
Abstract
Background:
Physician Orders for Life-Sustaining Treatments (POLST) is an advance care planning (ACP) tool that is designed to facilitate End-of-Life (EoL) care discussions between a medical provider and a terminally ill patient. It is often used as a tool to translate care wishes into a medical order, which can be honored across healthcare settings. With an increased utilization of the POLST paradigm in various healthcare settings along with continued dissemination across the nation, it is critical to examine whether documented wishes on POLST are concordant with subsequent care delivered. Purpose of this article was to examine concordance rate between POLST and subsequent care delivered in any care settings and communities.
Design:
Systematic review.
Results:
Of 1,406 articles identified, 10 articles met inclusion criteria. Together, included studies represent 5,688 POLST forms reviewed from individuals residing in a total of 126 nursing care facilities, 9 elderly care centers, 4 community settings, and 2 hospitals. Preference for cardiopulmonary resuscitation and actual delivery/ withholding of resuscitation was the most observed intervention in study of concordance (n = 8). It is also where highest concordance rate (97.5%) was reported. Seven studies compared care provided during EoL and the level of medical intervention requested on POLST forms (91.17% concordance). Preference to use artificial nutrition/ hydration, and actual delivery was 93.0% (n = 4 studies), and antibiotics use preference and delivery was 96.5% (reported in 4 studies).
Conclusion:
Published literature evidence suggests that EoL care wishes documented on POLST forms were largely concordant with subsequent care delivered. Additional research is needed to evaluate concordance between POLST documentation and care received among POLST users, who experienced multiple care transitions across healthcare settings, or across state during EoL care journey.
Introduction
In 2014, the Institution of Medicine (now the National Academy of Medicine) released a consensus report, Dying in America, which raised an awareness on the importance of providing high quality End-of-Life (EoL) care for those who are living with serious illnesses. In this report, appropriate EoL care was described as a vehicle that enhances quality of remaining life, and an essential factor to a more sustainable care system. 1 One of the conclusions called for an increased need for a state-wide adoption and active implementation of the patient-centered and communication-based advance care planning program, Physician Orders for Life-Sustaining Treatment (POLST). 1
The POLST program was first developed in early 1990s, to enhance the delivery of goal-concordant care among those who are living with frailty, and life-limiting illnesses. 2 The POLST form was specifically designed to facilitate EoL care discussions between a provider and a patient, and to encourage documentation of specific care wishes that align with one’s values, beliefs and care goals. What differentiated the POLST from other advance care planning tools (e.g., living wills or advance directives) was that documented care wishes on POLST forms become pre-signed actionable, and transferrable medical orders that can be honored across healthcare settings. 3
Often printed in a distinctive bright pink background, POLST form contains 3 key sections;
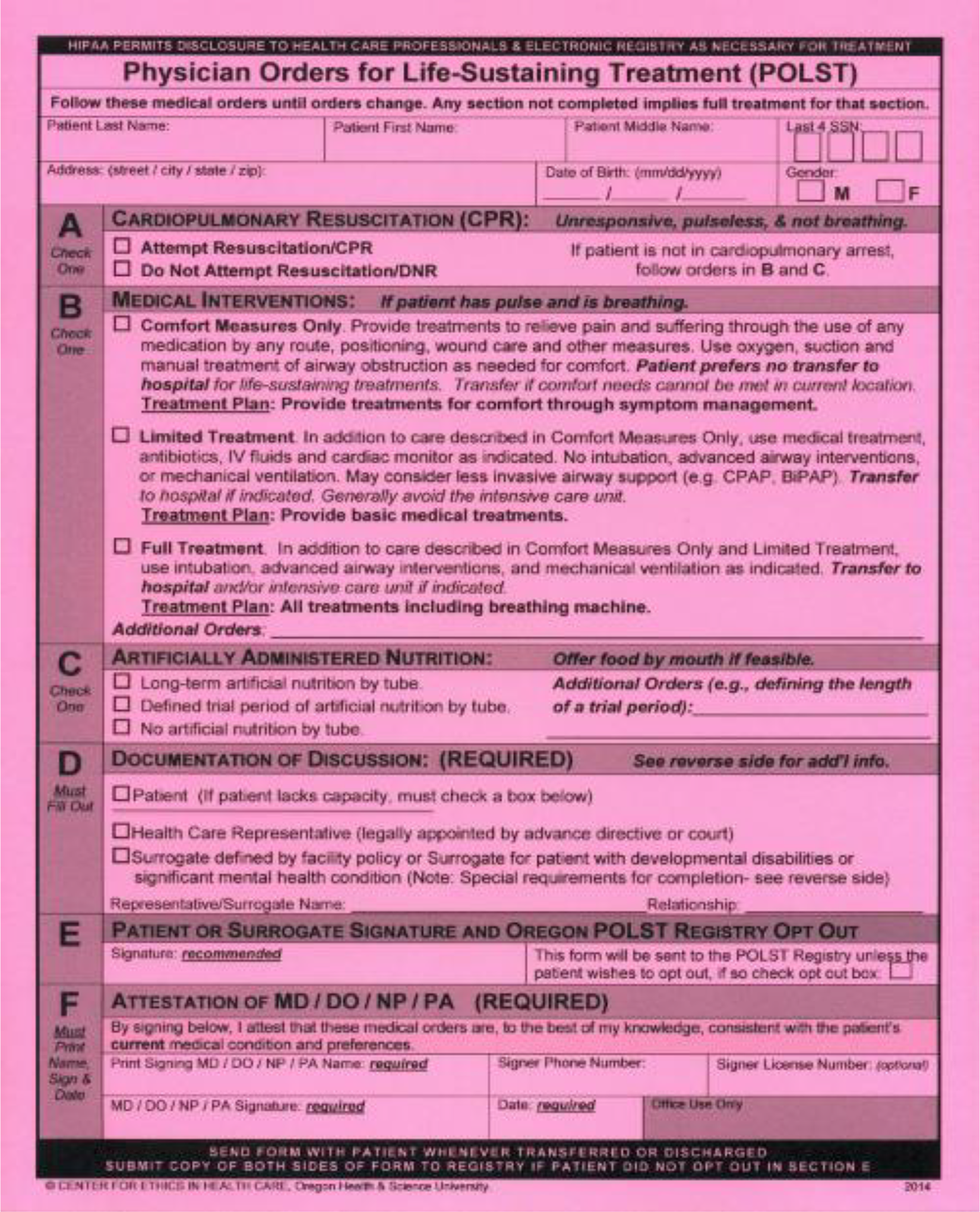
Sample POLST form.
Nearly 3 decades since the POLST program was first introduced, it has gotten increased attention across the nation. As of 2020, a majority of U.S. states have, or are developing a state-wide POLST program (n = 46, including Washington D.C.) and regional data from California, Oregon and West Virginia showed that the POLST program is actively being used in more than half of its regional medical facilities (e.g., hospices, nursing homes, and hospitals). 5 Moreover, scientific evidence indicating positive impacts of the POLST program (e.g., higher care satisfaction) on one’s EoL care journey continues to accumulate. For instance, POLST program usage was correlated with higher hospice service utilization, 6 -8 out-of-hospital deaths, 6,9 and higher likelihood of having treatment preferences documented as medical orders among older adults living with serious and/or terminal illnesses. 10 While current research evidence supports the association between POLST program and care outcomes that are indicative of high quality EoL care, there exists a gap in knowledge on whether the POLST documentation achieves what it was designed to achieve; deliver EoL care that are in concordance with documented care preferences.
In EoL care delivery, where honoring patient’s care wishes remain as a top priority, identifying concordance between POLST documentation and actual care delivered during EoL and/or at the time of patient death is highly important. Therefore, the objective of this systematic review is to examine published evidence to identify concordance between documented care wishes on the POLST form and actual care delivered to POLST users.
Methods
This systematic review followed the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).
Eligibility Criteria
Articles were eligible for inclusion if the authors examined the concordance between documented care wishes on POLST forms and subsequent/actual care delivered to patients. Other eligibility criteria included: studies that were written in the English; conducted in U.S.; used quantitative methods; and published in a peer reviewed journal. Studies were excluded if the authors examined: the patient and/or family satisfaction on POLST form usage and/or care delivered; the health care providers’ perspectives on the ease of POLST use; the legal or ethical issues surrounding advance directives; the effects of advanced care planning tools other than POLST (e.g., living wills and/or advance directives); or, the quality of POLST form completion. Editorials and qualitative studies were also excluded.
Search Strategy
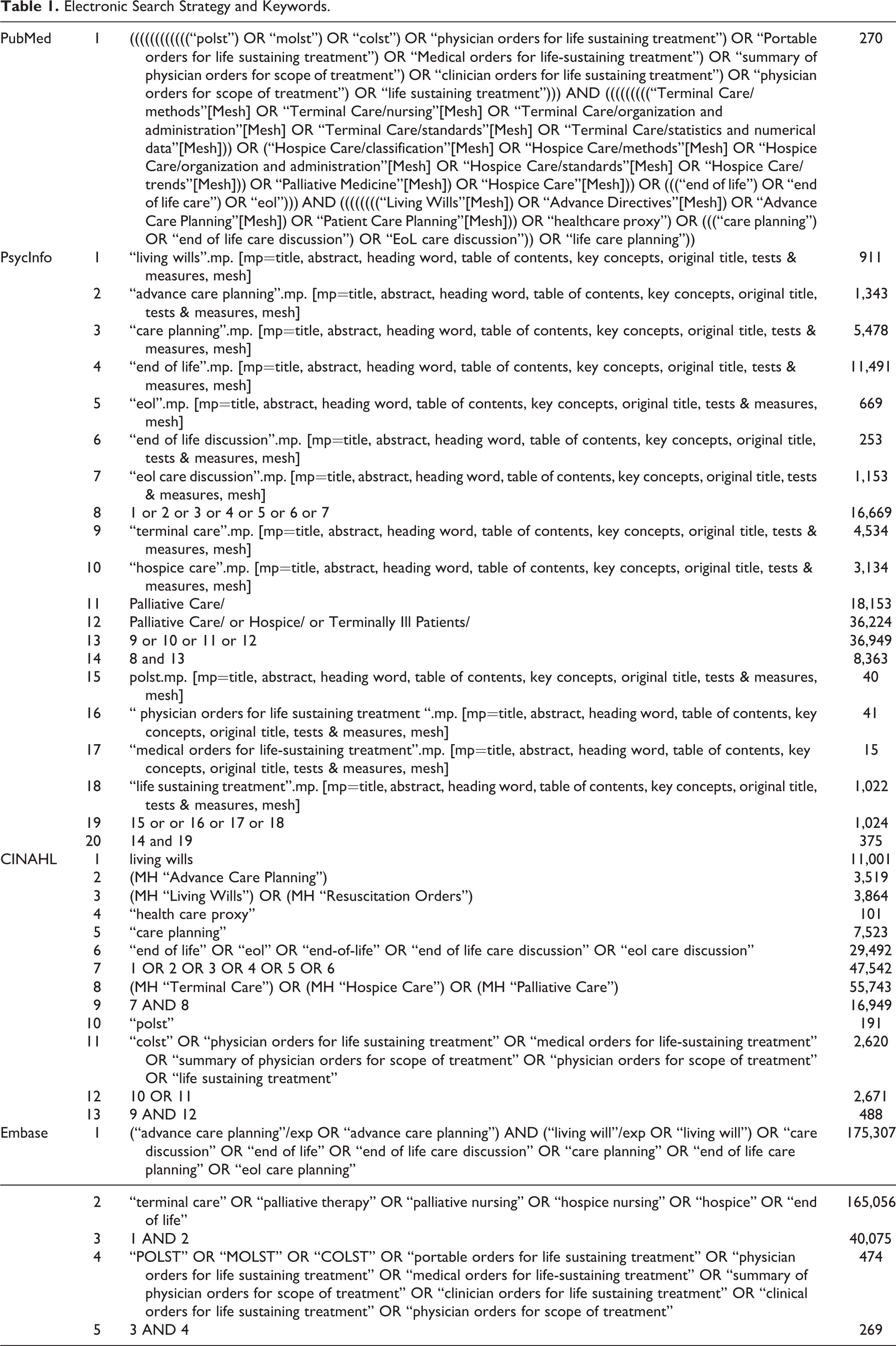
The literature search was conducted using 4 electronic databases: PubMed, PsycINFO, Embase, and Cumulative Index of Nursing and Allied Health Literature (CINAHL). A manual search of the reference lists to screen additional articles for eligibility was also conducted. After a consultation with a library informationist, a comprehensive search methodology was developed using free-text words and Medical Subject Headings (MeSH). Search terms included the following keywords: “Physician Orders for Life-Sustaining Treatment”, “POLST”, “MOLST”, “Advance Directive Adherence/Utilization”, “Advance Care Planning”, “Treatment Adherence and Compliance”, “End of Life Care Planning”, “Consistency”, “Congruence” and “Concordance”. Searches were not restricted by patient age, publication date, or care settings where the POLST user resided (e.g., home, nursing home, acute care facility, or hospice). This was to allow a comprehensive screening of articles that may meet our eligibility criteria. Table 1 contains a full list of search terms used for literature search. The initial search was conducted in February of 2019, then repeated again in August 2020 to ensure that all potentially eligible, and up-to-date articles are included.
Electronic Search Strategy and Keywords.
Study Selection
After removing duplicate articles, titles and abstracts were screened by 2 independent reviewers (AT, JS). When the article was deemed relevant, full text was obtained for further screening. Any discrepancies were resolved through a consensus discussion with a third reviewer (JP).
Data Collection Process
A standardized data abstraction tool included the following information about the manuscript demographics: title, last name of first author, and year study was published. Data audited on the study itself included: study design, data collection method, study setting, study region(s), sample number, sample characteristics, care intervention(s) examined for concordance (e.g., CPR, hospital transfer, Intensive Care Unit (ICU) admission, level of medical interventions (e.g., comfort-measures only, limited interventions, full treatment/life-preserving interventions), antibiotics and artificially administered nutrition. An evidence base table was developed to present the study characteristics and findings. Table 2 depicts overview of audited studies (i.e., study aim, design/ method, setting and important findings), and Table 3 contains detailed information on study characteristics (e.g., study region, sample number, demographics, participant criteria and outcome measured per each study).
Overview of Audited Studies.
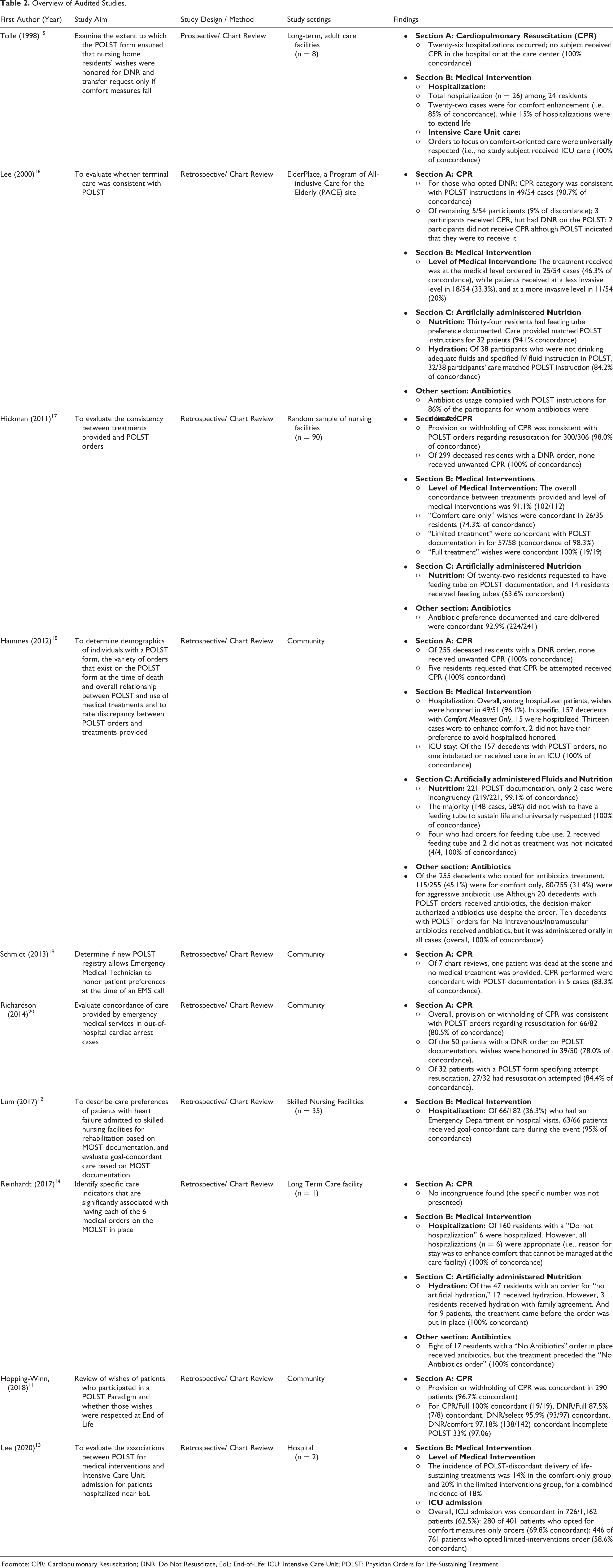
Footnote: CPR: Cardiopulmonary Resuscitation; DNR: Do Not Resuscitate, EoL: End-of-Life; ICU: Intensive Care Unit; POLST: Physician Orders for Life-Sustaining Treatment.
Study Characteristics.
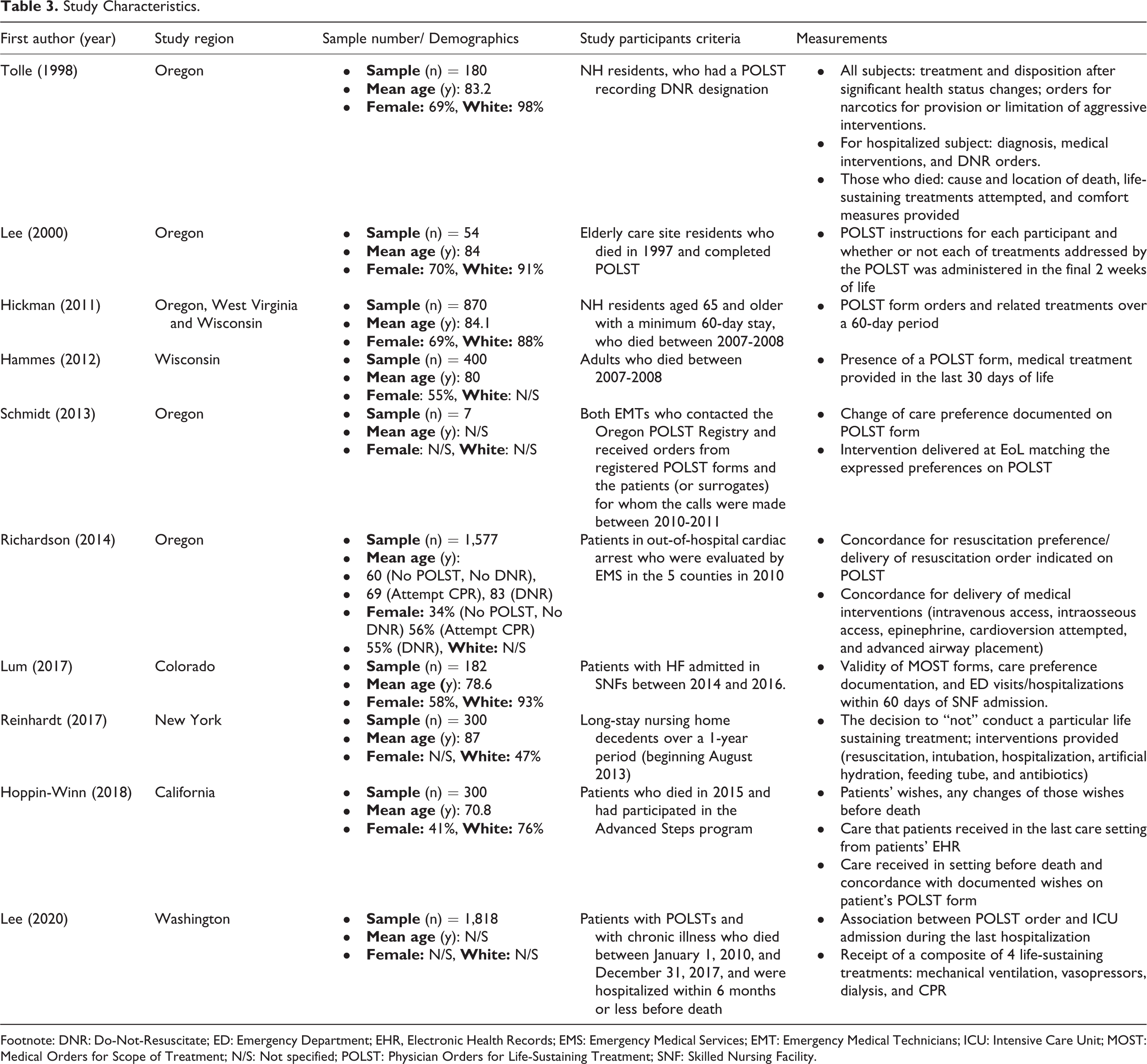
Footnote: DNR: Do-Not-Resuscitate; ED: Emergency Department; EHR, Electronic Health Records; EMS: Emergency Medical Services; EMT: Emergency Medical Technicians; ICU: Intensive Care Unit; MOST: Medical Orders for Scope of Treatment; N/S: Not specified; POLST: Physician Orders for Life-Sustaining Treatment; SNF: Skilled Nursing Facility.
Results
The search strategy yielded a total 1,406 results. After removing duplicated studies (n = 380), titles and abstracts reviews for 1,026 studies. One hundred and thirty-nine articles were deemed relevant to our study aim and were subjected to further review. After reviewing full-text of 139 studies, we found 10 studies that met eligibility criteria. PRISMA flow diagram is depicted in Figure 2.
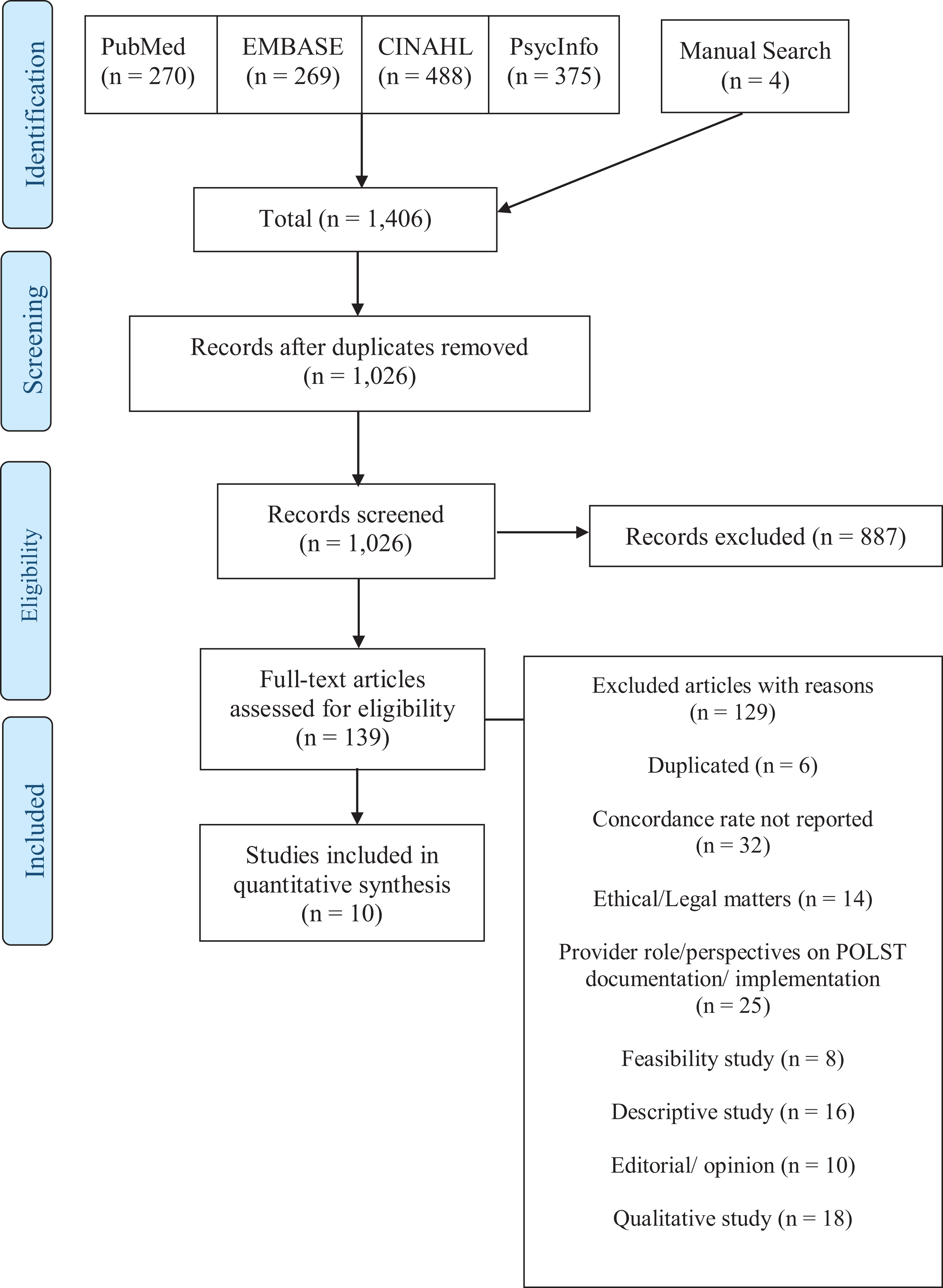
PRISMA flow diagram.
Overview of Included Studies
Four studies were published within the last 5 years, 11 -14 and the remaining 6 were published between 1998 and 2014. 15 -20 Most studies (n = 4) were conducted in Oregon, 15,16,19,20 and one study per California, 11 Colorado, 12 New York, 14 Washington, 13 and Wisconsin. 18 One study was conducted in multi-state setting (i.e., Oregon, Wisconsin and West Virginia). 17 While most study designs were retrospective cohort studies, 11 -14,16 -21 Tolle’s study was the only prospective study that collected data in real time and conducted chart reviews. 15
The combined study sample size was 5,688 individuals who documented EoL care wishes on POLST forms, recruited from a various care settings; nursing homes, 12,14,15,17 elderly care facilities, 16 community settings, 11,18 -20 and academic hospitals. 13 Majority of study samples were White (78.8%), female (54.3%), with mean age of 79.8 years.
Concordance for section A: Cardiopulmonary resuscitation (CPR)
Eight studies reported concordance between documented care wishes
Hammes and colleagues conducted a retrospective review of medical records of community dwelling adults who completed POLST forms prior to their deaths. 18 Authors found that of 300 individuals, 250 (98%) opted for Do-Not-Resuscitate (DNR) order under Section A, and none received CPR in the last 30 days of life. Five individuals (2%) requested resuscitations be performed, and their medical record indicated that all 5 were hospitalized at EoL, with admitting orders for full-code status. In Reinhardt and colleagues’ study, which was a review of 300 medical charts of long-stay nursing home (NH) residents, the researchers found that CPR wishes were honored at all times (100% of concordance). 14 Tolle and colleagues conducted a prospective study of 24 adults who opted for DNR option under POLST form Section A. The authors found that only 2 participants died in the hospital setting, and neither received CPR in the hospital or nursing home (2/2, 100% of concordance). 15
Hickman and colleagues also reported a highly concordant findings between POLST documentation and provision or withholding of CPR (300/306, 98% of concordance). 17 When the authors examined the cases where POLST documentation indicated DNR order, none of the 299 deceased residents with a DNR order received unwanted or erroneous resuscitation (100% of congruence). In a chart review of 54 residents from a single NH, Lee and colleagues investigated whether resuscitation performed were concordant with POLST documentation. 16 It was found that 49 residents (91%) received concordant care. One study, in which researchers randomly selected 300 community-dwelling adults who participated in advance care planning program, to identify whether CPR provided to POLST users were concordant with documented care wishes. It was found that wishes were honored in 257 individuals (97%). 11
Two studies showed concordance rates that were little over 80% of the time. Schmidt and colleagues conducted a study where authors examined accessibility of POLST registry for Emergency Medical Services (EMS) personnel working at the scene. 19 The authors noted an overall provision or withholding of CPR was concordant with patient’s POLST documentation 83.3% (5/6 cardiac arrests) of the time. It was noteworthy that one patient was dead at the scene and did not receive any medical interventions at the scene.
The lowest rate of concordance was found in Richardson and colleagues’ studies. 20 The authors also examined concordance of provision/ withholding of resuscitation delivered by EMS in out-of-hospital cardiac arrest cases. Of total 82 cases of cardiac arrests where EMS calls were made, only 66 (80.6%) received care that were aligned with POLST documentation.
Concordance for section B: Medical interventions
Seven studies examined if the care provided during EoL was concordant with written care wishes on POLST form, section B. Specifically, 3 studies compared the preferred level of care (e.g., comfort only vs. limited vs. full treatment) indicated on POLST forms and whether wishes were respected. 13,16,17 Four studies examined the POLST wishes for hospitalization, 12,14,15,18 and 3 studies examined the POLST wishes for the receipt of care in an ICU setting. 15,16,18
Overall, preferred level of medical interventions showed concordance of 68.5% (range: 46%-91.1%), and the wishes to avoid/ transfer to hospital or ICU settings were concordant wish documented wishes 94% of the time (median 95.5%, range 85-100%).
Level of Medical Intervention
The concordance rate reported for preferred level of medical intervention and the actual level of care delivered varied greatly, ranging between 46.0%-91.1%.
In a study where authors evaluated the concordance between treatment provided to patients who are dying and their written wishes for the level of medical care (i.e., full vs. limited vs. comfort-only levels of care), 17 authors noted an overall concordance of 91.1%. Specifically, of all patients who opted for full treatment level of medical care (n = 19) always had their wishes honored (100%). Similarly, those who opted for limited treatment level of medical intervention (n = 58) almost always (98.3%) had their wishes honored. However, when 35 POLST forms with comfort measures only level of medical care was reviewed, only 26 patients (74.3%) received concordant care. In the most recent study where authors evaluated association between POLST documentation for medical intervention, 13 it was found that one or more life-sustaining/ prolonging treatments were delivered to 86.0% of patients who had comfort measures-only and 80.0% of patients who opted for limited treatment as their preferred level of medical care (i.e., combined 82.0% concordance) .
In contrast, a retrospective chart review of 54 residents, conducted by Lee and colleagues, found that less than half of residents (46.0%) received EoL care at the level they requested; 33 percent (n = 18) received care at a less invasive level, while 20% (n = 11) received care at a more invasive level. 16
Hospitalization / ICU admission
Five studies examined concordance between documented wishes to be transferred and hospitalized for further management and whether such wishes were honored. 12 -15,18 When Tolle and colleagues examined 26 hospitalizations that occurred among 24 elderly residents, for whom POLST wish indicated transfer to hospital only for comfort enhancement, 22 hospitalizations were found to be for the management of pain and sufferings that were not controlled in their current care facilities (84.6% concordance). 15 The rest (15.4%) were for the life-sustaining purposes, contrary to residents’ POLST documentation. Authors also added that of all hospitalized residents, their wish to receive comfort-care were universally respected (i.e., none received aggressive treatments, or were admitted to ICU settings).
Hammes and colleagues examined the medical records and POLST documentation of community dwelling individuals to examine if preference for hospital admission and ICU utilization were honored. 18 Authors noted that of 157 decedents opted for comfort-measures only, and none received aggressive treatments (e.g., intubation or ICU admission). There were 15 hospitalization that were noted, and further chart review showed 13 cases were congruent with POLST documentation. That is, 13 decedents specified wishes to be transferred to hospital for comfort enhancement purposes only. And all 13 transfers were attributable to need for higher level of pain management. However, 2 cases were discordant as those individuals specified specific wish to avoid hospitalization.
Lum and colleagues examined medical charts of elderly patients living with heart failure, admitted to skilled nursing facilities. 12 Of 182 patients who had Medical Orders for Scope of Treatment (MOST) forms, 66 patients had hospital visits or were hospitalized. Although the authors stated that the majority received goal-concordant care during the hospitalization (95%), 12 no further information (e.g., specific medical intervention provided) was provided.
Reinhardt and colleagues examined 160 residents from a single care facility and had “do not hospitalize” order indicated on POLST forms. 14 Although medical chart review revealed 6 hospitalizations had occurred, all (100%) were deemed “appropriate” as all 6 hospitalizations were needed to enhance comfort (without using any aggressive measures while hospitalized).
The most discordant cases were found in a recent study, conducted by Lee and colleagues. 13 Authors examined a total of 1,818 patients who were hospitalized in 2 different hospitals and had ICU admissions near EoL. Of 401 patients who opted for “comfort measures only” level of intervention, 123 patients were admitted to ICU setting (69.3% concordance). For those who opted “limited treatment” level of intervention (n = 761), nearly half (n = 349) were admitted to ICUs, showing 54.1% concordance between POLST documentation and medical interventions delivered. Therefore, overall 60.9% concordance was achieved.
Concordance for section C: Artificially administered nutrition / hydration
Overall, documented care wishes to receive artificially administered nutrition (e.g., feeding tube) and/or intravenous hydration were generally concordant with the actual care delivered (mean 88.3%, median: 94.0%, range: 63.6%-100%).
A review of 221 POLST documentation showed only 2 cases (1%) were discordant. Little over half (58%) of patients indicated wishes to avoid feeding tube, and those wishes were universally respected (100% concordant). Four patients requested feeding tube to be used to sustain life; 2 received feeding tube at EoL, and 2 did not meet treatment indication (100% concordant when feeding tube was opted). 18 When Hickman and colleagues reviewed 22 medical charts of older adults who opted to receive feeding tube, only 14 received feeding tubes (63.6% of concordance), 17 and the rationale for those who did not receive feeding tube was not provided.
Reinhardt and colleagues reviewed 47 POLST forms that indicated patient wishes of “no artificial hydration” at EoL. Medical chart review revealed that despite “no artificial hydration” order in place, 12 patients (25.5%) received intravenously administered hydration. 14 However, authors explained that 3 residents received hydration with family agreement/ consents, and rest received hydration prior to the preparation of the POLST documentation. Therefore, the concordance was reported as 100%. In the Lee and colleagues’ study, 16 authors examined and reported concordance for both artificial nutrition and hydration. Of 37 participants who stopped eating sufficient calories to sustain life at EoL and had requested tube feeding, 34/37 patients received care that matched the POLST instructions (91.9% or concordance). Thirty-eight patients who were not drinking adequate fluids at EoL and specified preference to receive IV hydration on POLST forms, 32/38 participants received concordant care (84.2% of concordance). 16
Other section: Concordance for antibiotic treatment
Four studies reported whether the use of antibiotics treatment at EoL among POLST users were concordant with POLST documentation. 14,16 -18 In general, use of antibiotic treatments were highly concordant with POLST documentation (mean: 94.7%, median: 96.5%, range: 86.0%-100%).
Reinhardt and colleagues noted that there were 17 residents who had “no antibiotics” order indicated on POLST forms. 14 Chart review showed that 8 residents received antibiotics as treatment at EoL. However, further investigation of charts revealed that antibiotic treatment preceded the POLST order, in all cases (100% concordant). Similarly, Hammes and colleagues reviewed a total POLST forms to identify decedents’ antibiotics preference. 18 Authors found that the majority (n = 115, 45%) opted for antibiotics for comfort measures only, followed by antibiotics for aggressive treatments (n = 80, 31%). The chart review revealed that 20 decedents with orders for antibiotics for comfort measures only received antibiotics treatment despite the order. However, further investigation showed that in all 20 cases, the surrogate decision maker authorized antibiotics use which overrode patients’ wishes documented on POLST forms. In the same study, it was also noted that 10 decedents indicated “no IV or IM antibiotics” and in all 10 cases, the antibiotics used were administered via oral routes only. Therefore, all patients always had their wishes honored (100%). In the Hickman and colleagues’ study, antibiotic preference documented and care delivered were concordant 92.9% (224/241): 7 patients indicated wishes to avoid antibiotics but wishes were not respected at all (0% concordance); 60 patients opted for limited antibiotics and it was respected in 50 cases (83.3% concordance); all wishes for 174 patients who opted for full treatment antibiotics were fully respected. According to Lee and colleagues’ study, 16 antibiotics usage complied with the POLST documentation for 86% of the study participants, for whom antibiotics were indicated.
Discussion
To the best of our knowledge, this is the first systematic review that synthesized scientific evidence for the concordance between the documented care wishes on POLST forms, and subsequent care delivered to POLST users during EoL in both clinical and non-clinical settings.
Most of the studies included in this review were retrospectively conducted cohort studies, in medical facilities (e.g., nursing homes). Section A: CPR, preferences for receipt of resuscitation in the event of cardiac arrest, and the actual delivery of or withheld of resuscitation efforts was the most studied intervention of all. It is also where the highest congruence rates were reported.
There were several discordant cases noted in the delivery of EoL care interventions, namely, hospital transfers, antibiotics use, and feeding tube use. Most common reason for unwanted hospital transfers, or the use of antibiotics among dying patients were new onset of infections. 12,18 Previous studies on the health status of NH residents revealed that infections are, in fact, the most commonly encountered health problems among elderly population. 22 -24 Also, it is one of the most common factors that causes unplanned changes in one’s EoL care processes. 25 Combined with the fact that not all NHs are adequately equipped to provide screening of, or management of infections that are prevalent in EoL, it appears to be a challenging task to bring immediate changes, or measurable outcomes in this aspect of EoL care. 26 However, continued efforts in infection surveillance, antibiotic stewardship and in-depth understanding of resident’s EoL care goals are one of few strategies that can be implemented to minimize over-utilization of potentially harmful treatments.
Overall congruence between preferred use of feeding tube and actual care delivered revealed another area that needs improvement. Researchers pointed that discordant cases in feeding tube use were most commonly seen among those who opted to have feeding tubes only for a defined trial period. 17 Some patients had feeding tube in place for longer than 30 days, raising concern for what constitutes as a trial period, and some even died with feeding tube in place. Researchers called for the need for clarification of the term defined trial period as it has never been defined by the National POLST Program Task Force (NPPTF) organization. Although it is difficult to conclude that discordant cases in feeding tube use were solely due to lack of consensus on definition, such finding raised an important issue that languages used in medical forms, especially in advance care planning document, should avoid any terms that can be misinterpreted or misunderstood. 27
One of notable study findings was the evidence of high congruence for a preferred route of medication administration. Among those who expressed EoL care preferences to receive antibiotics, but only via oral routes, all (100%) study participants received care that was congruent with their written wishes. 18 This signifies a high specificity that can be achieved through use of POLST forms as an Advance Care Planning (ACP) tools. This finding resonates with previous research work, which noted an effectiveness of POLST forms in guiding EoL care. 28 Meier and Beresford explained that POLST provides a quick and clear guidance in the EoL care, through highly specific care preference documentation for common interventions used in EoL journey. 28 When examining concordance between POLST documentation and subsequent care delivered to seriously ill patients, it is important to understand that some discordant cases may arise from issues that are related to the POLST form itself (structural issues) or difference in familiarity of the POLST program among general population. While POLST is gaining increase attention across the nation, NPPTF allows each U.S. state to develop a state-specific POLST program and operate it independently. 27,29 This, in turn, leaves room for inherent differences to arise in the type of EoL care addressed and the options one can choose from. For example, the Wisconsin POLST form offers 4 different options under tube feeding preferences (i.e., no feeding tube, defining period usage, long-term use or determine the use when needed) while West Virginia only offers 2 (i.e., no feeding tube, or long-term feeding tube use).
The type of EoL care options captured on state forms also differ significantly. For example, antibiotics options are no longer being assessed through the POLST form in Oregon. In 2012, Oregon’s POLST coalition made an executive decision to remove antibiotics preference section from its POLST form, nearly 20 years after POLST program was developed. 30 Such a decision was due to a new research findings. That is, Hickman and colleagues found that the antibiotics section on POLST forms had little impact on the actual usage of antibiotics between 2 groups (patients who opted for antibiotics at EoL and patients who opted for no antibiotics at EoL). In this retrospective cohort study, the actual use of antibiotics at EoL were similar between 2 groups, regardless of written wishes indicated on the antibiotics section; 32.1% and 30.4% respectively. 17 In addition, lack of research evidence that antibiotics use at EoL enhances survival outcomes or comfort for those who are near death supported Oregon’s decision to remove the antibiotics use section in its entirety.
Each state participating in the POLST program has different levels of program designation, classified as maturity status. From lowest to highest status, a state POLST program can move from developing, endorsed, and mature status when it meets certain milestones or key criteria that NPPTF requires. 31,32 When the program first begins a state-wide dissemination of POLST, it obtains a developing status and then moves toward endorsed when the state consensus is met for a single state-wide POLST form, and then to mature status when POLST becomes a part of standard of care for elderly and frail patients and is used as an advance care planning tool in more than half of all medical facilities (e.g., nursing homes, hospitals, hospice care settings) within its state. 32 Depending on the maturity status of the POLST program, public awareness on the POLST program itself, and how it can be utilized to tailor one’s EoL care may vary significantly. For example, in an area where the POLST program is used in the majority of healthcare settings, medical providers may be more familiar with the fact that POLST forms should be re-visited when patient status improves or declines further, and patients be given many opportunities to reflect any changes in care preferences during the EoL care journey. Unfortunately, different levels of public or provider awareness and competency on how POLST can be utilized to tailor one’s EoL care remains unstudied, which could explain discordant cases observed in included studies.
Making the EoL care decision is a challenging process. It can also be emotionally draining for those who are faced with or involved in the decision processes. Informed ACP requires a utilization of a guiding tool that facilitates care discussions, while presenting treatment options that are relevant to EoL care. It should also be systematically monitored for continued quality improvement and be closely examined for the outcomes it brings to its target population. This systematic review synthesized published evidence on the congruence between POLST documentation and subsequent care delivered at EoL, and provides comprehensive resource for healthcare providers, health science researchers or policy makers who are seeking scientific evidence on POLST use and the impact it brings. It is clear that gathering additional scientific evidence on the use of POLST across different care settings or regions will help advance future EoL care practices.
Limitations
There are number of limitations that are worth mentioning. First, although we developed search strategy with the help of library informationist, it is possible that our search strategy may have not identified all relevant research articles on this topic. Second, while we limited our inclusion criteria to research articles published in peer reviewed journals, potentially important and relevant findings that addressed our research question could have been existed in grey literature, and/or unpublished articles. That is, publication bias may be present with studies not finding concordance not being published. Third, we found that several authors on the included research articles had affiliations with NPPTF; some served as consultants or board members. In addition, one of the authors in the included studies appeared as co-author on 2 other included studies.
Another significant limitation of this systematic review is that 5 of the included studies were conducted in Oregon, and 2 other multi-state studies included Oregon as one of their geographic study locations. Although this could be considered as a limitation, POLST was first developed, introduced, and disseminated in Oregon. Needless to say, as a birthplace of POLST program itself, the most number of resources and data are available from Oregon.
Conclusion
Based on our findings, POLST is an effective ACP tool that can be used to discuss, document, and to deliver EoL care that reflects patient’s care preferences. Provision of resuscitation at the time of cardiac arrest or time of death was universally respected, while there were mixed results in the use of feeding tube, and use of IV fluids use at EoL.
Additional research is recommended to identify congruence between documented care wishes and actual care delivered among patients who experienced multiple care transitions or have moved cross state near the time of death. Further studies should also compare congruence between POLST documentation and care delivered between groups of patients who may suffer from different medical conditions. Empirical studies are needed to ascertain the comprehensiveness of POLST items in capturing relevant and important EoL care interventions. There is a need to conduct prospective observational studies within various patient care settings, across all the life span.
Footnotes
Authors’ Note
A Tark: Analysis and interpretation of data, significant contribution to draft and revision of manuscript. J Song: Acquisition of articles, analysis, interpretation of data and contribution for manuscript revision. J Parajuli: Identify and acquisition of articles, contribution for manuscript revision.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Center for Improving Palliative Care for Vulnerable Adults with MCC (CIPC) National Institute of Nursing Research Grant (NINR) GRANT (P20NR018072-01); the Comparative and Cost-Effectiveness Research Training for Nurse Scientists (CER2) (NINR grant T32NR014205); Pain and Associated Symptoms Research Fellowship (NINR T32 (NR011147)