
Abstract
Background
Life-sustaining treatment (LST) orders are important communication tools used to ensure preference-concordant care at the end of life. Recent studies reveal concerning rates of discordance between current preferences and documented LST orders, especially in nursing facilities without POLST. Reasons for discordance in facilities using POLST have been explored, however the majority of nursing facilities in the United States do not yet use the POLST form.
Design
Qualitative descriptive study using constant comparative analysis.
Setting
Nursing facilities in Indiana (n = 6) not using POLST.
Participants
Residents (n = 15) and surrogate decision-makers of residents without decisional capacity (n = 15) with discordance between current preferences and documented LST orders.
Measurements
Do not resuscitate, do not hospitalize (DNH), and do not intubate (DNI) orders were extracted from medical charts. Current preferences were elicited using the Respecting Choices Advanced Steps model. A semi-structured interview guide was used to explore reasons for discordance between current preferences and LST orders.
Results
Reasons for discordance included: (1) inadequate information about the range of available LST options, what each involves, and how to formally communicate preferences; (2) no previous discussion with facility staff; (3) no documentation of previously expressed preferences; and (4) family involvement.
Conclusion
Reasons for discordance between expressed preferences and LST orders suggest that in facilities without a uniform and systematic LST order documentation strategy like POLST, these conversations may not occur and/or be documented. Staff should be aware that residents and surrogates may have preferences about LSTs that require strategic solicitation and documentation.
Keywords
Introduction
Adequate advance care planning (ACP) and decision making at the end of life has been identified as an unmet palliative care need for patients in long term care. 1 Medical orders addressing life-sustaining treatments (LST) such as hospitalization, intubation, and cardiopulmonary resuscitation (CPR) are used in nursing facilities to help ensure person-centered care at the end of life. These LST orders differ from other ACP documentation strategies, such as living wills, in that they are immediately actionable and focus on end-of-life procedures. LST orders serve as important communication tools when a resident or surrogate is unable to state their preferences and the situation is urgent.
However, residents’ current preferences and LST orders do not always align. Previous work found rates of discordance between current preferences and LST documentation ranging between 32% 2 and 93% 3 in the nursing facility setting and 60% in the hospital setting. 4 Understanding why current preferences do not match LST orders is a critical step in ensuring the delivery of preference-concordant care.
A key consideration is the variety of LST order documentation methods. In the United States, many facilities have adopted the POLST program—a uniform order set for documenting treatment preferences as orders. While an increasing number of states are working toward statewide use of POLST, the majority do not yet have this in place. 5
In prior work, we identified higher rates of discordance between stated preferences and documentation in non-POLST-using nursing facilities (65.1%) compared with POLST-using facilities (40.7%). 6 To understand the reasons for this finding, we conducted a qualitative study with residents and surrogates in POLST-using facilities. 7
In this current study, we analyze reasons for discordance between preferences and documentation in non-POLST-using nursing facilities. This analysis may offer a more comprehensive picture of reasons for discordance between current preferences and LST orders and enhance our understanding of how different LST order documentation strategies affect preference discordance.
Methods
Setting
This study was conducted in six non-POLST-using Indiana nursing facilities identified from a state telephone survey. 8 Data collection occurred between May 2017 and January 2019. The protocol was reviewed and approved by the Indiana University Institutional Review Board.
Participants
Study participants were nursing facility residents with decisional capacity and surrogates of residents lacking decisional capacity. Eligibility criteria included: (1) a resuscitation code status order on file addressing preferences for CPR, (2) resident length of stay ≥60 days, (3) resident aged 65 or older, (4) fluency in English, (5) a score ≥21 on the Telephone Interview for Cognitive Status (TICSTM), 9 and (6) discordance between current stated preferences in resident interviews and documented orders. Residents with POLST forms were ineligible. Residents were further screened using a consent verification process to assess capacity to consent. 10
Procedures
Interviews were obtained as part of a larger mixed methods study. 6 Participants in the mixed methods study were identified through chart reviews in which current orders for resuscitation, hospitalization, and intubation were extracted. The facility contact identified which residents were making their own healthcare decisions, confirmed the identity of the surrogate decision-maker where applicable, and eliminated potential participants who would be overly burdened by a researcher’s approach due to psychosocial or health concerns. Participants were interviewed about their current treatment preferences by research staff certified in the Respecting Choices Advanced Steps (RCAS) facilitation model, 11 and elicited preferences were compared with orders on file. Reasons for discordance were explored using open-ended questions in a semi-structured interview format. Participants included in this qualitative work are from a subset of completed interviews selected sequentially until thematic saturation was achieved.
Data Collection Tools
Participant characteristics
Participants provided information about age, race, gender, education level, and the surrogate’s relationship to the resident. A previously validated self-report tool was used to evaluate health literacy, rated on a 5-point Likert scale where a higher total score indicates lower health literacy. 12 Cognition was measured using the TICSTM, where scores <20 indicate moderate to severe impairment, 21-25 indicates mild impairment, 26-32 indicates ambiguous cognitive status, and 33-41 indicates no impairment. 24
Current treatment preferences
Current treatment preferences for CPR, hospitalization, and intubation were elicited using the RCAS interview, 11 and all research assistants (RAs) received certification in RCAS facilitation as well as supplementary training that included observed role-playing using standardized patients. This interview is a copyrighted, systematic program designed to support LST conversations with people with advanced illness or frailty 13 and involves integrating reflections upon experiences and values with educational information about treatment options. RAs guided participants in identifying values, exploring understanding of medical conditions and complications, reflecting on past experiences, and relating hopes and fears. RAs provided standardized education about the benefits and burdens of CPR, assistance with breathing, and hospitalization. After questions and reflections were explored, participants were asked to confirm treatment preferences based on these reflections and outcomes that were acceptable to them.
Existing LST orders
Medical orders for CPR, hospitalization, and intubation were obtained from nursing facility medical charts.
Reasons for discordance
A semi-structured interview guide was developed to explore reasons for discordance with participants. See Supplementary Data S1 for interview guide.
Qualitative Analysis
Interviews from the larger mixed methods study 6 were sequentially selected for transcription with a goal of equal inclusion of resident and surrogate participants. NVIVO (QSR International Pty Ltd Version 12.6) was used to manage the data. Qualitative descriptive methods were employed, beginning with open coding of interview transcriptions to inductively identify and label ideas. From these labels, 2-3 team members independently coded each transcript. Team members then discussed emerging themes and resolved discrepancies. Authors used constant comparative analysis across cases, and ceased sampling when we agreed thematic saturation had been accomplished. 14 A coding dictionary and memos were used to track coding decisions. Once all interviews were coded, 2 team members collaborated to create thematic summaries of each code. These summaries were then compared by the team and further distilled into themes.
Results
Participant Characteristics
Characteristics of Participating Decision-Makers (n = 30).
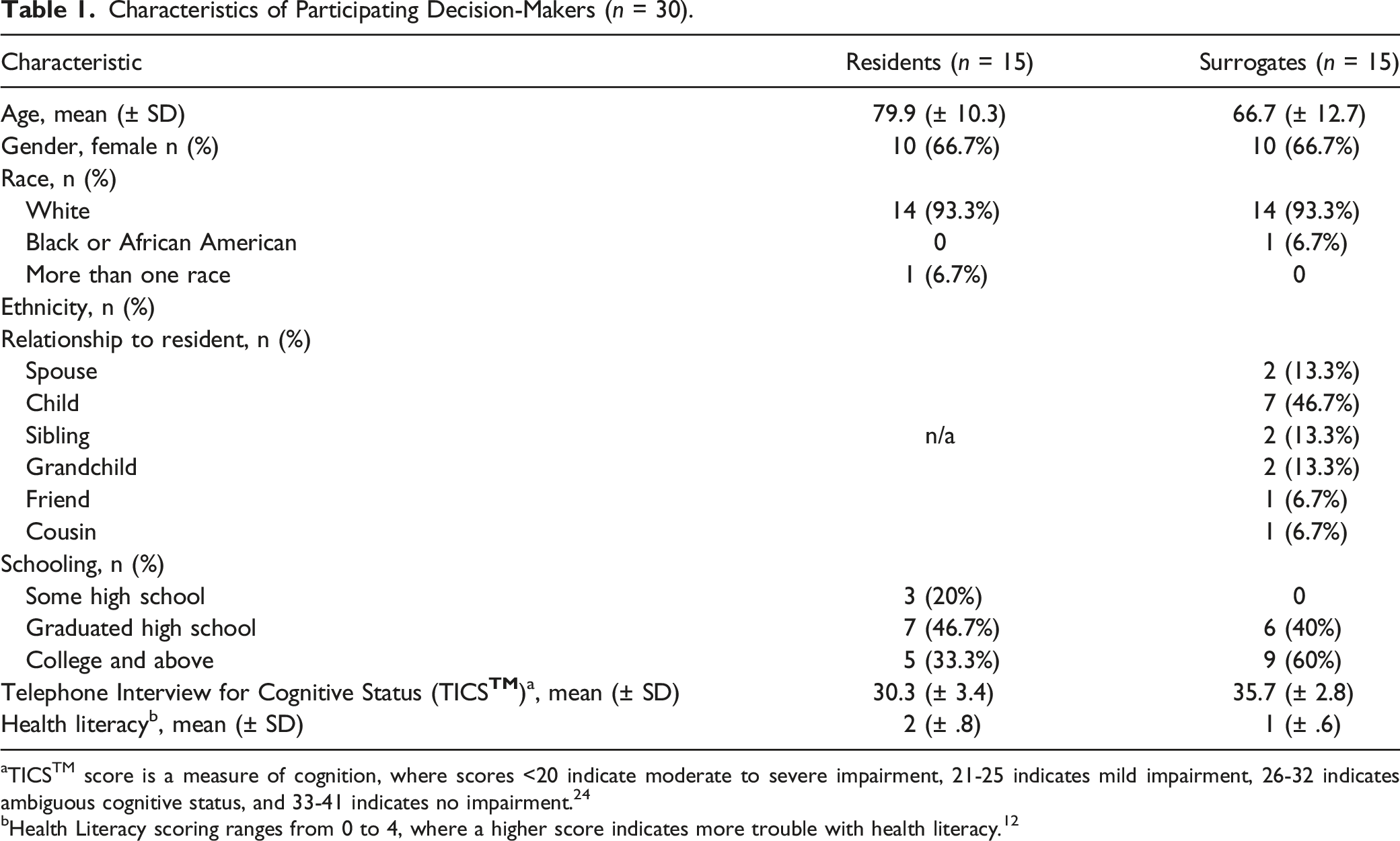
aTICSTM score is a measure of cognition, where scores <20 indicate moderate to severe impairment, 21-25 indicates mild impairment, 26-32 indicates ambiguous cognitive status, and 33-41 indicates no impairment. 24
bHealth Literacy scoring ranges from 0 to 4, where a higher score indicates more trouble with health literacy. 12
Discordance Characteristics
As compared to their existing LST orders, 6 (40%) residents and 1 (6.7%) surrogate in this sample reported different code status preferences, 10 (66.7%) residents and 15 (100%) surrogates reported different hospitalization preferences, and 10 (66.7%) residents and 15 (100%) surrogates reported different intubation preferences. No participants had hospitalization or intubation orders on file (see Figure 1 for types of documentation), so discordance in these categories resulted from an expressed preference to limit these treatments without corresponding LST orders as the default is to provide these treatments in the absence of documentation. It is notable that 13 (86.7%) residents and 14 (93.3%) surrogates wanted their orders updated after the interview, while the remainder preferred not to change their orders despite expressed preference discordance. LST orders discovered during chart review.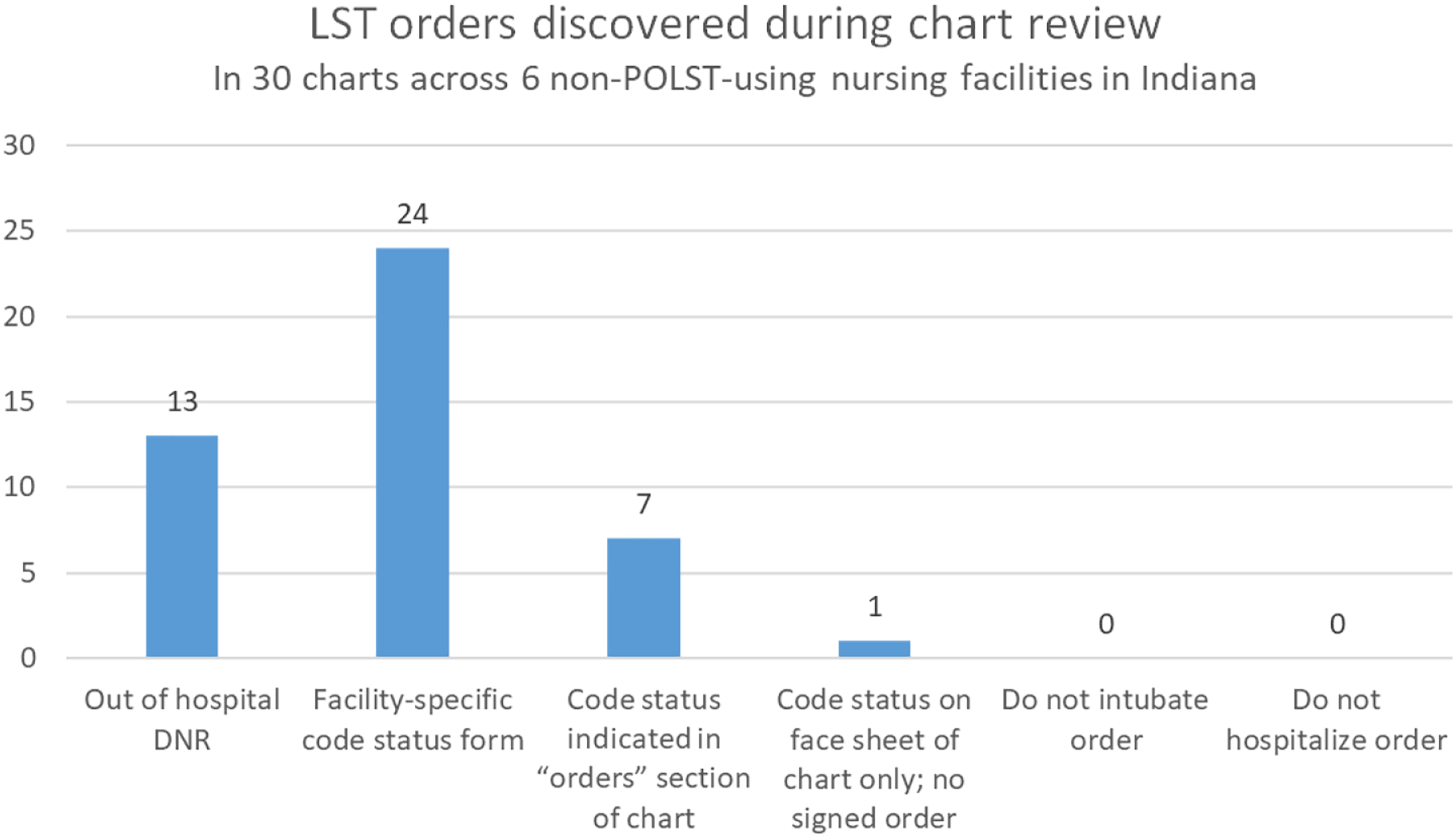
Discordance Themes
During the first stages of analysis we identified 22 codes, or recurring ideas, in the interviews. Over the course of analysis, 4 major themes emerged from these codes. Discordance was attributed to having had inadequate information, no previous discussion with facility staff, missing documentation of previously expressed preferences, and family involvement. In addition, there were several participants who indicated they did not know why there was discordance and did not appear to have insights to share.
Inadequate information
Participants described several types of information they had not understood prior to the RCAS interview. This included specific, prognostic information about medical interventions such as CPR and intubation and the range of available options, including limiting hospitalization and respiratory interventions. “Well, after seeing that three percent, that was something to make me think about….I was pretty much under the impression that it would help a lot if I had CPR.” (Resident) “We just talked about…the limited intervention which I had never [known] was an actual option. I think that’s the best choice for her at this point in time.” (Surrogate) “I didn’t know I had so many (options).” (Resident)
Others expressed a lack of familiarity with how to formally communicate these preferences – specifically the realization that preferences for intubation and hospitalization are not fully addressed by living wills and code status orders. “I thought your living will and stuff took care of all that but it doesn’t. So, that’s why that’s supposed to be on file.” (Resident) “Because I thought DNR [Do Not Resuscitate] meant that. So, that’s why, I guess. I didn’t know you had to clarify this and that - I thought DNR covered the bases.” (Resident)
Preferences not solicited
A prominent reason for discordance was the absence of a conversation with facility staff about treatment preferences. A few participants stated they had previously considered these topics, however most expressed a lack of awareness of their options, indicating they had never thought about it because no one had asked. “Because it [preferences for hospitalization and intubation] hasn’t been discussed with me. It hasn’t been discussed, until now. I have thought about it, what should I do, but I haven’t talked with anybody about it before. No one has ever asked me about it.” (Surrogate) “I haven’t really thought that much about it until now. I just haven’t. No one has ever asked me…” (Surrogate)
Some felt staff were at fault for not facilitating this discussion. Others expressed a sense of shared responsibility for not having initiated the conversation. “It wasn’t ever brought to our attention, but yet, we also didn’t ask or bring it to their attention. I think the fault lies in a lot of different places, why it doesn’t reflect what it would be currently, or what I think it should be currently.” (Surrogate)
Preferences not documented
Other participants reported a clear, existing preference and were surprised these preferences were not documented as medical orders. “Her path, her health has been pretty up, down, all around, but we have had a care plan meeting with them, in February I believe it was, and I’m kind of surprised that we didn’t somehow, that they either didn’t ask us about that? You know what I just said. We wouldn’t have said something different, so I’m not real sure why that’s not clear on her chart, if that was something that they didn’t cover, or why we don’t have that, it’s not on there.” (Surrogate) “I thought that I understood them very well. That’s why I am really kind of surprised that there is not, that her chart doesn’t reflect the same opinions that we talked about today.” (Surrogate) “I thought for sure I had it (preference on record).” (Resident)
The perceived reasons for this discrepancy varied and included that staff had been careless/uninvested or that staff had neglected to record a firmly stated preference. “I don’t think the goals have changed. I think the girls just get careless. The thing that bothers me, the short term people, I really didn’t make a kind of statement on that. I don’t think they are as dedicated, that they do everything every day like a person that knows them well.” (Surrogate) “I talked to them at the facility and I had no problem making the decision. None. My answer was firm and clear… I don’t know why it [the decision] wasn’t there [in the chart] because I thought that should have been there because we never know the time of death and it should be available to them at all times because we don’t know the minute or the hour. They know that and I will make sure it’s there.” (Surrogate)
Family involvement
Some residents expressed not wanting to upset family members with a preference for less intensive interventions. “My daughter wants it [for me to try CPR]. Of course you know she wants to keep me alive forever and it ain’t going to work…Sometimes it’s easier to go along with the flow than it is to try to fight with them…I didn’t want to upset her by telling her I didn’t want to try it [CPR]. I knew it would really upset her, you know.” (Resident)
Others trusted family members to make the right decisions as problems arose instead of in advance. One resident with decisional capacity attributed discordance to a family member making the decision without the resident’s involvement. Interestingly, the same resident stated that their family member knew what they wanted and would make the right decisions on their behalf. This internal inconsistency highlights the complexity of family dynamics and communication surrounding end-of-life treatment decisions. “I’ve got one sister who’s got power to make the decisions, and she knows what I want…she knows how I feel and everything, so she’d make the right one…I don’t know who put that [CPR order] in there [medical chart], because I didn’t. My sister must have. They must have talked to my sister about that… The only thing is maybe they didn’t ask completely me about it, they did my sister, and I haven’t told my sister about that yet, but it, I know I didn’t approve it, because I don’t want to [have CPR].” (Resident)
Discussion
Discordance between preferences and documentation in the medical record is concerning as it places nursing facility residents at risk of receiving care that is inconsistent with their preferences. In interviews with residents and surrogates with discordant documentation, we were able to understand reasons for discordance from their perspective. One common theme that emerged was a lack of adequate information to make and document an informed choice about LSTs. Several reported that no one had ever asked about LST preferences. These findings are striking because when invited to discuss LST preferences and provided with information, all participating surrogates and over half of the residents in this sample expressed preferences about intubation and hospitalization. When they learned that these preferences were not reflected in the medical record, a majority requested their records be updated. This finding is consistent with other work describing the willingness of nursing facility residents and families to participate in LST conversations and document preferences following these conversations. 15
Another theme that emerged is that some participants believed they had expressed their preferences to staff and were alarmed to discover these decisions were not documented in the medical record in a way that could be easily found. The need for more information and communication surrounding LST decisions is an important and modifiable area of concern and suggests the need for improved documentation practices as well as clear policies and procedures to support ACP. Formal intervention studies have utilized document-based toolkits, 16 specialty training and dedicated time for ACP conversations for staff,15,17 and delivery of information through video3,18 with some success. All these trials noted barriers of time, resources, and culture shift required for quality ACP in this setting.
A less common explanation for discordance was the involvement of family. Specifically, a few residents expressed a desire to protect family members’ feelings while others trusted family could make the right in-the-moment decisions on their behalf – or conversely suspected family had made decisions without their approval. These issues have the potential to be ameliorated by the same approach that will address the more commonly reported themes: policies and procedures that support systematic discussions about LST preferences between residents, family members, and staff. There is evidence that elderly residents at risk of dying have often not discussed their wishes with family members despite a belief that family members would make appropriate decisions on their behalf if the need arose. 19 Further, surrogate decision-makers report wishing they had known more about their loved one’s preferences. 20
This analysis of the reasons for discordance in nursing facilities that do not use POLST serves as a point of comparison with our prior analysis in POLST-using facilities. 7 In both studies, participants attributed discordance to inadequate information about LST interventions such as CPR as well as family dynamics. Both groups also had participants who were unable to explain the discordance. However, one key difference between the two samples is that participants with POLST frequently reported that the discordance was due to a change in preferences over time, whereas this was not identified as a reason for discordance in the non-POLST using sample. Participants without POLST described more issues of LST option unawareness and lack of LST conversations, whereas participants with POLST more commonly described process issues with how preferences were elicited and documented.
Limitations
This study took place in a state with a predominantly White population and our resulting sample reflects this lack of diversity. Additionally, we conducted interviews with only decision-makers (e.g., resident or surrogate). Including additional family members or trusted friends in the interview may have provided us with different insights into the reasons for discordance. Recall bias may also be significant in participants’ reported reasons for discordance. Finally, the minimal use of other LST orders (DNH, DNI) across our sample facilities, despite evidence of greater prevalence on a national stage,21-23 is a limitation. It is possible that we would find different reasons for discordance in facilities more routinely using these other kinds of LST orders.
Conclusion
Our data suggests that in facilities where POLST is not used, conversations about treatment options (such as hospitalization and intubation) may not regularly occur or be documented when they do occur. Nursing facility staff should be aware that preferences surrounding life-prolonging treatments, such as hospitalization and intubation, may exist and are in need of informed solicitation with consideration of family dynamics. There are existing ACP facilitation and LST documentation interventions that could address some of the issues identified here, and further research into the effects of these interventions on preference concordance is recommended.
Supplemental Material
Supplemental Material - Reasons for Discordance Between Life-Sustaining Treatment Preferences and Medical Orders in Nursing Facilities Without POLST
Supplemental Material for Reasons for Discordance Between Life-Sustaining Treatment Preferences and Medical Orders in Nursing Facilities Without POLST by Nicholette L. Heim Smith, Rebecca L. Sudore, Anne L. Myers, Bernard J. Hammes, and Susan E. Hickman in American Journal of Hospice and Palliative Medicine®
Footnotes
Acknowledgements
The authors would like to thank participating nursing facility residents and surrogate decision-makers for their time and thoughtful engagement in the interviews. The collaboration with Indiana nursing facilities was essential to this study’s success, and we thank administrators and staff who graciously welcomed the research team to their facilities. We are grateful to research assistants Curtis Williamson, LCSW; Marcie Sherman; Miranda Connors; and authors Nicholette Heim Smith, BSN and Anne Myers, MPH for conducting interviews with great care and professionalism. We are also grateful to Alexia M. Torke, MD, and Greg Sachs, MD, for their contributions in study design and analysis.
Author Contributions
Study concept and design: SH, RS, and BH. Acquisition of subjects and/or data: SH, AM, and NHS. Analysis and interpretation of data: SH, AM, NHS, RS, and BH. Preparation of manuscript: NHS, SH, RS, AM, and BH.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the RRF Foundation for Aging and Indiana University School of Nursing. RS was funded in part by the National Institute on Aging, National Institutes of Health (K24AG054415).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.