
Abstract
Background
Physiotherapists are often affected by musculoskeletal disorders owing to the physically demanding nature of their occupation. However, ergonomic practice guidelines for patient management are lacking. Determining the extent to which physiotherapists apply ergonomic principles in practice is essential for developing appropriate prevention measures against musculoskeletal disorders.
Objective
To evaluate the knowledge and application of ergonomic principles among physiotherapists and to investigate the association between sociodemographic characteristics and ergonomics knowledge and application among physiotherapists in Saudi Arabia.
Methods
A total of 386 licensed physiotherapists participated in this cross-sectional survey by completing a validated structured questionnaire. Multivariable models were constructed identify independent predictors of good ergonomics knowledge and practice.
Results
Good knowledge and practice of ergonomic principles were reported by 84.2% and 65.8% of the participants, respectively. Knowledge was significantly associated with region of residence (p < 0.05), whereas practice showed no significant association with demographic or professional factors (p > 0.05). Logistic regression revealed that living in the eastern region of Saudi Arabia was a predictor of better ergonomic knowledge (odds ratio [OR]: 9.36). Lower practice levels were associated with having a diploma or PhD (OR: 0.07 and 0.31 respectively).
Conclusions
Most Saudi physiotherapists exhibit good knowledge and practice of ergonomic principles, with the physiotherapists living in the eastern region showing higher knowledge than those living in the central region. These findings suggest that ergonomic principles should be incorporated into the physiotherapy curriculum. Integration of ergonomic training in continuing education programs is essential for improved practice and cultivation of safer work environments.
Keywords
Introduction
The rate of work-related musculoskeletal disorders (MSDs) among hospital personnel is nearly twice as high as the rates recorded in other service industries, making it a significant cause of absenteeism and decreased productivity. 1 Work-related MSDs are one of the most expensive forms of work disabilities, accounting for 30–40% of the costs associated with treating work-related injuries. 2 MSDs are prevalent among physiotherapists, primarily due the required manual handling of patients during clinical evaluations and therapy sessions. 3 Physiotherapists typically work in a forward-leaning posture, which induces fatigue and increases the risk of overuse injury due to the eccentric demands placed on the neck and back muscles. 4 The most frequently reported risk factors for work-related MSDs among physiotherapists include high daily patient volume, 5 working in awkward or cramped positions,6,7 working in the same position for prolonged periods, 8 and manual lifting of patients9,10 due to a lack of assistive handling equipment. 5 Notably, the reported 12-month incidence of work-related MSDs among Saudi physiotherapists is 83.8%, with the lower back, neck, and shoulders being the most affected regions. 11 This indicates that preventive efforts against work-related MSDs among Saudi physiotherapists should be focused on low back pain and rotator cuff syndrome. 12
Ergonomics is the practice of developing instruments and designing tasks to fit the individual, ensuring that work demands align with the worker's limitations and capabilities.13,14 Ergonomic awareness has successfully decreased lower back, neck, and shoulder pain among healthcare workers. 15 A study on the association between ergonomic knowledge and workplace conditions revealed that healthcare providers who were well versed in workplace ergonomics have a lower risk of developing work-related MSDs than those who are not.16–18 Furthermore, physiotherapists who avoid lifting and alter their work routines to enhance body mechanics exhibit a lower incidence of work-related MSDs than those who do not. 19 A recent study showed that incorporating ergonomic principles, interdisciplinary teamwork, and safety measures into physiotherapy department designs could enhance the work environment. 20
The lack of specific ergonomic guidelines for physiotherapists has contributed to the high prevalence of work-related MSDs among physiotherapists in Saudi Arabia. 21 Ergonomic practice guidelines are necessary for establishing safe and healthy work environments for healthcare providers. 15 Physiotherapists often rely on their knowledge and experience to prevent occurrence of MSDs1,9,22; however, even seasoned physiotherapists may possess limited proficiency in applying ergonomics principles during patient handling.9,23 This indicates the need for integration of good ergonomic practices into workplace campaigns for healthcare workers who have a high risk of developing work-related MSDs.21,24 These campaigns should be designed to address poor awareness of good ergonomic practices, which increases the risk of developing a range of health issues that decrease productivity and may even lead to unemployment in some extreme cases.18,24,25
Although ergonomics practice is essential for preventing work-related MSDs, 26 comprehensive nationwide research on the knowledge and application of ergonomics principles among Saudi physiotherapists remains lacking. Therefore, we conducted this study to evaluate the knowledge and practice of ergonomic principles among Saudi physiotherapists and analyze the association between sociodemographic variables and ergonomic knowledge and practice.
Methods
Study design
This was a cross-sectional study based on an online survey conducted between January and April 2024. This study was approved by the Scientific Research Ethics Committee of Taif University (Ref # 45-118). This study was reported in accordance with the recommendations in the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 27
Participants
Considering the number of Saudi physiotherapists with an active practice license (n = 12,544, according the Saudi Commission for Health Specialties), we calculated the total sample size (n = 360) needed to reach a 5% margin of error and a 95% confidence interval. Approximately 493 physiotherapists were sent the questionnaire link via email and social media applications created using Google forms. A total of 386 valid responses were received and analyzed (response rate: 78.30%) (Figure 1). Lack of time and refusal were the main reasons for non-participation.
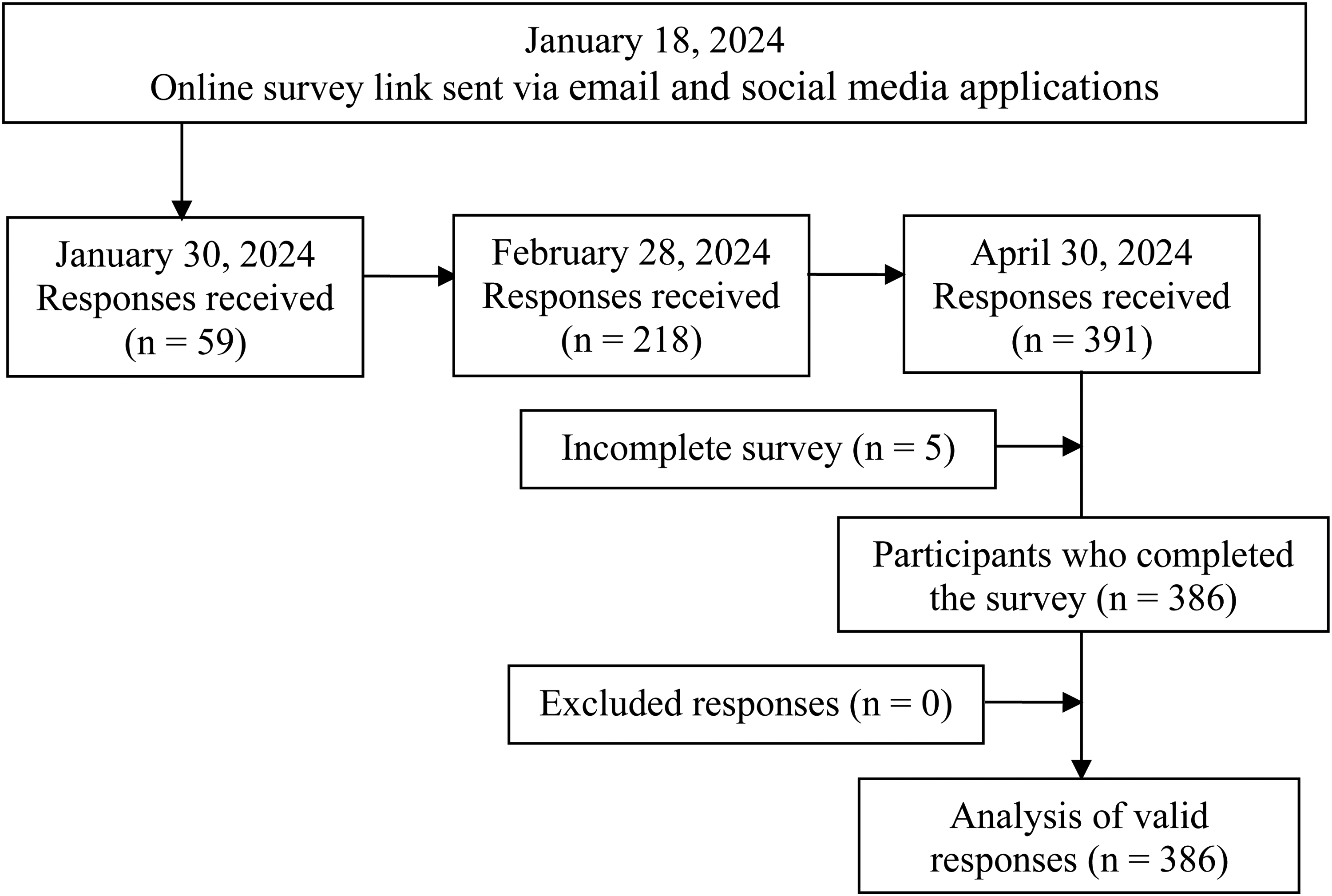
Flowchart of the study.
The following inclusion criteria were applied to ensure homogeneity of the sample: a) licensed Saudi Arabian physiotherapists; b) physiotherapists with two or more years of experience; and c) confirmation of participation. The exclusion criteria were as follows: a) physiotherapists who were not licensed to practice in Saudi Arabia; b) physiotherapists who were pregnant; c) physiotherapy interns. Participants were recruited from each of the five regions in Saudi Arabia (central, eastern, western, southern, and northern) to ensure balanced representation. An equal number of healthcare institutions were selected in each region (two Ministry of Health [MOH] hospitals, two private rehabilitation centers, and one primary health center, one university hospital, and one military hospital in each region).
Data collection
The survey questionnaire was divided into two segments. The first segment was an online debriefing page that contained information on consent to participate in the study, a general description of the study, the study objective, anonymity of the data collected, the legal rights of the participants before the commencement of the study, and instructions on how to complete the questionnaire. The questionnaire did not ask for respondents’ names or addresses to maintain anonymity. Each participant was sent three reminders to complete the survey. 28
The second segment consisted of 38 closed-ended questions, divided into sections A, B, and C. Section A (six items) included items on the participants’ sociodemographic data. Section B (17 items) included questions on the participants’ comprehension of ergonomic principles. In Section C (15 items), participants reported their application of these principles during patient handling. The participants were required to answer the questions in Sections B and C using a two-point Likert scale (“agree” or “disagree”). The second item in Section C has four sub-items, whereas the third, fourth, and fifth items have three sub-items each.
This questionnaire was developed based on information from previous studies.5,29 Adje et al. 9 previously reported that the questionnaire is valid and reliable. The content and face validity of the questionnaire were evaluated by a focus group of seven experts with vast experience in academics, clinical practice, research, and development of questionnaires related to ergonomics. The reliability of the questionnaire was 0.77 for all the items, and 0.68 and 0.69 for the items measuring knowledge and practice, respectively. The participants received one point for each correct answer and zero point for each incorrect answer. The total score for Section B and Section C was 17 points and 15 points, respectively. If participants received 50% or more of the total score of 17 or 15 points, they were considered to demonstrate good ergonomic knowledge or practice, respectively. For example, a score of 9 out of 17 points was considered indicative of good expertise. Scores less than 50% indicated weak knowledge. 5
Data analysis
The demographic variables are reported using descriptive statistics. The chi-square (χ2) test was used to evaluate the relationship between the physiotherapists’ sociodemographic characteristics and their knowledge and practice of ergonomics during patient handling. Logistic regression analysis of statistically significant variables was performed to identify predictors of the level of ergonomic knowledge or practice. Multivariable models were constructed to control for potential confounding variables and identify independent predictors of good ergonomic knowledge and practice. Data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 21.0, IBM Corp., Chicago, United States. Statistical significance was set at p < 0.05.
Results
A total of 386 physiotherapists completed the survey with valid responses. Most of the participants (68.1%) were male and approximately 64.5% and 25.9% were aged between 20 and 30 years and between 31 and 40 years, respectively. Approximately 46.9% of the participants worked in MOH hospitals, and 35.5% worked in private centers. Most of the participants (77.7%) had a bachelor's degree and 13.0% had a master's degree in physiotherapy. More than half of the participants (56.2%) lived in the western region of Saudi Arabia, 14.8% in the central region, 12.4% in the eastern region, 10.6% in the southern region, and 6.0% in the northern region. Most of the participants (59.8%) had been employed for two to five years, 15% for six to nine years, and 25.1% for more than 10 years. Approximately 84.2% of the participants showed good knowledge of ergonomic principles, while 65.8% reported good ergonomic practice. Furthermore, 65.8% of the participants with good knowledge of ergonomic principles also reported a good level of ergonomic practice. The participants’ characteristics are summarized in Table 1.
Participant characteristics (n = 386).
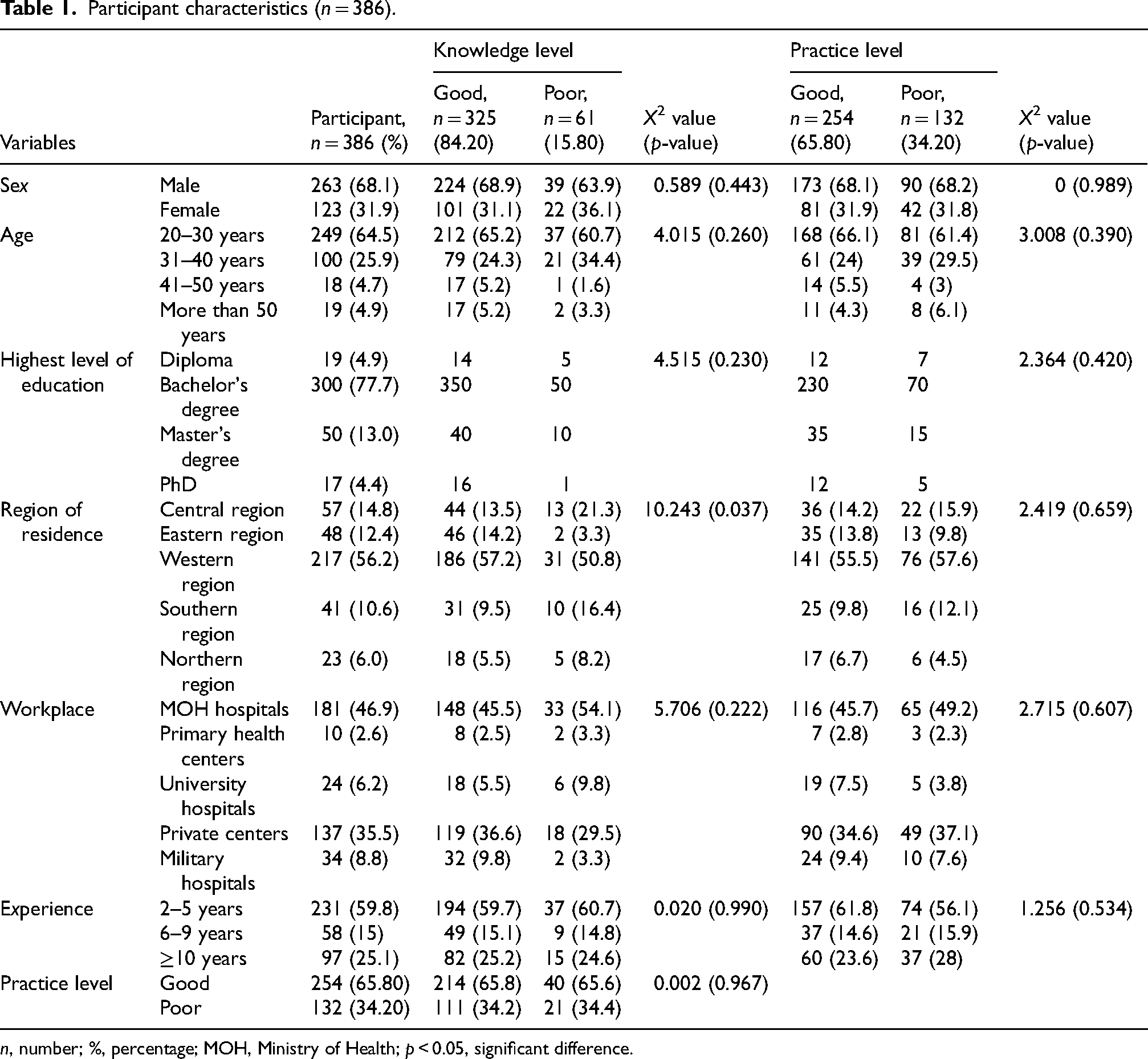
n, number; %, percentage; MOH, Ministry of Health; p < 0.05, significant difference.
The chi-square test showed that ergonomic knowledge was not significantly associated with sex, age, educational level, workplace, field of practice, or years of experience (p > 0.05). However, a significant association between ergonomic knowledge and regions of residence was observed (p = 0.037). Ergonomic practice was not significantly associated with sex, age, educational level, region of residence, workplace, field of practice, or years of experience (p > 0.05). In addition, there was no significant association between ergonomic knowledge and practice (p > 0.05) (Table 1).
Multivariate logistic regression analysis revealed that physiotherapists in the eastern region had significantly better ergonomic knowledge than those in the central region (odds ratio [OR]: 9.36, p = 0.007). In addition, physiotherapists working in university hospitals exhibited higher levels of ergonomics knowledge (OR, 0.12; p = 0.041). Univariate analysis showed a significant association between living in the eastern region and good ergonomic knowledge (OR: 6.80, p = 0.015). Physiotherapists with a diploma had significantly lower odds of demonstrating good ergonomics practice than those with a bachelor's degree (OR: 0.07, p = 0.001). In addition, physiotherapists with a PhD were less likely to demonstrate good ergonomics practice (OR, 0.31; p = 0.018). The other sociodemographic predictors were not significantly associated with ergonomic knowledge or practice (p > 0.05) (Table 2).
Predictors of the knowledge and practice of ergonomic principles (n = 386).
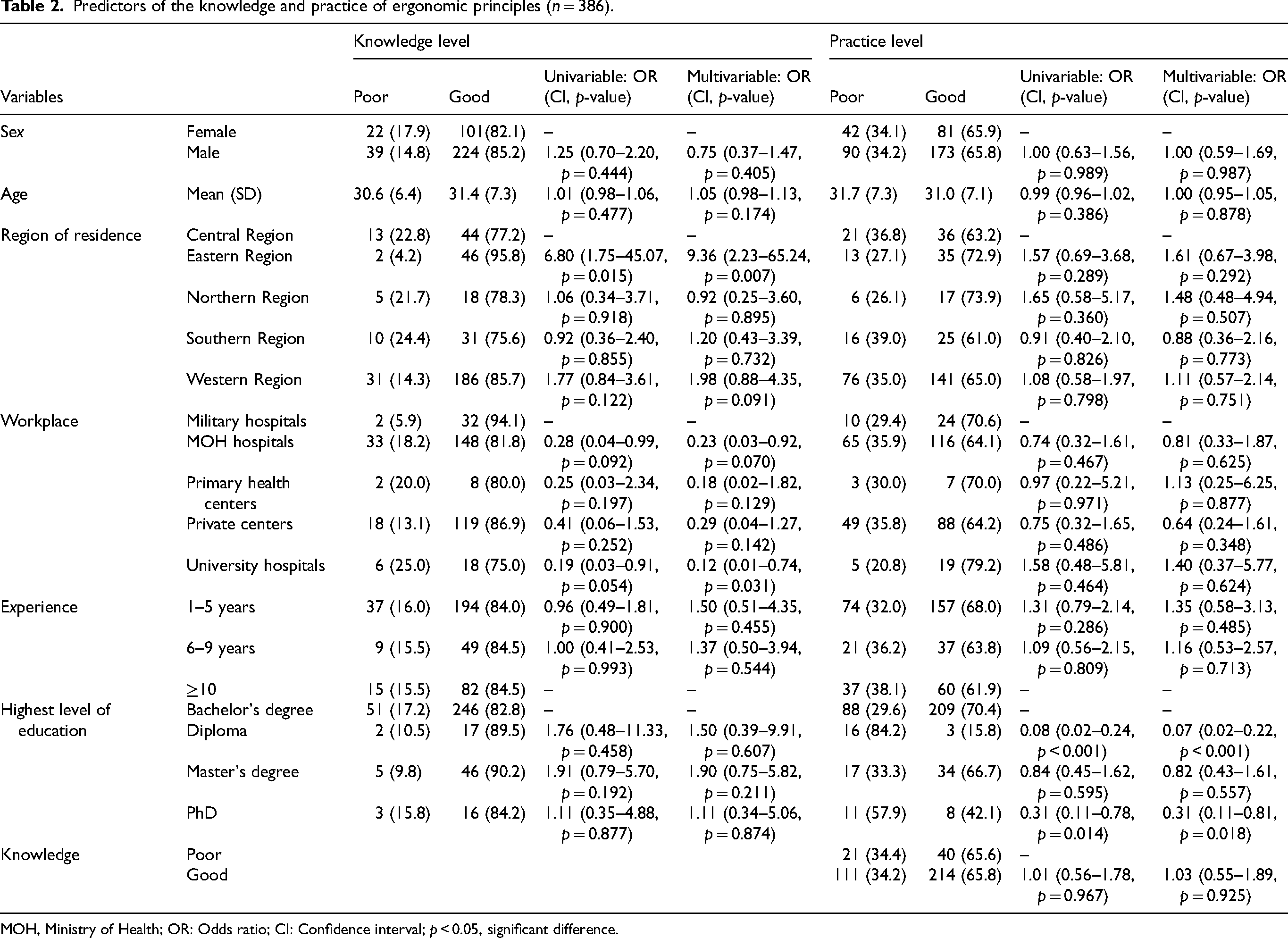
MOH, Ministry of Health; OR: Odds ratio; CI: Confidence interval; p < 0.05, significant difference.
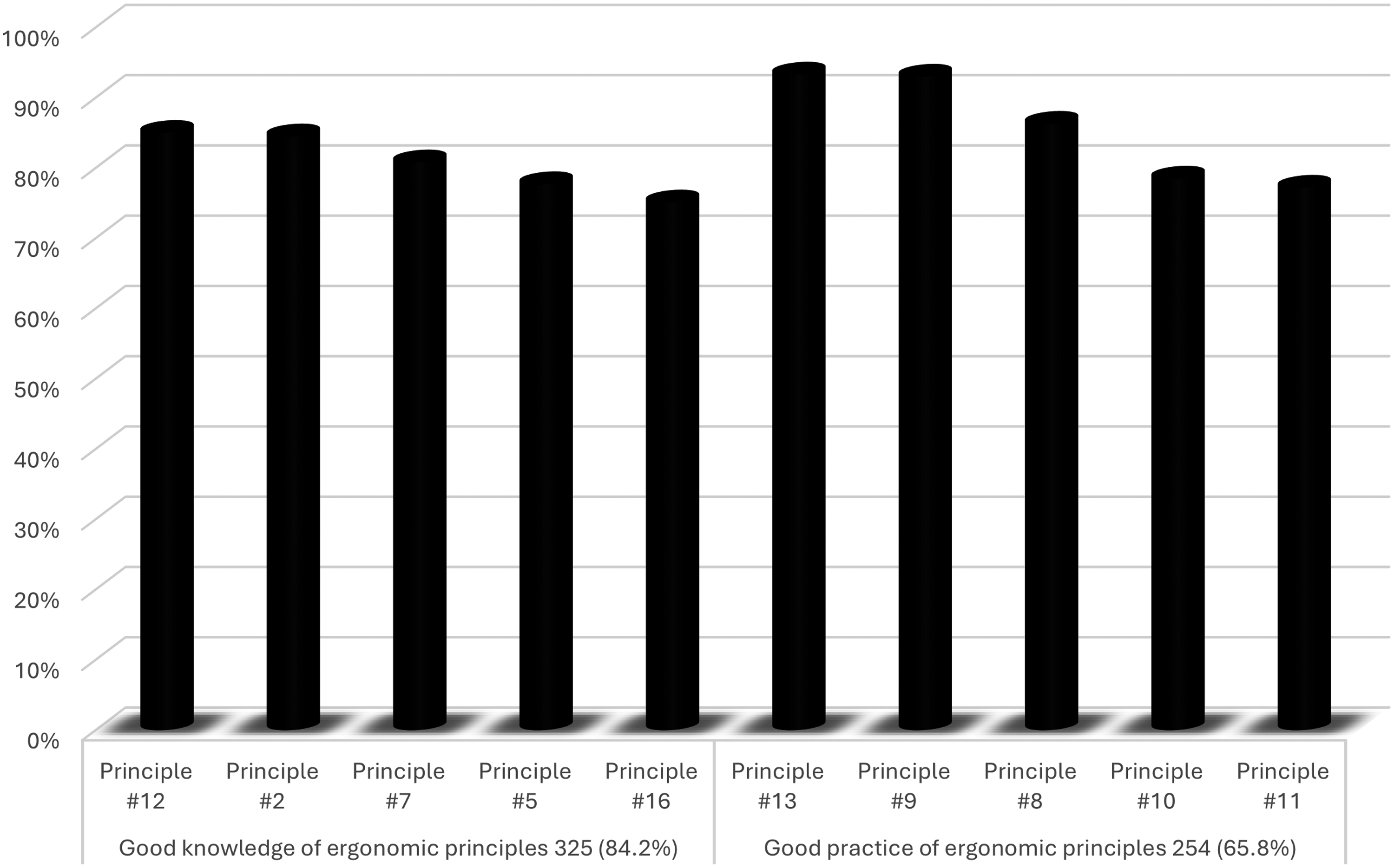
Regarding the knowledge of ergonomics, the highest percentage of correct answers was recorded for the twelfth principle (Plinth must be adjusted to match the physiotherapists’ height to aid transfer) and second principle (Patient handling involves moving or lifting a patient's body part) (85.0% and 84.5%, respectively), followed by the seventh principle (Poor ergonomics during patient handling can predispose one to injury), fifth principle (My physiotherapy training included application of ergonomic principles when handling patients), and sixteenth principle (Patient-handling training must be conducted once a year) (80.8%. 77.7%, and 75.1%, respectively) (Table 3 and Figure 2).
The top five ergonomic knowledge and practice principles with the highest frequency of correct answers.
Knowledge of ergonomic principles when handling patients (n = 386).
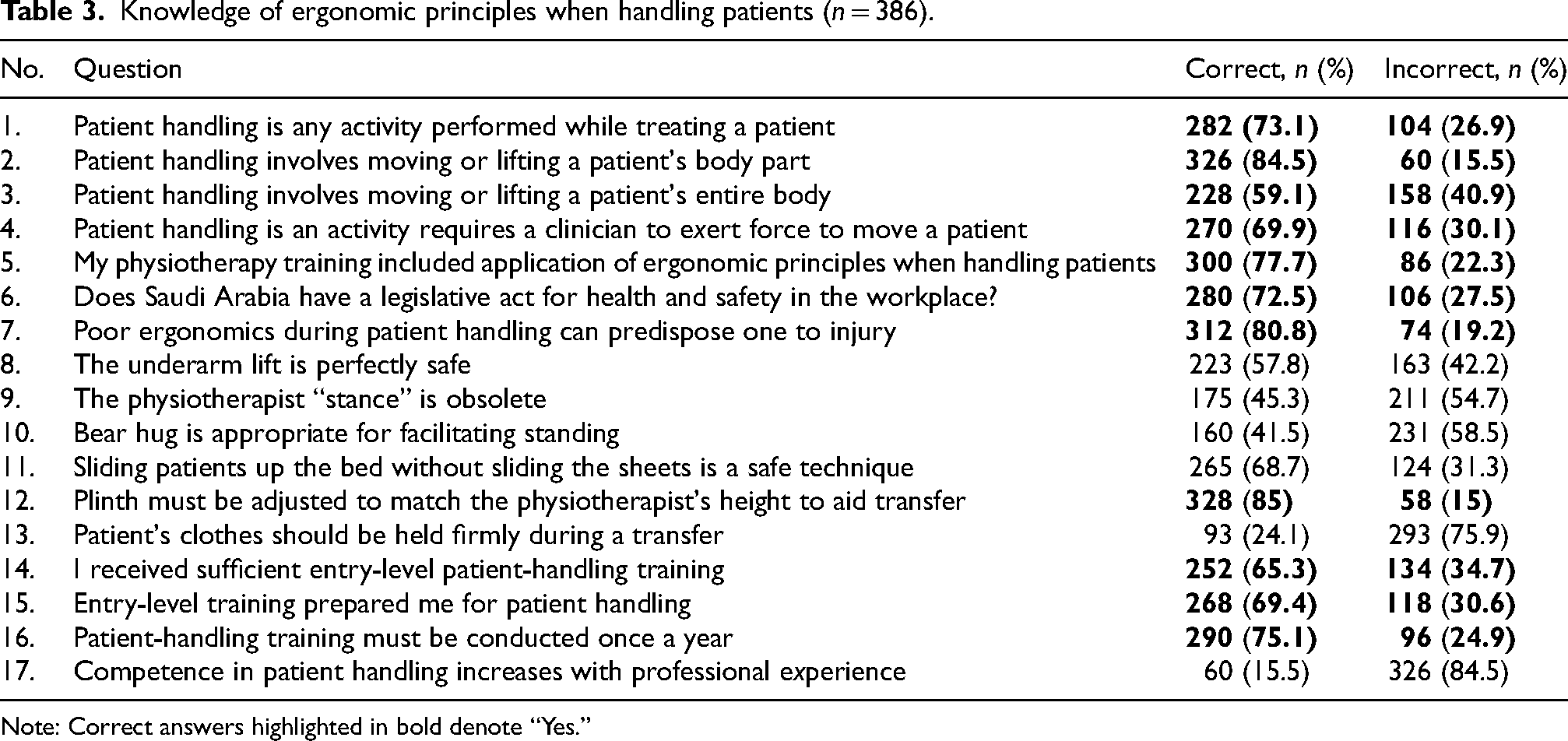
Note: Correct answers highlighted in bold denote “Yes.”
Regarding the practice of ergonomic principles, the highest percentage of correct answers was recorded for the thirteenth question (You always maintain a straight back when a static posture is required) and ninth question (You allow enough time for patient-handling tasks) (93.3% and 93.0%, respectively), followed by the eighth question (The equipment you need is readily available), tenth question (You purposely rotate your handling tasks), and eleventh question (You take breaks in between tasks) (86.3%, 78.5%, and 77.2% respectively) (Table 4 and Figure 2).
Ergonomics practice when handling patients (n = 386).
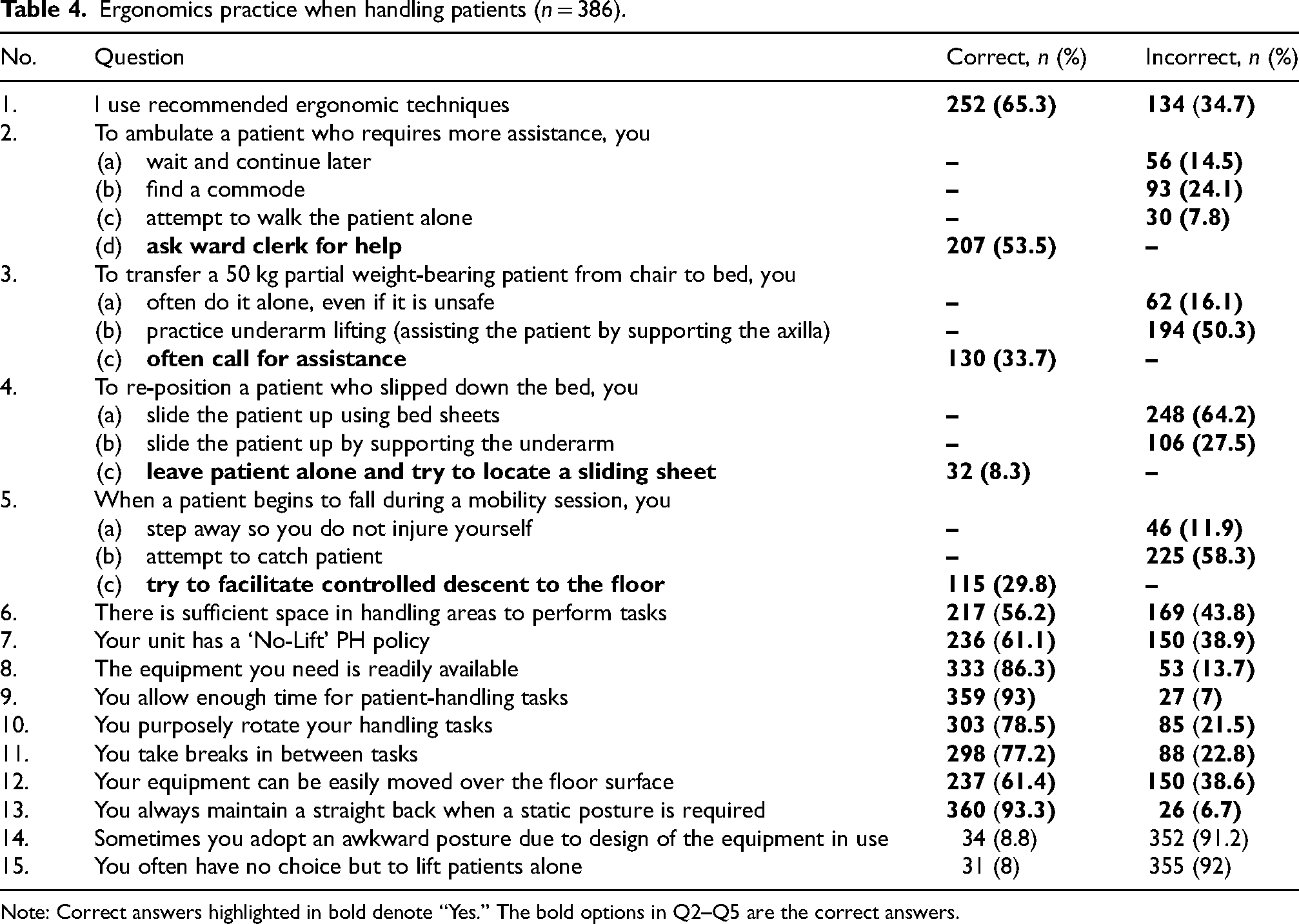
Note: Correct answers highlighted in bold denote “Yes.” The bold options in Q2–Q5 are the correct answers.
Discussion
Approximately 84.2% of the Saudi physiotherapists included in this study demonstrated good knowledge of ergonomics principles, surpassing the statistics previously reported for other Saudi healthcare workers. 21 This finding is consistent with previous reports indicating that healthcare workers often overlook ergonomic knowledge and practice in their daily clinical routines.21,30,31 However, this result is notably higher than those of a Pakistani study, in which only 48.0% of physiotherapists showed very good ergonomic knowledge, and 51% had a good attitude toward ergonomics. 32 In contrast, some previous studies have reported higher levels of ergonomic knowledge than those observed in the present study. Specifically, previous research has shown that most Nigerian physiotherapists (95.9%) exhibit good ergonomic knowledge during patient handling, 9 89.3% of healthcare providers in the United Arab Emirates have good ergonomic awareness, 15 and 95.1% of Indian healthcare professionals have a strong knowledge of ergonomics. 23 This indicates that ergonomics awareness training should be integrated into educational programs for physiotherapists 32 in Saudi Arabia to improve their knowledge levels, which will ultimately decrease the incidence of MSDs and promote safer healthcare delivery. 23
In the present study, the highest percentage of correct answers regarding knowledge of ergonomics was recorded for the twelfth principle (Plinth must be adjusted to match the physiotherapist's height to aid transfer) (85.0%). This finding aligns with those of some previous studies, which demonstrating that manual patient handling involves adjusting bed height during transport and treatment to ensure therapist and patient comfort.33,34 These studies also highlighted that an inappropriate plinth height increases mechanical load on the spine, increasing the risk of injury among healthcare providers. 35 These findings indicate that adjusting bed height to align with the therapist's height reduces the risk of lower back pain. 34
The second ergonomic principle (Patient handling requires moving or lifting a patient's body part) had the second highest percentage of correct answers (84.5%). Similar results were reported by Adje et al. 9 in their study of Nigerian physiotherapists. The authors reported that the seventh principle (Poor ergonomics during patient handling can predispose one to injury), which was ranked third in the present study, had the highest number of correct answers (99.7%), followed by the twelfth and second principles (96.9% and 95%, respectively). These findings show that the physiotherapists in both countries have adequate knowledge of patient handling and role of poor ergonomics during patient handling as a predisposing factor to MSDs, a finding consistent with reports from several studies.36–38
The eighth principle (Underarm lift is perfectly safe, 42.2%), ninth principle (Physiotherapist “stance” is obsolete, 54.7%), tenth principle (Bear hug is appropriate for facilitating standing, 58.5%), eleventh principle (Sliding patients up the bed without sliding the sheets is a safe technique, 31.3%), thirteenth (Patient's clothes should be held firmly during a transfer, 75.9%), and seventeenth principle (Competence in patient handling increases with professional experience, 84.5%) were incorrect principles. The results for these principles indicate the need for Saudi physiotherapists to acquire more comprehensive ergonomics knowledge. In addition, these findings align with those of a new Saudi study, which demonstrated the need for integration of ergonomics courses into physiotherapy educational programs. 21 Notably, a European study conducted to examine variations in curricula among universities showed that only 68.4% of the programs included patient-handling instructions. In addition, the authors reported inconsistencies in how curricula addressed workplace safety, risk assessment, use of assistive aids. 39
Regarding ergonomic practice, 65.8% of the Saudi physiotherapists in the present study demonstrated good ergonomic practice, whereas 84.2% of them exhibited good ergonomic knowledge. These findings align with previous findings indicating that Saudi physiotherapists fail to apply ergonomic knowledge during clinical routines, despite having a favorable attitude towards ergonomics. 21 Furthermore, a recent study reported that 63.5% of Emirati healthcare providers demonstrate good ergonomic practices, whereas 89.3% possess good ergonomic knowledge. 15 This reduced level of ergonomics practice compared to ergonomics knowledge mirrors the findings of an Irish study, which showed that occupational therapy students appeared to know very little about best practices and struggled to apply safe patient-handling techniques, despite having received formal training. 29 However, the level of ergonomics practice observed in the present study is greater than the those reported for Pakistani physiotherapists (41.3%) 32 and Nigerian physiotherapists (48.6%). 9 In contrast, our findings are lower than the 82.6% reported for Malaysian physiotherapy students. 40 This discrepancy could be attributed to the fact that the participants of the Malaysian study were students and had not yet encountered the practical workplace constraints that often hinder adherence to ergonomic principles in professional practice.
More than 65% of the participants in the present study reported application of ergonomic principles while handling patients. A recent study showed that working in the same position for prolonged periods is the primary risk factor for work-related MSDs among Saudi healthcare staff, whereas carrying, lifting, or moving materials and patients were the third and fourth most important risk factors. 8 These findings indicate that the quality of patient handling could be affected by workplace constraints. According to Fan et al., 41 reducing the occurrence of MSDs requires optimization of rehabilitation support equipment and incorporation of conventional ergonomics training courses into physiotherapists’ training programs. These findings are in line with recent findings indicating that nursing staff in Oman urgently need improved ergonomics practice to create a safe and sustainable work environment. 17
In the present study, the highest percentage of correct answers regarding ergonomic practice was recorded for the thirteenth principle (You always maintain a straight back when a static posture is required) and the ninth principle (You allow enough time for patient-handling tasks) (93.3% and 93%, respectively). These findings align with those reported by Nolan et al., 42 which indicated that avoiding rounding the back while lifting is a common belief among physiotherapists. However, another study indicated that healthcare providers in Belgium continue to hold false beliefs regarding the dangers of lifting a light weight with a rounded back. 43 Similarly, in the Nigerian study, the highest percentage of correct answers regarding ergonomic practice was recorded for the thirteenth and third principles (To transfer a 50 kg partial weight-bearing patient from chair to bed, you often call for assistance) (82.5% and 77.2%, respectively). The discrepancy regarding the second-ranked principle could be attributed to differences in settings and workplace constraints between the two countries. 9 Nevertheless, these findings indicate that proper use of body mechanics should be included in educational programs on ergonomic practice to reduce the risk of MSDs.44,45
The eighth principle of ergonomic practice (The equipment you need is readily available) had the third highest number of correct answers in the present study. This result is consistent with the findings of a recent review, which highlighted that the use of assistive devices for many patient-handling jobs is becoming increasingly supported by biomechanical evidence. Nonetheless, the benefits of using equipment for certain transfers have not yet been thoroughly examined. 46 Notably, lack of available equipment is the second most important factor that limits the application of ergonomic best practices among physiotherapists in Ireland. 29 This finding reflects the significance of the eighth ergonomic practice principle and suggests that Saudi hospitals could be well equipped compared to Irish 29 and Nigerian hospitals, 9 which may lack sufficient patient-handling equipment.
The third ergonomic practice principle (To transfer a 50 kg partial weight-bearing patient from chair to bed, you often call for assistance), fourth principle (To re-position a patient who slipped down the bed, you leave patient alone and try to locate a sliding sheet), fifth principle (When a patient begins to fall during a mobility session, you try to facilitate controlled descent to the floor), fourteenth principle (Sometimes you adopt an awkward posture due to design of the equipment in use), and fifteenth principle (You often have no choice but to lift patients alone) had the lowest percentages of correct answers in the present study. These results suggest that Saudi physiotherapists are predisposed to a high risk of work-related injury. Moreover, the findings align with those of a Syrian study, which showed that physiotherapists who use manual methods, lift or transport patients, and hold uncomfortable postures are 5–7 times more likely to experience neck and lower back pain. 37 The authors of an American study concluded that to reduce the risk of MSDs, hospitals should acquire beds and stretchers with power-drive technologies. 35 Our results regarding ergonomic practice principles indicate the need for further training programs or workshops for Saudi physiotherapists. In addition, our findings are consistent with those of previous studies that highlighted low ergonomic practice among Saudi physiotherapy students compared with non-Saudi professionals, emphasizing the need for further practical clinical training for Saudi physiotherapy students.21,47 These findings could be explained by the fact that undergraduate health curricula in non-Saudi universities include ergonomic courses, which were previously reported by expatriate healthcare workers employed in Saudi Arabia. 48
The results of this study revealed no association between ergonomic knowledge and practice among Saudi physiotherapists. This lack of correlation is consistent with the results of a British study, which indicated that nursing students have fair ergonomics knowledge but poor ergonomics practice. The authors attributed this theory–practice gap to unavailability of manual handling aids, lack of time, and patient needs, all of which hindered use of recommended manual handling techniques. 49 In addition, Irish physiotherapists have reported a lack of suitable equipment in their workplaces, 29 whereas Nigerian physiotherapists stated that they are forced to use manual lifting because mechanical lifters are unavailable. 9 The lack of association between ergonomic knowledge and practice could be attributed to several barriers that may be equipment-related (e.g., time constraints, device inaccessibility, and inconvenient storage), cultural and behavioral factors (peer pressure, resistance to change, and occupational socialization), and organizational factors (staff shortage and workload). 50
Job burnout is a critical occupational hazard that affects physiotherapists. 51 The results of the present study showed that age and years of experience had no significant impact on ergonomic knowledge and practice. This finding is consistent with the recent findings reported by Okayama et al., 52 which indicated that years of physiotherapist experience are not necessarily correlated with ergonomic skills. Similarly, previous reports have indicated that knowledge of ergonomics is not linked to professional practice or academic qualifications among practicing radiographers. 53 However, some studies have demonstrated associations between MSDs among healthcare workers and ergonomic awareness, age, years of experience. 15 Specifically, the results of the present study are inconsistent with those of a previous study that identified an association between ergonomic knowledge and years of experience, which was attributed the correlation to restrictions in physiotherapy departments. 9 In addition, previous reports have indicated a relationship between years of working experience and good ergonomic practices among biomedical scientists. 54 Notably, this contradiction could be attributed to differences in specialties between physiotherapy and biomedical science. These findings indicate that ergonomic practice among physiotherapists could be improved by developing prevention strategies and optimizing work conditions. 55 However, as adoption of correct body mechanics and implementation of practical skills are insufficient for preventing work-related MSDs, further research is required for the development of safer working environments. 56
In this study, physiotherapists living in the eastern region of Saudi Arabia had better ergonomic knowledge than those living in the central region. This result may be attributed to differences in physiotherapy educational curricula between these regions. 57 Notably, no study has been conducted to investigate differences in ergonomic knowledge or practice across geographical regions, which was one of the motives for recruiting physiotherapists from all regions of Saudi Arabia into the present study. This result is consistent with that of a recent study that highlighted better evidence-based physiotherapy practice skills among Saudi physiotherapists living in the eastern region. 58 These findings indicate that a sound understanding of ergonomic principles can have a positive impact on the physiotherapy profession. In addition, ergonomic training and exercise practices can reduce exposure to risk factors for work-related MSDs, improve physical fitness, and enhance job satisfaction. 59
The results of this study showed no association between sex and the level of ergonomic knowledge and practice, similar to the results observed among Nigerian physiotherapists. 9 In addition, some previous reports have indicated that sex is not related to knowledge of ergonomic work-related health issues among practicing radiographers. 53 However, this finding contrasts with the findings of a recent Saudi study, which showed lower levels of ergonomic knowledge and practice among female healthcare workers than among male healthcare workers. 21 For biomedical scientists, males show better knowledge than females, and both exhibit poor practices. 54 These findings indicate that both male and female physiotherapists in Saudi Arabia require further training in ergonomic practices.
This study showed no association between educational level and ergonomic knowledge and practice, a finding similar to that of a recent study that revealed a gap between physiotherapy knowledge and practice. 60 These findings suggest that ergonomic knowledge is acquired only at the undergraduate level without further postgraduate studies. In addition, this result may have been influenced by the uneven distribution of educational backgrounds in the cohort of the present study (77.7% had a physiotherapy bachelor's degree). Previous studies have indicated that education/academic level is not associated with the level of ergonomic knowledge or practice, suggesting that the ergonomic knowledge acquired at the undergraduate level could be sufficient for acquisition of good patient-handling skills.5,9
The absence of a relationship between educational level and ergonomic knowledge and practice in the present study is inconsistent with previous reports of relationships between the highest academic level and ergonomic knowledge, attitude, and practice among healthcare workers in Saudi Arabia. 21 Moreover, other studies have shown that educational qualifications are significantly associated with levels of practice but not ergonomic knowledge.5,9,61 Additionally, a recent study revealed a significant association between attitude towards ergonomics practice and years of education among Malaysian physiotherapy undergraduates. 40 The difference between this finding and our results could be explained by the participation of undergraduate students in the Malaysian study, who could undergo advanced ergonomics courses, compared with the participants of the present study, who graduated many years ago.
In the present study, we also investigated the relationship between workplace type and ergonomic knowledge and practice, an association that has not been explored in previous studies. Our results showed that workplace type was not related to ergonomic knowledge or practice, likely reflecting similarities in work environments, equipment, and resources between public and private hospitals in Saudi Arabia. This finding supports the previously reported absence of an association between the incidence of MSDs and workplace type (public and private hospitals) in Saudi Arabia. 8 Given that the results of the present study indicated good knowledge but poor ergonomics practice among Saudi physiotherapists regardless of workplace type, there is an urgent need for increased ergonomics awareness and training for physiotherapists in both private and public hospital settings in Saudi Arabia.
This study has some limitations. First, this was a cross-sectional study conducted using descriptive observational data. Therefore, future longitudinal studies are needed to track changes in ergonomic practice after implementation of educational reforms and to examine the impacts of specific ergonomic interventions. Notably, the design of the present study was selected to measure prevalence rather than incidence; consequently, it is susceptible to survivorship bias. Second, we could not determine whether a strong adherence to ergonomic knowledge and practice is prevalent in certain physiotherapy specialties. Future studies with larger sample sizes are needed to clarify the relationship between ergonomics knowledge and practice and physiotherapy specialties. Third, unlike interviews, an online survey does not allow participants to clarify some items. Furthermore, the use of a questionnaire for collection of personal data may have introduced response bias into the study's conclusions. However, self-report surveys are the most accurate methods for determining people's attitudes, beliefs, and opinions, which should be considered when conducting sociological research. 62 Fourth, we measured ergonomics practice using a questionnaire, which although valid and reliable, may not be as accurate as direct observation. Further research focused on revision of physiotherapy curricula Saudi Arabian universities, as well as the academic achievement of the participants, is required to address the reasons underlying the gap between ergonomic knowledge and practice among Saudi physiotherapists. In addition, further research is needed to explore the relationships between work-related MSDs, risk factors, and the knowledge and practice of ergonomic principles. Finally, researchers should ensure a proportionate representation of physiotherapists from different regions of Saudi Arabia in futures studies to achieve enhanced generalizability.
Conclusion
This study demonstrated that more than four-fifths of Saudi physiotherapists have good knowledge of ergonomic principles, while 66% exhibit good ergonomic practice when handling patients. In addition, our results showed no association between the knowledge and practice of ergonomic principles during patient-handling tasks. Collectively, the findings of this study highlight a knowledge–practice gap among physiotherapists in Saudi Arabia. Notably, the highest frequencies of correct answers regarding the principles of ergonomics knowledge were recorded for ‘Plinth must be adjusted to match the physiotherapist's height to aid transfer’ and ‘Patient handling involves moving or lifting a patient's body part.’ In addition, the highest frequencies of correct answers regarding ergonomics practice were recorded for ‘You always maintain a straight back when a static posture is required’ and ‘You allow enough time for patient-handling tasks.’ Furthermore, our results showed that the ergonomic knowledge of physiotherapists living in the eastern region of Saudi Arabia is more than nine times higher than that of those living in the central region. However, no significant association between region of residence and ergonomic practice was observed. Moreover, highest educational level, sex, age, workplace, and years of experience were not associated with the knowledge and practice of ergonomic principles. Our findings fill a gap in the existing literature by emphasizing the significance of ergonomic practice for prevention of MSDs in daily physiotherapy practice. In addition, these findings highlight the need for integration of ergonomic principles into physiotherapy curricula and training programs to promote ergonomic practice, which is necessary for creating safe work environments.
Footnotes
Acknowledgements
The authors are appreciative of the participants for their excellent contributions to this study.
Ethical approval
The Scientific Research Ethics Committee at Taif University in Saudi Arabia granted the required ethical approval (Ref # 45-118).
Informed consent
All participants signed an informed consent form which was approved by the ethical committee.
Authors contributions
Conception: RHS, and AAA. Performance of work: RHS, and AAA. Manuscript preparation: RHS, and AAA. Revision for important intellectual content: RHS, and AAA. Supervision: AAA.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data available on request.