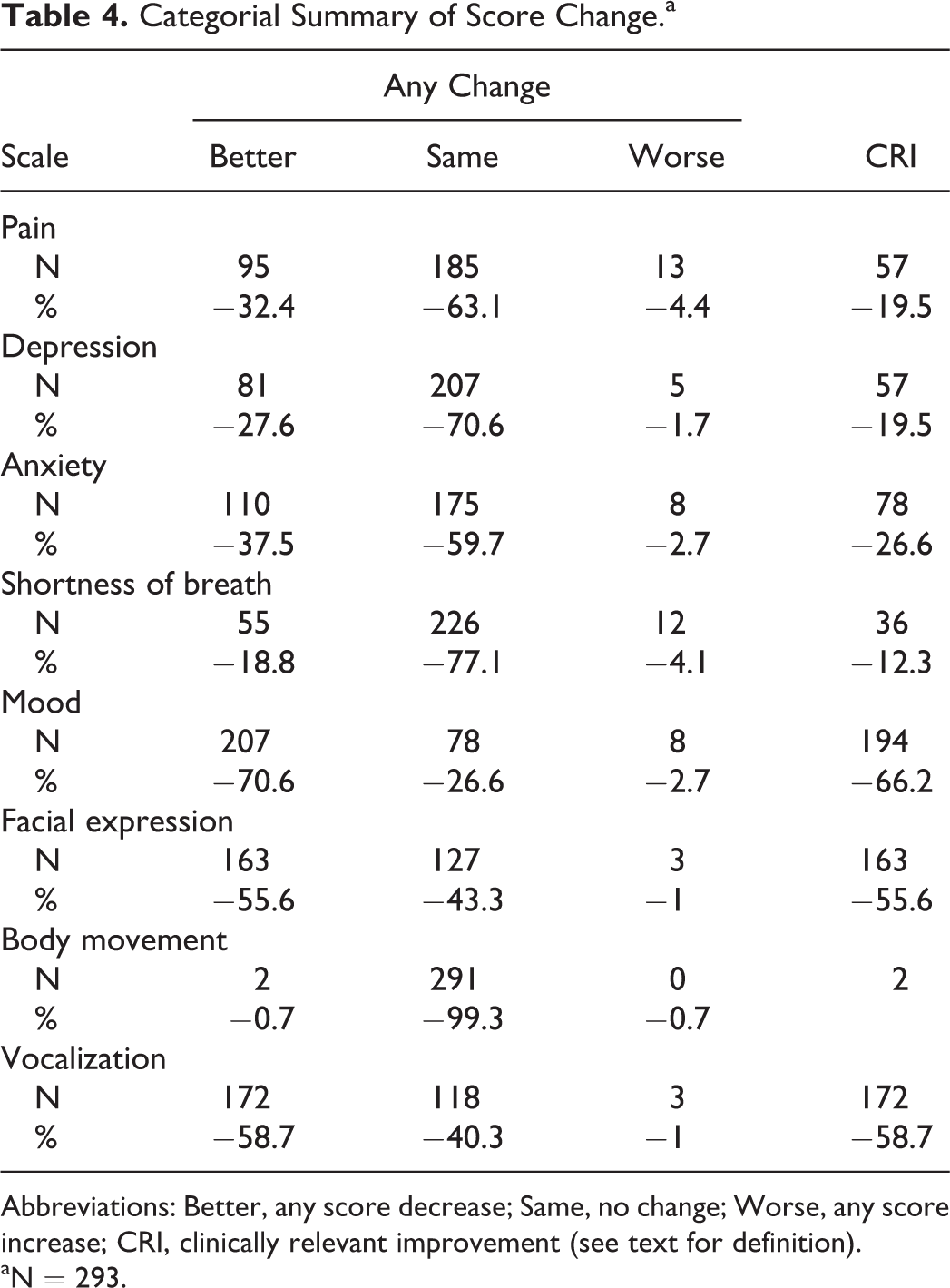
Abbreviations: Better, any score decrease; Same, no change; Worse, any score increase; CRI, clinically relevant improvement (see text for definition).
aN = 293.
Twenty variables were included in multiple linear regression analysis to determine their effect on change in each of the 8 scores (Tables 5 and 6). The most improvement in pain, depression, anxiety, shortness of breath, and mood was seen among patients who had each of these goals for their music therapy session. In addition, utilizing a vocal intervention also improved depression, anxiety, and mood while a verbal/emotional intervention improved mood. Facial expression significantly improved when vocal, emotional, and physical interventions were used. Vocalization significantly improved when a verbal/emotional intervention was used and when distraction was a goal of music therapy. No variable was associated with body movement. The demographics and cancer diagnosis had no impact on outcomes.
Multiple Linear Regression Models for Pain, Depression, Anxiety, and Shortness of Breath.a
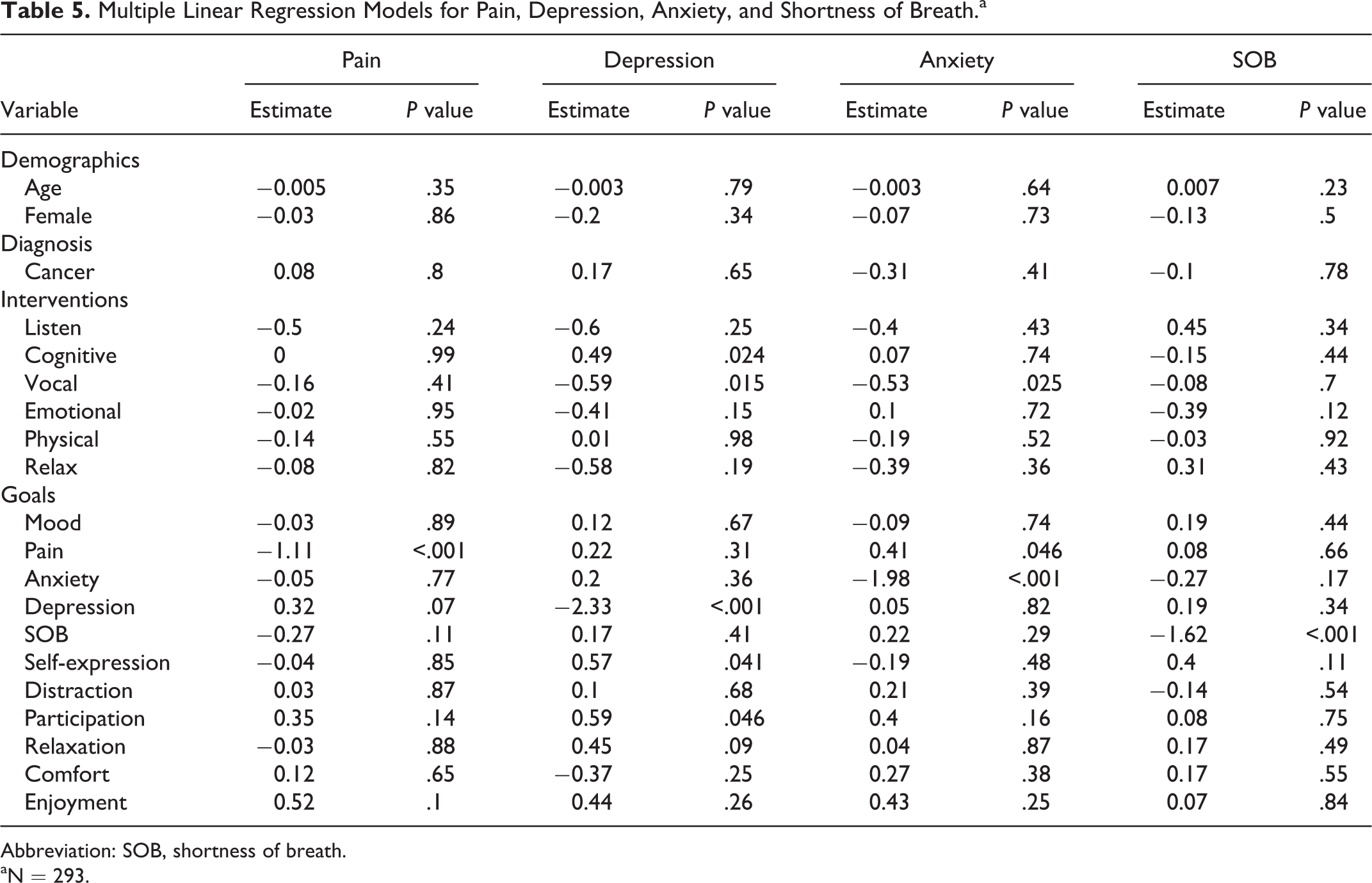
Abbreviation: SOB, shortness of breath.
aN = 293.
Multiple Linear Regression Models for Mood and Behavior.a
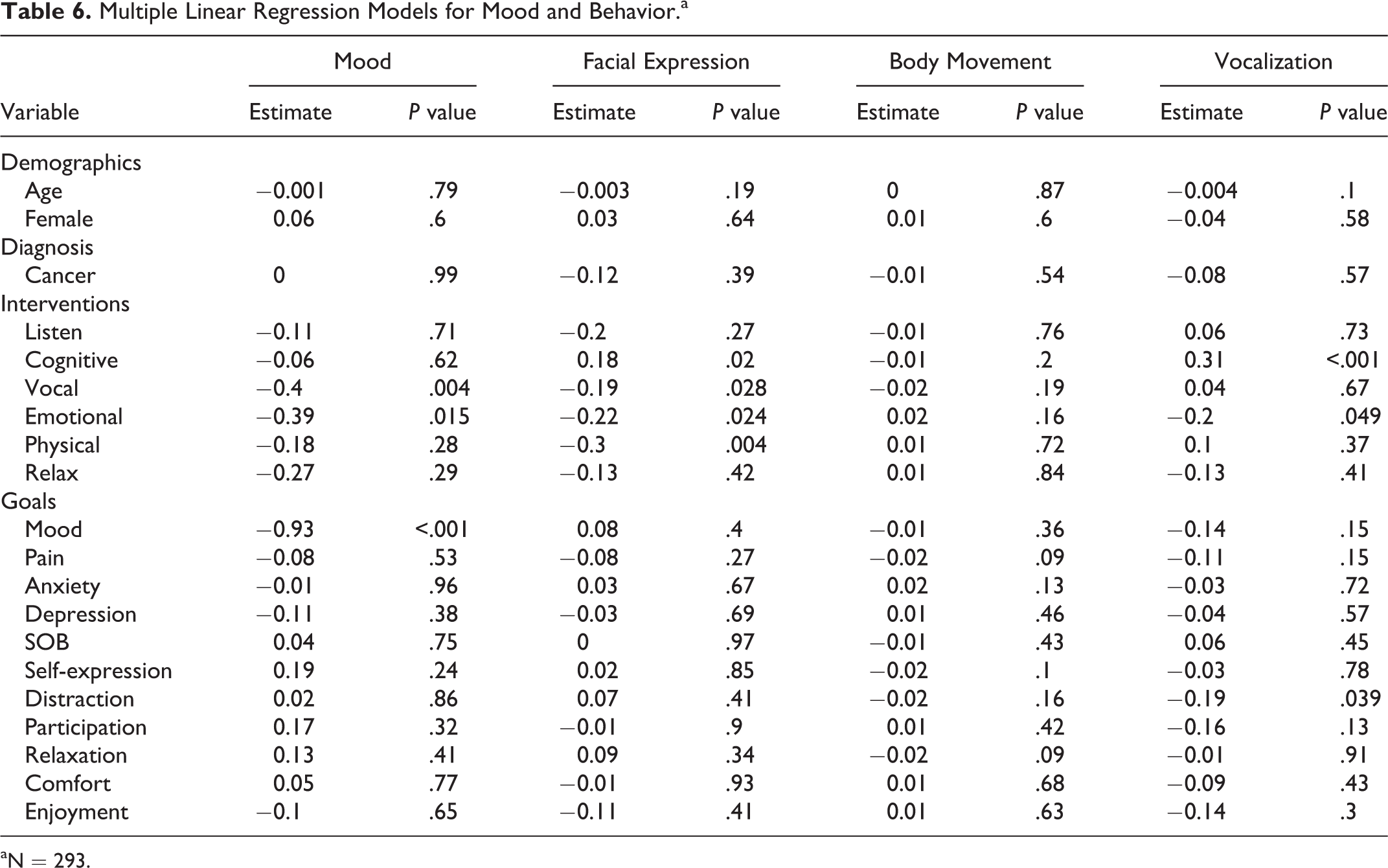
aN = 293.
Discussion
Music therapy was found to improve pain, anxiety, depression, shortness of breath, mood, facial expression, and vocalization at a statistically significant level (P < .001). The variables with the highest percentage of patients reaching a clinically relevant improvement were mood, vocalization, and facial expression. These results were consistent with our previous findings. 7,8
Although results were positive overall in addressing numerous goals with various interventions while attempting to improve 8 variables, some results were more positive than others. Based on the findings it can be concluded that vocal and verbal/emotional interventions have the most impact on improving symptoms. It was found that mood, pain, anxiety, depression, and shortness of breath all improved when the MT-BC specifically focused on these symptoms as goals.
In addition, the music therapists on the palliative medicine unit were often called in to assist with patients who were having extreme pain or who were having difficulty expressing their emotions. The music therapist was often seen as someone in which patients could easily confide, as they did not wear white coats and brought something aesthetically pleasing into the room. It was also noted on many occasions by the staff of the unit that once patients worked on difficult emotional or existential issues with the music therapist their physical pain often decreased. These anecdotal observations, combined with aggregate outcome data, strongly suggest that MT should be an integral part of the palliative care team.
This study is the largest of its kind in utilizing music therapy to address symptom management in palliative medicine. The study is unique, however, in that for the first time the results were compared to age, gender, diagnosis, interventions, and goals and that some of the results were significant at P ≤ .05. This supports that while we take age, gender, and diagnosis into consideration, what we are doing is working and we do not need to do anything different based on these variables. Specific intervention categories were identified and their effectiveness in meeting specific goals was ascertained. This study contains a large amount of data, calculated utilizing different methods in order to pinpoint the findings and identify the clinical and statistical significance of the results.
There are, however, some limitations. One is the use of observational behavioral data, which could be considered biased as it is based on the therapist’s opinion. Although only 1 MT-BC worked on the unit at 1 time, and all were trained by the original MT-BC, it is possible that they did not all interpret their observations in the same manner, and interrater reliability of the rating scales was not assessed. We collected data across a wide range of years, during which standards of care in palliative medicine have evolved. On the other hand, this time range allowed us to achieve a larger sample size. The MT-BC collected the pre- and postsession data, which could also be considered biased. If the MT-BC felt the patient was trying to skew the results, she would tell the patient she was looking for honest responses even if they did not appear favorable. Although this form of data collection may increase the opportunity for bias, it is realistic for clinical practice.
Another limitation is missing data in patients who experienced severe pain or high anxiety, were actively dying, had fallen asleep, or sessions were interrupted. Although the MT-BC often hung a sign on the door indicating that a music therapy session was in progress, sessions were still interrupted by patient transporters, physical therapists, nurses, and physicians. Many interruptions were brief and sessions could continue; however, many took several minutes. Although this sometimes negatively affected the postsession data, it often provided an opportunity for the patient to express feelings and process what was happening. There were also times when it was difficult or inappropriate to initiate the use of the scales such as when the patient was reluctant, confused about the scales, or stated they did not have the symptoms.
The 10-point scales were utilized for ease of use and patient understanding. Further research could validate these scales against existing validated scales for anxiety, depression, and so on. Other research is needed regarding the cost-effectiveness and duration of effect of music therapy as well as more in-depth look at the specific interventions used to address goals. Due to the possible impact of music therapy on patients in palliative medicine, it is necessary for more research to be conducted regarding the efficacy and value of music therapy to the institution, the patient, and the patient’s family.
Conclusion
This study demonstrated the importance of music therapy for addressing symptoms and behaviors of palliative medicine patients. There was a positive effect on pain, anxiety, depression, shortness of breath, mood, facial expression, and verbalization. In addition, the connection between the effect on change in each of the variables as compared with age, gender, diagnosis, goals, and interventions was identified. This will be an important addition to the literature. Based on these, as well as our previous findings, it is recommended that music therapy be utilized in palliative medicine settings to aid in symptom management.
Footnotes
Authors’ Note
The authors had full access to all of the data in this study, and we take complete responsibility for the integrity of the data and the accuracy of the data analysis.
Acknowledgments
The authors wish to acknowledge Dr Francois Bethoux for his support and help; Maria Jukic for her support; and the various music therapists and music therapy interns who conducted the music therapy sessions for our patients.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors wish to thank The Kulas Foundation and the Jack Belcher Music Therapy Fund for financial support which made this research possible.