
Abstract
Background
Carers of Persons with Parkinson’s disease (PwP) have significant palliative care needs that are not adequately addressed in current models of care. To provide holistic and targeted support to carers it is important to understand their perceptions of the multiple dimensions of caregiving (defined as domains) and associated core components within each domain (defined as key concepts).
Purpose
To (a) elicit carers’ perceptions and experiences of caregiving domains and associated key concepts within each domain, and (b) develop a framework of Parkinsons Disease (PD) caregiving incorporating the domains and their associated key concepts.
Methods
We conducted a qualitative descriptive study using perspective mapping, a novel hybrid mind-mapping method to develop a framework on the domains of PD caregiving. Semi-structured virtual interviews were conducted with former carers of PwP to elicit their experiences and perceptions of caregiving. Interviews were audio-recorded, de-identified, and transcribed. A codebook was developed and data were coded and analyzed to develop the framework of PD caregiving domains.
Results
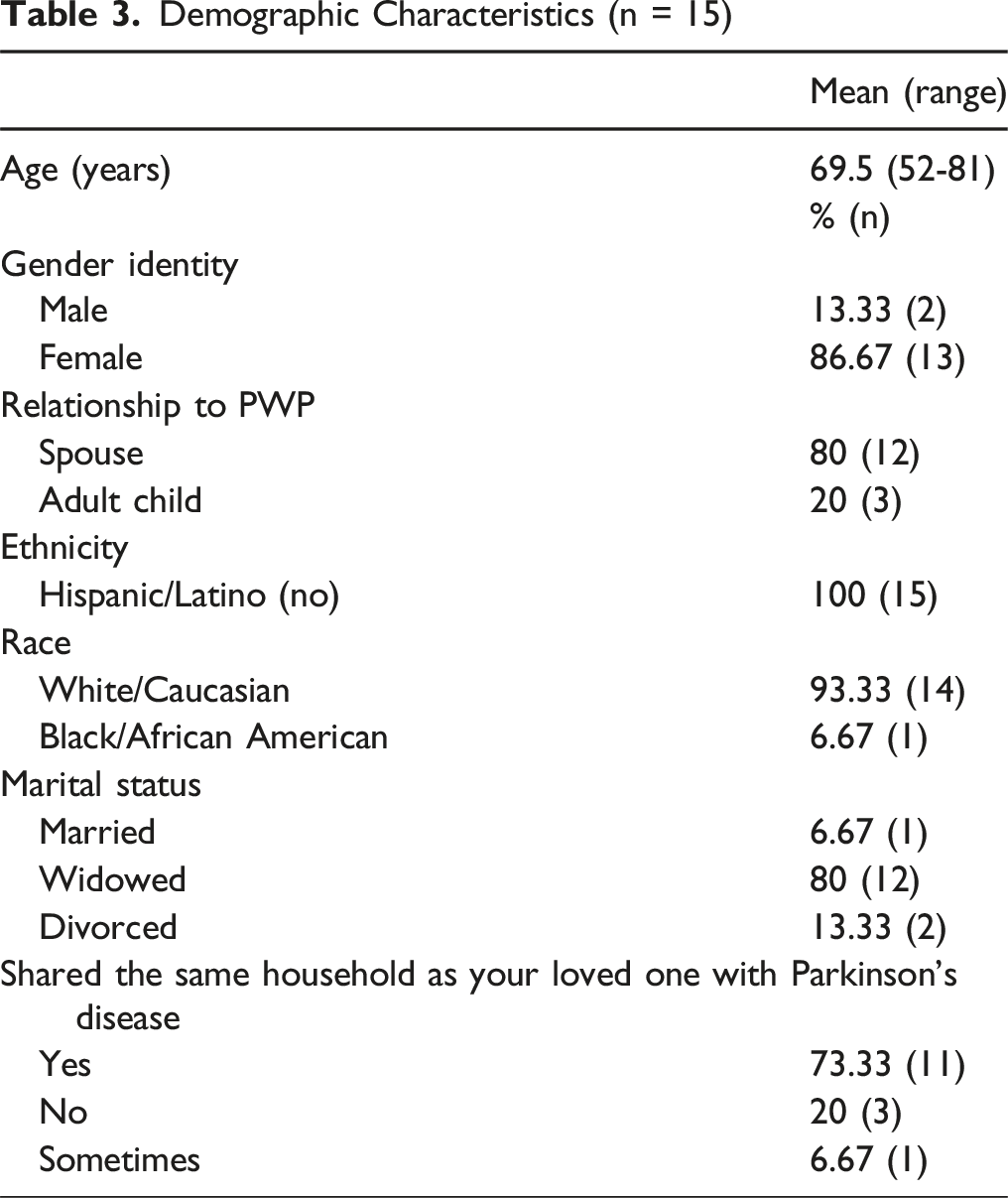
Fifteen carers participated in the study. A framework of PD caregiving was developed that comprised nine domains and 52 key concepts. The domains included decision-making, caregiving preparedness, care coordination, disease management, preserving self, emotional, spiritual, social/cultural, and physical.
Conclusions
A carer-elicited framework of PD caregiving is important to provide holistic support to PD carers. Both carers and clinicians may benefit from this framework that may help with identifying caregiving domains that require targeted support. Future research is needed to further refine the framework and build carer-centered intervention development.
Keywords
Introduction
Persons with Parkinson’s disease (PwP) experience multiple motor and non-motor symptoms including gait imbalances, tremor, pain, dementia, fluctuating cognition, neuropsychiatric behaviors, and sleep disruptions. These symptoms can result in emotional, physical, existential suffering, and high caregiving distress. From the time of receiving the diagnosis and throughout the illness trajectory PwP and their carers have a range of palliative care needs including managing symptoms, emotional, spiritual, and psychosocial needs, and financial hardships.1,2 Informal unpaid family carers who are often older adult spouses are at high risk for chronic illness,3,4 anxiety, and depression.5,6 Beyond knowledge of disease symptoms and medications, carers of PwP desire emotional, 7 social, and spiritual support and the lack of attention to their needs leads to demoralization, suffering, and reduced quality of life.
While palliative care specialists are integral to the care of those with intense and complex needs, all clinicians can use a palliative approach to address the needs of PwP and carers from the time of diagnosis and throughout the trajectory of the illness.8,9 The operational definition of palliative care for PD includes not just the management of non-motor symptoms and support for PwP’s emotional and spiritual needs, but also the recognition of and support for carers’ needs. 10 There is evidence that integrated outpatient palliative care improves PwP and carer outcomes. 11
Despite these efforts, in clinical settings caregiving has often been conceptualized as inherently stressful and burdensome and operationalized as an adverse effect of caregiving on social, emotional, financial, and physical functioning.12,13 Carer burden, often assessed using standardized instruments such as the Zarit Burden Inventory 14 is important to clinicians who are charged with the responsibility of managing PD symptoms and caring for the PwP. However, carers do not view caring for their family member as burdensome 15 and positive and negative experiences often co-occur during stressful times. 16
Although the importance of carers in supporting patients is undisputed 17 there aren’t any PD related standards or caregiving frameworks for clinicians to utilize to support carers. Yet it is known that carers desire practical guidance, strategies for managing disease symptoms, where and how to access resources, emotional and spiritual support, and to understand the road ahead including bereavement support when the time comes. 17 Within palliative care, there are models to guide care for patients and families, 18 and a conceptual model with key variables to guide interventions for family carers of those receiving palliative care that goes beyond stress and burden and encompass preparedness, social support, and the positive dimensions of the caregiving. 19 However, despite a growing body of literature on PD carer experiences and perceptions,15,20,21 there is a lack of framework of caregiving in PD and a lack of knowledge of carers’ perceptions of the domains of caregiving.
A participant-informed framework of PD caregiving will enable carers and clinicians to identify core caregiving needs that can guide conversations around carers’ changing needs and priorities over time. Thus, the aims of this study were to (a) elicit carers’ perceptions and experiences of caregiving domains and associated key concepts within each domain, and (b) develop a framework of Parkinson’s Disease (PD) caregiving incorporating the domains and their associated key concepts. Of note, in this study the term “domain” refers to a dimension of caregiving and the term “key concept” refers to a core component of the domain.
Methods
Study Design
We conducted a qualitative descriptive online interview study using perspective mapping. 22 Perspective mapping (PM) is an interview technique in which study participants and researchers co-create a branching visual diagram of the participant’s experiences related to a phenomenon of interest using mind mapping software. The approach has been used in prior studies to identify meaningful disease-related symptoms.23-25 PM is suitable for the development of frameworks grounded in the lived experiences of the population of interest. Consistent with the method of PM, in this study we refer to the dimensions of caregiving as domains and the core components of the domains as key concepts. 22
Participant Selection
We used purposeful sampling to recruit study participants as it allows for the selection of “information rich cases” who can provide in-depth information on the phenomenon of interest, 26 which for this study was to learn about caregiving in PD. Thus, study participants were former carers of PwP where the PwP had died between 1-2 years prior to study enrollment. We intentionally chose former carers as they had lived experiences in caregiving and could (a) provide informed perspectives on all the domains of caregiving over the course of the illness, and (b) had the time to engage in this study without the immediate pressures of caregiving. Eligible participants were English-speaking adults and included former carers recruited from (1) Parkinson’s Disease and Lewy Body Dementia support groups, (2) referrals from clinicians at a neuropalliative care clinic, and (3) a pool of carers known to the research team from prior studies who had expressed an interest in participating in future studies. The research coordinator contacted potential participants by telephone and explained the study procedures and goals to all study participants prior to enrollment.
Data Collection & Analyses
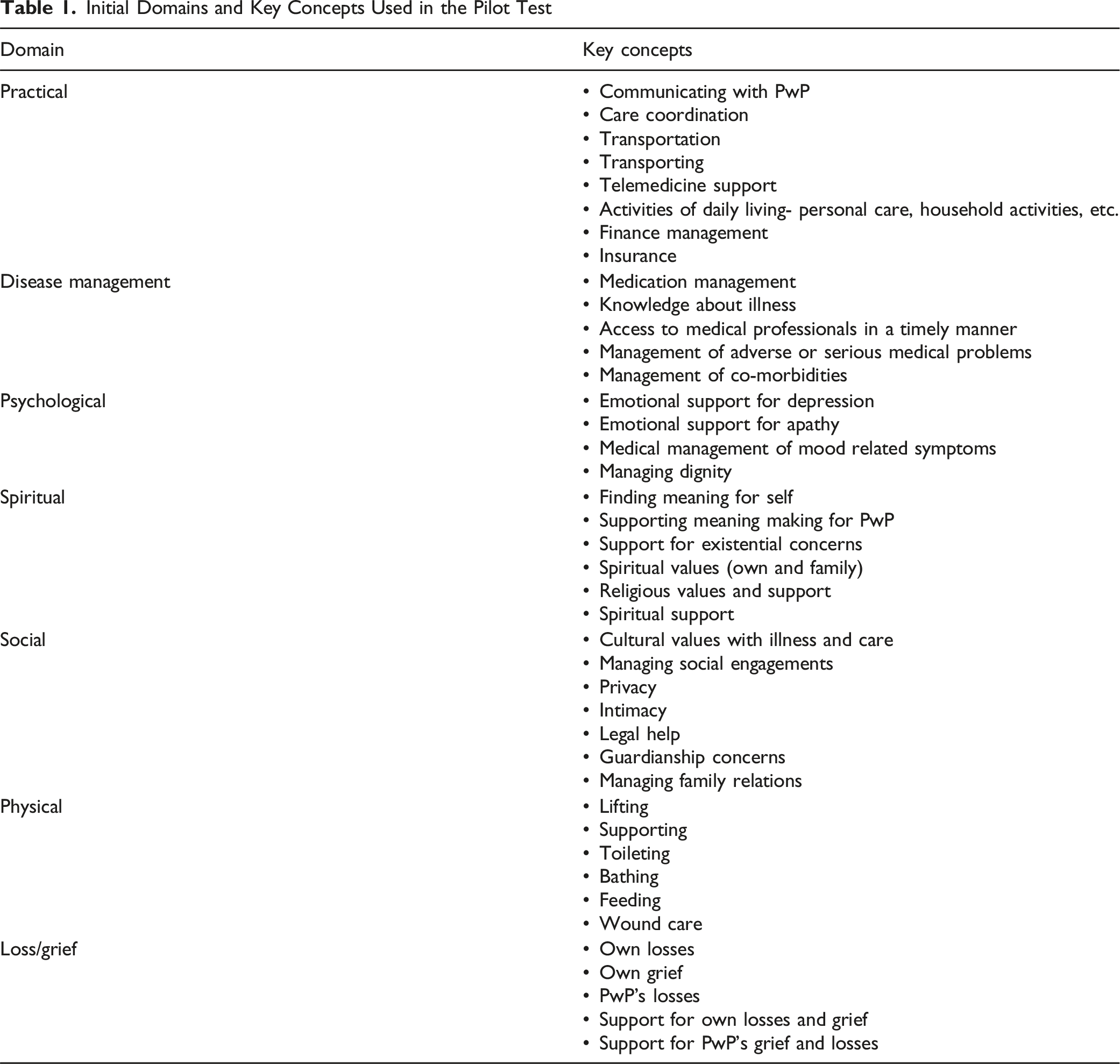
Initial Domains and Key Concepts Used in the Pilot Test
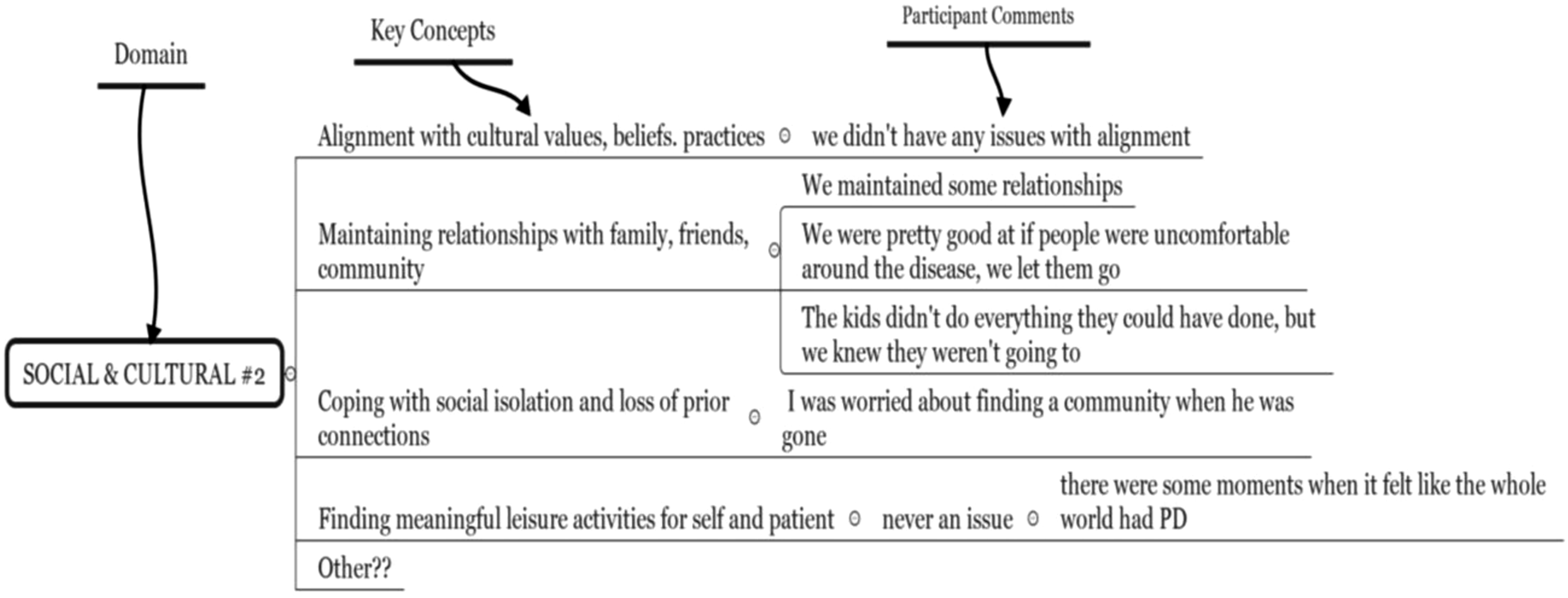
Sample mind-map and interview notes
Pilot Test of the Perspective Map
Authors SS and AC pilot tested the initial map with a former carer known to the research team to assess (a) the alignment of the domains and associated key concepts with caregiving experiences, and (b) the feasibility of using a virtual mind-map to guide the interview and facilitate effective data collection. After the interview, the participant’s feedback was sought and necessary modifications were made. For example, the domain “Loss/Grief” was renamed as “Emotional” based on participant feedback that they experienced love and gratitude in addition to loss and grief. The revised mind map was utilized for data collection.
Data Collection
Authors SS and AC conducted online semi-structured interviews between December 2024 and May 2025 via computer video conferencing. Interviews averaged 60 min in duration (range 45-90 min) and notes were taken in real-time. All interviews were audio-recorded, de-identified, and transcribed.
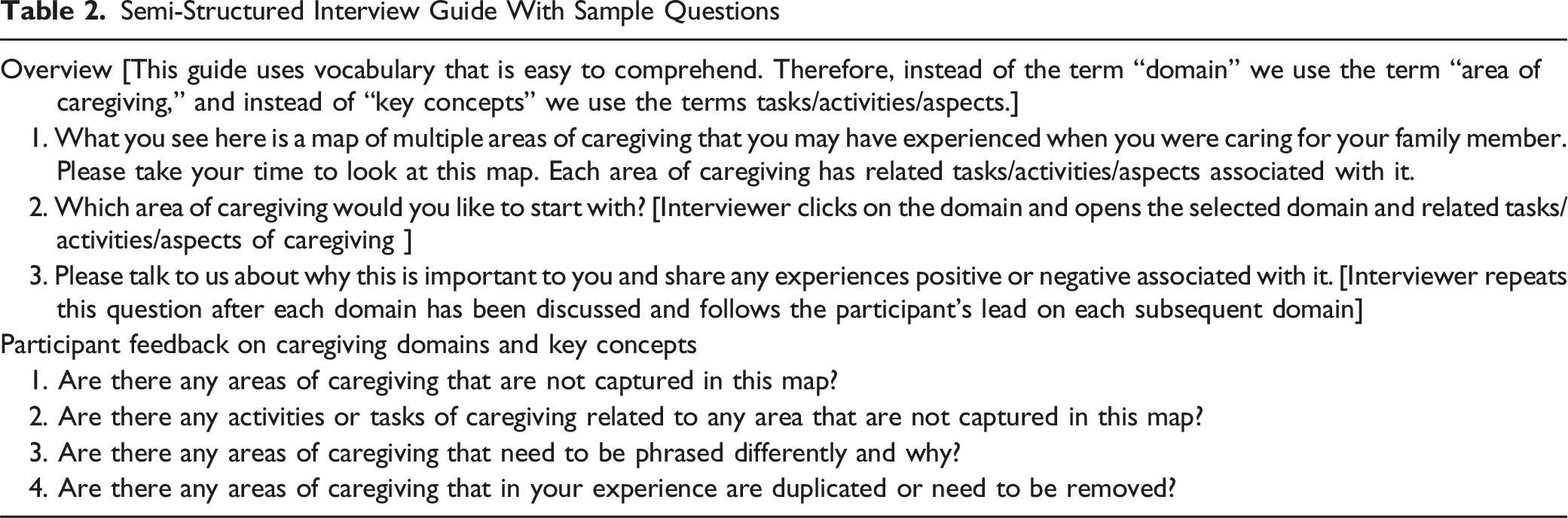
Semi-Structured Interview Guide With Sample Questions
Data Analyses
Researchers first reviewed transcripts, maps, and in-vivo notes gathered during the interview to inform the development of the codebook. Next, authors SS and AC coded five transcripts independently resolving any discrepancies through consensus. After that the remaining transcripts were coded and participant quotations and suggestions for modifications if any were extracted and organized on a spreadsheet. The research team reviewed the spreadsheet to identify patterns of responses and suggestions for modifications of wording of terms. For example, the key concept “Timely access to care” under the domain of Care Coordination was reworded as “Getting timely appointments” because the patterns of responses indicated participants’ responses related to obtaining timely appointments rather than accessing care.
Results
Demographic Characteristics (n = 15)
Study participants felt the framework of caregiving helped them reflect on their experiences and the enormity of the role that they had willingly undertaken. One participant said the having such a map that “could break it down visually like this” would have been very helpful to her when she was caring for her husband. Another participant felt it was “appalling” that most carers “do not have access” to the map so they could see “areas you need to be thinking about.”
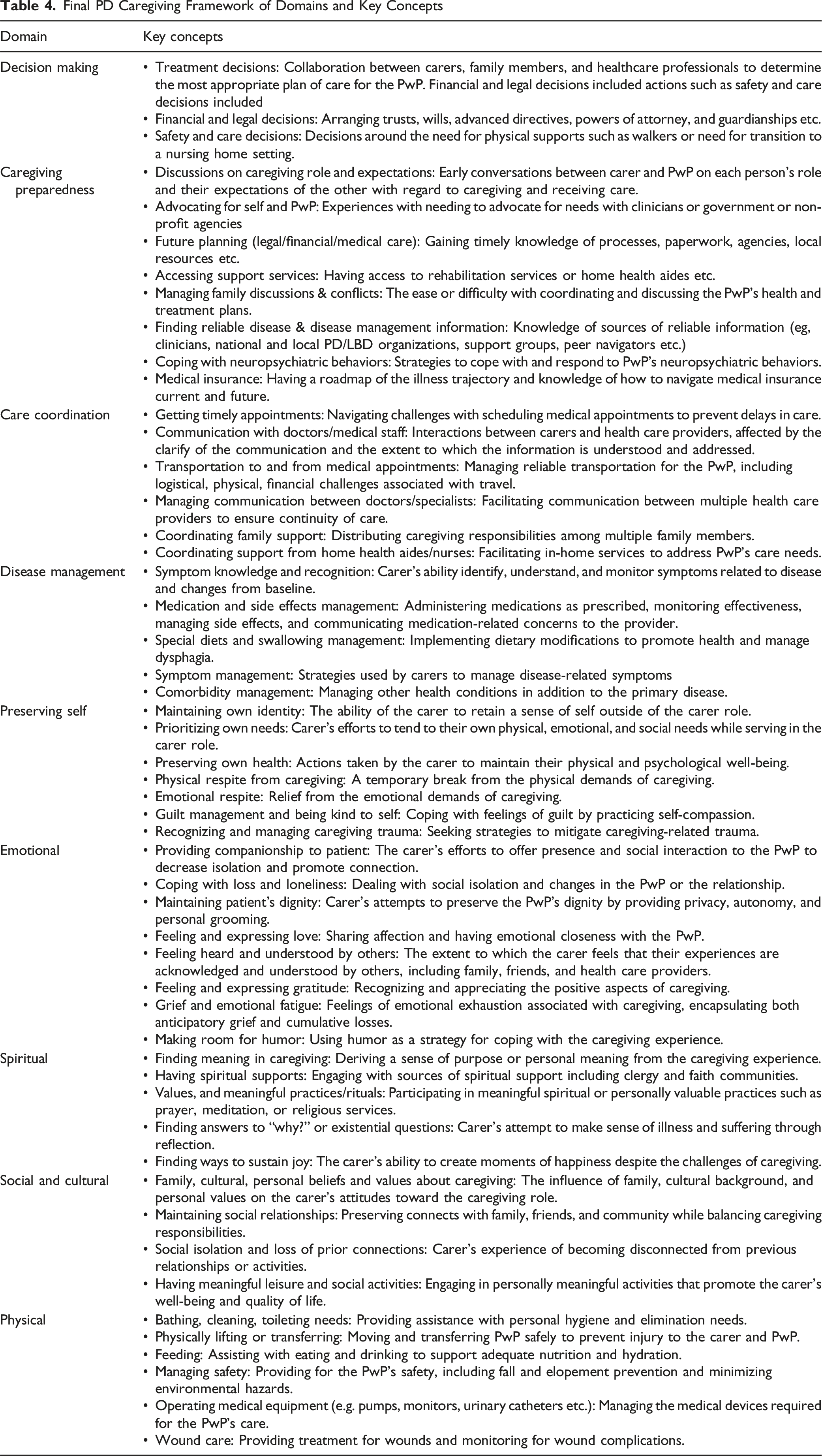
The final map of PD caregiving included 9 domains (Decision Making, Caregiving Preparedness, Care Coordination, Disease Management, Preserving Self, Emotional, Spiritual, Social and Cultural, and Physical) and 52 associated key concepts (Figure 2). Although the domains are depicted as distinct areas of caregiving, they are not intended to be discrete from each other as caregiving is woven into every aspect of daily life. A description of the domains and their associated key concepts is provided in Table 4 and a summary of study participants’ perceptions and experiences in relation to the domains and key concepts is provided below. Map of PD caregiving domains and key concepts Final PD Caregiving Framework of Domains and Key Concepts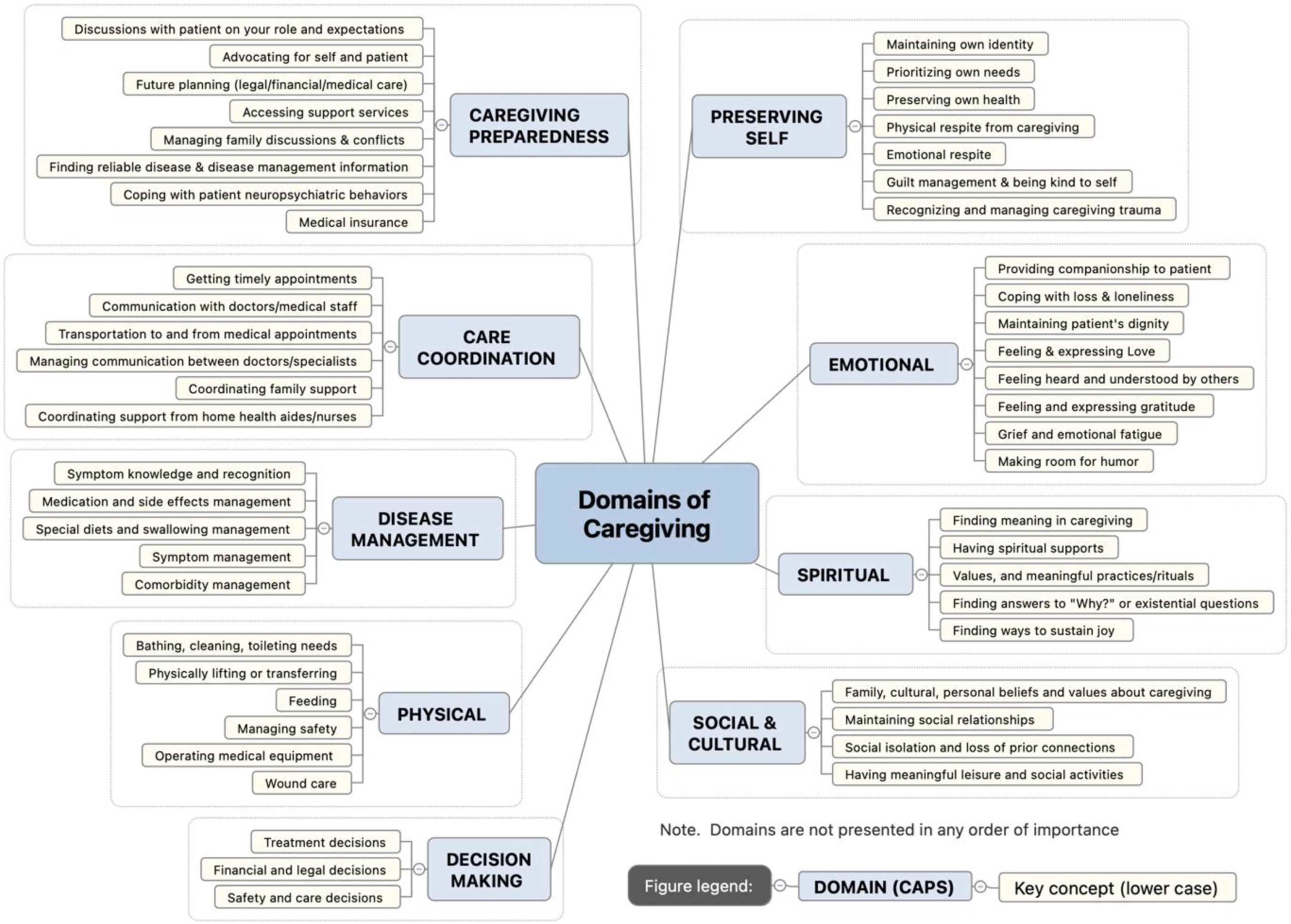
Decision-Making
The Decision-Making domain emphasizes the carer’s readiness and ability to engage in making decisions across three key concepts of treatment decisions, financial and legal decisions, and safety and care decisions (e.g. nursing homes). One participants found decision making to be challenging because she “..had to be the rational one… I wasn't allowed to have emotions because I had to make sure that I was providing education to my sister and my father, and making sure they understood.” Other participants who found this domain to be easy were able to joint decisions with their family members.
Caregiving Preparedness
Initially termed as “Access to Resources,” this domain was changed to “Caregiver Preparedness” based on participant feedback that caregiving entailed more than accessing resources. A study participant felt she had been unprepared despite reading and talking to the doctors and wished she had had the framework as it gave her specific areas to consider. She Participants reported varied experiences across the key concepts.
Care Coordination
During the pilot test this domain had been termed as “Practical.” The pilot test participant felt that the term “practical” was too broad and did not accurately represent their experiences and hence, it was changed to care coordination. To manage some non-motor symptoms, PwP are often referred to specialists such as gastroenterologists or cardiologists. Coordinating care and communication with multiple health care professionals or services can be challenging for carers. One participant reflected on his experiences with communicating PD related care with the primary care physician who “was not … an expert in her disease. So, it was literally me saying, ‘So we need a prescription for home care, and this is why,’ and getting the medical records…”
Disease Management
Managing multiple and sometimes complex PD symptoms such as dysphagia, hallucinations, or falls and symptoms related to the PwP’s comorbidities can be challenging. For a study participant, the key concept of managing medications and side effects was especially challenging, as she, “mostly learned about medication side effects on our own by looking stuff up, …’cause they’d have, you know, a million things on the side of every bottle.”
Preserving Self
With high caregiving demands, carers often experience a loss of their own identity and neglect their own needs. Initially termed as “Self-Care” this domain name was changed based on participant feedback to “Preserving Self” as it conveyed the importance of retaining their personal identity and participating in meaningful activities. This was exemplified by a participant who said, “…the other thing [about] preserving self was singing [in a choir]… gave [me back] a little bit of [my] own identity.”
Emotional
The map used during pilot testing comprised two domains, “Psychological” and “Loss-Grief.” Based on feedback that carers have positive and negative emotions and experiences, this domain was named as “Emotional” and comprised key concepts related to a range of emotions, activities, and experiences. As one participant said, “I would do a lot of crying, but not in front of him. ...I think...for a long time it for my emotions to calm down and just to dig in and do the best we could.”
Spiritual
The Spiritual domain encapsulates the carer’s and PwP’s spiritual needs and includes making sense of the challenges. Some carers often struggle to find meaning in the suffering of the PwP and others find comfort in meaningful activities. A study participant reflected on this domain and said, “…we would watch Mass together and we would pray together, … then the beliefs and rituals, like, meditations…I would…light a candle, ...take a few minutes for myself just to be present and breathe, you know? I could feel myself being restored”.
Social and Cultural
The Social domain was renamed as Social and Cultural to account for participants’ personal beliefs and values about caregiving. Caregiving often limited carers ability to interact with others as one participant recollected, “as time went on… I just didn’t go out much.” Other carers accepted these restrictions because, “… we had those cultural values. ...you get married, you stay for better or worse” even if that meant no social interactions with others.
Physical
The Physical domain includes tasks to physically care for the PwP’s such as lifting, turning the PwP in bed to minimize bed sores, affected their own health. These tasks can impact carers’ health as one participant explained, “…it got difficult getting him in the car. I only weighed 90 pounds...and...I had to… [pull] him out a chair, and I have horrible osteoporosis and pain in my back.”
Discussion
In this study, we developed a framework of the domains of PD caregiving derived from the perceptions of former PD carers on their lived caregiving experiences. The nine domains of PD caregiving and 52 key concepts in the framework illuminate the complex nature of caring for a PwP. There have been calls to recognize caregiving as a global public health issue, 29 and as a moral experience to address what really matter to carers and persons with serious illness that transcend financial costs. 30 Our framework that is based on carer insights, may facilitate clinical discussions around targeted areas of need over the long trajectory of the illness as well as the development of interventions and programs that address what matters most to carers.
Theories and models of caregiving in other illnesses have highlighted some caregiving concepts specific to different illness and stages of illness. An updated model of cancer family caregiving experience derived from concepts in the cancer caregiving literature highlighted concepts such access to treatment and support, illness related factors, and behavioral problems 31 that we found in our study as well. In a study of caregiving at end-of-life utilizing ground theory methods, a model of caregiving included four phases. 32 Broad concepts in caregiving in dementia include sociocultural factors 33 and components of self-management. 34
Several studies have examined carer burden in PD12,13,35 and caregiving has been shown to be linked to poorer carer health through increased carer burden. 36 However, in our study we examined both positive and negative aspects of caregiving. Using caregiving concepts identified in prior work18,19,27 as the foundation for our work our framework of domains of caregiving in PD focuses on contextual factors unique to PD caregiving and is based on the input of carers with lived experiences in caregiving. By deconstructing the concept of caregiving into multiple domains and related key concepts our framework provides a foundation for developing comprehensive, person-centered interventions that are aligned with what carers value most.
Clinical Implications
The domains of PD caregiving can provide clinicians with a checklist to assess and address the unique needs of carers of PwP and facilitate conversations between clinicians and carers on targeted areas of need. For example, in current models of care the emotional aspects of caregiving may be assessed through standardized depression or anxiety scales and addressed through medication or referrals to mental health counselors. Given that carers can experience emotional distress without necessarily being clinically depressed, this framework provides opportunities to go beyond referrals to mental health specialists and or pharmacological treatment. Clinicians and carers may be able to explore both positive and negative emotions so as to identify a targeted area for additional support.
The framework may guide assessment and care planning and shift the singular focus on carer burden and disease management tasks. It may help clinicians to better align care with family values and preferences, particularly within the neuropalliative care setting. Given the long trajectory of PD, this framework can be used to assess, monitor, and address the changing palliative needs of carers over time.
Strengths & Limitations
A major strength of the framework of PD caregiving is that it breaks down caregiving into concrete (though interrelated) domains and key concepts and was developed by eliciting PD carers’ perceptions of both positive and negative aspects of multiple domains and related key concepts of caregiving.
However, several limitations exist. First, the sample, though intentional, comprised former carers of PwP as opposed to current carers, which may introduce recall bias. Second, as the focus of the study was to develop a framework of PD caregiving that could lead to better support throughout the disease trajectory, we did not focus on caregiving at end of life. Third, all participants in this study were English-speaking and predominantly white, potentially excluding important cultural influences relevant to caregiving. Lastly, data collection was completed via computer video conferencing and may have excluded individuals who did not have access to computers or the internet.
Future Directions
Future research could expand on this framework by validating the domains of PD caregiving in more diverse populations of current carers. This framework can be utilized to elicit the perspectives of different types of current carers (spouses, adult children, extended family members) on the domains of caregiving that matter most to them and enable the development and testing of targeted person-centered interventions and/or programs.
Conclusions
This study provides a framework that captures the complex and multifaceted nature of PD caregiving that can facilitate targeted support to address PD carers’ unmet needs. It provides a foundation for developing targeted interventions, improving clinical practice, and informing future research aimed at supporting the well-being of PD carers.
Footnotes
Acknowledgments
The authors would like to thank the carers who participated in the interviews and contributed their insights based on their caregiving experiences.
Ethical Considerations
The Research Subjects Review Board at the University of Rochester approved this study (RSRB 00009980) as exempt.
Consent to Participate
The authors confirm that as per the approved study protocol, verbal consent to participate was obtained from study participants and written consent was not required for this work and hence was not obtained.
Author Contributions
(1) Research Project: A. Conception, B. Design C. Execution. (2) Analysis: A. Design, B. Execution, C. Review and Critique. (3) Manuscript Preparation: A. Writing of the First Draft, B. Review and Critique.
S.S: 1A, 1B, 1C, 2A, 2B, 2C, 3A, 3B. KCM: 2C, 3A, 3B. A.C: 1A, 1C, 2A, 2B, 2C, 3B. J.R.M.: 1A, 1B, 2A, 3B. B.M.K.: 1A, 1B, 2A, 2C, 3B.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: First author, S. Seshadri received funding from National Institute on Aging, National Institutes of Health (1K01AG084878-01A1), and senior author, B.M. Kluger received funding from the National Institute on Aging K02AG062). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. All other authors report no relevant disclosures and declare there are no conflicts of interest relevant to this work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Individual participant data will not be shared. Although data were de-identified, it may be possible to identify respondents based on demographics and interview responses. Aggregated data are provided in the manuscript and can be shared upon request with qualified investigators whose proposed data use is approved by the study team.