
Abstract
While parents are often expected to advocate for their children with disabilities throughout their lifespans, little is known about the beginning advocacy experiences for parents of young children with disabilities. The purpose of this study was to examine the advocacy experiences of caregivers of children with disabilities during early intervention. Altogether, 24 caregivers of children with disabilities participated in individual interviews about their lived experiences with advocacy in early intervention. Findings revealed that participants often engaged in advocacy during early intervention. Some advocacy strategies were similar to advocacy for school services (e.g., learning one’s rights). In addition, some strategies included using effective communication strategies and being assertive and persistent. Implications for research and practice are discussed.
Advocacy can be defined as speaking or acting on behalf of one’s self, another individual, or a group of people to address their needs, preferences, and strengths (Wolfensberger, 1977). Parents of children with disabilities are often expected to advocate for their offspring from the time of diagnosis through adulthood (Burke, 2012). Advocacy can occur before or in response to challenging situations. In the context of an empowerment framework, when parents actively advocate in response to an identified need or potential or actual challenging situation (e.g., navigating service delivery systems), there are improved outcomes (e.g., the child receives appropriate services; Jones & Prinz, 2005).
While parent advocacy typically occurs throughout the lifespan, less than a handful of studies have examined advocacy during early intervention (EI, Schraml-Block & Ostrosky, 2022; Wright & Taylor, 2014). The dearth of research about advocacy among parents and caregivers of children receiving EI services is problematic given the potential for strong effects of advocacy such as increased access to appropriate diagnoses and needed services for their children with disabilities (Taylor et al., 2019; Wright & Taylor, 2014). Thus, the purpose of this study was to explore the advocacy experiences of families of children with disabilities during EI.
Reasons for Parent Advocacy
Understanding the context for parent advocacy during EI is essential. At a systemic level, parent advocacy has been instrumental. Parent advocacy facilitated the inclusion of EI in the Individuals with Disabilities Education Act (IDEA) in its 1986 reauthorization (Schraml-Block & Ostrosky, 2022). At an individual level, it is important to understand the reasons for parent advocacy during EI. A key tenet of EI is family-centeredness (Dunst, 2002). Thus, a goal of EI is to enhance caregivers’ capacity to become effective advocates for their young children by increasing their knowledge about their rights, the services they are entitled to receive, and what to do if they are not accessing the services they need (Wright & Taylor, 2014). However, advocacy can also be a stressor for parents (Ryan & Quinlan, 2018; Wright & Taylor, 2014) and by identifying the reasons for advocacy, circumstances can be targeted to reduce overreliance on parent advocacy for meeting the needs of their young children with disabilities.
Advocacy Strategies
It is also important to characterize the advocacy strategies used by families during EI. To advocate effectively, parents need to gain knowledge about the systems of care available for their children and about their child’s disability and their needs (Burke et al., 2016). In addition, they may need additional resources such as time, interest, social support, and the capacity to assume the role of an advocate (Wright & Taylor, 2014). In the context of school services, Trainor (2010) identified four types of parent advocacy strategies: strategist (e.g., using knowledge of special education law to access services), intuitive (e.g., relying on one’s gut instinct), disability expert (e.g., relying on knowledge about the child’s type of disability), and agent of systemic change (e.g., spearheading legislative change). However, her study did not include parents of children in EI. Unlike school services, EI services focus on the child and the family. In addition, advocacy may look different during the EI period due to several reasons, for example, parents may be new to parenthood, and/or having a child with a disability. To that end, parents may have not developed a network or know how to access resources.
Facilitators and Barriers to Advocacy
Furthermore, it is critical to identify facilitators and barriers to advocacy during EI. Similar to school services, there is jargon and bureaucracy in EI (Williams et al., 2013). Parents often report that terminology and paperwork are barriers in advocacy (Burke et al., 2019). Barriers to advocacy may also include limited knowledge about education and legal rights (MacLeod et al., 2017). Identifying barriers to advocacy is a first step to discern, develop, and implement ways to ameliorate barriers.
In contrast to barriers and in alignment with an empowerment framework, a facilitator to advocacy may be empowerment. When parents are empowered, they are significantly more likely to advocate (Ashcraft et al., 2019). Social capital has also been identified as a potential facilitator of advocacy (Trainor, 2010). Social capital is comprised by the social networks and relationships developed by parents (Trainor, 2010). Social capital may be developed by parents strengthening their social networks as well as through participation in parent support groups or other organizations that provide opportunities to parents to build relationships and share advocacy strategies (Burke et al., 2016). Finally, given the family-centeredness in EI, researchers have suggested that professionals—such as service coordinators—may facilitate parent advocacy (Bailey et al., 2012; Thompson et al., 1997). By identifying facilitators to advocacy, interventions can be developed to capitalize on facilitators.
Outcomes of Advocacy
Finally, the outcomes of parent advocacy during EI need to be understood. Although limited to school and adult disability services, prior research has suggested that parent advocacy can yield effects on children with disabilities and their families. Regarding the former, advocacy may enable children with disabilities to access appropriate services (Burke et al., 2019; J. L.Taylor et al., 2017). However, there may be more mixed outcomes of advocacy for families. On a positive note, some families report that advocacy improved their coping strategies (Ewles et al., 2014). In contrast, families also report that advocacy can take time away from other family activities as well as increase stress and anxiety (Ryan & Quinlan, 2018). Advocacy may also increase maternal stress (Burke & Hodapp, 2014) and reduce family quality of life (Wang et al., 2004). Understanding the outcomes of advocacy during EI is instrumental to determine whether advocacy has unintended outcomes.
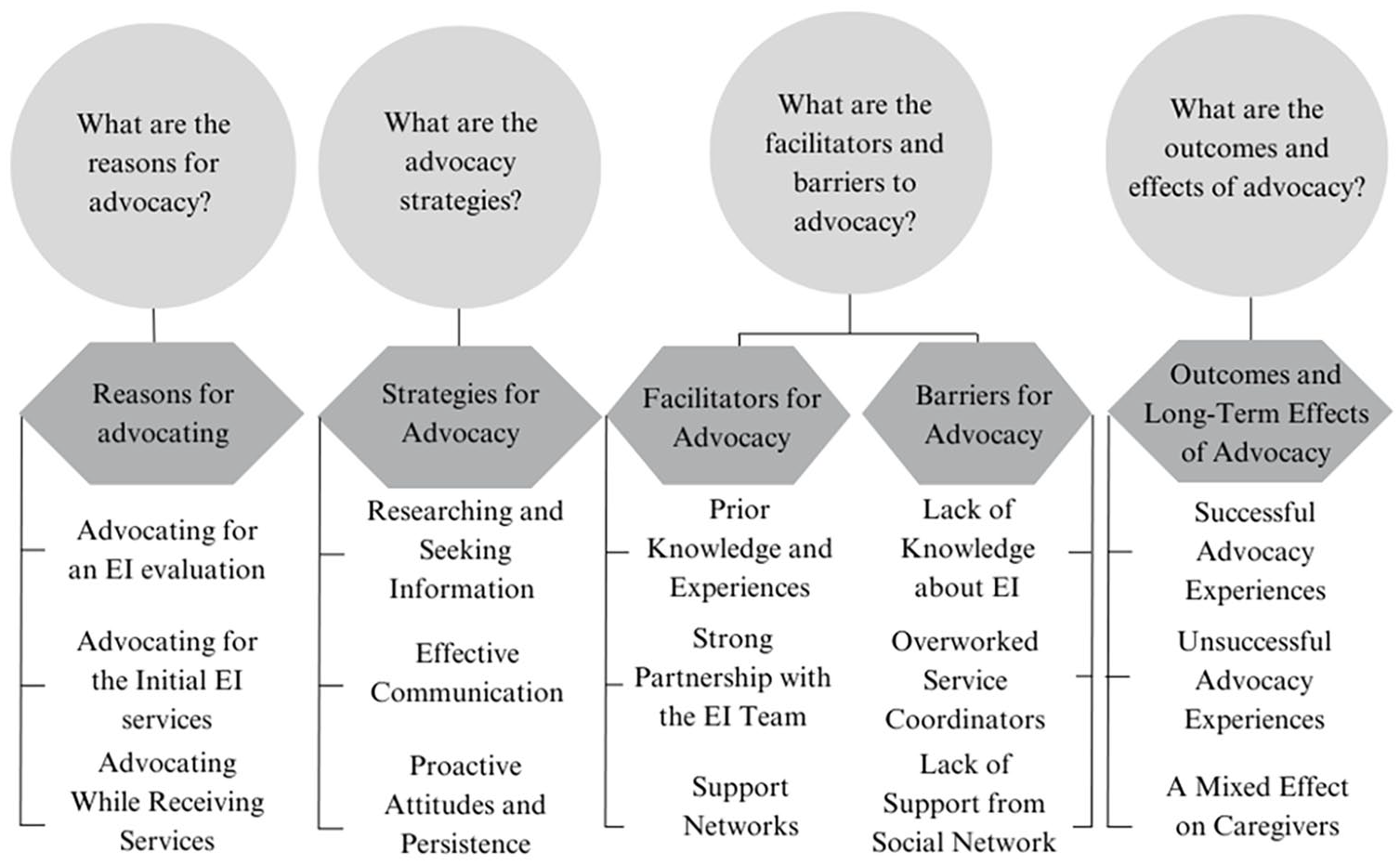
Altogether, there is a need to understand parent advocacy during EI to best support families. Indeed, one of the desired family outcomes of EI is to “know one’s rights and advocate for one’s child” (Bailey et al., 2012). Yet, there is little research exploring advocacy during EI (Schraml-Block & Ostrosky, 2022). To this end, using an empowerment framework, there were four research questions for this study: Among caregivers of children with disabilities during EI, (1) What are the reasons for advocacy? (2) What are the advocacy strategies? (3) What are the facilitators and barriers to advocacy? and (4) What are the outcomes of advocacy?
Method
Design
In this study, a qualitative approach was chosen to explore the advocacy experiences of caregivers (primarily parents) of children with disabilities in EI. Considering the limited research on advocacy during EI (e.g., Schraml-Block & Ostrosky, 2022), an interview design was employed.
Participants
A total of 24 participants were included in this study. Inclusion criteria required participants to be a primary caregiver of a child who currently or recently (within the past 6 years) received EI services, interested in attending an EI leadership program, and residing in a specific Midwestern state. The 6-year window ensured that participants’ recollections of EI services were relatively recent. Participants were a subsample from a broader study focused on the effects of leadership training for caregivers of young children (ages 0–8) with disabilities, specifically in advocacy during early childhood.
Of the 24 participants, 16.67% (n = 4) came from under-represented racial and ethnic backgrounds. The majority were female (95.83%, n = 23) and most had completed college or graduate school (95.83%, n = 23). The single male participant was married to a female participant in the study. Most participants were parents (95.83%, n = 23), with one grandmother included. The average age of participants was 37.7 years of age (SD = 5.66 years, range: 28–58). The average age of the participants’ children was 3.39 years old (SD = 1.95, range: 1–9). See Table 1 for detailed demographic information.
Demographic Characteristics.

Note. All participant names are pseudonyms. CP = cerebral palsy; DD = developmental delay; EBD = Emotional/Behavioral Disorder; HC = health condition; HI = hearing impairment; ID = intellectual disability; LD = learning disability; NR = not reported VI = visual impairment; SLI = speech/language impairment. All child disabilities were caregiver reported and no verification was done by the members of the research team.
Participants were parents of the same child. b Caregiver was a grandmother.
Procedures
Institutional Review Board approval was obtained prior to participant recruitment, which involved several strategies. Recruitment flyers were distributed to EI professionals, parent groups, and disability agencies via email and social media. Participants received a $25 gift card for their interview participation. Convenience sampling was used, with specific efforts to recruit a racially and ethnically diverse sample. Recruitment materials were reviewed by community-based disability and family organizations for cultural responsiveness and distributed to organizations serving families of color in the state.
Interested participants completed screening questions, via RedCap, to determine eligibility. Eligible participants were directed to the online consent form, followed by a demographic questionnaire and scheduling of the interview. A total of 22 individual interviews and one joint interview with two parents of the same child were conducted via Zoom. The interviews, conducted by five researchers with experience in qualitative research and disability, lasted an average of 30 min. Fidelity to the interview protocol was maintained at 100%, ensuring all interview questions were asked. Interviews were recorded and transcribed verbatim for analysis.
Measures
Demographic Questionnaire
The demographic questionnaire asked questions about the parent (e.g., educational background, race, ethnicity) and child who receive(s/d) EI services (e.g., type of disability, current age).
Interview Protocol
The interview protocol was developed in alignment with an empowerment framework and based on extant literature about advocacy during EI (Burke et al., 2020; Schraml-Block & Ostrosky, 2022) and advocacy more broadly (e.g., S.Taylor et al., 2019; Trainor, 2010). Prior to the study, the protocol was piloted with a parent whose child received EI services. Based on the pilot, minor changes were made to the protocol. For example, the parent suggested that the protocol include a question about the amount of time their advocacy efforts took during EI. We asked participants to share an advocacy experience in which they were successful in obtaining their desired outcomes, and an advocacy experience in which they were unsuccessful in obtaining their desired outcomes.
Analysis
We read the transcripts multiple times to familiarize ourselves with the data (Tesch, 1990). Then, we used emergent design (Patton, 2002) to code the transcripts. Emergent design seeks to understand a phenomenon or topic allowing the research design and methods to evolve or emerge based on ongoing data collection and analysis (Patton, 2002). Given the limited extant literature about advocacy during EI, an inductive data analysis strategy was appropriate. There were no a priori codes. Using Microsoft Word, we imported the interview transcripts and added continuous line numbering. Then, using a line-by-line approach, we individually coded all text related to the research questions. First, we randomly selected five transcripts and independently coded the five transcripts by comparing each piece of data with other data and annotating each piece of data with a specific phrase (Creswell, 2003). We then compared each new piece of data with previously coded data to check whether the new data reflected a new idea or an existing code. Then, all authors met to compare codes and resolve differences. Based on our discussion, we created a preliminary codebook. We (two researchers) used the preliminary codebook to independently code five additional randomly selected interviews. We met to discuss whether new codes should be added to the codebook. We used the revised codebook to independently code the remainder of the interviews. We grouped the codes into subthemes and organized the subthemes into themes grounded in the data. After each time we independently coded the data, we met to discuss the coding process and resolve differences until consensus was reached (Saldaña, 2021). For example, the codes diligent, proactive, and persistence were grouped into the Proactive Attitudes and Persistence subtheme, which was then included in the theme Strategies for Advocacy.
Trustworthiness
We made several efforts to ensure the credibility and trustworthiness of the data collection and analysis. For example, we conducted a first-level member check at the end of each interview (i.e., we briefly summarized the interview and asked if the participant had anything to add or change). By conducting member checking, participants could assess the validity of the findings (Guba & Lincoln, 1989). After completing the data analysis, we created a summary of the findings which included the final themes, subthemes, and sample quotes for each category. We conducted a second-level member check of the analyzed data with each participant to validate our findings by seeking confirming or disconfirming evidence, and providing participants with the opportunity to reflect and add data (Birt et al., 2016). Only seven participants responded to the second-level member check. For example, Taylor commented “I’ve read through the findings, and I think it does a good job showing a balance of perspectives and experiences.” Similarly, Hellen commented, “That’s a lot of wonderful insight and info. Thanks for capturing that.” In addition to the member checks, all four authors participated in weekly peer debriefing meetings. During these meetings, we discussed data collection and analysis (Brantlinger et al., 2005). We replaced names with pseudonyms.
Positionality and Reflexivity
We acknowledge the importance of reflecting in our positionality, and how our previous experiences and background may affect our selection of research topics, methodology, and data analysis (Glesne, 2016; Shaw et al., 2020). Our research team was comprised of four researchers, three doctoral students and one faculty member. In addition, two researchers, a doctoral student, and a postdoctoral research associate in special education assisted the research team in conducting interviews but did not participate in data analysis. All researchers had experience as practitioners and one is also a parent of a child who received EI services. Each of us had extensive experience working with young children with disabilities. Each interviewer briefly disclosed their positionality to the participant at the beginning of the interview. Our familiarity with the experiences of children in EI was a strength in conducting this study and analyzing the data. However, each of us also brought our own lived experiences and perceptions to the study. For example, each of us believed that caregivers advocated for EI services and that advocacy would likely yield positive effects. To address our potential biases, we each recorded field notes that included our thoughts and reflections after conducting the interview, and during the data analysis process. We also engaged in peer debriefing to identify and mitigate our biases (Saldaña, 2021).
Findings
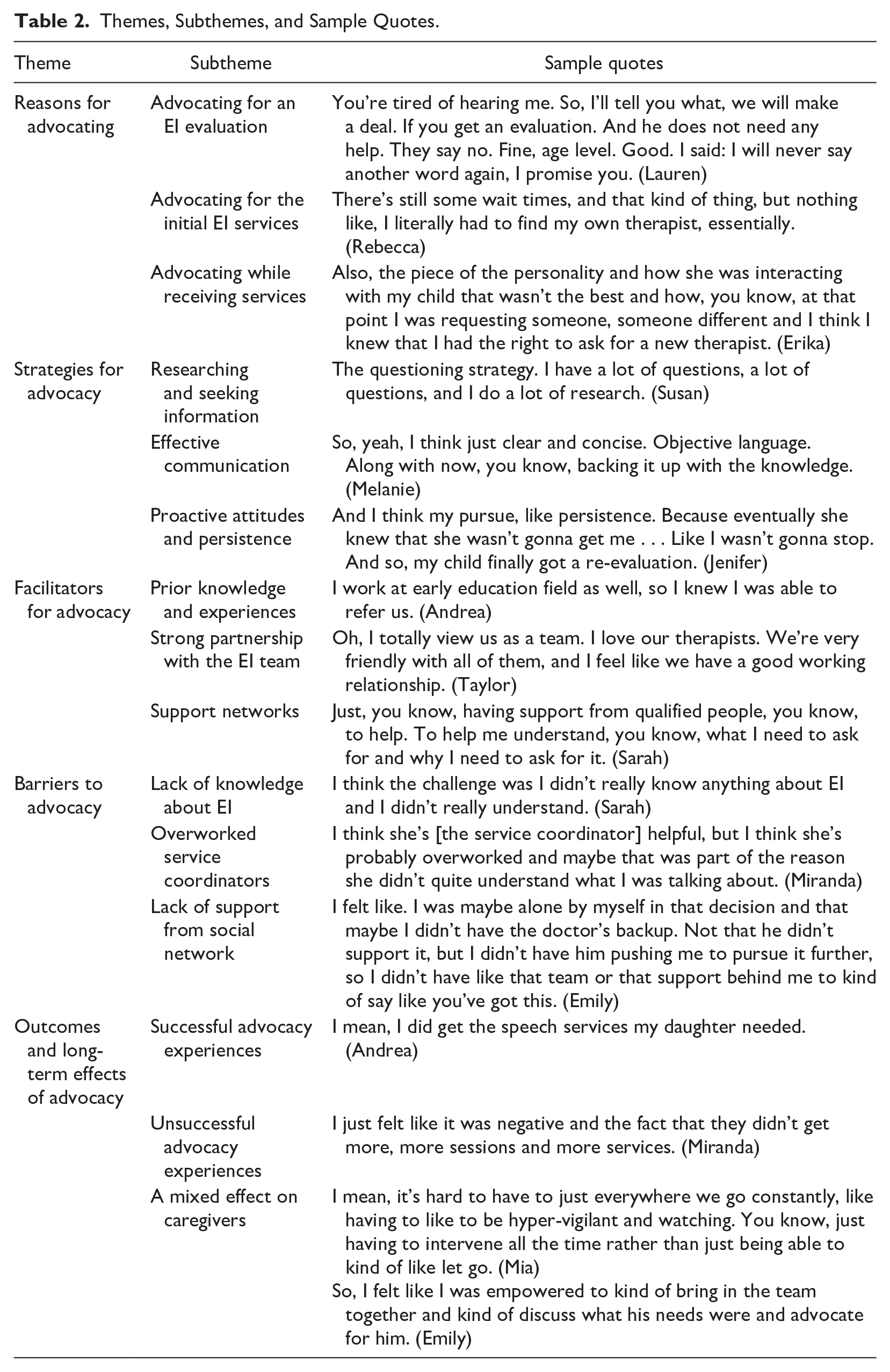
Through thematic analysis (Saldaña, 2021) and guided by our research questions, we identified five themes. See Figure 1 for an illustration of how themes and subthemes relate to the research questions. See Table 2 for additional quotes on the themes and subthemes.
Research Questions, Themes, and Subthemes.
Themes, Subthemes, and Sample Quotes.
Reasons for Advocating
Advocating for an EI Evaluation: “. . . and Then We Did the EI Evaluation”
Some participants shared that their advocacy began with advocating to access EI evaluations. For example, some participants reported advocating for referrals from a health care provider to EI or for an EI evaluation. To that end, some participants began advocating at their pediatricians’ offices. Stephanie, the mother of a 3-year-old boy with a developmental delay, shared her advocacy with her pediatrician at her son’s 2-year pediatrician appointment:
I said to his pediatrician, “You know, he’s, I believe he has a speech delay. His vocabulary is not where it should be.” And she was like, “Oh, he’s fine.” And I was like, “No, I really would like him to be evaluated.” And she was, you know, it took a couple of minutes back and forth and she was like, “Okay, if you really believe that, well, you know, here’s a referral.”
Makena, the parent of a 5-year-old son with a developmental delay, reported that she advocated for an evaluation only to be dismissed by her pediatrician. In response to her advocacy, the pediatrician stated, “let’s wait.” Makena reported she had to insist for a referral: “I was advocating, advocating, advocating for him, like all the way.”
Some participants reported advocating for an evaluation with the EI system. Jenna, the mother of a 2-year-old with multiple disabilities, recalled advocating for an EI evaluation before her son was born. Jenna’s older son was already receiving EI services. During a meeting for her older son, she began advocating for her unborn child:
I mentioned to her [service coordinator] that “Hey, I just got this diagnosis. I know he’s gonna need early intervention. I would like to know like how do I get him started?” Day one, you know, not like day one, but like when he’s home.
Lauren, the grandmother of a boy with a developmental delay also advocated for an EI evaluation. She reported, “I was pushing, you know, evaluation, evaluation, evaluation. Finally, they agreed to their evaluation. And he was diagnosed, and you know a diagnosis then, it opens the doors.” Hellen, a mother of a 4-year-old boy with a learning disability and speech/language impairment, shared her advocacy for a hearing evaluation during a meeting with the service coordinator:
I spoke about it during the meeting, about getting [child] a hearing exam, because we were worried. Our Service Coordinator said that like typically they like to wait until a child is having services for a few months before they do a hearing evaluation.
Hellen continued to advocate at the 6-month meeting, and although the speech language pathologist agreed that the child needed a hearing evaluation, the child did not receive it during EI.
Advocating for the Initial EI Services: “A Waitlist for Everything”
Some participants advocated for the initial receipt of EI services. Participants frequently reported being on long waitlists for EI services. Lauren stated, “I know some of the therapists have waitlists. I think right now even there’s speech waiting lists, so we are waiting for a therapist to become free to start speech.” Rebecca advocated to her service coordinator for speech therapy, but had to wait more than 3 months to start receiving services: “When I asked the case coordinator, basically [she] just said ‘Well, we don’t have any therapy available . . . ’ He was diagnosed with apraxia in May, and it took me until August to get speech therapy for him.”
Advocating While Receiving Services: “We Already Had It Rolling”
Participants also reported advocacy while receiving EI services. The most prevalent reasons to advocate included trying to receive more accurate documentation and finding an appropriate provider. Erika, the mother of a 2-year-old son with a developmental delay, shared her frustration with mistakes in her child’s evaluation report: “But her [the service coordinator’s] response was ‘it doesn’t really matter because he qualified [for services].’ But you know, I think for me it’s just that piece of making sure that things are documented correctly.” Similarly, Taylor reported advocating to correct her child’s paperwork: “My primary complaint is that our service coordinator provided inaccurate information in my son’s paperwork that unnecessarily limited who could provide services.” The report mistakenly stated that the child used a g-tube for feeding. As a result, there was an 8-month delay in receiving speech therapy.
Participants also advocated for new EI providers. Miranda was concerned that her provider canceled EI appointments frequently; consequently, Miranda’s child was not making progress. Melanie, whose child was receiving EI services at a childcare center, shared: “I trusted that she [EI provider] was working with my child an hour per week as the plan [Individualized Family Service Plan] is written. Well, [I] came to find out she only met with my daughter twice in 6 months.” Accordingly, Melanie advocated for a new provider. Eliza was frustrated when a non-certified speech and language pathologist was assigned to provide services for her family: “She [the service coordinator] found me a speech therapist, but she’s not certified . . . I was like, why are we hiring therapists who aren’t certified yet?” Eliza advocated for a certified provider.
Strategies for Advocacy
Researching and Seeking Information: “I Talked to Some Friends and Family, Did Some Research Online”
Participants described their advocacy as seeking information either from people (i.e., family, friends, and other parents of children who received EI services) or online. Sarah, the mother of a 6-year-old boy with autism, commented,
It was a lot of like just research, just going out and finding things on my own. Talking to other parents, just like looking things up, right? There wasn’t one specific place for any of these like you know, things . . . I was just kinda looking everywhere for some answers and resources.
Similarly, Taylor commented that she felt privileged to have the resources and skills to access information and resources for advocacy. She conducted online searches, talked to other families, and learned about state EI regulations. Taylor stated,
I’m privileged enough to be aware that I can look those things up, or even what to look up, and I by no means have a full grasp of everything related to EI, but I feel like I have an unusually strong foundation for someone just entering into this world.
Effective Communication: “Just Having Like an Open Dialogue”
Participants reported that proactive communication with their EI team was an effective advocacy strategy. Audrey and James, the parents of a 2-year-old boy with a developmental delay and hypotonia, emphasized the importance of stating clear expectations and asking clarifying questions with EI professionals:
Be very communicative, you know, I think, in situations. Yeah, clear expectations. And if we didn’t know saying, “I need you to explain this to me.” I think it’s very easy to get intimidated in situations like this. And I think also talking to each other about, we need to be his advocate because he can’t advocate for himself. So, I think we just kinda went into it with the mindset of be[ing] very communicative, you know, if we don’t like something, we don’t understand something [we] want clarification, and that’s still how we operate.
Proactive Attitudes and Persistence: “Not Taking a Back Seat and You Know, If You Want Something Done Right, You Gotta Do It Yourself”
Participants highlighted proactive attitudes while advocating for their child. Participants commented that persistence was key to advocacy. Andrea, the mother of a 3-year old with a speech and language impairment, reported her persistence advocating for accessing EI services:
I googled and I looked them up myself and I typed in like my information into it and then they called me and but really working with them and like keeping track of things and calling them back, that, persistence.
Susan described the advocacy process as a long battle requiring perseverance:
It’s a long battle. It’s a long battle that we’re still battling every day. But I think if you stay calm and you try to educate the best you can. Just take those small steps. If it doesn’t happen in a day, it takes years. I think the biggest thing is for parents, and anyone in advocacy it’s [to take] small steps. And then look at it year later and see the big win you have. But it’s a lot every day of the small steps to get there.
Relatedly, being diligent was another attitude identified as helpful for advocacy. Dana described being diligent as “being the glue that holds it together.” She elaborated,
Being on top of emails and joining everyone together and stuff, you know, and stuff like that. [. . .] just very diligent in getting back right away, making sure the whole team was on the same page with you.
Remaining calm was also identified as a helpful attitude. Miranda shared her advocacy of being calm when the EI provider kept canceling appointments: “I had to take a step back in order to not reply or respond when I was angry. You know, I didn’t want to do that.”
Facilitators for Advocacy
Prior Knowledge and Experiences: “I Know a Little Bit Easier How to Navigate the System”
Nine participants reported that their previous experiences working as an educator or health care provider helped them navigate the EI system, know their rights, and advocate for their child. Emily, the mother of a 1-year-old with a developmental delay, shared how although she was not familiar with the EI system specifically, her prior knowledge of the health care system acted as a facilitator to her advocacy: “I am a physical therapist by background, so I have a little bit of working knowledge on the system. I don’t know the [EI] system itself. So, I think I know already some ways to navigate the healthcare system.” Christina also described how her work in the disability field empowered her to advocate:
I work with adults with disabilities, and I work in the home-based services sector of it all. Just seeing other people and how they thrived and seeing these amazing parents who have thrived with these adults. I would say that was my background, you know, just seeing what you could have and what you should have.
In addition, three participants described having an older child who received EI services as a facilitator for advocating for their younger child. As Teresa, the mother of an older daughter with complex health needs and a 3-year-old daughter with a developmental delay, said:
[With my first child] I was walked through everything. Now that I have a second one, yes, I know exactly what to ask for now. But before, no. I couldn’t even tell you. I wouldn’t even know what it was.
Background knowledge equipped some participants with a deeper understanding of how systems work, their rights as caregivers, and how to effectively advocate for their child.
Strong Partnership With the EI Team: “Oh, I Totally View Us as a Team
I Love Our Therapists”
Positive and strong family-professional partnerships facilitated advocacy. Participants described practitioners as “allies” in their advocacy journeys. Mia described how a practitioner educated her about her rights:
She [provider] was the one who kind of suggested that you know maybe [another provider] it’s just not the right therapist for him. Maybe she’s just not a good fit. And you know, you can request another therapist. So that was what I did and then I spoke to the therapist directly and I spoke to the coordinator.
Similarly, Susan described how the EI team supported their transition out of EI: “The therapist and the early intervention coordinator really were able to help us kind of have that transition, and to keep pushing for the IEP and not letting them play the wait and see game.” Audrey shared her positive relationships with her EI team:
They made it feel, they made us feel like we were part of it, and part of the decision making, and made us feel comfortable, and what we were signing him up for, and in what we were scheduling. I felt very empowered.
Establishing and maintaining positive relationships with the EI team emerged as a crucial facilitator for effective advocacy. Caregivers characterized practitioners as valuable sources of information, guidance, and support.
Support Networks: “Having Someone to Talk to You About It”
Several participants identified building support networks as an advocacy strategy. Katherine commented that her family served as a support network for her advocacy: “Confiding in my husband, discussing it as a family. Having someone to talk to you about it.” Similarly, Taylor shared how her extended family supported her advocacy:
They’ve [grandparents] been so cooperative and collaborative in helping support him and providing additional, just additional people who can help implement, you know, and who are aware and asking questions by him and are interested in, and invested in his growth and development. So, we’ve like, a really good supportive family system. And I think some of that has come from me being [. . .] on top of things. I’m very much the leader of the advocacy, for my son, even with my husband. But I have a mutual expectation that they will be up to date and asking questions and aware of all the things that I share with them.
Other participants sought to build networks with other parents of children receiving EI services. Rebecca stated,
Actually, there’s a group called “the mommy districts.” And they posted on a couple of those [posts] trying to reach out to other parents who had been in early intervention to try to get names of therapists in my area.
Barriers to Advocacy
Lack of Knowledge About EI: “I Didn’t Really Understand the Components of the Program”
Some participants reported that a lack of knowledge about EI was a barrier to their advocacy. At the most basic level, some participants reported that they did not know what EI was or that it was available to them. Makena stated,
I felt like I discovered this treasure, and then the same parents that I talked to about my child having issues. They were like, “Oh, yeah, early intervention.” They knew it existed, but they didn’t tell me about it. It was so shocking.
Similarly, Stephanie said, “The state provides these resources and people just don’t know.” Audrey described understanding how the system works as a confusing process: “When we first started, we were pretty confused about like what services are, what he would get . . . especially because we got him evaluated at like 3 months old, so like we were brand new parents.”
She elaborated explaining that lack of knowledge makes it impossible to know what EI services to request.
Overworked Service Coordinators: “[We] Had to Reach Out to Her a Few Times and We Finally Got a Hold of Her Again”
Some participants identified overworked service coordinators as barriers to their advocacy. Stephanie reported that the service coordinator had good intentions to support her child but could not fulfill those intentions because she was overextended:
I think she [service coordinator] would be more hands on with advocacy help if she had more time. I feel like she’s definitely overbooked and like some of her emails will come in after work hours and I know she’s just going out of her way to make sure that I’m getting the services I need . . . I do believe that she’d be able to help more if she had, you know, more help.
Hellen reported the high turnover of service coordinators in her area: “We had two service coordinators, and then we were given to a manager for the last few months of our services after our second one left. And those transitions were hard.” Taylor described it as systemic issue: “they’re just so slammed by their caseload that I think it’s really difficult to maintain any kind of substantive contact. So, there’s some systemic issues in there.” Thus, while service coordinators played crucial roles in guiding families through the EI process, their heavy caseloads and time constraints hindered their ability to provide advocacy support. Caregivers expressed gratitude for the efforts of service coordinators but noted that their effectiveness could be enhanced if they had more time and resources.
Lack of Support From Social Network: “They Were Going Through a Really Hard Time”
Another barrier identified by caregivers was lack of support. Sometimes participants reported that they were not receiving support from other family members. Makena shared,
My son’s father did not think that he even needed services . . . It was stressful when the doctor, when you’re advocating the doctor’s not listening, then it’s hard, harder for family members who aren’t coming around, so if the doctor is like listening to you, then they’re conveying this information and go breaking down a barrier you know, for other family members who, you know, might have the stigma around it.
Participants expressed their desire to receive support from other caregivers of children receiving EI services. Rebecca reported that, on top of addressing her child’s needs, it was difficult to meet other caregivers of children with disabilities. She stated,
I wish that there was like a parent liaison that could come and kind of walk alongside of you to be like, you know, we felt kind of stuck, you know, through the process, because we were, you know kind of left to our own to figure it out.
While some caregivers identified parent support groups as a facilitator to advocacy, some caregivers—like Dana—shared that she would benefit from additional resources and opportunities to connect with other caregivers and access these support groups:
I just wish there were more parent resources, or you know, moms to talk to moms or dads with dads. Because everything is so focused on the kids. It should be, but this is . . . it’s a huge emotional, physical, financial undertaking, having, you know, a special needs child.
As participants shared, the absence of a strong support network hindered their ability to navigate the complex EI system and their advocacy efforts.
Outcomes of Advocacy
Successful Advocacy Experiences: “And I Felt Like My Opinion Was Heard”
When participants discussed their successful advocacy experiences, they described accessing services and their child’s developmental gains as the main outcomes of their advocacy. Christina shared,
She [child] did receive physical therapy. They did find her viable for services. And she graduated from them few months ago and she’s still in the other therapies, but I was glad that we had it for those few months.
As a result of her advocacy, Katherine reported that her daughter made tremendous progress in her communication skills:
She was able to get speech twice a month and then when she turned 2 it switched to weekly and it was with the speech therapist that we loved. When she started in EI, she was a year and a half couldn’t say any words. And by the time she left the program, she was speaking in 2 to 3 word sentences, explaining what she wants, her needs.
Unsuccessful Advocacy Experiences: “It’s Something That I Asked for
And I Couldn’t Get It, and I Didn’t Have It, and I Regret Not Having It”
Conversely, participants also reported experiences in which advocacy did not lead to their desired outcomes. Participants reported being frustrated when they were not able to achieve their goals. Rebecca shared,
It was kind of frustrating because we were kind of left to like [we were] basically told, “Well, you have to deal with this, or you don’t get services.” And that’s not beneficial to either me or the child . . . And we still have that current PT . . . I would say the delay in services really did impact it really, really did impact [him].
Although Hellen advocated for a hearing evaluation, her team refused to evaluate her son’s hearing. Hellen reported,
I think the delay in fixing his ears definitely led to frustration . . . pain, because he ended up having a couple of infections that did need antibiotic treatments, and I think it made his life harder because, if we had known earlier, then we would have been able to treat it earlier. And he wouldn’t have had as much frustration when he was trying to communicate with us.
Likewise, Makena described how the delay in receiving services hindered her child’s language development:
I think that he would have been a little further along for him and in the amount of like, words that he does try to get. Had it been, say, if she [the pediatrician] would have listened to me like even 6 months prior, I think that would have made a huge difference. Just us just even 6 months would have made a huge difference.
A Mixed Effect on Caregivers: “It Definitely Changed My Perspective”
Some participants reported that advocacy worsened their health and well-being. For example, some participants reported that advocacy caused stress in light of their other caregiving responsibilities. Miranda reported,
It’s frustrating to have to, you know, juggle and carry more especially, you know, with all the other stuff. I’ve got, these two kids in early intervention, working full time, just trying to, just trying to keep up on life and. It’s really difficult. [. . .] You know, I was frustrated. Just accept, I guess I accepted the fact that you know, my kids have special needs and I might have to take more time away from work, or I might have to do more to advocate for them.
Some participants reported other negative outcomes of advocacy on their health and well-being. Mia reported, “It’s a good thing, you know, to kind of become an advocate and be able to speak up. But it’s also kind of traumatizing to be honest.”
Conversely, some participants reported that their advocacy positively affected them. Specifically, they reported that their advocacy empowered them and increased their self-confidence. Taylor shared, “I feel very confident that I can be a voice for my son until he hopefully has a voice of his own. But it’s empowering to go through what we’ve been through and see the positive progress he’s made.” Similarly, Stephanie commented,
I’m really proud of myself for staying on like on top of, making sure that I got that evaluation. Like, I had to first argue with the pediatrician and then I had to fight to get an appointment for him and I’m just really glad that I was able to do that.
Some participants reported that their advocacy helped them learn more about their rights and spurred peer and systemic advocacy. For example, Daysi reported that her advocacy helped her learn more about parental rights: “I just learned better you know, what parents’ rights are. And you know, you really have to fight for getting your kid help.” Relatedly, Lauren shared how advocacy helped her learn more about her grandchildren’s needs: “It made me more knowledgeable. It made me more curious to learn more about what a child needs, what a baby needs.” With respect to facilitating more advocacy, Dana reported that when advocating for her child, her advocacy may affect other children receiving EI services: “It just feels good. To make positive change, not just for yourself, but for things that are bigger than you, ’cause it could affect other kids in the same situation and parents in the same situation.”
Similarly, Jennifer shared how her advocacy helped her learn skills that she can use to support other families: “I have taken the time to make the phone calls to do the research. I’ve been able to help other families.” Some participants reported that advocacy for their own child spurred them to conduct systemic advocacy. Rebecca reported that her frustrating advocacy experience made her want to change things in EI, not only for her but for other families too: “It’s made me really want to change some things within EI, because I think parents need a lot more support.” Jennifer described how her advocacy led her to get involved in collective legislative advocacy, not only within EI, but in early childhood advocacy in general:
I think like my experience with EI has led me to like, on a more broader . . . like early childhood advocacy work in terms of writing to senators and representatives and having that voice, especially most recently when we tried to get when we worked so hard, a bunch of us across the state worked so hard to get that Smart Start [State] pass. I think that little bit there and helping other people in my community realize that like EI is available. And what your rights are as an EI, [it] has really been positive.
Discussion
The purpose of this study was to explore the advocacy experiences of caregivers of young children who receive EI services. The findings highlight the crucial role that advocacy plays in EI, and its impact on caregivers and their children. We had four main findings. First, in alignment with Schraml-Block and Ostrosky’s study (2022), our findings suggest that caregivers start advocating for their children early in their child’s life and continue to do so while receiving EI services. This finding aligns with an empowerment framework suggesting that parents often encounter challenges during EI which prompt them to advocate. While most studies about parent advocacy focus on school-based services suggesting that advocacy begins at age 5 (Burke, 2012), our study confirms that advocacy occurs during EI services. Indeed, some of our results further suggest that advocacy can begin in utero advocating for a child to receive EI services upon birth.
This finding has tremendous implications for future research. More research is needed exploring advocacy during EI. Relatedly, longitudinal research about parent advocacy over time—beginning in EI and extended into adulthood—is also needed. Prior advocacy experiences often affect parents’ future advocacy experiences (Burke et al., 2019). As our study suggests that advocacy begins during EI, it is possible that families’ early advocacy experiences predict their future advocacy efforts. Thus, research is needed to investigate advocacy during EI and to explore whether early experiences impact how parents advocate as their children age into school services.
Second, there were some similar and some different advocacy strategies during EI and school-based services. With respect to similarities, some of the advocacy strategies aligned with the strategist advocacy and disability expert advocacy suggested by Trainor’s (2010) study with parents of school-aged children with disabilities. Furthermore, some participants aligned with being “agents of systemic change” (Trainor, 2010) by advocating for other families and pushing for legislative changes for all children with disabilities. The shared advocacy strategies used during EI and school services suggest that such strategies can be generalizable across age-periods and settings.
However, a few advocacy strategies reported by participants did not align with Trainor’s (2010) categories and seemed more related to the personality of the participant. For example, participants mentioned that having a proactive disposition, persistence, and open communication style were critical to their advocacy efforts. While these characteristics were characterized by participants as strategies, they could also be viewed as facilitators of effective advocacy. This distinction is important, as personality traits—such as grit, as identified by Goldman et al. (2019)—are inherent characteristics that may influence how advocacy strategies are employed but are less likely to be strategies that can be taught or adopted through training.
This finding does align, to some extent, with other literature suggesting that assertiveness and communication are important elements of parent advocacy (e.g., Bourke-Taylor & Jane, 2018; Goldman et al., 2019). However, it may be helpful to further clarify the distinction between advocacy strategies, which are actions and behaviors that can be learned or adopted, and facilitators, which are traits or resources (such as personality characteristics or social capital) that support the effectiveness of these strategies. Future research is needed to better understand how personality traits and attitudes intersect with advocacy strategies, and how supports can be tailored to accommodate unique communication styles and personality characteristics to enhance advocacy skills.
Third, an identified facilitator of advocacy was access to social capital. Specifically, access to a support network was critical for advocacy, while the absence of support was seen as a barrier. These findings suggest that a support network is crucial for families of children in EI. For parents of school-aged children with disabilities, peer support has been documented as an effective way for families to learn about service delivery systems (Jamison et al., 2017). The larger body of literature about parents of individuals with disabilities also confirms that parents want to connect with other parents of children with disabilities (Iadarola et al., 2020). While parents of school-aged children may have opportunities to meet other families at school, EI services are often provided in the home, making it more challenging for families to connect. This highlights the need for practitioners to consider ways to facilitate connections between families in EI.
Fourth, knowledge about one’s rights and the service delivery system matters. Specifically, participants reported that greater knowledge about rights and services facilitated advocacy; conversely, the absence of knowledge was a barrier to advocacy. This finding aligns with the extant literature suggesting that knowledge is key to advocacy (Goldman et al., 2019; Zuckerman et al., 2017). Fortunately, knowledge is a malleable barrier. There are many advocacy programs that target knowledge as a way to facilitate advocacy (e.g., Pearson & Meadan, 2021; Rios et al., 2021). Our finding underscores that such advocacy programs should consider including families of children in EI who may also benefit from learning their rights.
While knowledge can be addressed by extant interventions, the systemic barriers (e.g., high caseloads for service coordinators) may require more effort, time, and funding to overcome. There is a national shortage of EI professionals (Council for Exceptional Children, 2020; Vail et al., 2018). Solutions to address systemic problems include improving compensation and financial incentives for professionals; strengthening program management and organization; moving toward a positive climate and culture; and offering more opportunities for training and mentoring (Yeager et al., 2023). Such solutions are laudable and needed. However, such solutions often require a comprehensive approach across multiple systems—a large and daunting effort.
Limitations
While an important launching point to understanding the advocacy experiences of caregivers of children in EI, this study had several limitations. First, the participants reflected a convenience sample. Specifically, many participants had college or graduate degrees; several participants worked in the disability field. All participants were interested in participating in a leadership program and only reflected one state. Notably, the state in this study may differ from other states. For example, in the state of this study, there is a waiting list of more than 10,000 children for EI services. Families in other states may have different advocacy strategies if their states do not have waiting lists. Because of these characteristics, there may be limited transferability of the findings. Second, some participants reported on their experiences in EI 5 years ago, whereas other participants reported on their current experiences. While we did not find differences between participants who currently (vs previously) received EI services, it is possible that recalling advocacy experiences was more difficult for families of older children. Also, within the past 5 years, the COVID-19 pandemic occurred; thus, it could be that there are differences in advocacy experiences among the participants.
Directions for Future Research
There are several directions for future research. Future research may consider disentangling the relation between a strong family–professional partnership and parent advocacy. In this study, participants reported that their positive partnerships with EI providers facilitated their advocacy. However, other studies suggest that advocacy occurs when there are negative partnerships with school professionals (e.g., Burke & Hodapp, 2016; Pearson & Meadan, 2018). Close examination of how a family’s relationship with professionals can enhance or inhibit parent advocacy is warranted. Furthermore, it is important to understand the sequence of effects with respect to these two constructs: Does a stronger partnership lead to greater advocacy? Does a strong partnership lead to less advocacy? Does advocacy lead to a stronger partnership? or Does advocacy lead to a weaker partnership with professionals? Future research may include longitudinal data to help discern the direction of effects.
Research is also needed to further examine the effect of advocacy on the child as well as the family as a whole. In alignment with prior research, this study suggests that parent advocacy can yield positive effects for the child (e.g., increased access to services) as well as neutral effects for the child (e.g., no changes in service receipt). Furthermore, this study suggests mixed effects for families including positive effects (e.g., greater empowerment) and negative effects (e.g., greater stress). Such findings align with prior research about the potential effects of advocacy for children with disabilities (Burke et al., 2019; J. L.Taylor et al., 2017) and families (Ashcraft et al., 2019; Burke & Hodapp, 2014). Future research should more closely examine the effect of advocacy on children and families including identifying moderators of effects (as suggested by the current study and extant research). Because of the mixed self-reported outcomes identified in this study, an important next step is for research to consider the circumstances under which positive and negative outcomes occur. Future research should also examine whether there are patterns in relation to positive and negative advocacy experiences.
Implications for Practice
Based on our findings, EI professionals should continue to educate and empower families to advocate. In addition to being a key outcome of IDEA, this study suggests that practitioners play important roles in educating families about their rights and empowering families to advocate for services. EI professionals, including service coordinators, should refer parents to Parent Training and Information Centers, foster a collaborative approach with parents, encourage open communication, engage in shared decision-making, and provide families with clear and accurate information about their rights. Such roles and responsibilities are key for EI providers and service coordinators as they may help families not only during EI but also as their children enter school-based services. The shortage of EI professionals poses challenges to timely access to services and advocacy support for families. Policy efforts aimed at addressing the EI provider shortage are crucial to ensuring that all children who need EI services are able to receive services. To that end, policy efforts may need to include increased funding for EI programs and expanded training and certification opportunities for EI professionals.
Furthermore, EI professionals should consider extending more opportunities for families to participate in peer and systemic advocacy. This study suggests that families are organically helping other families advocate and/or engaging in systemic advocacy. To this end, practitioners may recruit families to serve as formal parent liaisons so they can help other families in EI. Also, practitioners may make targeted efforts to invite families to serve on their Statewide Interagency Coordinating Councils to help inform decision-making about EI services.
Conclusion
This study added to the incipient body of literature exploring parent advocacy during EI, revealing important insights for practice, policy, and future research. The findings underscore the early onset of parent advocacy and the need for further research exploring advocacy during EI. The identified facilitators and barriers to parent advocacy in EI suggest that policies should focus on addressing the systemic challenges in EI to ensure access to needed services. EI professionals should educate and empower families to advocate, recognizing advocacy is a tenet of IDEA.
Footnotes
Author Contributions
Development of the interview protocol, data collection, and data analysis were performed by AKT, KF, AH, and MB. All authors are contributing writers and reviewed all versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Institutional Review Board of the University of Illinois Urbana Champaign.
Informed Consent
Informed consent was obtained from the participants.