
Abstract
Patients with advanced hematological malignancies often have red blood cell (RBC) transfusion needs at the end of life (EOL) to improve debilitating anemia-related symptoms. Given that patients with hematologic malignancies and their caregivers find that transfusions improve energy and quality of life, access becomes a critical factor influencing hospice enrollment decisions, given variable access to transfusions in hospice settings. Additionally, because blood is a finite resource, this raises important questions about its availability in hospice care. This paper aims to explore the clinical, ethical, financial considerations surrounding RBC transfusions at the EOL for patients with hematological malignancies by drawing on literature in hematology, bioethics, and palliative care. One notable clinical consideration is that RBC transfusions improve anemia-related symptoms, such as fatigue, weakness, and dyspnea. At the same time, ethical considerations include the scarcity of blood. Moreover, some financial factors to consider include the cost of blood transfusions and reimbursement rates. These complex considerations impact hospice agencies’ capabilities to provide RBC transfusions at EOL. As a result, patients often delay enrolling in hospice, resulting in more aggressive treatments at the EOL and poorer EOL outcomes. Having a better understanding of such considerations will help create protocols that balance justice for all patients while improving EOL care for patients with hematological malignancies.
Introduction
Patients with advanced hematologic malignancies (HM) often have transfusion needs at the end of life (EOL), described by Mannis et al as the “transfusion tether”. 1 In a 2021 retrospective study of patients with advanced cancer receiving home hospice care in Bologna, Italy, patients with HM had the highest probability of receiving a transfusion, with the average number of transfusions per patient higher than in solid tumors. 2 For example, in acute myeloid leukemia (AML), the median number of red blood cell (RBC) transfusions was 16 in the last 6 months of life. 3 Although there is no high-quality evidence for the benefits of RBCs at the EOL, multiple studies report that HM patients experience subjective improvements in bothersome symptoms, including fatigue, bleeding, weakness, and dyspnea, following RBC transfusions.1,4 As a result, transfusion availability plays a role in hospice decisions.
Patients and malignant hematologists alike note the crucial role of access to RBC transfusions in hospice enrollment decisions.5-7 In a survey study, 61.7% of malignant hematologists agreed or strongly agreed that they would refer more patients to hospice if transfusions were provided by all hospice agencies. 8 Delays in hospice enrollment due to transfusion needs lead to worse EOL outcomes. 9 Additionally, transfusion-dependence, given the noted improvement in anemia-related symptoms with transfusions, is the most common reason for disenrollment from hospice. 10
Main Ethical, Clinical and Financial Considerations for Red Blood Cell Transfusions at the End of Life
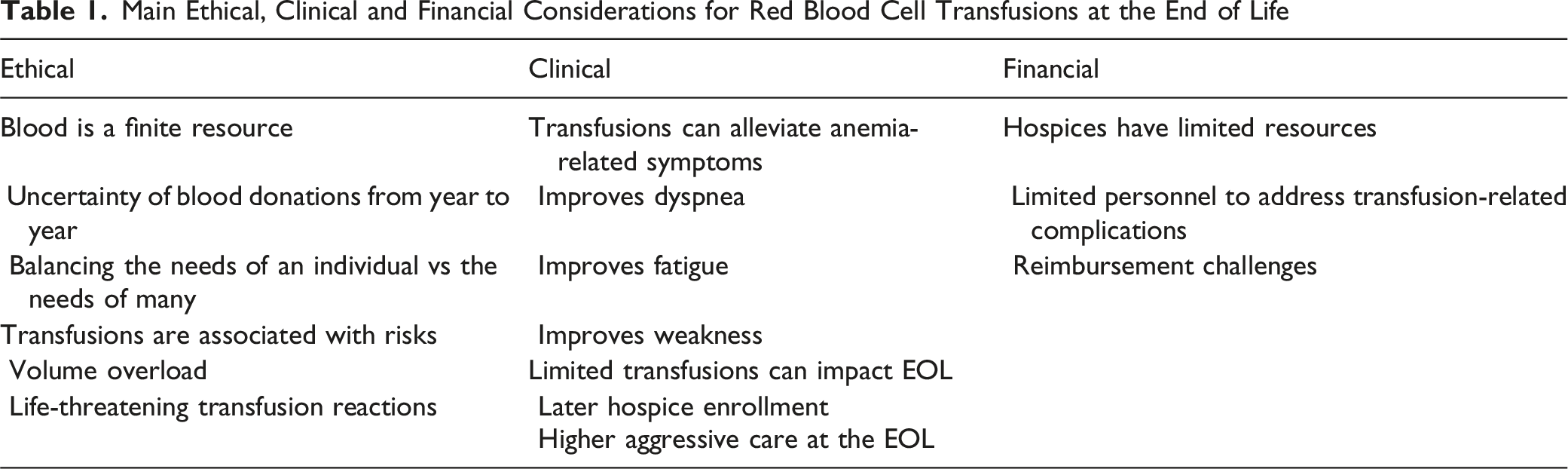
Clinical Considerations
RBC Transfusion Support Alleviates Symptoms at the EOL
There is significant evidence suggesting the benefits of RBC transfusions at the EOL. 13 However, the level of supporting evidence is low given the absence of randomized studies, which are admittedly very difficult due to ethical concerns, hence their absence in the literature. 14 Additionally, objective measures correlating with patient-reported improvements in symptoms with RBC transfusion are lacking, which can also make the benefits of RBC transfusions difficult to appreciate.15,16 Irrespective of this, the subjective improvement in symptoms with RBC transfusions has been noted in multiple studies in up to 70% of patients, though these benefits may not be durable.14,15,17,18
Orme et al. explored the experiences of hematology patients in the UK receiving RBC transfusions in a day hospice setting, who reported improvements in fatigue and dyspnea with transfusions. 13 Similarly, a prospective cohort study of 97 patients with advanced malignancies, including hematologic malignancies, evaluated the impact of transfusions on dyspnea, weakness, and overall sense of well-being using visual analog scales with total scores ranging from 0 to 10. Scores reported by patients post-transfusion reflected improvements in dyspnea, weakness, and overall well-being. 19
Despite the time commitment and risk of complications, patients and caregivers alike endorse that transfusions improve energy, allow patients to engage in desired activities, and ultimately enhance QOL during their remaining time. 20 With this in mind, the 2020 American Society of Hematology guidelines for AML in older patients included a conditional recommendation for RBC transfusions for older adults with AML not receiving anti-leukemic therapy (EOL or hospice care). 21
There is a clear benefit from a symptom perspective with transfusions at the EOL, but it is worth noting that providing such services can be intensive. For patients and caregivers, transfusion services are not routinely provided at home, so they must travel back and forth to the clinic, introducing the concept of time toxicity.22,23 Transfusions at the EOL also have the potential to 1) increase strain on transfusion services for cross-matching blood, as this can become more challenging with more transfusions over time, and 2) require greater manpower from a nursing perspective to administer transfusions, in some cases outside of regular hours, and monitor transfusion reactions. 24
Limited Access to Transfusions Negatively Impacts EOL Care
Limited access to RBC transfusions at EOL delays hospice enrollment, increases the rates of hospital utilization, chemotherapy use, and death in the hospital away from home.3,18,25 In a cross-sectional survey of hospices in the US, only 2.7% reported always providing RBC transfusions, 40.7% sometimes offered transfusions, and 54.9% never offered transfusions. 9 For those who ultimately enroll in hospice, the limited access to transfusions can result in a shortened length of stay of 6 vs 11 days for transfusion-dependent vs transfusion-independent patients, respectively. 26
Hospice utilization improves EOL by reducing aggressive care. Among Medicare beneficiaries enrolled in hospice, 96% were less likely to die in an inpatient setting, 44% were less likely to have an ICU stay in the last 30 days of life, and 62% were less likely to receive chemotherapy in the last 14 days of life. There was also a 38% decrease in mean Medicare spending at the EOL for those on hospice. 25
In contrast, in a retrospective study of patients from the Surveillance, Epidemiology, and End Results (SEER) cancer registry with myelodysplastic syndrome from 2006-2012 who died, transfusion-dependent patients were more likely to be admitted to the ICU within the last 30 days of life, receive chemotherapy within the last 14 days of life, and were less likely to enroll in hospice. 27 Similarly, in a retrospective study of AML patients using SEER-Medicare linked data, fewer than half of the population enrolled in hospice, and the increase was driven by late enrollment, with 47.3% and 28.8% enrolling in the last 7 and 3 days of life, respectively. 28
Ethical Considerations
Transfusions Are Finite Resources
Donors altruistically provide RBC units with an unpredictable supply from year to year, so blood may be perceived as a finite resource. 15 For example, during the COVID-19 pandemic, mandated quarantines and widespread fear of visiting healthcare facilities led to a decline in blood donations and blood product shortages. 29
The ethical principles of autonomy, non-maleficence, and beneficence at the individual patient level have been noted to be important to balance with justice for all patients when considering transfusions at the EOL, given the finite nature of RBCs. 15 Some also raise concerns about futility in allocating RBCs at the EOL, given their scarcity. Futility is a challenging concept, as perspectives of all parties involved may differ; thus, in clinical practice, it may be necessary to involve an ethics committee to help make decisions. 30
Given the finite nature of blood and the futility argument raised, some have proposed guidelines to assist in decision-making regarding RBC transfusions at the EOL for patients with anemia-related symptoms.30-32 Smith et al. proposed the following guidelines: limit transfusions to the minimum necessary to provide symptom relief, review cases requiring >2 transfusions per week with transfusion medicine, and defer transfusions for patients at the EOL if products are scarce. 30 Overall, careful thought and consideration should be given when administering RBC transfusions, given the finite and scarce nature of blood.
Transfusions Are Associated With Risks and Are Contradictory to Hospice Care
Transfusions can be associated with mild allergic reactions or life-threatening complications such as transfusion-related acute lung injury, circulatory overload, and anaphylaxis. These potential complications of varying severity and some of which can be life-threatening, in a population for which a traditional risk assessment may not be accurate, given medical complexity often with poor nutrition, co-morbidities, frailty, and deconditioning, are of concern.13,15 As a result, some hospice agencies decide that these risks outweigh the benefits and choose not to offer transfusions, but the frequency of these transfusion reactions is debatable, and pilot studies of transfusions at home have not noted such reactions.33,34
Secondly, given the scarcity of high-quality evidence on the benefits of EOL transfusions and the subjectivity of what constitutes a good death, some hospice services believe the provision of transfusions is inconsistent with hospice care.4,17
Financial Considerations
Cost, reimbursement, and related patient volume concerns are also recognized as barriers to EOL transfusions in hospice care, despite the benefits of EOL transfusions from a symptomology perspective. Hospice agencies with a high daily patient census (>50) were more likely to provide transfusions than those with a low daily patient census (≤50). 9 As of 2026, the daily reimbursement rate for routine hospice care is $225 for days 1-60 and $177 for days 61+, regardless of the level of care, which is often lower than the cost of ∼ $900-1000 per RBC unit.35,36 In a cross-sectional survey of hospices in the US, additional reimbursement for blood transfusions in hospice care was cited as “very helpful” in increasing hospice enrollment rates for patients with HM. 9 Since transfusion support at home is not routinely provided in the US, there is also an additional cost for coming to the clinic for transfusions, and it’s unclear if this should be covered as part of hospice reimbursement.
Discussion
In summary, although high-quality evidence for RBC transfusions at the EOL is limited, they clearly provide substantial benefits to patients with hematologic malignancies by improving anemia-related symptoms. 14 Thus, transfusion support at the EOL is a critical component of symptom-directed care that improves the quality of life of patients.18,25 A move towards symptom-based transfusions at the EOL would represent a shift in care for hospice agencies. Additionally, transitioning from transfusions driven by laboratory numbers alone to symptom-based triggers would represent a marked change for patients and clinicians alike and could affect wait times for transfusions. 3
A widespread improvement in access to RBC transfusions at the EOL will minimize hospitalizations and promote early hospice enrollment, which provides an opportunity to experience the full benefits of hospice care. Since RBCs are finite and scarce resources, it is not surprising that we must consider ethical concepts such as individual patients’ autonomy, non-maleficence and beneficence, and justice for all. However, the needs of many should not necessarily supersede the needs of an individual at the EOL. 15 And there is no clear evidence that providing RBC transfusions in this setting negatively impacts the supply for others who are not at the EOL.
In conclusion, policy-level changes, in the form of Medicare hospice benefit supplements, are needed to offset the costs and reimbursement challenges faced by hospice agencies, enabling them to provide transfusion support for patients with hematologic malignancies at the EOL and, overall, to improve EOL outcomes.
Footnotes
Acknowledgements
We would like to thank Dr. Misha Angrist at Duke University for reviewing and providing feedback on early versions of this manuscript. AOT is supported by the National Clinician Scholars Program, the American Society of Hematology Fellow Award, and Conquer Cancer. TWL is a Scholar in Clinical Research of Blood Cancer United.
Ethical Considerations
This article is a synthesis of previously published literature, no new studies involving human participants or animal subjects were performed.
Author Contributions
Taylor: conceptualization, background research, writing and editing of initial and final drafts
Reyes-Rodriguez: background research and writing
LeBlanc: supervision, reviewing, and editing
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Taylor: The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Reyes-Rodriguez: The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. LeBlanc: The author has received honoraria for consulting/advisory boards from AbbVie, Agilix, Agios/Servier, Apellis, Astellas, Autolus, BMS/Celgene, Daiichi-Sankyo, Genentech, Geron, Gilead, GSK, Lilly, Menarini-Stemline, Novartis, Novo Nordisk, Pfizer, Syndax, and Taiho; speaking related honoraria from AbbVie, Agios/Servier, Astellas, BMS/Celgene, Daiichi-Sankyo, Geron, GSK, Incyte, Kura, Menarini-Stemline, Syndax, and Rigel; equity interest in Dosentrx and ThymeCare (stock options in privately-held companies); royalties from UpToDate; research funding from AbbVie, AstraZeneca, BMS, Deverra Therapeutics/Coeptis, GSK, Jazz Pharmaceuticals, and Novartis.
Data Availability Statement
Relevant references available for review in reference section.