
Abstract
Background
Recurrent hamstring strain injuries are associated with deficits in eccentric strength and altered muscle-tendon extensibility, which may persist and contribute to reinjury risk.
Objective
To examine the relationship between hamstring flexibility, assessed by Askling H-test, and isokinetic strength ratios; concentric-to-eccentric (Con:Ecc) and hamstring-to-quadriceps (H:Q) in elite soccer players with previous hamstring strain.
Methods
Fifty-two male professional players (27 ± 5 years) with clinically confirmed prior hamstring injury completed the Askling H-test and bilateral isokinetic testing at 60°·s⁻1 (concentric) and 180°·s⁻1 (eccentric). The mean of three maximal efforts was used to calculate peak torques. Pearson correlations and multiple linear regression examined the relationship between flexibility, age, and strength ratios (α = 0.05).
Results
Mean ± SD Con:Ecc ratio was 86 ± 9% and H:Q ratio 63 ± 7%. Hamstring flexibility correlated inversely with the Con:Ecc ratio, moderately in the dominant limb (r = -0.65 [95% CI −0.78 to −0.46], p < 0.001) and weakly in the non-dominant limb (r = –0.34 [95% CI −0.56 to −0.06], p = 0.02). No significant correlation was observed between flexibility and the H:Q ratio (p = 0.38). Flexibility remained an independent predictor of the Con:Ecc ratio after adjusting for age (β = –0.61, p < 0.001; R2 = 0.38).
Conclusions
Reduced hamstring flexibility is associated with a higher Con:Ecc ratio, indicating relatively reduced eccentric capacity, but is not related to H:Q balance. These findings highlight the role of flexibility in hamstring strength balance and warrant longitudinal investigation.
Keywords
Introduction
Hamstring strain is one of the most common non-contact injuries among elite soccer players and often leads to substantial time lost from play. 1 Despite advances in prevention and rehabilitation, recurrence rates remain high; up to 30% within the same competitive season.2,3 The most common risk factors include, but are not limited to, strength deficits, altered muscle activation, and reduced flexibility.4–9 Yet the interaction between these modifiable characteristics after return to sport (RTS) remains insufficiently characterized.
Isokinetic testing is widely used to quantify the muscular performance of the knee flexors and extensors. Two conventional indicators are commonly derived: the hamstring-to-quadriceps (H:Q) ratio, expressing inter-muscle balance, and the concentric-to-eccentric (Con:Ecc) ratio, reflecting the functional relationship within the hamstring itself.6–12 Lower H:Q ratios may reflect insufficient knee-flexor contribution during high-speed deceleration,8–10 while elevated Con:Ecc ratios indicate relatively reduced eccentric hamstring capacity, potentially compromising energy absorption during terminal swing and increasing strain on muscle fibers.13–15 Both metrics provide complementary insights into neuromuscular balance that can guide rehabilitation progression.16,17
Flexibility, particularly reduced hamstring extensibility, has been proposed as a modifiable risk factor for hamstring strain injury and recurrence.10–14 The Askling H-test is a dynamic straight-leg-raise maneuver specifically developed to identify residual hamstring extensibility deficits and functional insecurity following strain injury. 12 Functional insecurity refers to movement-related apprehension, protective motor behavior, or reduced confidence during rapid or high-velocity limb actions that may persist despite clinical resolution of symptoms and return to sport. 12 The Askling H-test demonstrates excellent intra-rater reliability (ICC = 0.94) and a minimal detectable change of 2.3° in elite athletic populations.12,13 Despite these established measurement properties, the extent to which active hamstring flexibility is associated with isokinetic strength characteristics after hamstring injury remains unclear.
Conceptually, restricted hamstring flexibility may increase passive muscle-tendon unit stiffness and amplify inhibitory neural feedback, thereby reducing the muscle's capacity to generate and control eccentric torque during high-velocity movements. 13 Such alterations may disrupt normal neuromuscular coordination and compromise the hamstrings’ ability to absorb energy during rapid lengthening, a critical function during sprinting and terminal swing.14,15 Clarifying these interrelationships may provide important insight into residual functional deficits that persist following hamstring strain injury.
Previous studies have primarily examined flexibility and strength as independent predictors of injury risk, with few investigating their concurrent association or potential confounding by age and limb dominance.18–22 Moreover, the hamstring Con:Ecc ratio has received limited attention compared with the conventional H:Q ratio, despite its direct reflection of intramuscular function. 19 Therefore, the present cross-sectional study aimed to determine the relationship between hamstring flexibility, assessed by the Askling H-test, and isokinetic strength ratios (Con:Ecc and H:Q) in elite soccer players with a history of hamstring strain. We hypothesized that reduced hamstring flexibility would be associated with higher Con:Ecc ratios, indicating a relative imbalance between concentric and eccentric torque, but would show no significant association with the conventional H:Q ratio.
Materials and methods
This cross-sectional study was conducted in the isokinetic laboratory at Alhayah University and Fizik Physical Therapy and Rehabilitation Center between August 13, 2024, and November 7, 2024. The Board Council of Higher Education of the Faculty of Physical Therapy and the Institutional Review Board of Higher Education and Research of Cairo University approved the study (approval number: P.T.REC/012/005295). The study is prospectively registered with ClinicalTrials.gov (NCT06818929) and was conducted in accordance with the Declaration of Helsinki (2013 revision) and conforms to all STROBE guidelines. All players provided written informed consent prior to participation.
Participants
Fifty-two male professional soccer players (mean age: 28 ± 7 years; BMI: 22.98 ± 1.16 kg/m2) competing in the Egyptian Premier League were recruited from multiple soccer clubs via banners and direct contact with the supervising coach. All had sustained a clinically diagnosed grade I-II hamstring strain within the previous 6–18 months and had completed a full return to unrestricted team training and competition. Inclusion criteria were age 18–35 years, participation in ≥ 4 training sessions per week, and absence of pain or injury at testing. Players with prior knee or hip surgery, current lower-limb injury, neurological disease, or hamstring re-injury within 3 months were excluded. Sample size was determined by G*Power (v3.0.10) using a biserial correlation model (α = 0.05, power = 0.80, effect size = 0.38), derived from prior hamstring injury research, 14 and producing a minimum required sample of 47; 10% was added for attrition (final n = 52).
Standardization and familiarization procedures
Testing occurred in a controlled laboratory (temperature 23 ± 1 °C, relative humidity 45 ± 3%) during the mid-season competitive phase to ensure stable performance conditions. All players refrained from fatiguing exercise 48 h before testing. To minimize measurement variability, all testing procedures, including participant instruction, dynamometer setup, anatomical landmark alignment, and data acquisition, were performed by the same senior physical therapist with more than ten years of experience in isokinetic assessment. Chair, dynamometer, and adapter settings followed Computer Sports Medicine Inc. (CSMI) guidelines. 23 Participants completed a standardized warm-up (5-min stationary cycling at ∼60 W) and dynamic stretches for hamstrings and quadriceps, then performed submaximal familiarization trials for both the H-test, followed by the isokinetic testing, before maximal testing.
Askling H-test
Active hamstring flexibility was assessed using the Askling H-test as described in Askling et al. 12 Participants lay supine; the contralateral limb, hip, and trunk were stabilized with straps, and two visual markers were placed on the greater trochanter and lateral malleolus of the tested limb. A knee support (Orthopedic Bracewear Air-X©) was applied to the tested limb to maintain knee extension and prevent flexion during the movement 24
The procedure began with three slow, actively performed hip flexion movements for familiarization, followed by three maximal-velocity active hip flexion trials. Each trial was separated by 30 s of rest to minimize the Cavagna effect, defined as enhanced force output resulting from elastic energy storage during preceding movements. 25 The hip flexion movement was terminated immediately if the player reported a sensation of discomfort, insecurity, or pain. The endpoint was defined as the maximal hip-flexion angle tolerated without compensation. Hip flexion kinematic data were captured using a Canon EOS M50 mirrorless digital camera (60 frames/s⁻1; Canon Inc., Japan) positioned perpendicular to the sagittal plane at hip level and 3 meters from the player. A 1-meter calibration bar was placed parallel to the limb to ensure geometric accuracy for subsequent angle analysis 24 (Figure 1).

Askling H-test setup for assessment of active hamstring flexibility.
Video recordings were analyzed using Kinovea motion-analysis software (version 0.9.5; France). The hip-flexion angle was determined as the intersection between the longitudinal axes of the trunk and thigh at the frame corresponding to end-range elevation. Each limb was tested three times with 30 s rest intervals, and the mean of the three valid trials was used for statistical analysis. The sequence of testing (dominant followed by non-dominant) was counterbalanced between players to control for order effects. The test–retest reliability of the examiner for the current study, based on a pilot sample of ten athletes, showed an intra-class correlation coefficient (ICC = 0.93), confirming measurement consistency. A greater H-test angle represented greater hamstring flexibility, while lower values indicated reduced extensibility or residual stiffness following prior injury. 25
Isokinetic strength testing
Knee flexor and extensor muscle strength was assessed using an isokinetic dynamometer (HUMAC NORM, CSMi, Stoughton, MA, USA) in accordance with established reliability and sports rehabilitation guidelines.6–9,23 Testing took place in a controlled laboratory environment under the same conditions as the Askling H-test to minimize diurnal variation in muscle performance. The HUMAC system was calibrated before each session according to manufacturer specifications. Intra-session coefficients of variation for torque did not exceed 5%, confirming consistent performance.
Participants were then seated on the dynamometer chair with the hip flexed at 85° and the trunk upright. The pelvis, thigh, and torso were stabilized with broad Velcro straps to prevent extraneous movement during contractions. The dynamometer's axis of rotation was precisely aligned with the lateral femoral epicondyle, and the lever arm pad was positioned just proximal to the lateral malleolus to ensure consistent moment arm length across participants. 26 To account for gravitational and inertial artifacts, gravity correction was automatically performed using the HUMAC software's built-in calibration routine before each test. 23 This minimized the torque measurement error to < 2% of recorded values.
Testing was performed bilaterally, beginning with the dominant leg, followed by the non-dominant leg. Participants completed three submaximal familiarization trials to ensure they understood the movement and to eliminate learning effects. After a 1-min seated rest, each participant performed two separate contraction modes:
Concentric contractions of both the quadriceps and hamstrings at an angular velocity of 60°·s⁻1, and Eccentric contractions of the hamstrings at 180°·s⁻1.
Each contraction mode was performed in a separate set, with a 1-min rest period between sets to minimize fatigue and avoid residual force enhancement or depression effects.
26
The movement range was standardized to 90° of knee flexion, with 0° representing full extension. During all test repetitions, participants were instructed to “push and pull as hard and as fast as possible”, and standardized verbal encouragement, along with real-time torque feedback displayed on the HUMAC monitor, was provided to ensure maximal effort. Each testing set included three maximal repetitions, and only the trials performed with a full range of motion and without compensatory movements were accepted. The mean peak torque from the three highest valid repetitions was used for analysis. Peak torque values (Nm) were normalized to body mass (Nm·kg⁻1) to permit inter-subject comparison.
8
The bilateral testing order was counterbalanced between sessions to control for fatigue bias.
(1) the concentric-to-eccentric hamstring ratio (Con:Ecc) = (hamstring-concentric / hamstring-eccentric) × 100%, and (2) the conventional hamstring-to-quadriceps ratio (H:Q) = (hamstring-concentric / quadriceps-concentric) × 100%.
All strength ratios were calculated using peak torque values normalized to body mass (Nm·kg⁻1) and are expressed as percentages (%) to enhance clarity and avoid misinterpretation, while the term “ratio” is retained to denote the proportional relationship between torque measures. 8 Values <100% indicate greater eccentric than concentric torque, consistent with normal physiological muscle behavior, whereas typical hamstring-to-quadriceps (H:Q) ratios in elite soccer players range from 50–70%.8,10,27
Statistical analysis
All analyses were performed using IBM SPSS Statistics (v. 29.0; IBM Corp., Armonk, NY, USA). Data was first checked for completeness, entry accuracy, and outliers via boxplots and standardized z-scores. Normality and homogeneity of variance were assessed using the Shapiro-Wilk and Levene's tests, respectively, supplemented by Q-Q plot inspection. Descriptive statistics are reported as mean ± standard deviation (SD). Between-limb differences in strength ratios and flexibility measures were assessed using paired-sample t-tests. In addition to p-values, we present 95% confidence intervals (CIs) and Cohen's d effect sizes, interpreted as small (0.2–0.49), medium (0.5–0.79), or large (≥ 0.8). 18 Relationships among hamstring flexibility (H-test angle), age, and isokinetic strength ratios (Con:Ecc and H:Q) were examined with Pearson's product-moment correlation coefficients (r), with strength interpreted as small (0.10–0.29), moderate (0.30–0.49), large (0.50–0.69), or very large (≥ 0.70). 17
Variables showing significant univariate associations were entered into separate multiple linear regression models (one for Con:Ecc, one for H:Q), with hamstring flexibility (H-test angle) and age as predictors. Model assumptions (linearity, normality, homoscedasticity) were confirmed via residual plots; multicollinearity was evaluated using variance inflation factors (VIF < 2). Regression results are reported as standardized regression coefficients (β), 95% CIs, coefficients of determination (R2), and p-values. Emphasis is placed on the magnitude and direction of effects alongside statistical significance (α = 0.05).
Results
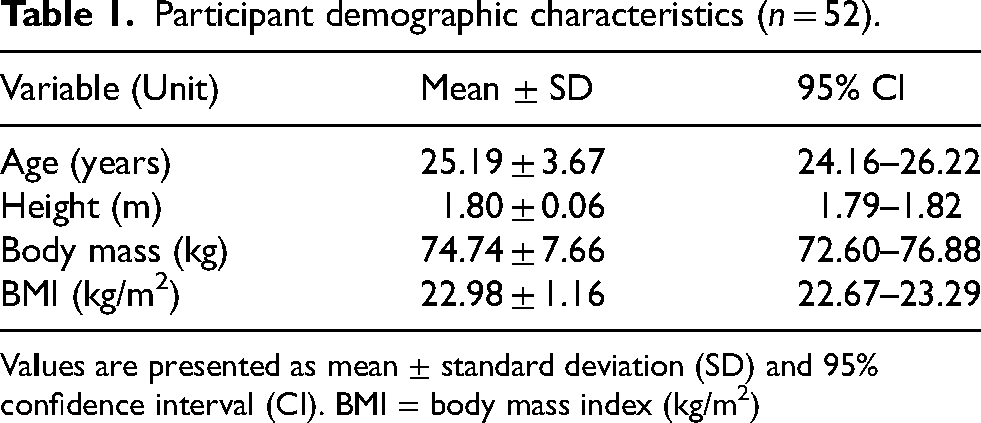
All fifty-two participants completed the full testing protocol without adverse events or missing data. Descriptive characteristics of participants, including age, body mass, and height, are presented in Table 1. The mean age, body mass, height, and BMI values indicate a homogeneous sample representative of professional-level athletic profiles.
Participant demographic characteristics (n = 52).
Va
Positional and leg dominance data
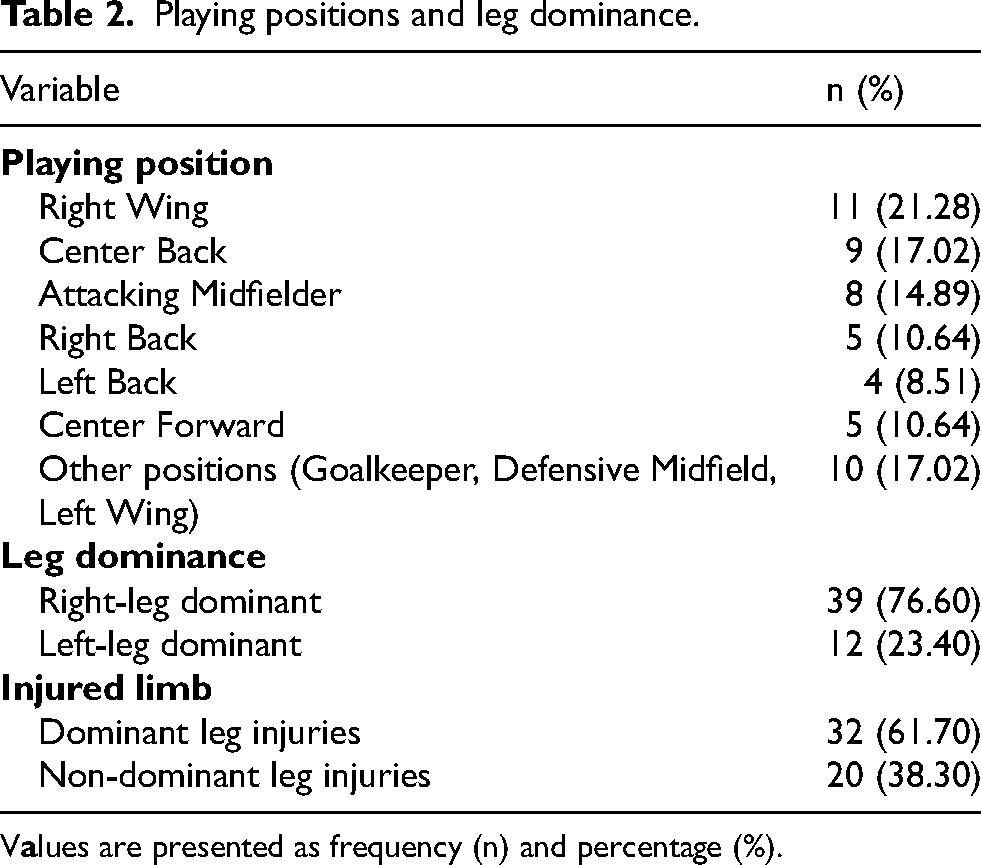
Participants represented a broad range of playing positions (Table 2), with the Right Wing being most common (21.28%), followed by Center Back (17.02%) and Attacking Midfielder (14.89%). Other positions included Right Back (10.64%), Left Back (8.51%), and Center Forward (10.64%). This positional diversity ensured adequate representation of both offensive and defensive player roles. Leg dominance was determined by self-reported preferred kicking leg. A total of 76.60% of players were right-leg dominant, and 61.70% of recorded prior hamstring injuries involved the dominant leg.
Playing positions and leg dominance.
V
Askling H-test hip-flexion angle
Mean Askling H-test hip-flexion angles are presented as descriptive outcomes of active hamstring flexibility. The mean hip-flexion angle was 71.4 ± 6.2° for the dominant limb and 72.1 ± 5.9° for the non-dominant limb, indicating comparable flexibility between limbs.
Normality testing
Normality of all key continuous variables was verified using the Shapiro–Wilk test, supported by visual inspection of histograms and Q-Q plots. Results confirmed that H:Q ratios and Askling H-test scores were normally distributed in both limbs, allowing for parametric analyses. For the H:Q ratio, W = 0.976 (p = 0.433) for the dominant leg (Figure 2(A)) and W = 0.983 (p = 0.739) for the non-dominant leg. For the Askling H-test, W = 0.680 (p = 0.594) for the dominant leg (Figure 2(B)) and W = 0.721 (p = 0.634) for the non-dominant leg. The hamstring Con:Ecc ratios yielded W = 0.351 (p = 0.094) for the dominant leg (Figure 2(C)) and W = 0.218 (p = 0.112) for the non-dominant leg, also indicating no significant deviation from normality. These results confirm that assumptions for subsequent parametric tests were satisfied.
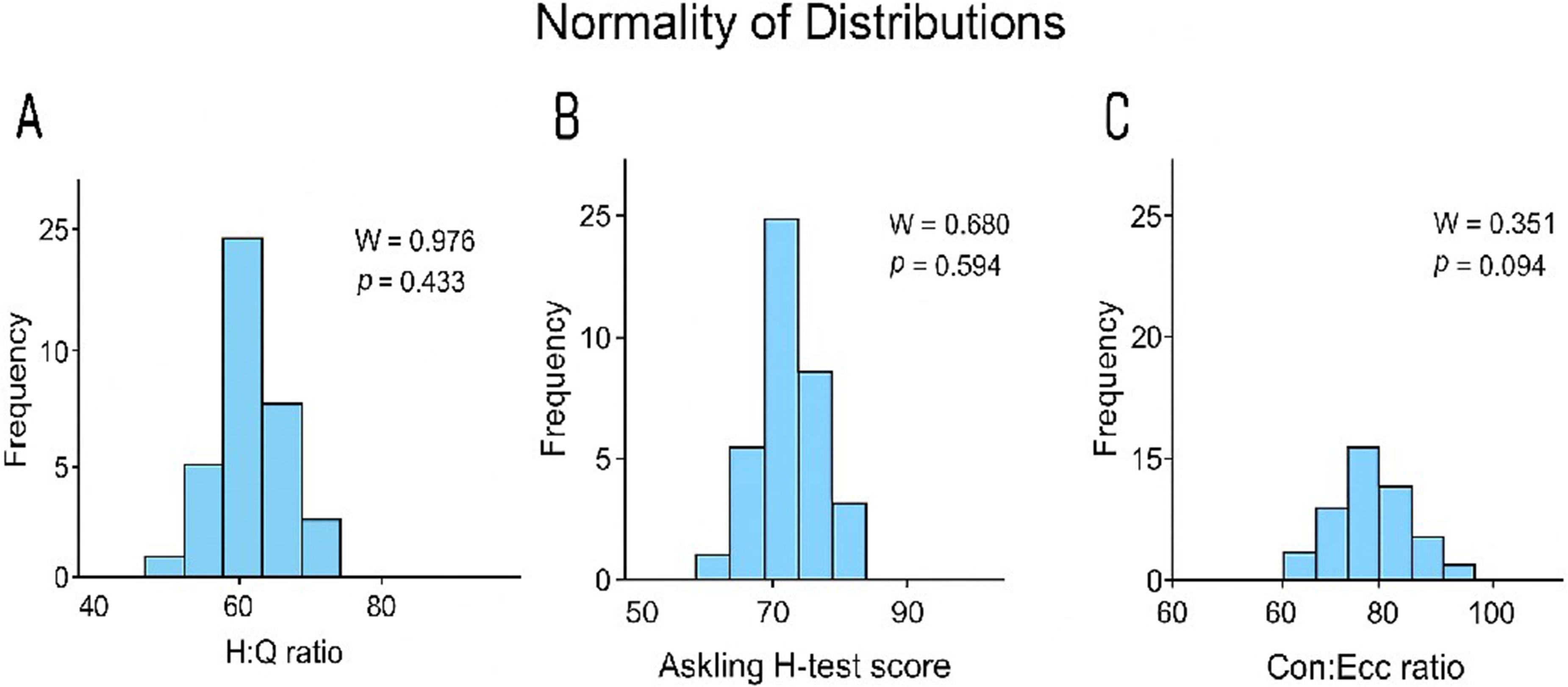
Normality of distributions histograms illustrate the normality of distribution for (A) hamstring-to-quadriceps strength ratio, (B) Askling H-test hip flexion angle, and (C) concentric-to-eccentric hamstring strength ratio (n = 52). Each panel reports the (W) and p-value. All variables approximated a normal distribution (p > 0.05), supporting the use of parametric analyses in subsequent correlations and regressions.
Reliability of isokinetic measurements
Intra-session reliability of isokinetic torque measurements was assessed in a subset of ten participants who completed repeat testing on separate days. Excellent reliability was observed for hamstring strength measures, with an intra-class correlation coefficient (ICC) of 0.96 for concentric torque and 0.95 for eccentric torque. The coefficient of variation for repeated measures did not exceed 4.5%, indicating high measurement consistency across testing sessions.
Isokinetic torque and ratio data
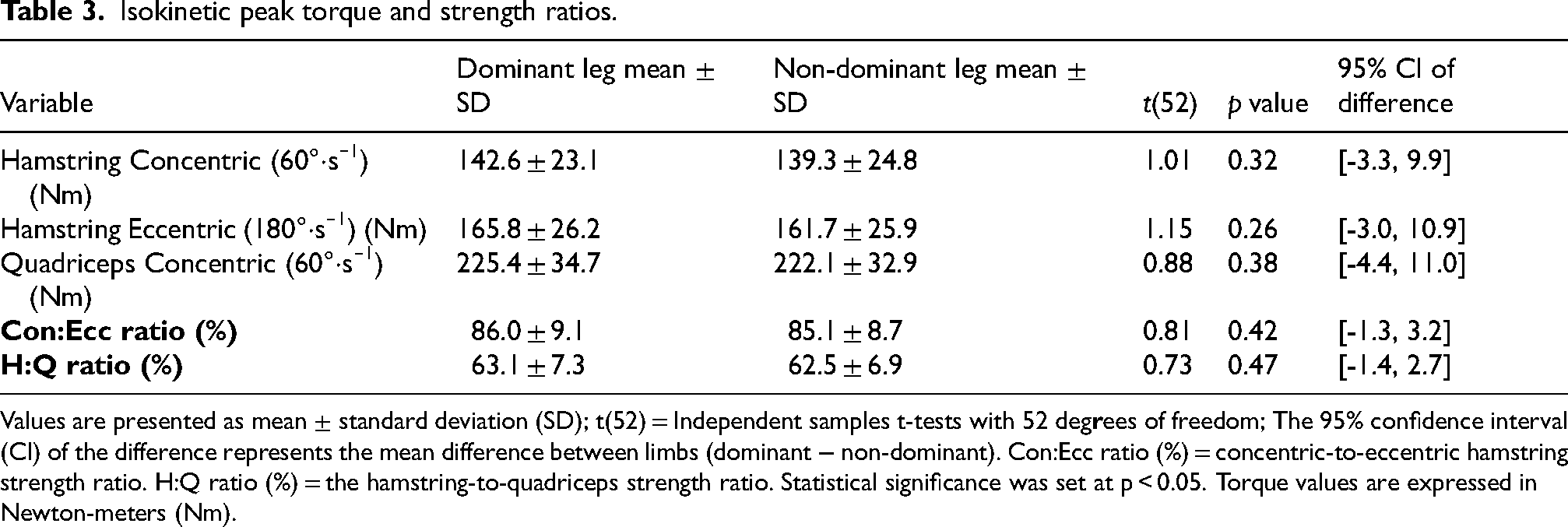
Mean strength torques and ratio data are presented in Table 3. No significant between-limb differences were observed for concentric or eccentric modes (p > 0.05). The mean Con:Ecc ratio was 86.0 ± 9.1% (dominant) and 85.1 ± 8.7% (non-dominant), both below 100%, consistent with expected physiological values. Between-limb differences in either ratios were not significant (p = 0.42 for Con:Ecc; p = 0.47 for H:Q), and the mean asymmetry did not exceed 10%.
Isokinetic peak torque and strength ratios.
Values are presented as mean ± standard deviation (SD); t(52) = Independent samples t-tests with 52 deg
Correlation analysis
Bivariate correlations between Askling H-test scores, age, and isokinetic ratios are summarized in Table 4 and illustrated in Figures 3 and 4. A large inverse correlation was identified between Askling H-test angle and hamstring Con:Ecc ratio for the dominant leg (r = –0.653, 95% CI [–0.78, −0.46], p < 0.001). A moderate negative correlation was observed for the non-dominant leg (r = –0.342, 95% CI [–0.56, −0.06], p = 0.019). Correlation coefficients for the H:Q ratio were weak and not statistically significant for either limb (r = –0.12, p = 0.38 for dominant; r = –0.08, p = 0.47 for non-dominant). No significant association was found between age and any of the strength ratios (r < 0.20, p > 0.05).
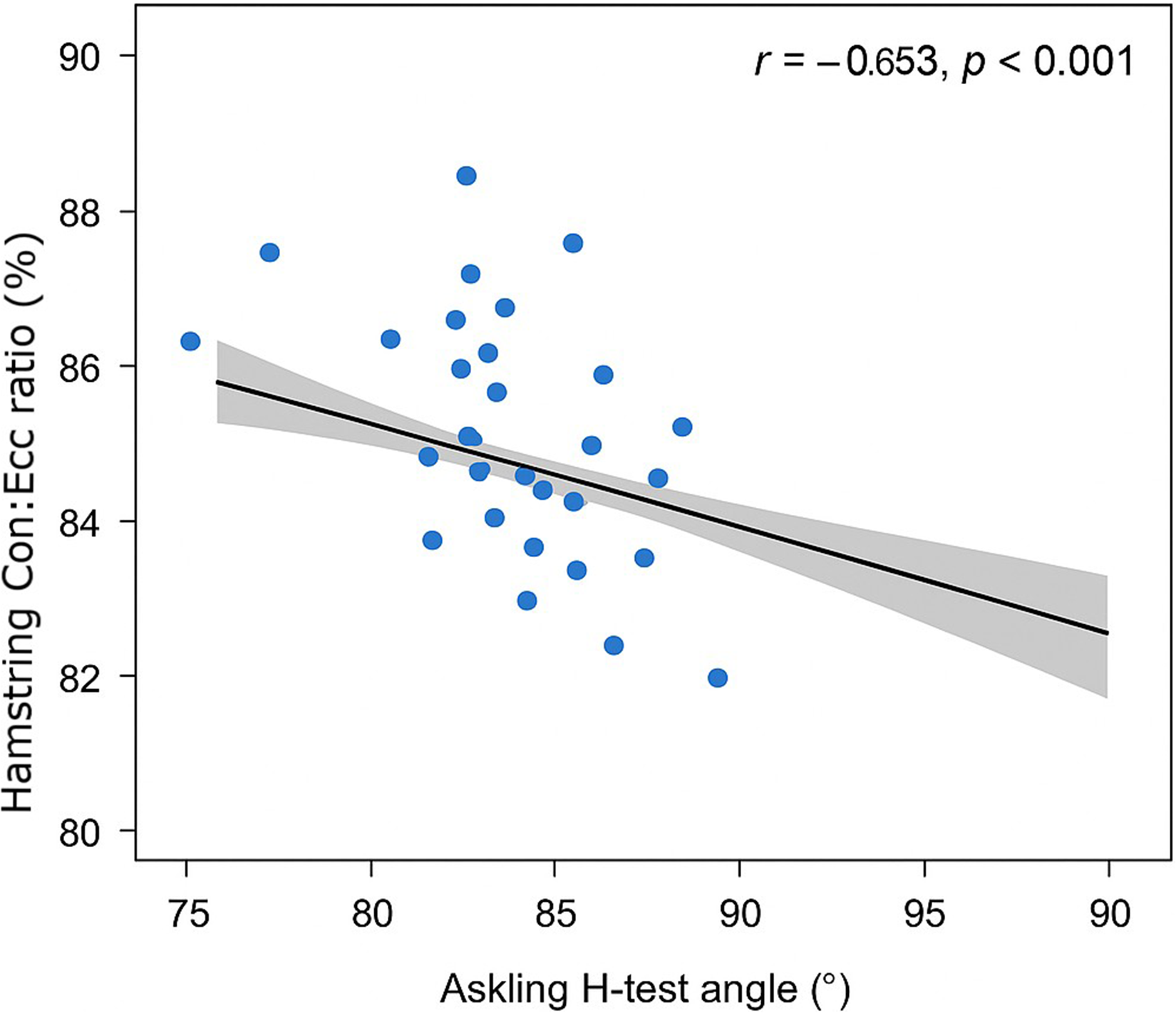
Correlation between askling H-test angle and con:ecc strength ratio scatterplot illustrating the relationship between askling H-test hip flexion angle and hamstring concentric-to-eccentric ratio for the dominant leg. Each point represents one participant (n = 52). A significant negative correlation was observed (r = –0.653, 95% CI −0.78 to −0.46, p < 0.001), with a regression line and 95% confidence band shown.
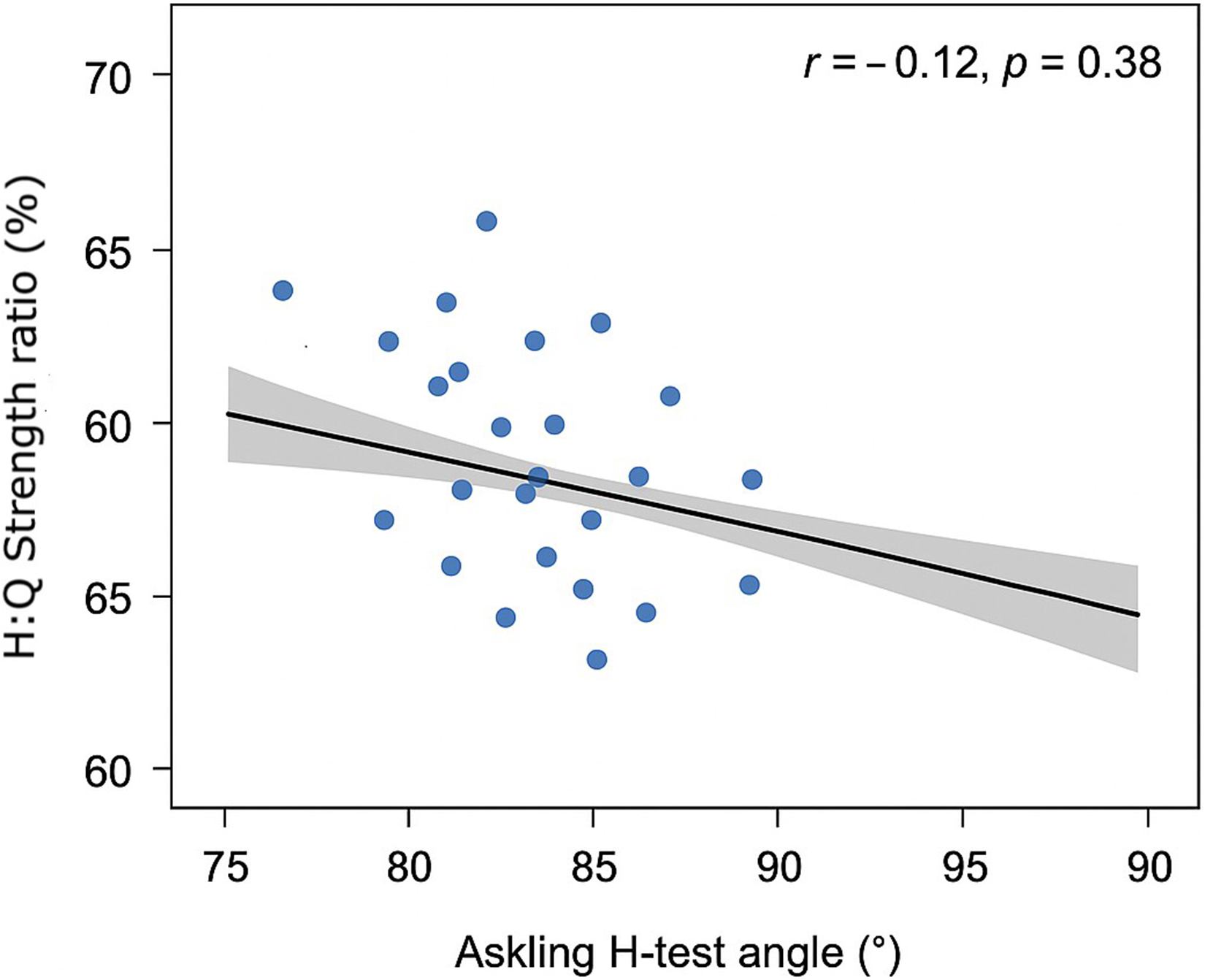
Correlation between askling H-test angle and H:Q strength ratio scatterplot demonstrating the relationship between askling H-test hip flexion angle and the hamstring-to-quadriceps ratio for the dominant leg. A weak and non-significant association was found (r = –0.12, p = 0.38). The regression line and 95% confidence band are displayed for reference.
Correlations between askling H-test, age, and strength ratios.
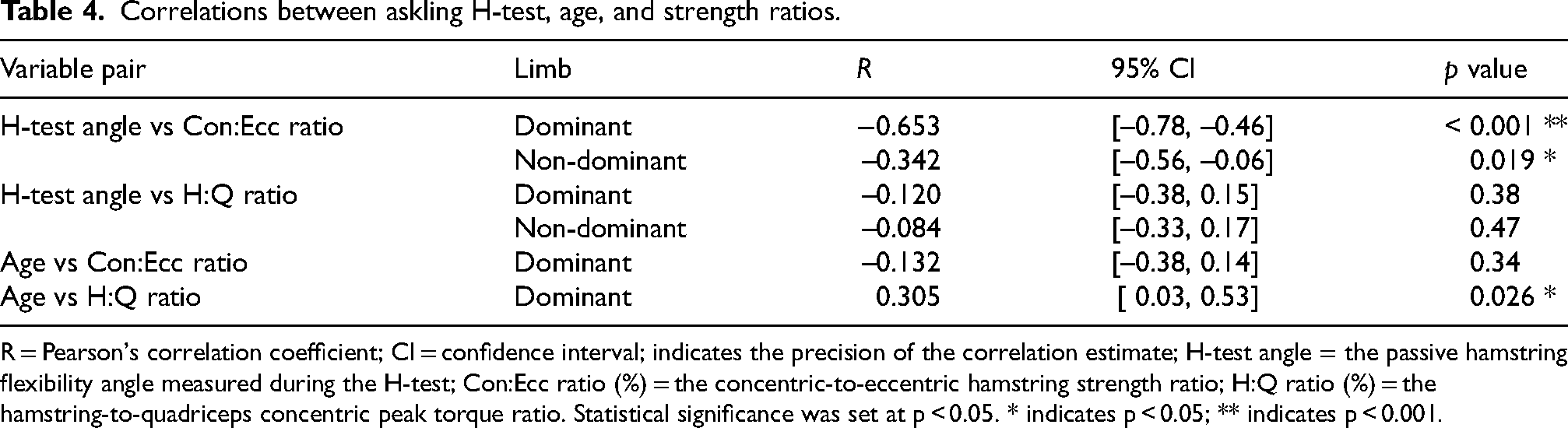
R = Pearson's correlation coefficient; CI = confidence interval; indicates the precision of the correlation estimate; H-test angle = the passive hamstring flexibility angle measured during the H-test; Con:Ecc ratio (%) = the concentric-to-eccentric hamstring strength ratio; H:Q ratio (%) = the hamstring-to-quadriceps concentric peak torque ratio. Statistical significance was set at p < 0.05. * indicates p < 0.05; ** indicates p < 0.001.
Regression analysis
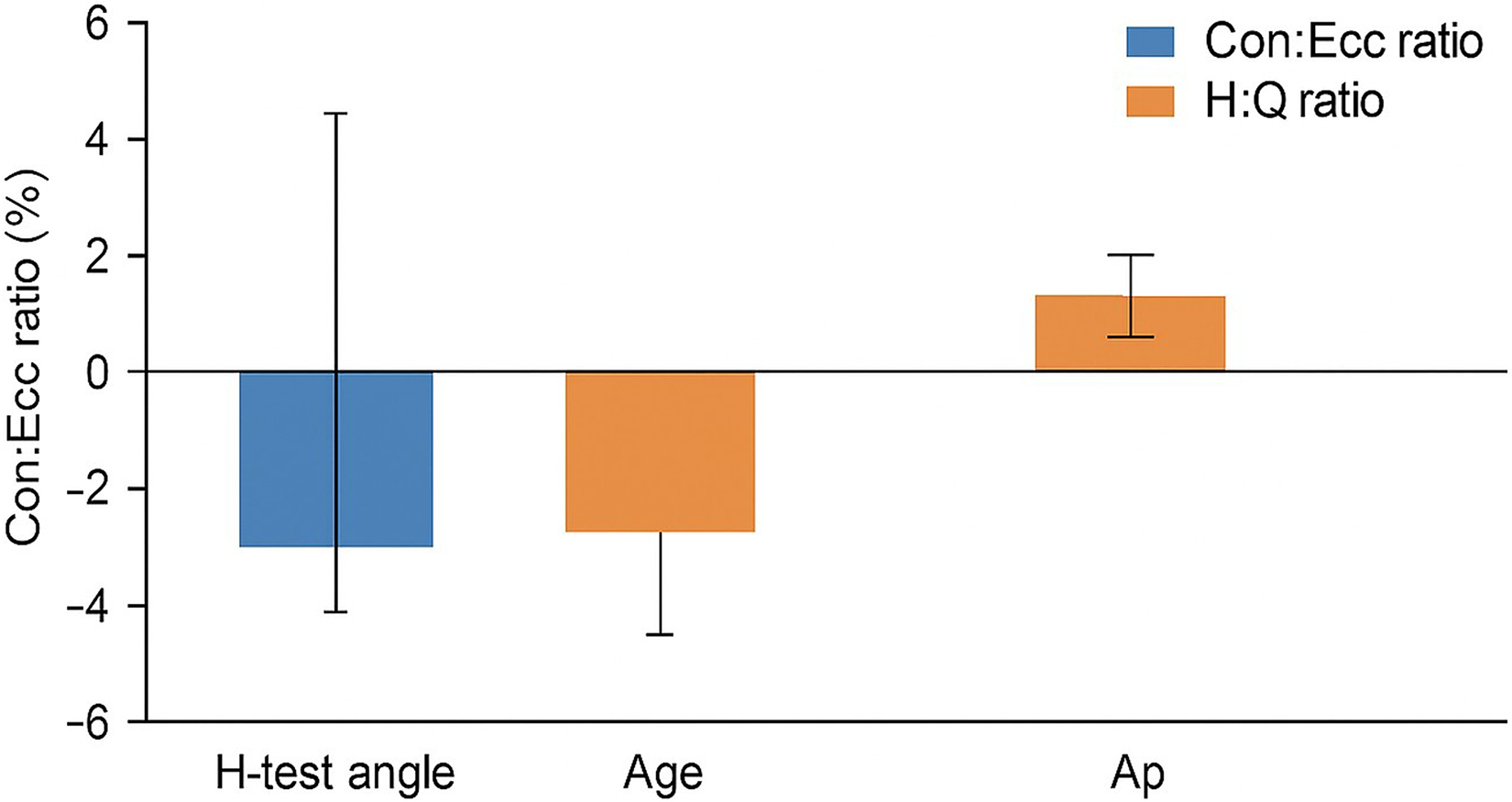
Results of multiple linear regression models are presented in Table 5 and visualized in Figure 5. For the H:Q ratio, age emerged as a significant predictor, explaining 20.1% of the variance in the dominant leg (R2 = 0.201, p = 0.011) and 19.3% in the non-dominant leg (R2 = 0.193, p = 0.014). For the hamstring Con:Ecc ratio, none of the predictors, including age, Askling H-test scores, or their interaction, reached statistical significance (p > 0.05). All regression assumptions were met (normality of residuals, homoscedasticity, VIF < 2).
Multiple regression model summary
Multiple linear regression models predicting strength ratios.
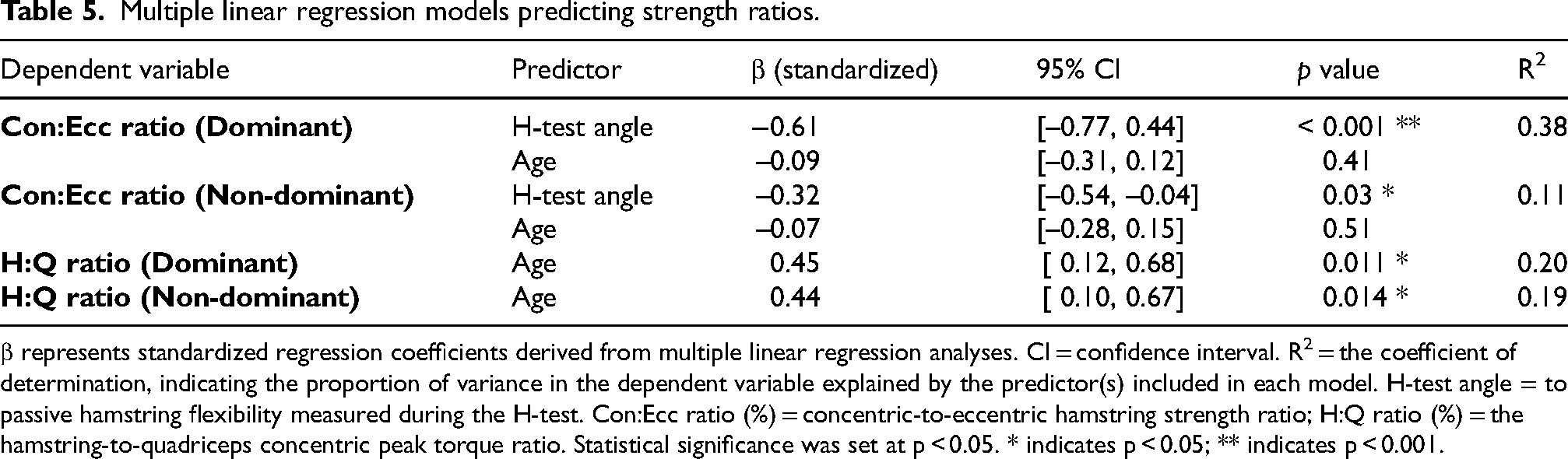
β represents standardized regression coefficients derived from multiple linear regression analyses. CI = confidence interval. R2 = the coefficient of determination, indicating the proportion of variance in the dependent variable explained by the predictor(s) included in each model. H-test angle = to passive hamstring flexibility measured during the H-test. Con:Ecc ratio (%) = concentric-to-eccentric hamstring strength ratio; H:Q ratio (%) = the hamstring-to-quadriceps concentric peak torque ratio. Statistical significance was set at p < 0.05. * indicates p < 0.05; ** indicates p < 0.001.
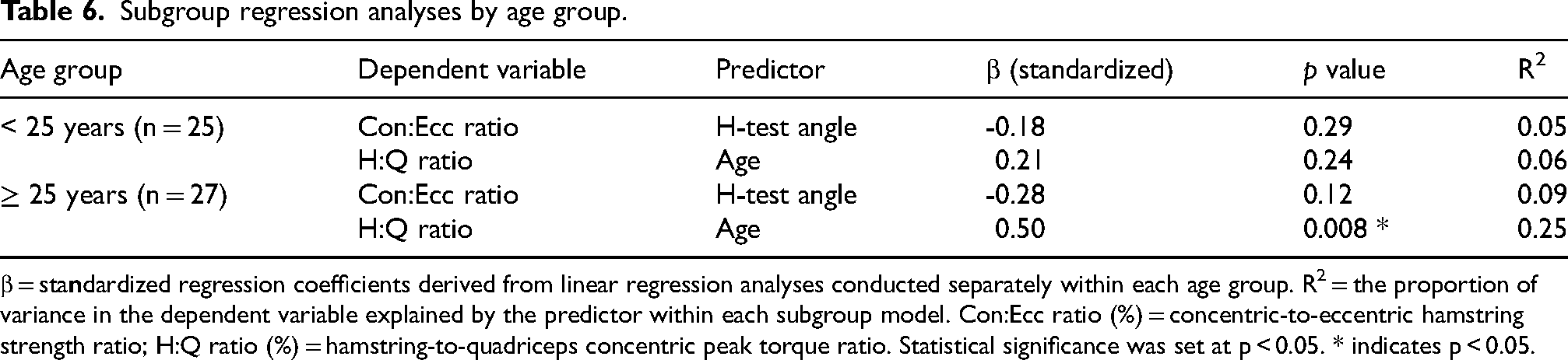
Subgroup analysis
Subgroup analyses compared players aged ≥ 25 years and < 25 years (Table 6). Among players ≥ 25 years, age remained a significant predictor of H:Q ratio (R2 = 0.251, p = 0.008). Among players < 25 years, none of the predictors demonstrated significance (p > 0.05). For the Con:Ecc ratio, no significant predictors were identified in either age group.
Subgroup regression analyses by age group.
β = sta
Discussion
This study integrated two-dimensional (2D) video analysis of the Askling H-test with isokinetic strength ratio assessment in elite soccer players. The primary objective was to examine the relationship between active hamstring flexibility, as measured by the Askling H-test, and isokinetic ratios of Con:Ecc hamstring strength and conventional H:Q strength ratios. The results revealed that hamstring flexibility was significantly and inversely correlated with the Con:Ecc ratio, particularly in the dominant limb, while no meaningful association was observed between flexibility and the H:Q ratio.
Key findings and interpretations
The most relevant finding was the significant inverse correlation between Askling H-test scores and the hamstring Con:Ecc ratio on the dominant side (r = –0.653, p < 0.001) and a moderate one on the non-dominant side (r = –0.342, p = 0.019). These findings indicate that greater hamstring flexibility is associated with a lower Con:Ecc ratio, reflecting a more balanced eccentric control relative to concentric output. A higher Con:Ecc ratio reflects relatively reduced eccentric hamstring strength, a factor that has been implicated in hamstring strain injury risk. 25 These results align with existing literature underscoring the role of eccentric strength in functional performance and hamstring injury prevention.27–29 The stronger correlation observed in the dominant limb can likely be explained by the pronounced right-leg dominance (76.6%) and the higher proportion of injuries in that leg (61.7%). Such findings are consistent with prior work indicating neuromuscular adaptations and asymmetrical loading patterns in the dominant limbs of soccer athletes. 25
In this previously injured cohort, greater hip-flexion angle during the active Askling H-test was associated with a lower Con:Ecc ratio, indicating relatively greater eccentric capacity. While causality cannot be inferred, this pattern may reflect more effective rehabilitation adaptation and potentially reduced susceptibility to reinjury.
Contrary to initial expectations, no significant correlation was observed between the Askling H-test and H:Q ratios. This suggests that H:Q ratios, reflecting overall knee flexor-extensor balance, may not adequately capture the dynamic flexibility characteristics assessed by the H-test. 29 This finding reinforces the view that these two measures represent distinct facets of muscle performance. Traditional H:Q ratios, which are typically measured under isolated concentric conditions, have shown limited predictive value for hamstring injury risk in elite players.28,29 Functional H:Q ratios that incorporate eccentric loading appear to better represent performance-relevant muscle balance and injury resilience. 30
Age emerged as a significant predictor of H:Q ratios, explaining approximately 20% of the variance in both limbs (dominant: p = 0.045; non-dominant: p = 0.028). In subgroup analyses, this relationship was more pronounced among players aged ≥25 years, where age accounted for 25.1% and 20.8% of the variance for the dominant and non-dominant limbs, respectively. These results align with prior studies identifying age as a critical factor influencing muscle balance and injury susceptibility.1,4,9,14,16,30 Age-related declines in neuromuscular coordination, reduced tendon elasticity, and sarcopenic changes in type II muscle fibers may contribute to altered H:Q ratios.16,31 Interestingly, the Con:Ecc ratio did not vary significantly with age, possibly reflecting the preservation of eccentric strength capacity through consistent exposure to high-load eccentric demands in soccer. This observation corresponds with reports that eccentric training can mitigate age-related declines in hamstring performance.14,16,30,32
Bilateral differences and dominance effects
Bilateral asymmetries were evident in both strength ratios and flexibility. The dominant limb demonstrated slightly higher Con:Ecc (86.0 ± 9.1%) and H:Q (63.1 ± 7.3%) ratios compared to the non-dominant side (85.1 ± 8.7% and 62.5 ± 6.9%, respectively). Although these differences did not exceed the 10% asymmetry threshold commonly cited as a risk criterion for lower-limb injury, 33 the trend toward dominance-related variation aligns with known sport-specific neuromuscular adaptations. 34 Such adaptations are likely the result of repetitive unilateral actions (e.g., kicking, cutting, and pivoting), which impose asymmetrical eccentric loading on the hamstrings. These differences may influence motor control strategies and contribute to differential fatigue or injury patterns between limbs. 34
Flexibility measurement: active vs. Passive
The association between active flexibility and the Con:Ecc ratio supports the inclusion of dynamic flexibility measures such as the Askling H-test within musculoskeletal screening and injury prevention frameworks. This relationship underscores the relevance of assessing flexibility under active, sport-specific conditions, as dynamic flexibility may more accurately reflect functional muscle and tendon behavior during high-speed tasks. 32 However, prior studies have also emphasized the role of passive flexibility assessments, such as the straight leg raise or passive knee extension tests, in identifying athletes at elevated risk of hamstring strain.34–36 These inconsistencies suggest that active and passive measures assess different physiological components of the muscle-tendon unit, such as neural control versus passive tissue extensibility. Consequently, the choice of flexibility test should align with the assessment purpose: active flexibility for RTS evaluation, and passive measures for general injury screening.
Limitations and future directions
This study has several limitations that must be considered when interpreting the results. Isokinetic testing occurs under controlled conditions that may not fully replicate the multi-planar and high-velocity demands of soccer-specific movements. The cross-sectional design precludes establishing causal relationships between flexibility, strength ratios, and injury risk. Furthermore, potential confounding effects from training load, seasonal phase, and prior rehabilitation exposure could not be fully controlled. Future longitudinal research incorporating electromyographic and 3D kinematic analyses is recommended to clarify causal mechanisms linking dynamic flexibility, strength balance, reinjury risk, and recovery outcomes.
Conclusion
This study demonstrated a significant inverse association between active hamstring flexibility, assessed via the Askling H-test, and the Con:Ecc strength ratio among elite soccer players, particularly in the dominant limb. In contrast, flexibility showed no meaningful relationship with the conventional H:Q ratio, suggesting that these indices capture distinct aspects of neuromuscular performance. Age emerged as an independent determinant of H:Q ratios, explaining up to one-quarter of their variance in older players, whereas Con:Ecc ratios appeared less influenced by age. Although limb asymmetries were present, they did not exceed the recognized 10% risk threshold. The study's cross-sectional design precludes causal inference.
Clinical implications
Incorporating dynamic flexibility measures such as the Askling H-test alongside eccentric strength testing provides a more comprehensive assessment of hamstring performance than traditional H:Q ratios alone.
Targeted eccentric strengthening should be emphasized, particularly in athletes aged ≥25 years, as older players demonstrated less favorable H:Q ratios, underscoring the need for age-specific strength monitoring and individualized rehabilitation strategies.
Routine bilateral monitoring of Con:Ecc and H:Q ratios can identify meaningful asymmetries and guide individualized training or rehabilitation plans.
Combining active and passive flexibility tests may enhance screening accuracy for injury prevention and readiness-to-play evaluations.
Footnotes
List of Abbreviations
Acknowledgements
“No acknowledgements are declared in this study.”
Ethics approval and consent to participate
“Ethical approval was granted by the Institutional Review Board of Cairo University's Faculty of Physical Therapy (Approval No.:P.T.REC/012/005295). All participants provided written informed consent prior to inclusion. The study adhered to the Declaration of Helsinki and was prospectively registered on ClinicalTrials.gov (NCT06818929). Participants were informed of their right to withdraw at any stage.”
Consent for publication
“Informed consent obtained from participants included permission to publish anonymized data. No identifiable personal information appears in this manuscript.”
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
“The datasets generated and analyzed during this study are included in the supplementary materials accompanying this manuscript and are available upon request. ”