
Abstract
Introduction
Heart failure (HF) is associated with substantial functional impairment and a significant global burden, particularly in rural settings. Health status is a key patient-reported outcome, and palliative care provides supportive care that improves quality of life (QOL).
Purposes
The purposes are to assess HF-related health status as a patient-reported outcome and to examine how palliative care and psychosocial factors are jointly associated with HF health status among individuals receiving home-based care in rural Appalachia.
Methods
A cross-sectional correlational design was employed using baseline survey data from rural Appalachia. Participants were adults (≥50 years) with advanced HF (N = 79) enrolled in an ongoing clinical trial. Patient-reported HF status was assessed the Kansas City Cardiomyopathy Questionnaire (KCCQ). Also, the Integrated Palliative Outcome Scale (IPOS), psychological and sociodemographic variables were measured as independent variables. Stepwise multiple regression analyses were conducted.
Results
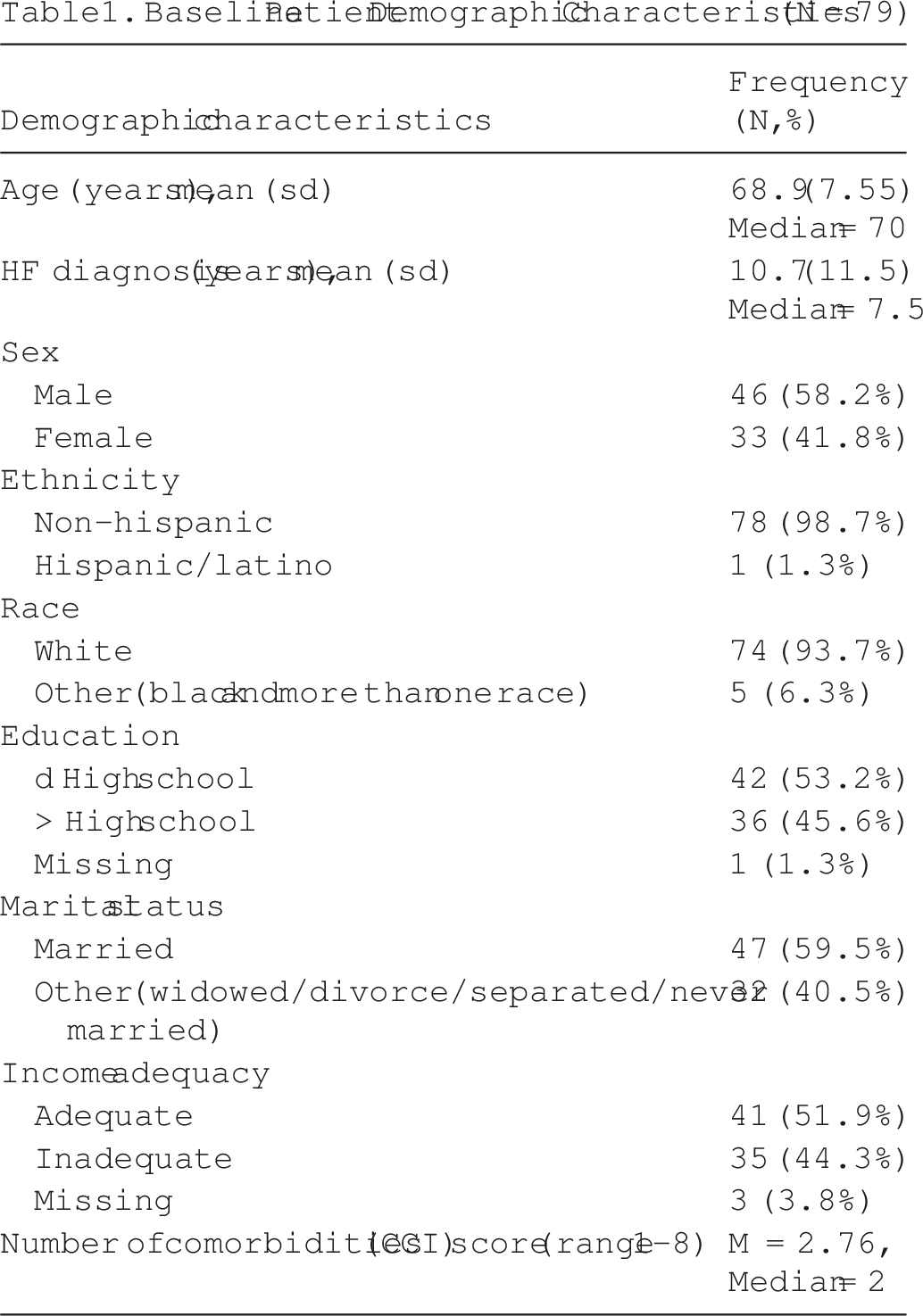
Participants’ mean age was 68.9 years (SD = 7.55); predominantly White (93.7%) and male (58.2%). The model showed strong results (R2 = .60, P < .001), with greater palliative care needs (β = −.34) and depression (β = −.28) as the main contributors to poorer HF health status, while greater income adequacy (β = .19) was associated with better HF status.
Conclusion
The HF-related health status of individuals with HF is influenced by the complex, interrelated effects of physical symptoms, psychological distress, and social factors. Integrating palliative and psychosocial measures helps identification of unmet needs and enables more targeted, patient-centered care in rural, home-based HF populations.
Keywords
Introduction
Heart failure (HF) is a chronic, progressive syndrome characterized by the heart’s inability to meet the body’s oxygen demands, spanning a broad clinical spectrum from asymptomatic structural heart disease (Stages A-B) to advanced disease with high mortality (Stage D). 1 Advanced HF causes significant functional impairment and contributes to a substantial global health burden, particularly in rural settings.2,3 HF risk increases markedly with age, 4 and population aging is expected to further raise HF prevalence. 5
HF-Related health status is a critical patient-reported outcome in HF, encompassing the complex and interrelated effects of physical symptoms, psychological distress, and social factors. The Kansas City Cardiomyopathy Questionnaire-12 (KCCQ-12) is a validated, disease-specific measure designed to assess health status in individuals with HF, including symptoms, physical and social limitations, and QOL. It generates an overall summary score that is highly sensitive to variations in disease severity and changes over time, making it a valuable tool for both clinical assessment and research. 6 Lower KCCQ-12 scores are consistently associated with an increased risk of hospitalization and mortality, whereas improvements in scores reflect better clinical outcomes and prognosis. 7
Palliative care is an essential component of HF management, providing support that improves QOL. 8 It addresses physical symptoms (eg, dyspnea, edema, fatigue), psychosocial and emotional distress, 9 while facilitating shared decision making aligned with patient values across the disease trajectory. Randomized trials show variable effects of palliative care in HF. The PAL-HF trial demonstrated significant improvements in QOL (KCCQ +9.49) and psychosocial outcomes. 10 Yet, the ENABLE CHF-PC trial found no benefit, possibly due to higher baseline health status (ceiling effect). 11 Consistent with these findings, a recent meta-analysis reported modest improvements in QOL, depression, and anxiety, but no significant effects on symptom burden or mortality. 12 These studies suggest that the effectiveness of palliative care may vary by the baseline HF health status, with greater benefits in patients with more advanced disease and poorer initial QOL. Despite these benefits, integration into home-based care for advanced HF remains inconsistent due to prognostic uncertainty and communication gaps, 13 highlighting the need to better assess palliative care needs and their impact on varying HF populations.
Depression, anxiety, and loneliness are common in rural populations due to limited mental health care access, socioeconomic hardship, transportation barriers, and chronic disease burden. 14 These challenges are pronounced in rural Appalachia, where HF mortality remains high and access to specialty and palliative care is limited. 15 In HF, psychological distress is associated with poorer QOL, increased hospitalizations, and greater health care utilization.16,17 Persistent rehospitalization and mortality despite guideline-directed therapy suggest that nonclinical factors (such as social, economic, and contextual factors) influence HF outcomes. 18
Conceptual Theory
The Theory of Unpleasant Symptoms guided this study. 19 The theory highlights three core components: (a) symptom experience, (2) influencing factors (physical, emotional, and communication/practice), and (3) clinical outcomes (ie, health status and QOL). 20 It emphasizes symptom co-occurrence and interaction, which are highly relevant in palliative care where overlapping symptoms compound functional decline.21,22 This framework guided data collection and analysis to identify symptom, contextual, and functional factors influencing HF health-related QOL and palliative care needs in rural home-based settings.
The purposes of the study are to assess HF-related health status from a patient-reported survey and to examine how palliative care and psychosocial factors are jointly associated with HF health status among individuals receiving home-based care in rural Appalachia. The guiding research question was: “What is the association between HF-related health status and palliative care, psychosocial, and sociodemographic characteristics among patients with HF?”
Methods
Research Design, Sample and Setting
This cross-sectional descriptive correlational study used baseline data from patients (N = 79) enrolled in an ongoing clinical trial. 23 Participants resided in West Virginia and rural counties and included adults aged ≥50 years with advanced HF (NYHA Class III-IV; ACC/AHA Stages C-D), characterized by marked functional limitation and symptoms at rest. 1 National data indicate that 34% of adults aged ≥45 years with Stage B HF progress to advanced stages within 5 years. 24 Patients unable to complete surveys or with LVAD placement or transplant listing were excluded due to differing care pathways. The study was approved by the University Institutional Review Board (IRB #2408021376; approved August 26, 2024).
Data Collection Procedures
Baseline data were collected from February 2025 through January 2026. After providing informed consent, participants completed baseline questionnaires and returned them via prepaid envelopes. Trained staff de-identified all materials and entered data into a secure REDCap database. Rate of missing data across instruments was monitored by the project director resulting in less than 2% occurrences. This small amount of missing data was spread randomly across all instruments and thus no missing items were repeated in large enough numbers to introduce any data bias. Missing data across study instruments were minimal (<2%) and were assessed as missing at random. Participants who screened positive for severe depressive symptoms were followed up by a faith community research nurse to ensure safety and provide referrals if needed; no referrals were required.
Measures
Measures for this study were selected based on empirically validated palliative care research22,25 and guided by the Theory of Unpleasant Symptoms. 19 These measures were chosen to assess factors relevant to palliative HF home-based care in rural Appalachia.
Dependent Variables
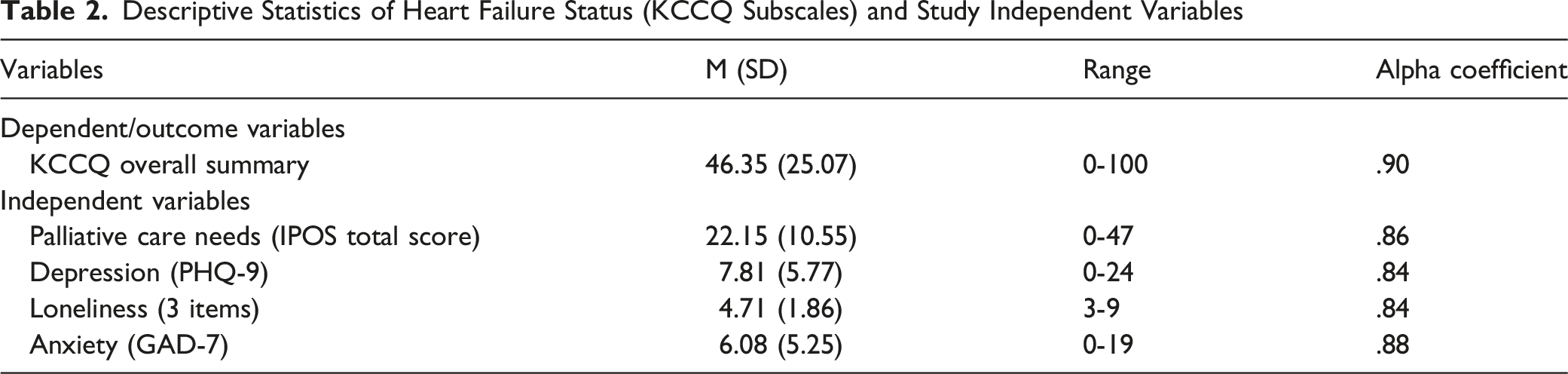
Heart failure status was assessed using the Kansas City Cardiomyopathy Questionnaire-12 (KCCQ-12), a validated patient-reported outcome measure using a 5-point Likert scale. 6 Overall summary scores were calculated, with scores standardized from 0 to 100 (higher scores indicate better health; norm-based mean = 50, SD = 10). The KCCQ Overall Summary Score was used as the primary measure, as it captures a broad patient-centered assessment including physical limitation, symptom frequency and severity, HF-related QOL, and social limitation. Internal consistency was strong (α = .90).
Independent Variables
Depression was measured by the 9-item Patient Health Questionnaire (PHQ-9), a validated self-report instrument assessing the presence and severity of depressive symptoms over the past 2 weeks. 26 Items are rated on a 4-point Likert scale (0-3), with total scores ranging from 0 to 27 (ranging from no depression to severe depression); higher scores indicate greater depressive symptom severity. A sample item was “Over the last 2 weeks, how often have you been bothered by feeling down, depressed, or hopeless?” The internal consistency (α) in this study was .84.
Anxiety was measured by the 7-item Generalized Anxiety Disorder-7 (GAD-7), a validated self-report assessing the severity of anxiety symptoms experienced over the past 2 weeks. 27 Items are rated on a 4-point Likert scale (0-3), with total scores ranging from 0 to 21; higher scores indicate greater anxiety severity. A sample item was “Over the last 2 weeks, how often have you been bothered by Feeling nervous, anxious, or on edge?” The internal consistency (α) in this study was .88.
Loneliness was assessed by the UCLA 3-Item Loneliness Scale, a brief, validated measure of perceived loneliness that evaluates relational connectedness, social connectedness, and feelings of isolation. 28 Each item is rated on a 3-point scale ranging from 1 (hardly ever) to 3 (often), yielding total scores from 1 to 9, with higher scores indicating greater loneliness. A sample item was “How often do you feel that you lack companionship?” The internal consistency (α) in this study was .84.
Integrated Palliative Outcome Scale (IPOS), a validated patient-reported measure (17 items), was used to assess symptom burden and supportive care needs. 29 The IPOS assesses physical symptoms (eg, pain, breathlessness, fatigue), emotional (eg, anxiety, low mood), and practical or communication problems (eg, information needs, practical problems). Each item is rated on a 5-point scale, with higher scores indicating greater problems or higher palliative care needs. All 17 items are summed to generate a IPOS total score. The internal consistency (α) in this study was .86.
Patient Demographic Characteristics were collected at baseline. These variables included age, duration of HF diagnosis, gender (male/female), education (high school or higher), race (white vs non-White); marital status (married vs other), and number of comorbidities. Income adequacy was dichotomized, with responses of “I can’t make ends meet” and “I have just enough, no more” coded as not adequate, and “I have enough with a little extra” and “I always have money left over” coded as adequate. Race and ethnicity were included for descriptive purposes only and excluded from analysis due to the predominantly White (93.7%) and non-Hispanic (98.7%) sample, consistent with the demographics of West Virginia. 30
Data Analysis
Data analysis was led by the principal investigator in collaboration with a biostatistician and a graduate student research assistant. Descriptive statistics summarized demographic characteristics and scale scores using frequencies, proportions, means, and standard deviations. Bivariate correlations assessed relationships among KCCQ overall summary scores, independent variables, and sociodemographic factors. The coefficient alpha statistics were used to assess the internal consistency reliability of the scale scores, while Pearson correlations were used to screen variables for inclusion in regression models. Variables with P < .20 were initially retained and subsequently removed through stepwise reduction to establish a parsimonious and well-fitting model. 31 Backward stepwise regression was applied to identify key predictors (independent variables) and simplify the model. 32 Multicollinearity was assessed using variance inflation factors (VIF) and tolerance statistics. Variance inflation factor (VIF) values ranged from 1.06 to 2.59, all below the threshold of 5, indicating no significant multicollinearity among the variables.33,34 Model fit was evaluated using adjusted R2, standardized beta coefficients (β), and overall F tests (P < .05). 32 Analyses were performed using SPSS version 31 (IBM Corp., 2025).
Power Analysis
Seventy-nine patients with advanced HF completed the baseline questionnaires. Sample size estimation was conducted using G*Power, based on a linear regression framework examining relationships between multiple predictors (independent variables) and the outcome variable (UCLA, n.d.). With a two-tailed significance level of α = .05, a sample size of 79 participants was required to achieve ≥80% statistical power to detect a moderate Cohen’s effect size of 0.2, assuming up to 5 predictors (independent variables) in the model. This sample size was considered sufficient to support the detection of clinically meaningful associations in the regression analyses.
Results
Demographics Descriptives
Baseline Patient Demographic Characteristics (N = 79)
Description of Dependent and Independent Variables
Descriptive Statistics of Heart Failure Status (KCCQ Subscales) and Study Independent Variables
Correlations Between KCCQ Overall Summary Score, Independent, and Socioeconomic Variables
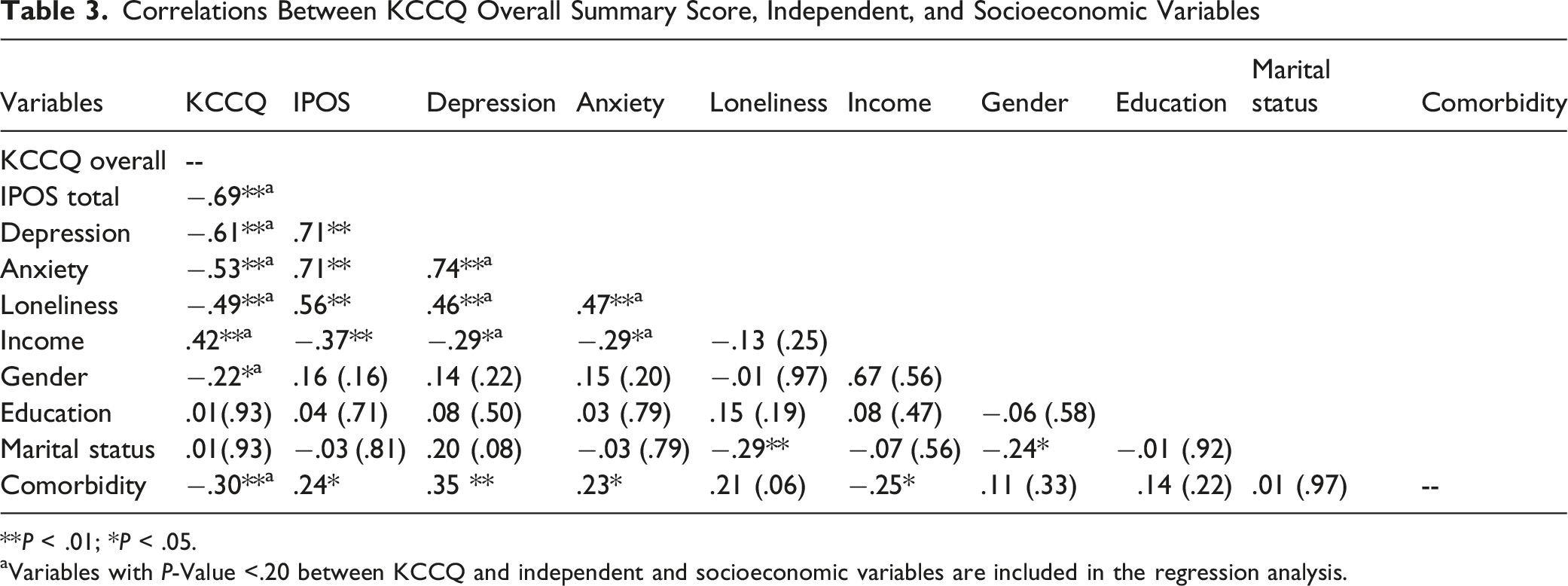
**P < .01; *P < .05.
aVariables with P-Value <.20 between KCCQ and independent and socioeconomic variables are included in the regression analysis.
Multiple Regression Results
Multiple Regression Results for Factors Associated With KCCQ Overall Summary Scores and Clinical Summary Scores
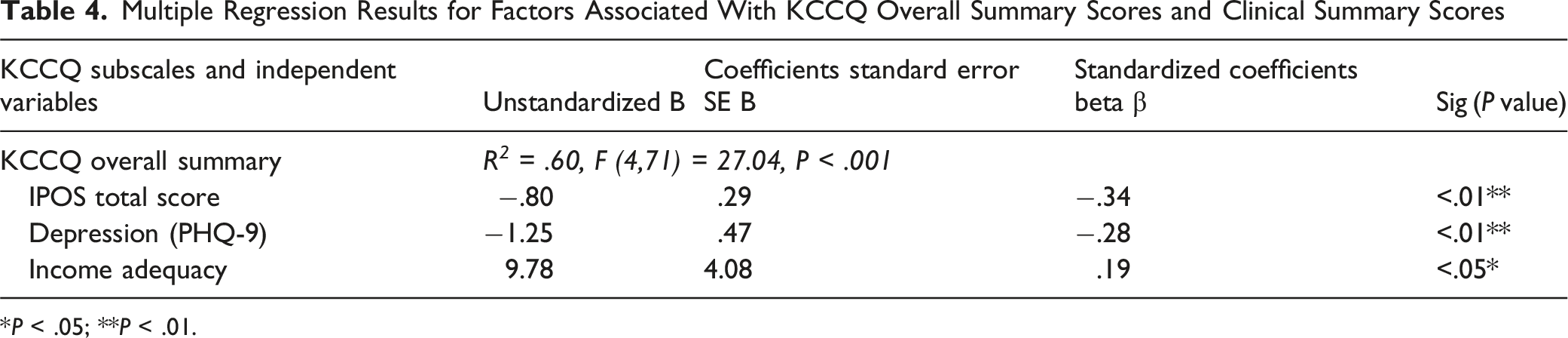
*P < .05; **P < .01.
Discussion
Main Findings of the Study
Guided by the Theory of Unpleasant Symptoms, this cross-sectional study reveals the significant and interconnected influence of palliative care needs, psychosocial factors, and socioeconomic conditions on HF health status among individuals receiving home-based care in rural Appalachia.19,20 The findings underscore that greater symptom burden, unmet palliative care needs (including emotional support, practical skills, and communication), depressive symptoms, and limited income adequacy are all strongly associated with poorer HF health status, highlighting the critical importance of integrated, multidimensional care approaches for this vulnerable population. 21
What This Study Adds?
These findings align with prior research showing variability in HF health status and HF-related QOL, 36 with implications for increased risks of mortality and hospital readmissions. Socioeconomic disadvantage and psychosocial distress likely exacerbate these risks by affecting access to care, treatment adherence, and continuity of disease management. 37 Collectively, the results underscore the critical role of nonclinical factors and support the need for patient-centered HF care that integrates physical, psychological, and social dimensions.
Independent variables associated with KCCQ Overall Summary Score were palliative care needs (physical, emotional, and communication/practical), depressive symptoms, and income adequacy. Among these, palliative care needs measured by the IPOS were the strongest predictors of poorer patient-reported HF health status, highlighting the central role of symptom burden in shaping function and QOL.38-40 The observed concordance between higher IPOS scores and poorer KCCQ outcomes is consistent with prior evidence supporting the sensitivity of IPOS to symptom burden in HF.41,42 Notably, the IPOS may enhance concordance between patient-reported symptoms and clinician perceptions, particularly in identifying psychological distress, which is often underrecognized. 15
Further, routine use of the KCCQ and IPOS is important for identifying patient needs; however, screening alone is insufficient. The KCCQ has strong prognostic value, with scores <25 associated with a threefold higher risk of hospitalization and mortality compared with scores ≥ 75. 7 The 2022 AHA/ACC/HFSA guidelines recommend that palliative and supportive care be offered to all patients with HF from the time of diagnosis to improve QOL and reduce symptom burden43,44 Notably, the mean KCCQ score in this study (M = 46.35, SD = 25.07) falls between those reported in prior trials, suggesting a moderate level of health status.10-12 This supports our finding that patients with lower KCCQ scores have greater palliative care needs and may derive greater benefit from targeted palliative care interventions. 23 To be clinically meaningful, these tools should be embedded in structured HF and palliative care pathways that link identified needs to specific actions, such as symptom management, psychosocial support, spiritual care, and advance care planning.
Psychosocial distress emerged as a significant determinant of health status in patients with HF. Depressive symptoms, in particular, were strongly associated with poorer perceived HF health status, consistent with extensive evidence linking depression to adverse HF outcomes.45,46 Although depressive symptoms, anxiety, and loneliness were each significantly associated with poorer KCCQ scores in bivariate analyses, only depressive symptoms remained significant in multivariable models. This attenuation likely reflects shared variance among these constructs, suggesting that they capture overlapping dimensions of psychosocial distress. Notably, loneliness was independently associated with diminished social functioning, reinforcing the well-established link between social isolation and poorer cardiovascular outcomes. 17 These findings highlight the importance of examining psychosocial variables both individually and collectively, as multivariable modeling clarifies their relative contributions and identifies the most influential variables within the study population.
These psychosocial burdens may be especially pronounced in rural populations, where limited access to mental health services, socioeconomic disadvantage, transportation barriers, and a high burden of chronic disease further compound vulnerability. 14 Consistent with prior research, income adequacy emerged as a key socioeconomic determinant of HF health status, quality of life, and social functioning in rural Appalachia, where structural challenges are further compounded by elevated HF mortality and constrained access to specialty and palliative care, amplifying their impact on patient outcomes. 15 Aligning with findings from national HF registry studies, greater income adequacy was independently associated with better overall HF health status, enhanced QOL, and fewer social limitations.18,47 These findings underscore the pivotal role of income as a fundamental determinant of HF outcomes, shaping access to care, capacity for self-management, psychosocial well-being, and living conditions, factors that collectively influence disease progression, QOL, and survival. 48
In summary, the Theory of Unpleasant Symptoms provides a strong framework for understanding symptom burden and home-based HF care needs, informing more targeted supportive and palliative care strategies. The study findings are consistent with prior research supporting the use of the KCCQ-12 as a robust patient-reported measure of symptoms, functional status, and QOL in HF,6,39 with score variations reflecting differences in disease burden and clinical risk. 37 Depressive symptoms were significantly associated with poorer HF health status, underscoring the critical role of psychosocial distress in palliative HF care. These findings highlight the need to integrate patient-reported outcomes with palliative, targeted interventions addressing symptom burden, mental health, and social needs to improve clinical outcomes.17,49
Clinical Implications
The strength and consistency of associations between, HF status, and palliative care needs, psychological distress underscore the critical importance of HF home-based care. Optimizing guideline-directed medical therapy alongside targeted management of common symptoms such as dyspnea and pain (using medication titration, nonpharmacologic symptom management) is essential. Routine use of the KCCQ and IPOS can help identify patients at higher risk; however, meaningful improvement depends on structured care pathways that translate patient-reported data into timely clinical actions (eg, symptom management plans, palliative care referral, advance care planning discussions). 49 Screening for depression is warranted given its association with poorer HF outcomes; integrating mental health support (eg, counseling or pharmacotherapy) into HF care has been associated with reduced hospitalizations, emergency visits, and better clinical outcome. 50
Addressing unmet social needs through interdisciplinary, team-based palliative approaches (eg, linking patients to community resources, transportation, or financial assistance) may further improve outcomes.7,16 High-quality, patient-centered HF care should include routine screening for social risk factors with linkage to supportive services as needed. 47 Sustained engagement of rural populations in cardiovascular and palliative care research remains essential to advancing equitable, patient-centered HF home care. 51
Study Limitations
This cross-sectional observational study precludes causal inference, and unmeasured contextual factors (eg, social support, treatment changes) may have influenced results. Generalizability is limited by local care contexts and the predominantly White sample (93.7%), which precluded analysis of racial differences. Future research should include more diverse populations and additional contextual factors. 52 A limitation is the lack of HF type, ie, reduced (HFrEF) vs preserved pumping function (HFpEF), and ejection fraction data. This may limit identification of specific palliative care needs, especially given the underrepresentation of HFpEF in the literature. 53
The backward stepwise approach retained the strongest independent variables while excluding correlated psychosocial variables, potentially obscuring independent effects. Planned longitudinal analyses will clarify temporal ordering and directionality. Notably, a limitation is the overlap between the IPOS and KCCQ as both assess similar domains such as physical symptoms, functional limitations, and psychosocial distress. A larger study is needed to apply analyses (eg, factor analysis or residual scores) to separate shared variance and examine KCCQ and IPOS subdomains. This will help clarify independent effects and better understand palliative care needs in HF. Despite its limitations, this study’s strengths include the use of reliable, valid patient-reported outcome measures (PROMs) to comprehensively assess palliative care needs and HF health status. 54 Indeed, the majority of patients with poor HF status scores can benefit from palliative and psychosocial care.
Conclusion
The health status of individuals with HF is influenced by the complex, interrelated effects of physical symptoms, psychological distress, and social factors. The model showed strong results, with palliative care needs and depression as the main contributors to poorer HF health status, while greater income adequacy was associated with better HF health status. Integrating palliative care outcomes with psychosocial measures enhances detection of unmet supportive care needs and supports more targeted, patient-centered care in rural, home-based HF populations.
Footnotes
Acknowledgments
We acknowledge the International Palliative Care Outcome Scale (IPOS) team for granting permission to use the English version of the IPOS in this study. A paid license was obtained to use the Kansas City Cardiomyopathy Questionnaire (KCCQ) scales and subscales. The measures of comorbidities (CCI), depression (PHQ-9) and anxiety (GAD-7) are in the public domain and do not require permission or licensing fees. The authors gratefully acknowledge the patients with heart failure for sharing their experiences and completing the survey.
Ethical Consideration
The study was approved by the University Institutional Review Board (IRB #2408021376; approved August 26, 2024). Participant confidentiality was ensured through data de-identification and secure storage on an encrypted, firewall-protected server at the Health Science Center. A Safety Monitoring Committee oversees the ongoing trial. Written informed consent was obtained from all participants. All research staff completed required human subjects’ protection training.
Author Contributions
UP led the conceptualization, methodology, formal analysis, and drafting of the manuscript and served as principal investigator. CS contributed to study design, methodological guidance, and critical scientific review. UP, SW, and MW conducted formal statistical analyses. SY, JM, and SB contributed to writing, review, and editing, including review of results and the final manuscript. RON provided expert review, clinical interpretation, and palliative care context. All authors revised and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Institute of Nursing Research (NINR) Ubolrat Piamjariyakul, PhD, RN (Principal Investigator, Grant Number: 1R01NR021630).
Declaration of Conflicting Interests
The authors declare that there are no conflicts of interest related to the research, authorship, or publication of this article.
Data Availability Statement
Data supporting the study findings are available upon reasonable request. The final dataset will be made available upon completion of the longitudinal study, in compliance with National Institute of Nursing Research requirements.