
Abstract
Background
The emotional demands in resource-limited ICUs challenge nursing management. Trait emotional intelligence (trait EI) is a key competency, yet its link to nurses’ valuation of caring behaviors remains underexplored.
Objective
To assess the relationship between trait EI and the self-reported importance of caring behaviors among ICU nurses in Palestine. This study explicitly examines nurses’ perceived importance of caring behaviors rather than observed clinical performance, a distinction maintained throughout.
Methods
A cross-sectional study surveyed 228 ICU nurses using the SSEIT and CBAN-SF. To mitigate social desirability bias, anonymity was guaranteed and questionnaire order counterbalanced. All regression analyses report VIF and Tolerance values confirming no multicollinearity.
Results
Participants reported high trait EI (M = 118.1, SD = 11.1) and caring behavior importance (M = 99.6, SD = 10.0). A strong positive correlation was identified (r = 0.671, p < 0.001). Regression identified trait EI as the strongest predictor (B = 0.562, p < 0.001, 95% CI [0.473, 0.651]). Multicollinearity diagnostics confirmed acceptable VIF (< 2.5) and Tolerance (> 0.40).
Conclusions
This study confirms trait EI significantly predicts the value nurses place on caring behaviors in resource-limited ICUs. Conclusions pertain to perceived valuation of caring, not directly observed performance. EI development represents a viable, human-focused strategy to enhance staff resilience and care quality. The novel contribution lies in demonstrating this relationship within the understudied context of Palestinian ICUs.
Keywords
Introduction
Nurses are the backbone of healthcare systems, delivering the majority of direct patient care and significantly influencing patient outcomes. 1 This is especially true in Intensive Care Units (ICUs), where nurses and their managers face uniquely high-stress conditions characterized by critical patient acuity, complex ethical dilemmas, and frequent exposure to mortality.2–4 These environments are further challenged by understaffing and heavy workloads, which are known risk factors for compromised patient safety. 5 For nurse managers, a primary challenge is to foster a supportive work environment that mitigates burnout and promotes the retention of skilled staff within such constrained systems.6,7
These universal ICU challenges are profoundly amplified in settings like Palestine, where healthcare workers operate against a backdrop of prolonged political conflict and community-wide trauma. 8 The resulting psychological distress can cascade, impacting not only individual nurse wellbeing but also their capacity to deliver compassionate care. 9 Healthcare systems in such contexts must function with severely constrained resources, 10 where traditional technological and infrastructural solutions are often unavailable, placing a premium on human-focused strategies such as effective team functioning and leadership. 11
In these demanding environments, Emotional Intelligence (EI) emerges as a potentially crucial mitigating factor. It is important to distinguish between two main conceptualizations of EI: trait EI and ability EI. Trait EI refers to a constellation of emotional self-perceptions located at the lower levels of personality hierarchies, 12 measured via self-report. In contrast, ability EI conceptualizes emotional intelligence as a cognitive ability that should be measured with performance-based tests. This study focuses on trait EI, which reflects individuals’ self-perceptions of their emotional abilities and is particularly relevant for understanding personal coping and behavioral dispositions in the workplace. Theoretical models, such as the Broaden-and-Build Theory, suggest that positive emotional competencies can broaden nurses’ thought-action repertoires, building lasting personal resources that facilitate adaptive behaviors like empathy and compassion. 13
For nursing management, trait EI represents a trainable competency that can be cultivated to improve team dynamics, communication, and staff resilience. 14 Research indicates that EI is significantly linked to effective leadership approaches and conflict management styles in healthcare settings.15,16 Nurses with higher trait EI may be better equipped to manage their own and others’ negative emotions under pressure, thereby conserving cognitive and emotional resources that can be directed toward compassionate care. The relevance of EI is further underscored by its established relationship with enhanced critical thinking skills among regional nursing students. 17 Our findings align with other research from this context suggesting that nurses’ internal resources, such as self-concept, 18 are significant predictors of professional behaviors. Importantly, the Broaden-and-Build Theory is applied here not merely as an introductory framework but as an active explanatory lens: within the resource-limited, conflict-affected Palestinian ICU context, the theory predicts that nurses with greater emotional positivity will accrue broader psychological resources, thereby buffering the depletion caused by chronic stress and sustaining their valuation of caring behaviors even under adverse conditions. Future research with experimental designs could test whether EI-building interventions directly expand nurses’ caring values through the mechanisms this theory proposes.
Research gap, significance, and management imperative
A clear research gap exists between theoretical expectations and empirical evidence in real-world ICU settings. While theory suggests EI should enhance caring values, and prior studies in general wards support this,19,20 there is a lack of concrete evidence within the specific, high-pressure context of resource-limited ICUs. In Palestine, ICUs face severe shortages of staff and equipment, yet nursing care quality remains a priority. However, there is a lack of empirical evidence on how nurses’ internal resources, such as trait EI, influence their professional values under such constraints. Palestinian ICUs exemplify these challenges, where nursing leadership must rely heavily on fostering emotional regulation and interpersonal connections to maintain care standards despite severe systemic constraints.
The stress-resilience dynamic has been documented among nursing students in clinical training during periods of political violence, 9 and concerning levels of burnout and compassion fatigue have been identified in Palestinian ICUs.21,22 This aligns with global concerns about nurse burnout and workplace violence linked to high-stress environments.23,24 This creates an urgent imperative for nurse managers to identify and leverage human-focused strategies that can strengthen their teams’ capacity to deliver high-quality care under extreme conditions.
This study provides new findings by empirically demonstrating the strength of the trait EI-caring behavior relationship in this unique context and identifying trait EI as the strongest predictor among several variables. The findings aim to provide actionable insights for nurse managers to develop targeted, evidence-based interventions that support their teams and enhance care quality despite systemic constraints.
Methods
Study design
A descriptive, quantitative, cross-sectional study design was selected to efficiently examine relationships between variables at a single point in time, appropriate for initial exploration in this understudied population. The study was conducted across multiple mixed medical-surgical ICUs in Palestine between January 10 and March 30, 2025.
Population, sampling, and cultural context
The study population consisted of 500 nurses working in Palestinian ICUs. A systematic random sampling procedure with a random start was employed to ensure representativeness. Every second nurse was selected from comprehensive, alphabetically-ordered staff lists provided by the participating hospitals. These lists were checked and confirmed to not be ordered by seniority or any other characteristic that could introduce systematic bias. The target sample size was 218 participants (calculated using Raosoft software with a 95% confidence level and a 5% margin of error, based on a 50% response distribution for maximum variability). To account for potential non-response, 250 nurses were initially invited to participate.
A total of 228 nurses completed the questionnaires, yielding a high response rate of 91.2%. The gender distribution (66.7% male) is a notable and contextually specific characteristic of the ICU nursing workforce in this region. Cultural, historical, and socioeconomic factors in Palestine have led to a greater proportion of males in certain nursing specialties, particularly critical care, compared to global nursing norms. This demographic reality shapes the professional environment in which caring values are formed and expressed. Rather than treating this as a simple demographic variable, Section 4.3 of the Discussion draws on gender role theories to explore how a predominantly male nursing workforce may construct and enact professional caring identities differently from the largely female samples reported in international literature. This contextual specificity enhances internal validity for this population while appropriately limiting generalizability to more female-dominated nursing contexts.
Data collection instruments
Participants filled out a self-administered questionnaire comprising three parts:
Data analysis procedure
Data analysis followed a systematic sequence: (1) data cleaning and screening for missing values and outliers, (2) descriptive analysis of all variables, (3) bivariate analysis using Pearson correlation to examine relationships, (4) multivariate analysis using multiple linear regression to identify predictors while controlling for covariates. All variables (trait EI, age, gender, education, experience, shift) were entered into the regression model simultaneously based on theoretical relevance. Assumptions of linearity, homoscedasticity, normality, and independence of residuals were checked and met. Multicollinearity was explicitly assessed using Variance Inflation Factor (VIF) and Tolerance statistics. All VIF values were below 2.5 and all Tolerance values exceeded 0.40, confirming that multicollinearity was not a concern despite the inclusion of the correlated variables age and work experience (see Tables 1 to 4 and text below). To mitigate potential common-method variance, participant anonymity was ensured, validated scales were used, and questionnaire order was counterbalanced. Additionally, Harman's single-factor test was conducted, revealing that no single factor accounted for the majority of the variance, suggesting common-method bias was not a critical threat. 30 We acknowledge that Harman's single-factor test is considered a limited approach by contemporary standards and may not fully rule out common-method bias. Future research should therefore employ multi-wave or multi-source designs, such as nurse manager evaluations of caring behaviors, to more rigorously address this concern. The concurrent self-report nature of the data collection remains a limitation of the current study.
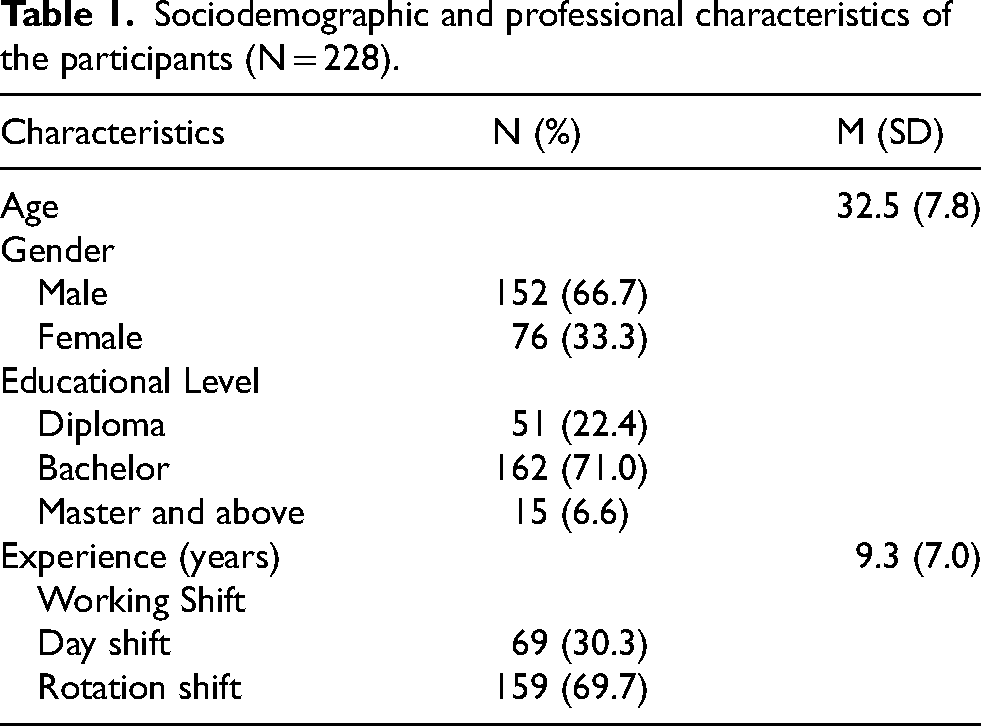
Sociodemographic and professional characteristics of the participants (N = 228).
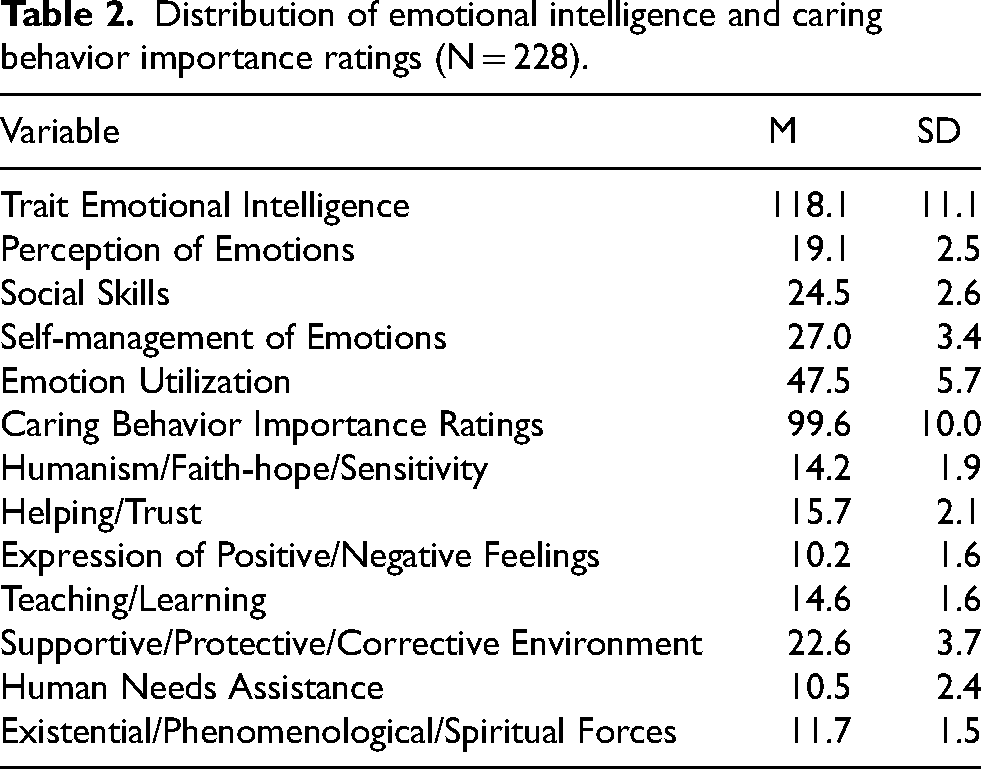
Distribution of emotional intelligence and caring behavior importance ratings (N = 228).
The relationship between trait emotional intelligence and caring behavior importance ratings (N = 228).
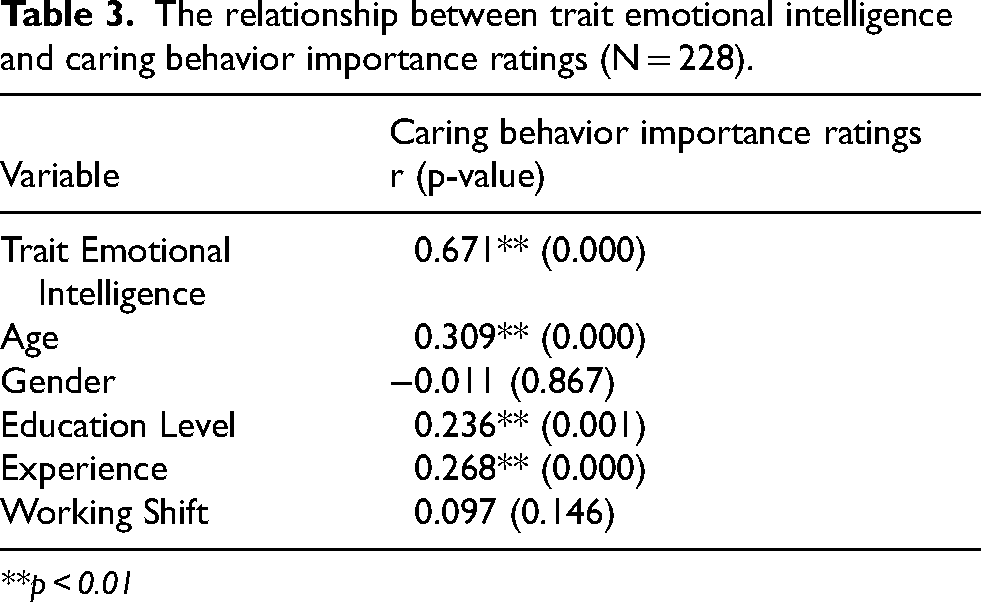
**p < 0.01
Factors associated with caring behavior importance ratings: multiple linear regression.
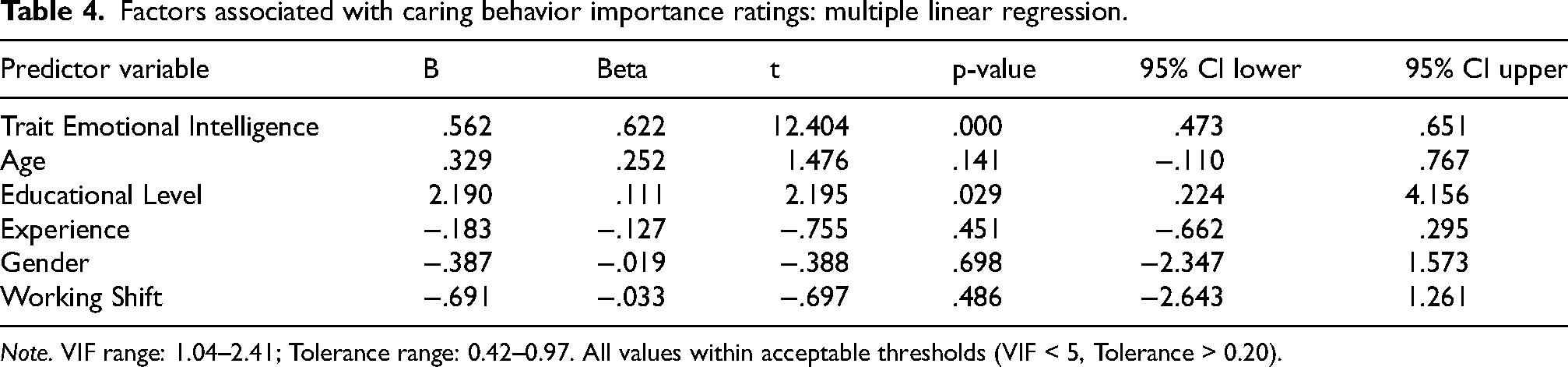
Note. VIF range: 1.04–2.41; Tolerance range: 0.42–0.97. All values within acceptable thresholds (VIF < 5, Tolerance > 0.20).
Results
Participants’ characteristics
The main result regarding participant recruitment is the high response rate (91.2%), supporting the representativeness of the sample for this specific population. Of the 250 invited nurses, 228 completed the study. The mean age was 32.5 (SD = 7.8) years. Most participants were male (66.7%), held a bachelor's degree (71.1%), and had a mean of 9.3 years (SD = 7.0) of experience. The majority worked rotational shifts (69.7%) (see Table 1).
Descriptive statistics for trait EI and caring behavior importance
The key descriptive finding is that both trait EI and caring behavior importance scores were notably high, suggesting a workforce that perceives itself as emotionally competent and places high value on caring behaviors despite contextual challenges. These high scores should be interpreted with caution, as they may partly reflect social desirability effects inherent in self-report instruments assessing professionally valued constructs. The mean total trait EI score was 118.1 (SD = 11.1). The “emotion utilization” subscale had the highest mean score (M = 47.5, SD = 5.7), while “perception of emotions” had the lowest (M = 19.1, SD = 2.5). The mean score for caring behavior importance was 99.6 (SD = 10.0). The “supportive/protective/corrective environment” domain was rated highest (M = 22.6, SD = 3.7) (see Table 2).
Correlational analysis
The most significant bivariate result was a strong positive correlation between trait EI and caring behavior importance ratings (r = 0.671, p < 0.001). Age (r = 0.309, p < 0.001), education level (r = 0.236, p = 0.001), and work experience (r = 0.268, p < 0.001) also showed significant positive associations (see Table 3).
Regression analysis
The primary multivariate result was that trait EI emerged as the strongest and most statistically significant predictor of caring behavior importance ratings. Multiple linear regression revealed a statistically significant model (p < 0.001, R2 = 0.488, Adjusted R2 = 0.479). Trait EI was the strongest predictor of caring behavior importance (B = 0.562, p < 0.001, 95% CI [0.473, 0.651]), accounting for the largest share of unique variance. Educational level was also a significant predictor (B = 2.190, p = 0.029, 95% CI [0.224, 4.156]). Age and experience were not significant in the multivariate model. Gender and working shift were also non-significant predictors (p = 0.698 and p = 0.486, respectively). Multicollinearity diagnostics confirmed that all predictors had acceptable VIF values (range: 1.04–2.41) and Tolerance values (range: 0.42–0.97), indicating that the simultaneous inclusion of age and work experience did not compromise the integrity of the regression estimates (see Table 4).
Discussion
This study provides clear evidence of a strong association between trait emotional intelligence and the importance ratings of caring behaviors among ICU nurses in Palestinian hospitals, offering concrete, actionable insights for nursing management in high-stress, resource-constrained environments.
Interpretation of association between trait EI and caring behavior importance
Each key result is interpreted as follows: The strong positive correlation (r = 0.671, p < 0.001) suggests that nurses who perceive themselves as more emotionally skilled also place greater professional value on caring behaviors. It is critical to emphasize that both measures are self-reported perceptions: the correlation reflects an association between self-perceived emotional ability and self-rated importance of caring, not between EI and objectively observed caring performance. This aligns with international literature. For instance, studies in Turkey and Iran have similarly found that nurses with higher EI report more positive patient-centered attitudes and greater professional commitment.19,20 Meta-analytic evidence further supports that EI is positively associated with job performance in nursing. 31 This relationship can be explained through behavioral mechanisms; nurses with higher trait EI are likely more adept at emotion regulation, which buffers against stress and conserves cognitive resources. This, in turn, may facilitate empathic concern and the energy required for prosocial, caring actions, as suggested by the Affect-as-Information Theory, where positive emotional states inform positive interpersonal judgments and behaviors.
The subscale analysis provides a clear diagnostic tool for managers: while nurses feel competent in “utilizing” emotions, the lower scores in “perception of emotions” indicate a specific area for development, enhancing the recognition of emotional cues in patients and colleagues.
Consistency with previous studies and explanation of differences
The findings are largely consistent with previous studies linking EI to positive professional outcomes.19,20,31 However, a potential difference lies in the strength of the correlation, which appears stronger in this study than in some general nursing population studies. 32 This difference may be explained by the acute stress and resource limitations of the Palestinian ICU context, where emotional competencies may become more salient and critically tied to professional identity and coping mechanisms. This contextual amplification effect has been noted in other high-stress healthcare environments. 33
Demographic associations and universal professional competency
The positive association with education level underscores the role of advanced critical thinking in valuing caring behaviors, supporting investments in continuing education. This aligns with evidence that educational advancement enhances nursing practice and critical thinking. 34 The absence of a significant gender association in our data warrants substantive theoretical discussion, particularly given the atypical gender distribution of our sample (66.7% male). In global nursing literature, samples are predominantly female; therefore, the majority-male composition of this study is a distinctive regional characteristic that requires contextualization beyond a simple note of non-significance. Drawing on gender role theory, caring in nursing has historically been constructed as a feminine attribute in Western contexts. However, in the Palestinian ICU setting, the high proportion of male nurses may reflect a different professional socialization process, in which caring behaviors are framed as markers of clinical competence and professional identity rather than gender-role expression. The absence of gender differences in caring value ratings suggests that, within this context, a strong professional identity as an ICU nurse may override gender-role-based differences in caring orientation. This finding supports the universality of caring as a professional nursing value when strong professional socialization is present, and reinforces the importance of designing EI development programs that engage all staff equally, regardless of gender. Future research should directly examine whether professional identity mediates the relationship between gender and caring values in male-dominated nursing workforces.
The Palestinian ICU context: A leadership challenge
The notably high self-reported trait EI scores among nurses working under chronic stress and resource scarcity merit a nuanced theoretical interpretation. Several explanatory mechanisms are plausible. First, these high scores may reflect a genuine adaptive resilience: nurses who have remained in ICU practice amid prolonged political conflict and systemic deprivation may represent a self-selected group with stronger emotional resources. Second, the scores may partly reflect a defense mechanism or cognitive adaptation, whereby healthcare professionals in contexts of chronic adversity maintain an elevated self-perception of emotional competence as a form of psychological self-protection. Third, a degree of socially desirable responding cannot be excluded, as emotional intelligence and caring are both highly valued professional identities in nursing. These three possibilities are not mutually exclusive, and their relative contributions cannot be disentangled with the current cross-sectional, self-report design. Future qualitative research should explore how Palestinian ICU nurses themselves understand and narrate their emotional experiences to illuminate which of these mechanisms predominates. This finding, coupled with documented barriers to evidence-based practice in similar settings,35,36 places a direct onus on nursing leadership to formally integrate EI into unit culture. Effective leadership has been shown to be critical for safety outcomes in hospital settings. 37 Investing in EI development is a strategic, low-resource approach to addressing the high burnout and compassion fatigue identified in Palestinian ICUs,21,22 thereby improving retention and sustaining care quality where technological solutions are scarce.
Study limitations and their implications
This study has several limitations. First, the cross-sectional design and concurrent self-reports prevent causal inference and are susceptible to common-method variance and social desirability bias, where participants may overrate their EI and caring values. The high mean scores on both instruments are consistent with potential social desirability inflation, a risk that is particularly elevated for constructs tied to professional prestige. Future studies should include a validated social desirability scale (e.g., the Marlowe-Crowne Social Desirability Scale) as a covariate to statistically control for this bias. To mitigate common-method bias, we ensured anonymity and counterbalanced the questionnaire order, and conducted Harman's single-factor test. We acknowledge that Harman's test is an incomplete safeguard by current standards. Future studies should employ multi-wave longitudinal designs or include nurse manager (supervisor) evaluations of caring behaviors as an objective, multi-source criterion variable, which would substantially strengthen causal and criterion validity. Second, and critically, we measured the perceived importance of caring behaviors, not their actual demonstration in clinical practice. Therefore, it is essential to clarify that the findings relate exclusively to nurses’ valuation of caring, not to directly observed care performance. Conclusions about actual caring performance should not be drawn from this data. Future research should employ longitudinal, multi-method designs (e.g., combining self-reports with 360-degree feedback or direct observation) and qualitative interviews to deeply explore the “how” and “why” behind these relationships. Third, the gender imbalance and specific Palestinian context may limit generalizability, though they enhance internal validity for this population. In interpreting these findings, a distinction should be made between statistical generalizability (to broader populations) and contextual transferability (of insights and management strategies to similar resource-limited, high-stress ICU settings). These limitations suggest that while trait EI is a significant predictor of caring values, it is one of several factors influencing the professional orientation nurses bring to care delivery.
Implications for nursing management and leadership
The findings provide important strategic guidance for nursing management, highlighting several avenues for practical application. First, assessment and targeted training using trait EI assessments can serve as a diagnostic tool to identify team development needs. Based on these assessments, managers can design focused training initiatives, emphasizing weaker subscales such as “emotion perception” through role-playing exercises, simulated patient interactions, and reflective practice groups.
Second, the development of concrete programs is essential. Nursing leaders should advocate for institutional resources that support evidence-based EI interventions, including communication workshops, peer coaching for stress regulation, and simulation-based training to prepare staff for challenging emotional situations. To enhance practical applicability, managers could implement low-cost, high-impact interventions such as: (1) structured brief reflective debriefings after critical incidents to process emotions collectively, and (2) establishing a peer mentoring system where nurses with higher EI support colleagues in developing emotional coping strategies.
Third, cultural integration of EI into professional practice is crucial. Leaders can champion EI as a core value by embedding it in everyday activities such as team meetings, debriefing sessions, and performance evaluations, thereby normalizing its importance across the workforce.
Finally, policy advocacy plays a key role in sustaining impact. These findings provide evidence to support the integration of EI training into national nursing curricula and continuous professional development frameworks in Palestine and comparable regions, aligning with broader international priorities for nursing workforce strengthening outlined by global health organizations.38,39
By actively fostering EI, nurse managers can create more resilient teams, which in turn contributes to improved staff retention, reduced burnout, and the cultivation of a stronger unit safety culture.
Conclusion
This study confirms that trait emotional intelligence is a significant predictor of the self-reported value nurses place on caring behaviors within the high-stress, resource-constrained environment of Palestinian ICUs. These findings pertain strictly to nurses’ perceived importance of caring behaviors as measured by a self-report instrument; they do not constitute evidence of observed caring performance in clinical practice. For nursing management, this is a clear call to action: investing in EI development is a strategic, human-focused tool to build resilient nursing teams capable of delivering compassionate care against formidable odds. The novelty of this study lies in its contextual focus—demonstrating the predictive role of trait EI within the under-researched and highly challenging setting of Palestinian ICUs, thereby extending the existing literature on psychosocial resources in healthcare. The accurate benefit reflected is that EI development offers a practical management strategy to enhance staff resilience and care values in settings where other resources are limited.
Future research should build on these findings by employing experimental or intervention-based designs, such as randomized controlled trials evaluating the impact of EI training programs on both nurse well-being and tangible patient care outcomes. Furthermore, mixed-methods studies are needed to explore the contextual and behavioral mechanisms linking EI to actual caring performance in practice.
Footnotes
Acknowledgements
We sincerely thank all ICU nurses who participated in this study. Your valuable time, dedication, and insights into the emotional and professional challenges of critical care were essential to this research.
Ethical approval
The study was approved by the Institutional Review Board of Palestine Ahliya University (Reference No: CAMS/BSN/6/2025) and conducted in accordance with the principles of the Declaration of Helsinki.
Informed consent
All participants provided written informed consent after being fully informed of the study's objectives, procedures, risks, and benefits. Participation was voluntary, and participants could withdraw at any time without penalty.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.