
Abstract
At the beginning of the 21st century, the interdisciplinary model for treating patients suffering from chronic pain has been adopted by a growing number of health centers. There is not, however, enough research examining how patients treated in clinics guided by this philosophy experience their condition and treatment. The purpose of this study is, therefore, to gain a closer understanding of the experience of these chronic pain patients. Semistructured interviews were conducted with 15 men and women aged 24 to 54 years who have suffered from chronic pain for over a year. The interviews were analyzed using the interpretative phenomenological analysis method. According to our analysis, participants experience themselves as trapped within endless pain that blurs their sense of identity and autonomy and isolates them from their environment. Participants expressed their desire for a close and caring relationship with their doctors as a way of relieving their sense of isolation. Based on our analysis, we suggest a patient-centered model for guiding doctors caring for chronic pain patients, which highlights the patients’ social and emotional experiences in addition to their medical condition.
The International Association for the Study of Pain defines pain as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage” (Nanna et al., 2016, p. 1599). Pain is a signal informing the individual that the body is undergoing an attack. Pain lasting longer than 3 months is defined as chronic and addressed as a disease in its own right rather than merely a biological indicator (Waddel, 1998). In 2008, the American Academy of Pain recognized that chronic pain syndrome had become an epidemic, reaching a rate of between 11% and 55% among adults in western countries (Neville et al., 2008), with higher rates found among women (Kindler et al., 2010) and older people (Jackson et al., 2016; Kindler et al., 2010). A 2016 meta-analysis of chronic pain prevalence in low- and middle-income countries demonstrated 5% to 42% of people within general populations suffering daily headaches as well as 10% suffering daily headaches and 79% suffering musculoskeletal pain among the working population (Jackson et al., 2016). A survey carried out in China (n = 19,665) showed chronic pain incidence of 32.17% and 39.92% among men and women, respectively (Chen et al., 2016). In the United Kingdom, a meta-analysis revealed a frequency of 35.0% to 51.3% of chronic pain (Fayaz et al., 2016), and in a survey conducted in Israel between 2013 and 2015, 53.7% of those surveyed reported occurrences of back pain and 25.3% neck pain during their lives (Israel Center for Disease Control, 2014). All the aforementioned studies support findings showing that the prevalence of chronic pain is higher among women and older people.
Various longitudinal studies have suggested that chronic pain triggers a vicious cycle of emotional and behavioral responses including mood disorders and anxiety (Annagur et al., 2014), sleep difficulties (Finan et al., 2013), drug addiction (Vowles et al., 2015), and suicide ideation or attempts (Campbell et al., 2015). Participants in phenomenological studies often describe pain as an untamable monster attacking a rebellious, traitorous body and perceive their lives as controlled by pain and their continuous search for a cure (Connor et al., 2008). They also point out the powerful influence of physical pain on emotions, identity, and everyday life (Ojala et al., 2015). Additional themes relate to a sense of isolation and frustration due to loss of independence and the need for the acknowledgment of their pain by, specifically, health professionals (Hansson et al., 2011).
The understanding of pain as a biopsychosocial phenomenon has given rise to various theoretical models that highlight and attempt to explain its different aspects. Loeser’s (1991) onion model regards pain as comprised of four layers: the first layer, at the heart of the onion, is nociception—the sensory nervous system’s response to (potentially) harmful stimuli; the second layer is the feeling of pain; the third layer is suffering; and the fourth and outer layer is the demonstration of pain behavior through words, actions, or expressions. Of the four layers, only the latter is outwardly visible; the inner layers of suffering, pain, and nociception are experienced only by the patient. The onion model illustrates that in order to provide effective treatment, the patient’s hidden layers must be acknowledged and understood (Robins et al., 2016).
Loeser’s onion model has been widely used in the education of professionals and patients, both within the context of pain relief clinics and outside of it (Atkinson & Zacest, 2016; Loeser, 2006; Robins et al., 2016; Vasudevan, 2015).
In recent years, growing attempts have been made to help chronic pain patients in multidisciplinary clinics. While some have praised these pain clinics for focusing on pain behavior and attempting to reshape it (Breton et al., 2008), others have suggested that this approach is ineffective because of its narrow perspective on the patients’ whole experience (MacDonald, 2000). The aim of this study was to explore the experiences of chronic pain patients treated at a multidisciplinary pain relief clinic in order to get a broader perspective and, specifically, to shed light on their perceptions of interactions with the professionals treating them at the clinic.
Method
Qualitative analysis was chosen as the appropriate method for this study. Qualitative research aims to capture complex, highly subjective life phenomena by collecting data from which themes are extracted. Semistructured interviews were conducted, which enable the interviewer to approach the inner world of the interviewees while accommodating their preferred pace and degree of exposure.
In an attempt to remain as close as possible to the authentic voice of the interviewees, we chose the interpretative phenomenological analysis (IPA) as our method for the analysis of the interviews. IPA aims to convey the participant’s own perception of an experience rather than present an objective account of it and thus enables the analysis to go beyond the standard thematic one (Smith & Osborn, 2009). This, paired with the narrative nature of the final analysis of IPA and its usefulness in portraying the complexity of human experiences, was the reason it was chosen for this study (Smith & Osborn, 2003).
Authorization for the research was obtained from the ethics committee of the academic institute and the Helsinki Committee of the hospital in which the research took place. All participants signed an informed consent form prior to the interview.
Participants
Fifteen participants (seven men and eight women aged 24–54 years) were recruited via an advertisement posted at the pain clinic and subsequently interviewed. All participants had been receiving treatment at the clinic for over a year.
Data Collection
Semistructured interviews were conducted in line with Smith and Osborn’s (2003) guidelines. Each participant was informed of the purpose of the study and then asked: “Could you tell me freely and in your own words about your experience of living with pain?” Further questions included: “What are your needs as a person living with pain?” and “Can you tell me about your interactions with the medical staff?” The interviews were recorded and transcribed, and the participants’ personal details were disguised to maintain confidentiality.
Data Analysis
The interviews were recorded and transcribed following Smith and Osborn’s (2003) guidelines. The first transcript was read and reread, notes were made, and key phrases extracted. The rest of the transcripts were then read and analyzed in order to identify subordinate themes which reoccur in the various interviews. Further analysis enabled the grouping of the subordinate themes into superordinate themes. Transcripts were then reread with the intention of gleaning a sense of the whole as well as further solidifying the grouping of the themes. This circular manner of analysis forced the authors to check for coherence between their interpretations in a consistent manner. Another experienced researcher reviewed the stages of the analysis and added her insights in order to provide a comprehensive perspective on the data during all phases of the research. The authors then held an intensive discussion on the findings and possible interpretations based on a comprehensive theoretical basis (Shkedi, 2003). We ended up with a narrative which attempts to capture some of the experience described by the interviewees.
Results
Our analysis identified nine subordinate themes: a cage of pain, to live with pain forever, loss of autonomy, lost identity, invisible pain, no one understands, disappointing treatments, the disappointing doctor, and the good doctor. The nine subordinate themes were then grouped into four superordinate themes: life imprisonment, the vanishing self, loneliness, and the medical system (see Figure 1).
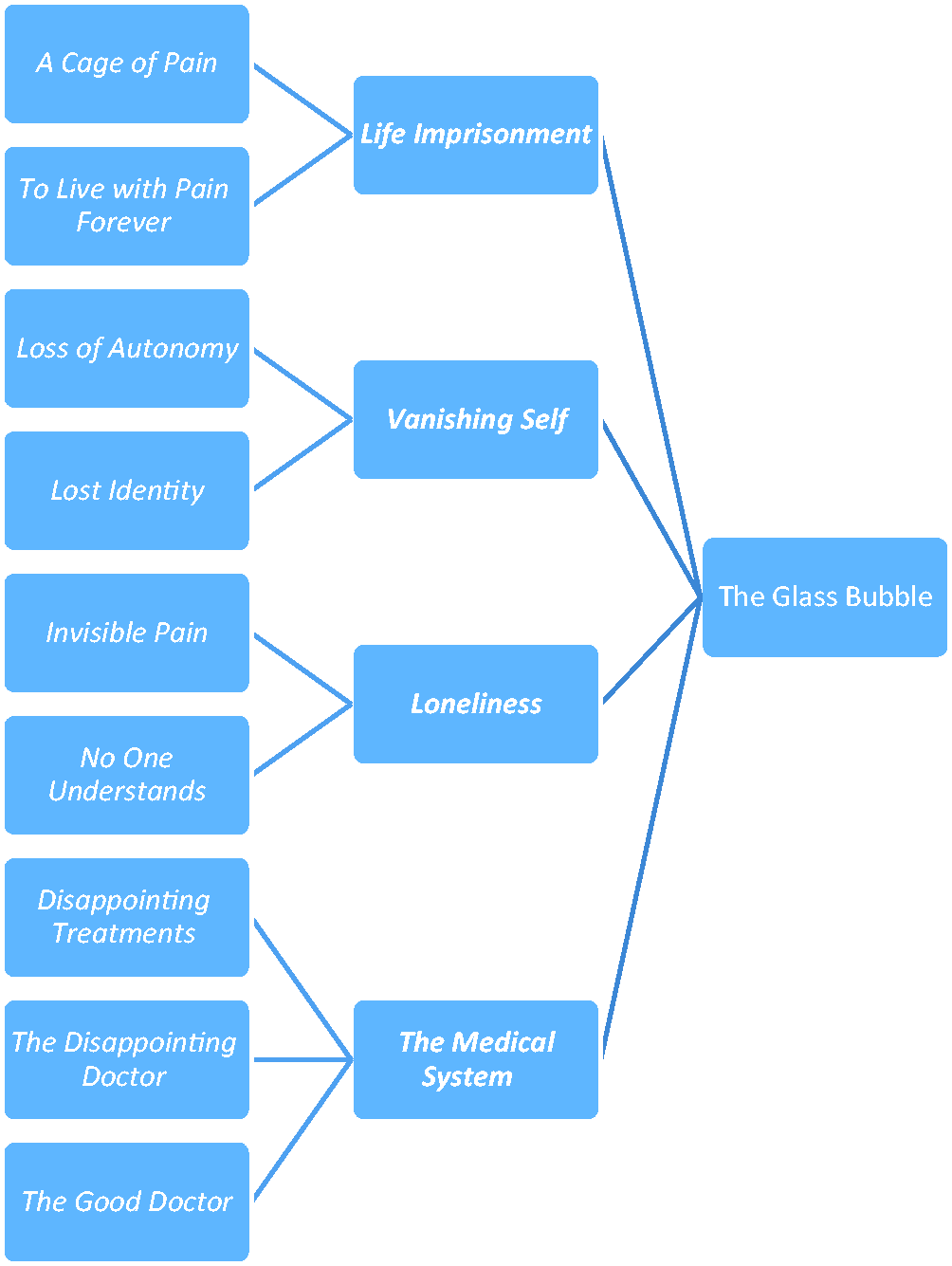
Relationship Between the Subordinate and Superordinate Themes.
Life Imprisonment
A Cage of Pain
Participants described their pain as confining and feeling “stuck” or “blocked” behind its walls, which obstructed their path to normal life: “I’m now in a situation where I feel trapped. What can I do? No money, no job, no hope for a future … I’m stuck” (Abraham). 1
To Live With Pain Forever
Whether from acceptance or despair, the participants expressed a sense of being destined to live with pain from now on, pessimism regarding their chances of recovery, and concern for their future: “What will I do when I have kids? How will I lift a baby? How will I even give birth … breast feed?” (Michal). Participants frequently expressed their yearning to return to a time when they were free of pain: “To go back in time. To remove from myself all the injuries, all the pain, the paralysis brought on by the pain. To get my life back” (Debbie). They, nonetheless, acknowledged the unfeasibility of regaining a pain-free life: “but now I know that it is not possible” (Adina).
Vanishing Self
Loss of Autonomy
Participants described themselves as unable to operate freely within their surroundings, that is, at work and home and in their social relations. They also expressed a belief that the medical and rehabilitative staff regard them as cognitively impaired and incapable of making decisions. Abraham, for example, agreed to undergo surgery even though no one explained its implications to him: No one tells you what may happen to you during the operation, they only tell you: “We want to operate and there is an opening next week so don’t eat anything and be there.” … I went along with it because I thought there was no other alternative. I was stupid, blind, I blindly believed it would improve things.
Lost Identity
Participants also spoke of how the pain “robbed” them of what had defined them in the past: their roles, resources, and personality attributes. Benny mentioned his loss of identity as a parent: To play with the kid. Now I can’t even throw him a ball. He takes the ball to the yard and throws it against the wall, as if playing with the wall … he’s already stopped asking: “Dad, come down and play with me.” But just looking at him, it’s … guilt. And shame.
Loneliness
Invisible Pain
Participants explained that as their pain is invisible, others find it difficult to relate to it as “real”: “I don’t … sit in a wheelchair or something, like some of the people here at the clinic. So … from that perspective, I’m not, like, ‘disabled’” (Benny). Many wondered—often angrily—whether people in their surroundings actually believe them when they say that they are suffering; others were seeking to achieve confirmation and validation from their surroundings.
No One Understands
Participants perceive their pain experience as a singular phenomenon and expressed their frustration at the absence of a common language with healthy people. They claimed that even those treating them do not truly understand their experience: You see that they [the doctors] don’t really understand you, they don’t really understand why you make such a fuss of your life, they don’t understand it can hurt so badly you wanna die. You come out of meetings with them and feel even more fucked up, like, you can’t even explain what you’re going through. (Abraham)
The Medical System
Disappointing Treatments
Participants described themselves as embarking on a long journey in search of a cure for their pain—an odyssey including numerous diverse treatments and medications. The results are usually disappointing, and treatments frequently fail to achieve the desired solution. Even more frustrating are medications that alleviate the pain for a short period of time but quickly stop having any effect: Each time something new reaches the shelves I say, let’s do it, bring it on. But then you discover that it doesn’t exactly work, or doesn’t work at all, or that the alleviation is only for a short time, and then—bang comes the pain again. (Keren)
The Disappointing Doctor
Chronic pain patients frequently experience the medical system as well as their own doctor as unable to help. Following long periods without any real solutions for their plight, many revise their image of the all-knowing doctor asking themselves whether they can indeed be trusted. This sense of inefficacy gives rise to feelings of anger: “Many of the doctors I’ve met don’t know a whole lot about chronic pain. They guess a lot … they have no idea, they don’t know any more than you do” (Keren).
The Good Doctor
Reading between the lines, participants’ descriptions of their encounters with different types of doctors expose their image of the “good doctor”: In fact, during the visit today I think I met a really good doctor here at the clinic. He listened to me; he acted like he really believed what I was saying and gave me time to speak. He didn’t treat me as if I was dumb or bothersome. It felt like … a small victory! He even had some good recommendations, I think, and I’m optimistic about the medicine he prescribed. He also suggested referring me to someone who actually specializes in my problem. It was luck, it doesn’t happen often. So today I’m happy. (Keren)
Chronic pain patients also express a deep desire for a benefactor or a “good doctor” figure who will not just try to solve the medical problem but will also find a way to overcome the elusive and invisible nature of their pain. This is a doctor who can contain the suffering patient’s pain, demonstrate support, and provide a calming and respectful presence. By listening to their pain narratives, the “good doctor” will validate their experience while still looking for a medical solution. This doctor thus overcomes the tendency of the biomedical model to construct the illness narrative as a narrative of separation “of doctor from patient” and “of person from body” (Radley, 2000), treating patients as embodied, subjective, and autonomous human beings rather than objects that need to be rewired and thereby engaging in an empathic rather than just a functional interaction.
Discussion
Loeser’s (1991) stratified onion model highlights the fact that pain is internal, personal, and private and thus unamenable to objective observation or measurement, with the exception of the outlying pain behavior. However, the onion model allows no access—in fact seems to ignore—patients’ subjective experience. It positions doctors outside of their patient’s pain experience, leaving them to focus on the external, objective pain behavior in an effort to find a medical solution. The internal, subjective layers of the patient’s pain narrative, especially their suffering and feelings of pain, all exist within the patient’s hidden world, to which the doctors have no access.
While the onion model may be useful during the acute stages of pain by directing the doctor to look for objective findings pertaining to the specific pathology indicated by the pain, its application to chronic pain causes difficulties at the personal and interpersonal levels. This is because the onion model encourages doctors to examine chronic pain patients in a partial manner, limiting themselves to the narrow context of the disease, for example, pain behavior, while neglecting other aspects of the patient’s identity. Such attitudes may reinforce patients’ feelings that their chronic pain blurs their personality and that they are being treated merely as objects.
Doctors guided by the onion model might therefore continue their search for the causes of the pain behavior, making use of the objective tools available to them and prescribing medications, while often disregarding their patients’ need for empathy as well. These attitudes can be detrimental to the doctor–patient relationship. Doctors who limit their attention to objective pain behavior may not be empathetic toward their patient’s suffering, sometimes becoming impatient or angry at what they perceive to be the acts of difficult and overdemanding patients. Returning, untreatable patients who do not progress according to expectations tend to evoke a sense of failure in doctors, which leads to negative consequences for themselves as well as for their patients and may possibly affect the quality of their treatment (Spickard et al., 2002). Coping with patients whom they cannot help causes demoralization and burnout among doctors (Kenny, 2004; Spickard et al., 2002).
The onion model also encourages a fragmentary view of patients. While multidisciplinary clinics address patients’ range of needs, the artificial separation between the various spheres of life with chronic pain often means that patients are treated by a number of professionals who have no interaction with one another or common language.
The mental processes that patients undergo when coping with their status as chronic pain patients—including rage, mourning, and reconciliation—take place in a way that leaves the doctor uninvolved. When these processes emerge during doctor–patient encounters, the doctors do not typically possess the appropriate tools for dealing with them. The fact that their doctor is not privy to their internal world contributes to the patients’ sense of anger, anxiety, and helplessness.
In this study, participants expressed their frustration and anger at not being “taken seriously” and at insinuations that their pain is “only in their head” and their fear that they might be losing their minds. Encounters between doctors in pain clinics and their patients as a dialogue between the deaf and the dumb suggest possible detrimental impacts on the healing process (Kenny, 2004).
Allegretti et al. (2010) portrayed the incongruence between doctors’ and patients’ models of pain through the case of a patient for whom his doctor’s acknowledgment of his pain as real—even in the absence of objective findings—was seen as a form of salvation and victory.
Our Proposed Model
The experiences described by participants in our study suggest that doctors can play a central role in transforming the realm inhabited by chronic pain patients. They can make it a more bearable and humanistic experience with patients more willing to acknowledge their authority and to entrust them with their hopes. A meaningful evaluation of chronic pain patients requires not only a clinical examination of objectively measurable findings but also attentiveness to their subjective reports of their experiences (Fishman et al., 2010) and recognition of the person inside the bubble.
Based on the analysis presented earlier, we wish to propose a new model for understanding patients’ pain experience. While based on the four pain components described by Loeser (1991), instead of the closed form of an onion, our model suggests an open, flower-like shape (see Figure 2).
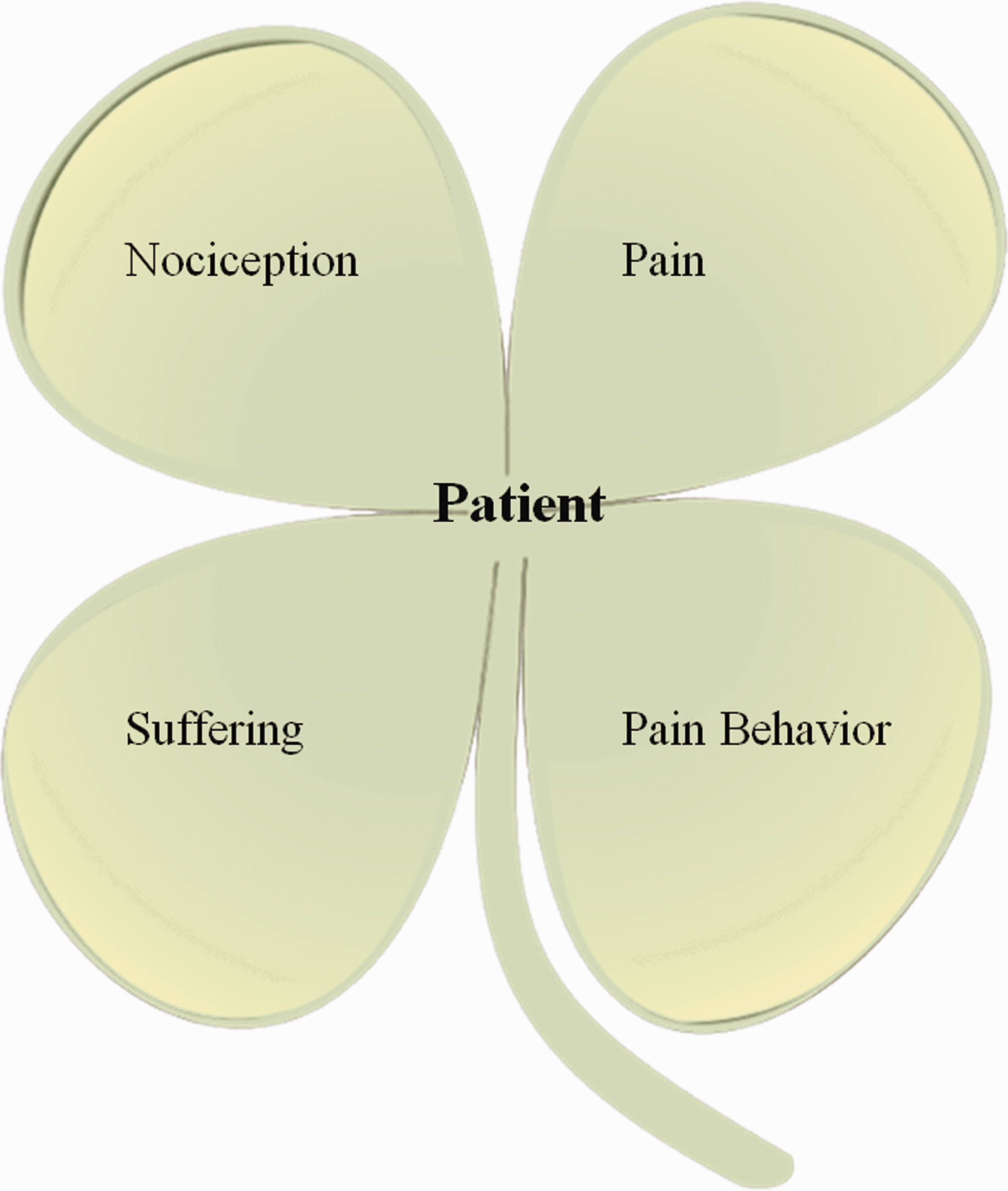
A Flower Model of Pain Experience.
By presenting this model, we hope to encourage doctors to take into consideration the overall range of components, neural, emotional, and cognitive, which together comprise patients’ total pain experience. An emphasis on the complex relations between these components and the need to perceive them as a whole experience rather than a series of fragments serves as a reminder that within the “pain syndrome” there exists an individual who yearns to be listened to and believed and to have their feelings affirmed. We believe that the adoption of such a stance will contribute to the implementation of the biopsychosocial model which, while strongly advocated, is yet to be fully integrated into medical services (Lane, 2014).
In this sense, our model represents a transition from the disease-centered approach of the onion model to a patient-centered approach that considers biological, psychological, and social factors, all of which affect the process of coping with pain (Fishman et al., 2010). Such an approach has been proved effective in several aspects relating to patients’ coping including adherence to treatment, improved physical condition, and a sense of reassurance (Connor et al., 2008).
To validate our findings and transform the alternative model presented from a theoretical to a practical framework, the experience of medical professionals adopting this model in the treatment of chronic pain patients should be examined. We believe that this model may not only help chronic pain patients receive better treatment from their caregivers but also improve doctors’ experience of working with chronic pain patients and, hopefully, lessen their compassion fatigue and burnout that results from the ongoing treatment of chronic patients (Spickard et al., 2002).
The subjective, evasive, and predominantly psychological nature of pain all demonstrate that it should be understood as occupying an intermediary position between physiological pathology and emotional distress—pain as the body’s emotion. The insights gained from this study join a relatively small corpus of phenomenological research on chronic pain patients. We hope that additional research will expand the study of populations whose suffering is invisible.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.