
Abstract
Deaths from COVID-19 have exceeded 6.5 million people globally. Although many people are mourning the loss of loved ones to this deadly disease, little is known about the validity of measuring coronavirus-related anxiety with this particular group of people. Therefore, the objective of this study is to determine if the coronavirus anxiety scale (CAS) measures the coronaphobia construct the same way for mourners with and without dysfunctional levels of grief. The results indicated that the four-item version of the CAS has acceptable fit indices and is partially invariant between people with dysfunctional and non-dysfunctional grief. Moreover, the CAS demonstrated adequate criterion validity and reliability with this group of bereaved adults. In conclusion, the CAS can be used to measure anxiety due to COVID-19 in people who are going through dysfunctional and non-dysfunctional grieving processes.
Keywords
Introduction
Since the announcement of the first case of COVID-19 at the end of 2019 (World Health Organization [WHO], 2020), there were many reports of a high increase of infections until the pandemic was finally declared in March 2020 (Pan American Health Organization [PAHO], 2020). In response, different countries around the world took preventive actions to avoid the spread of this deadly virus. For instance, in El Salvador, the measurements included mandatory home quarantine (López & Domínguez, 2021) and in the case of deaths from COVID-19, a specific protocol prohibited funeral ceremonies (Ministry of Health, 2020). However, the COVID-19 pandemic caused effects that went beyond physical health. According to PAHO (2020), the prevalence of anxiety and depression worldwide has increased by 25% as a result of the COVID-19 pandemic. In the case of El Salvador, evidence indicates a high prevalence of anxiety symptoms due to COVID-19 since the beginning of the pandemic (Chacón-Andrade et al., 2020; Gutiérrez-Quintanilla et al., 2020; Lobos-Rivera et al., 2022; Orellana & Orellana, 2020). Although a moderate level of anxiety can be helpful during disease outbreaks, as they motivate people to actively cope with immediate threats, severe levels of these reactions can be debilitating and develop into mental conditions (Taylor, 2019). In the context of the COVID-19 pandemic, debilitating anxiety about the coronavirus has been referred to as coronaphobia (Asmundson & Taylor, 2020).
Coronaphobia has been examined in numerous studies across the globe. The primary instrument used to measure this form of anxiety is the coronavirus anxiety scale (CAS; Lee, 2020). The CAS measures physiological reactions to anxiety generated by information or thoughts related to the coronavirus. The CAS presents solid psychometric properties and has been validated in different countries, such as Turkey (Evren et al., 2022), Peru (Caycho-Rodríguez et al., 2020; Caycho-Rodríguez, Vilca, Carbajal-León, et al., 2022), Bangladesh (Ahmed et al., 2020), and Portugal (Magano et al., 2021), among others. In addition, different studies have verified the invariance of CAS measurement based on sex (Caycho-Rodríguez, Vilca, Carbajal-León, et al., 2022; Silva et al., 2020), age (Franco-Jimenez, 2020), and the country where they reside (Caycho-Rodríguez, Valencia, et al., 2022). CAS research has revealed that coronaphobia is linked to a wide range of mental health issues, such as emotional distress (Choi et al., 2022; Lee et al., 2020a), drug and alcohol coping (Lee, 2020; Lee et al., 2020a), suicidal ideation (Lee, 2020; Lee et al., 2020b) and low levels of resiliency (Labrague, 2022; Skalski et al., 2022). More importantly, coronaphobia has been shown to be so disruptive to people's day to day lives, that many have been functionally impaired by this particular form of pandemic anxiety (Chen et al., 2021; Choi et al., 2022; Lee, 2020).
Clinicians and researchers alike have long observed that the high arousal states that accompany grief can sensitize some bereaved to also experience clinical anxiety (Jacobs et al., 1990; Shear & Skritskaya, 2012). In fact, several studies have documented a positive correlation between grief symptom severity and levels of anxiety (Byrne & Raphael, 1998; Eisma et al., 2017; Lee, Mathis, & Jobe, 2021). Although the relationship between grief and anxiety is well established, this connection has not been systematically examined within the context of the COVID-19 pandemic. More specifically, the extent to which coronaphobia, as measured by the CAS (Lee, 2020), is measured in the same way for the bereaved with and without dysfunctional levels of grief has yet to be empirically examined. This question of the CAS's measurement invariance is particularly important to answer, given the significant number of bereaved individuals who will need to be evaluated for both complicated grief (Lee & Neimeyer, 2022) and dysfunctional levels of anxiety (Fischer et al., 2020) during this global health crisis. Moreover, evidence of CAS measurement invariance will allow researchers, health professionals, and public health policy makers and legislators to have accurate information to compare and assess the true differences in COVID-19 anxiety between people with and without dysfunctional grief.
In the present study, we aimed to evaluate the measurement invariance of the CAS (Lee, 2020) between bereaved Salvadorans who present dysfunctional and non-dysfunctional levels of grief. Specifically, we examined the factorial structure and reliability of the CAS. Although there is no previous evidence to prove the invariance of the CAS measurement between people with different types of bereavement, we expected that the scale maintains the invariance that it has shown when comparing it between other kinds of groups (Caycho-Rodríguez, Vilca, Carbajal-León, et al., 2022; Caycho-Rodríguez, Valencia, et al., 2022; Franco-Jimenez, 2020; Lieven, 2021; Silva et al., 2020). Similarly, we expected that the CAS would maintain its one-dimensional structure and yield adequate reliability, as it has in previous studies already mentioned. Additionally, we evaluated the criterion validity of the CAS by examining score correlations with another measure of generalized anxiety. We expected that CAS scores show positive and significant relationship with a measure of generalized anxiety, as it has been reported in previous scientific literature (Ahmed et al., 2020; Caycho-Rodríguez, Vilca, Peña-Calero, et al., 2022; Padovan-Net et al., 2021).
Method
Design and Participants
This study is a secondary analysis of Salvadorans who are mourning the loss of a loved one to COVID-19. The purpose of the original study was to identify factors that predict dysfunctional grief, while this study is focusing on the psychometric features of the CAS (Lee, 2020). This study used a retrospective design (Ato et al., 2013) and a non-probabilistic snowball recruiting strategy to obtain participants. The participants were Salvadorans of legal adult age, who lost a loved one to COVID-19 and who gave their informed consent to be part of the study. The Soper (2020) software was used to create structural structure models (SEM) with the data obtained for this study. When we considered the number of observed variables (five items in the case of CAS) and latent variables (one latent variable, anxiety due to COVID-19), the size of the anticipated effect (lambda = 0.1), the desired probability (0.05), and statistical power (0.95), our sample of 435 Salvadorans exceeded the minimal requirement of 100.
Instruments
Coronavirus Anxiety Scale (CAS, Lee, 2020). The CAS was developed to measure physiological symptoms of dysfunctional anxiety generated by thoughts or reminders of the coronavirus. The CAS is made up of 5 items with five response options, ranging from not at all = 0 to almost every day = 4. Participants answered how often they experienced anxiety symptoms during the last two weeks prior to the application of the survey. The total score of the CAS ranges from 0 to 20, where a higher score expresses a higher frequency of anxiety symptoms due to COVID-19. In this study, the Spanish version validated by Caycho-Rodríguez, Vilca, Carbajal-León, et al. (2022) and which has demonstrated adequate psychometric properties and measurement invariance in 12 Latin American countries, including El Salvador (Caycho-Rodríguez, Valencia, et al., 2022).
General Anxiety Disorder-2 (GAD-2; Kroenke et al., 2007). The GAD-2 assesses two central symptoms of anxiety according to the DSM-IV. The two items that make up the GAD-2 are “how often did you feel nervous, restless, or on edge?” and “How often did you feel like you couldn't stop worrying or couldn’t control the worry?” Participants answered how often they had experienced these symptoms in the last 2 weeks. Response options were “0 = Never,” “1 = Several days,” “2 = More than half the days,” and “3 = Almost every or every day.” The total score of the GAD-2 is obtained from the sum of the scores of each of its items. This results in scores ranging from 0 to 6, with a higher score indicating a higher frequency of anxious symptoms. In this study, the Spanish version of the GAD-2 used by Caycho-Rodríguez, Valencia, et al., 2021) was used, which has shown adequate reliability and significant relationships with pandemic bereavement. For this study, the reliability was acceptable (α = .88).
Pandemic Grief Scale (PGS, Lee & Neimeyer, 2022). The PGS is made up of five items that measure the symptoms of dysfunctional grief due to the death of a loved one by COVID-19. Participants rated how often they experienced each of the grief symptoms (e.g., “I found it difficult to have positive memories of the deceased”) based on four response options (0 = not at all to 3 = almost every day). The total score ranges from 0 to 15, where a higher score indicates a higher frequency of symptoms of dysfunctional grief due to COVID-19. In addition, scores less than 7 would indicate the presence of non-dysfunctional grief, while a score greater than 7 indicates that grief is dysfunctional with clinical relevance. This study used the Spanish version of the PGS, which has adequate psychometric evidence in a group of Latin American countries, including El Salvador (Caycho-Rodríguez, Vilca, et al., 2021). The reliability, using the internal consistency method, of the PGS in this study was .92.
Procedure
The study received approval from the Institutional Committee for the Protection of Human Subjects in Research (CIPSHI) of the University of Puerto Rico (No. 2223-006). After that, we developed an online survey on the Google Form platform, which was administered to the study participants. Data collection took place between February and April 2021. We distributed the online survey link in El Salvador through different social media platforms and email. The participation was voluntary and the participants consented before answering the questionnaire. The study followed the recommendations of the Declaration of Helsinki of 1975. The confidentiality and anonymity of all participants was guaranteed. In addition, we informed the right of the participants to withdraw at any time.
Data Analysis
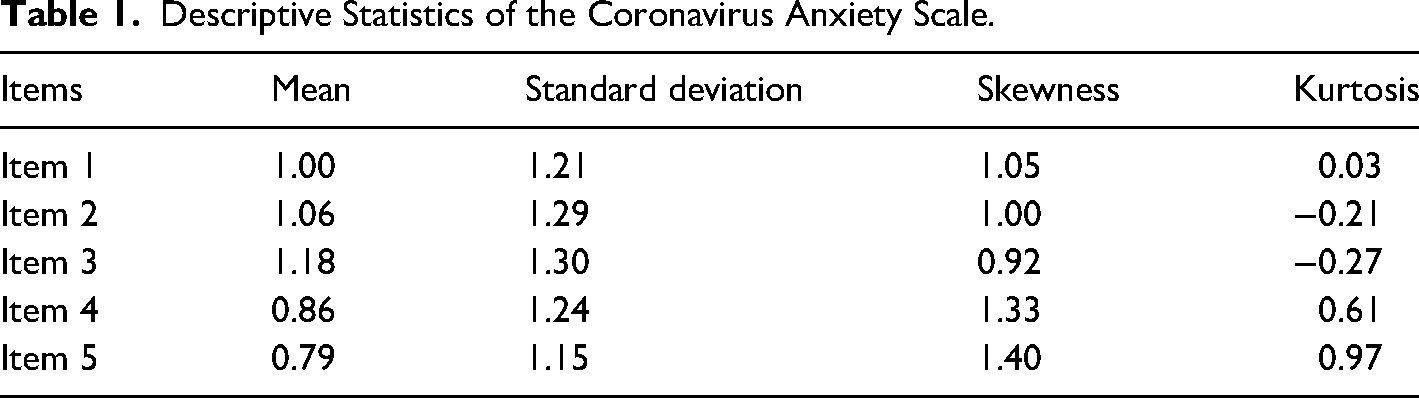
First, we calculated the descriptive measures to describe the characteristics of the study participants and the CAS items. Continuous data were reported as means (M) and standard deviations (SD); whereas, categorical data was reported as frequencies and percentages. The skewness and kurtosis values of the CAS items were also calculated. Values less than +/− 1 suggest the absence of violations of normality (Tabachnick & Fidell, 2013). The factorial structure of the CAS was evaluated using confirmatory factor analysis (CFA). For this, the robust maximum likelihood estimator (Brown, 2015) was used. The fit indices of the CFA considered were the Chi-squared test (χ2), the comparative fit index (CFI), the Tucker–Lewis index (TLI), the root mean square error of approximation (RMSEA) and the root mean square residual (SRMR). CFI and TLI values greater than .90 indicate an acceptable fit, while values greater than .95 are indicative of a good fit. Likewise, RMSEA and SRMR values less than .10 indicate an acceptable fit and values less than .05 indicate a good fit (Hu & Bentler, 1999; Schumacker & Lomax, 2015). The reliability of the CAS was estimated by calculating the Cronbach’s alpha coefficient and the omega coefficient, where values greater than .70 are considered adequate (Viladrich et al., 2017). The confidence intervals of the Cronbach’s alpha and Omega coefficient were calculated as recommended by Caycho-Rodríguez (2017a) and Ventura-León, (2017). Measurement invariance was evaluated at the configurational, metric, scalar, and strict levels. The difference of the CFI (ΔCFI ≤ 0.01) was used as a criterion for the rejection or acceptance of invariance (Chen, 2007). Finally, the correlation between the CAS and GAD-2 scores was explored using Pearson's product-moment test (r) where r < .30 was a weak correlation, r = .30–.59 moderate and r ≥ .60 strong (Andresen, 2000). Additionally, the confidence interval of r was calculated according to those suggested by Caycho-Rodríguez (2017b).
Results
Descriptive Statistics
The sample of 435 Salvadoran adults is composed by 165 (37.9%) men, 268 (61.7%) women, one non-binary person (0.2%), and one transgender person (0.2%). The overall mean age was 29 years (SD = 8.75). Based on the presence of pandemic grief, 153 (35.2%) have dysfunctional pandemic grief and 282 (64.8%) showed non-dysfunctional pandemic grief. Regarding residence, 338 (77.7%) are from the urban area and 97 (22.3%) belong to the rural area. Depending on whether they suffer from a chronic disease, 58 (13.3%) do suffer from a chronic disease, while 377 (86.7%) do not. Finally, Table 1 details the descriptive statistics of the CAS items, which have adequate values in the mean, standard deviation, skewness, and kurtosis.
Descriptive Statistics of the Coronavirus Anxiety Scale.
CAS Factorial Structure and Reliability
Both in the group of people with dysfunctional grief and without dysfunctional grief, two factorial models were tested: (1) a one-dimensional model made up of the five original items (Lee, 2020) that has already been validated in Latin American samples (Broche-Pérez et al., 2022; Caycho-Rodríguez, Vilca, Carbajal-León, et al., 2022); (2) one-dimensional model made up of four items (excluding item five of the original model) that has been validated and demonstrated measurement invariance in a sample of 12 Latin American countries (Caycho-Rodríguez, Valencia, et al., 2022). The AFC indicated that, both in the group of people with dysfunctional grief and in the group without dysfunctional grief, the four-item model presents better fit indices compared to the original CAS model. In this sense, the four-item model will be used for subsequent analyses. To verify the fit indices obtained, see Table 2.
Goodness-of-Fit Indices of Two Models of the Coronavirus Anxiety Scale in Salvadorans Who Present Dysfunctional (n = 153) and Non-Dysfunctional (n = 282) Grief.
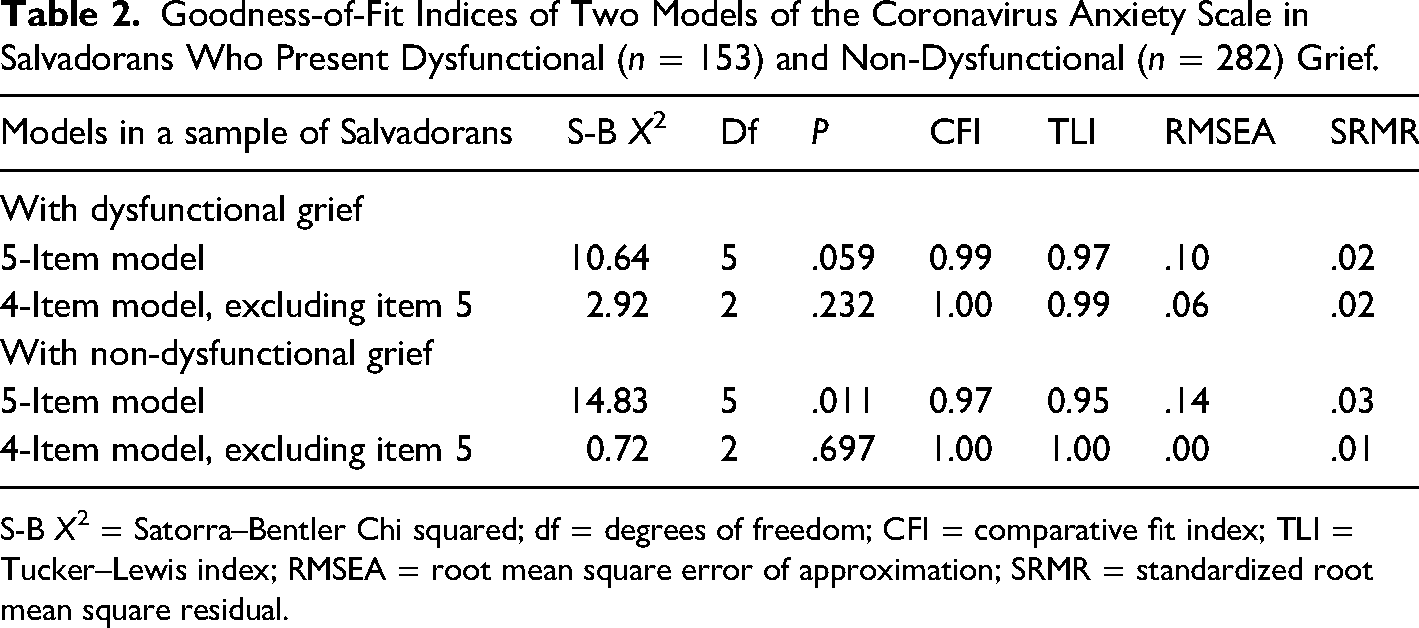
S-B X2 = Satorra–Bentler Chi squared; df = degrees of freedom; CFI = comparative fit index; TLI = Tucker–Lewis index; RMSEA = root mean square error of approximation; SRMR = standardized root mean square residual.
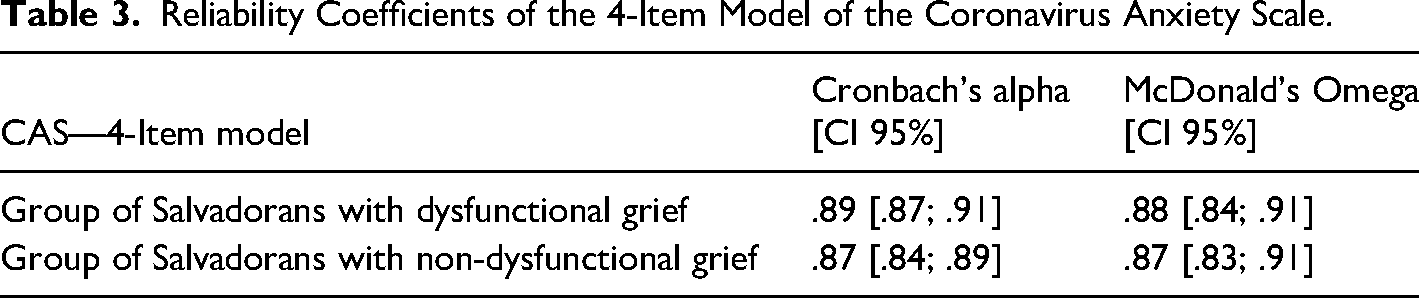
The Cronbach’s alpha and McDonald’s Omega values indicate very good reliability due to internal consistency in both study samples (Table 3).
Reliability Coefficients of the 4-Item Model of the Coronavirus Anxiety Scale.
Measurement Invariance
The goodness of the indices of the fit indices for the measurement invariance test of the four-item model in the different groups according to the presence or absence of dysfunctional grief and the variations in the CFI and RMSEA indices between the models are in Table 4. The factorial structure of the four-item CAS has shown evidence of metric invariance for the groups compared.
Invariance of the Coronavirus Anxiety Scale Depending on Whether or Not They Suffer From Dysfunctional Grief.
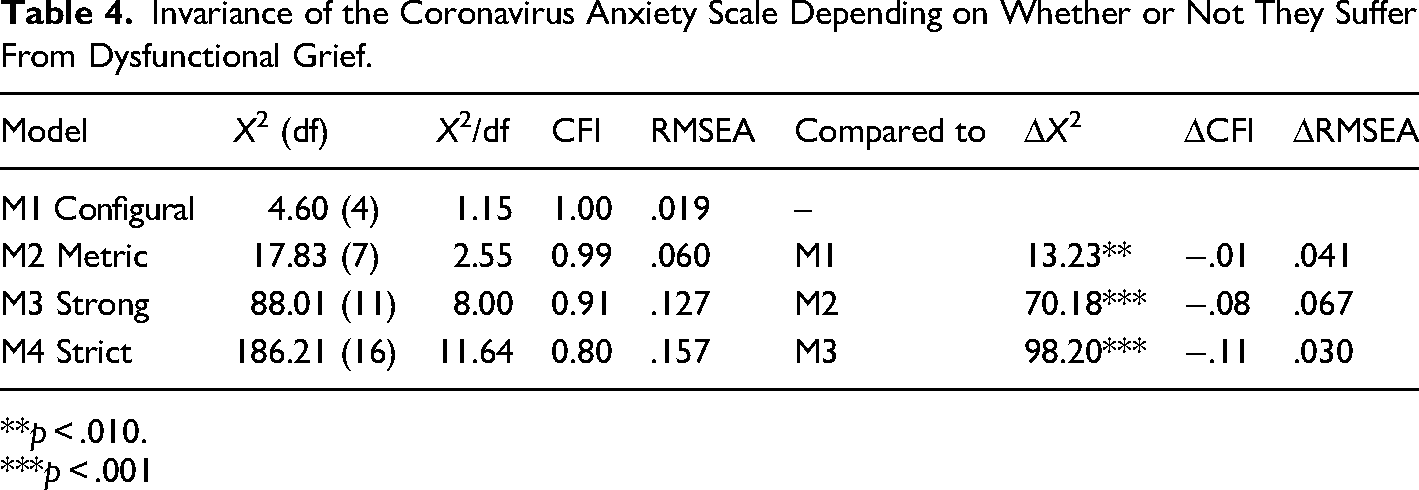
**p < .010.
***p < .001
Criterion Validity
Finally, the validity of the convergent criterion was evaluated using Pearson's r coefficient. As mentioned before, for interpretive purposes only the value of the Pearson correlation coefficient and statistical significance were used. Thus, a positive and strong correlation (r = .652; p = .001) was reported between the CAS and GAD-2 scores. This indicated adequate criterion validity.
Discussion
Coronaphobia is a pandemic-related phenomenon studied worldwide, so clinical work and research examining this mental health condition must have a valid and reliable measurement instrument that guarantees the absence of bias or measurement errors. Accordingly, the CAS (Lee, 2020) is important because it is a brief instrument that measures this specific type of pandemic-related anxiety and that has been validated in multiple contexts, including Latin America (Caycho-Rodríguez, Valencia, et al., 2022). Therefore, we carried out the present study with the purpose of verifying the measurement invariance of the CAS using a sample of Salvadoran adults with and non-dysfunctional levels of grief.
First, the original five-item CAS model did not show adequate goodness-of-fit indices. However, the four-item model suggested by Caycho-Rodríguez, Valencia, et al. (2022), which was shown to be invariant in 12 Latin American countries showed excellent fit indices, both in the group of Salvadorans with and without dysfunctional grief. This was similar to that reported in the general population of El Salvador (Caycho-Rodríguez, Valencia, et al., 2022). The four-item model had the elimination of item five that refers to stomach problems due to exposure to information about the pandemic. The study by Caycho-Rodríguez, Valencia, et al. (2022) eliminated item five as it showed residual correlations with item four (which also refers to digestive problems, specifically loss of interest in eating), which suggested the presence of possible similarities in the content of the items, task demands, measurement errors and response styles between items (Brown, 2015). The reliability findings of the four-item model of the CAS were also psychometrically sound in the groups of Salvadorans with and without dysfunctional grief. This finding is similar to what has been reported in other studies with a Latin American sample (Carrillo-Valdez, 2020; Caycho-Rodríguez, Valencia, et al., 2022). Taken together, the most appropriate CAS model for Salvadorans who have lost a loved one to COVID-19 and who do or do not present dysfunctional grief, is made up of four items referring to the physiological symptoms of anxiety due to COVID-19: dizziness, sleep disturbances, body immobility and loss of appetite.
Second, we verified that the four-item model of the CAS has metric invariance between the groups of people with or without dysfunctional grief. The presence of metric invariance indicates that the factor loadings are similar between people with and without dysfunctional grief and, therefore, assesses the degree to which the relationship between the items and the factor is identical between the groups. This implies that people with and without dysfunctional grief interpret and respond to the coronaphobia items in the same way. In addition, all four CAS items are important for both groups (Campbell et al., 2008). On a practical level, metric invariance will make it possible to directly compare the relationships between anxiety symptoms due to COVID-19 and other variables between people with and without dysfunctional grief. If there is no evidence of metric invariance, it is difficult to determine if the associations are different due to differences resulting from metric problems in the scale or true differences due to the presence or absence of dysfunctional grief in the associations. However, this finding differs from other studies where it has been shown that the CAS has strict, scalar invariance and even equal means depending on other sociodemographic characteristics such as age, sex and country of residence (Caycho-Rodríguez, Vilca, Carbajal-León, et al., 2022; Franco-Jimenez, 2020; Silva et al., 2020). However, it is important to note that verifying invariance based on whether the subject presents dysfunctional grief or not has not been studied before and therefore partial evidence, understood as the equivalence between groups of a subset of item parameters (Byrne et al., 1989), should be tolerated. Identification of non-invariant item parameters is done by reassessing the fit of the model after removing equality constraints for a single parameter, such as a factor loading. However, the presence of partial invariance is questioned, since it can significantly alter the construct being measured and limit meaningful comparisons of means between groups. Faced with these questions, it was decided not to prove partial invariance. Future research should examine the validity of these findings.
Additionally, we could see that the four-item version of the CAS has adequate criterion validity, finding large positive correlations with the GAD-2 scores. Despite the fact that the CAS measures physiological symptoms of anxiety and the GAD-2 measures cognitive and emotional symptoms, the correlation between both scales made it possible to verify that the four-item CAS does indeed measure symptoms of anxiety during the COVID-19 pandemic. This finding is similar to that reported in previous studies, which performed the same contrast and obtained a high positive correlation (Ahmed et al., 2020; Caycho-Rodríguez, Vilca, Peña-Calero, et al., 2022; González-Rivera et al., 2020; Padovan-Neto et al., 2021).
Limitations
The results must be interpreted considering some limitations. First, we used a non-probability snowball sampling to select participants with and without dysfunctional grief. Therefore, the sample was not necessarily representative of the general population of El Salvador grieving the death of a loved one. This leads to the need for future studies to use nationally representative samples to confirm the findings reported here. Second, the study did not assess the stability of the four-item version of the CAS over time. Therefore, future research should evaluate test-retest reliability of this instrument. Despite the fact that the findings showed that the four-item version of the CAS for Salvadorans with and without dysfunctional grief has adequate psychometric properties, these should be evaluated at different moments of the pandemic or post-pandemic. This is even more important given the evidence that mental health problems vary throughout the pandemic (Wang et al., 2020). Third, the use of self-report measures would mean that the results may be affected by social desirability. Thus, it would be advisable to evaluate anxiety due to COVID-19 objectively, even more so if the CAS measures physiological symptoms of anxiety.
Implications
People who experience the death of a loved one are at increased risk of anxiety symptoms, which are associated with the presence of distress and impairment and can be an obstacle to the normal grieving process (Horenstein & Charney, 2020). Therefore, having a measure with adequate psychometric properties, such as the four-item version of the CAS, may be useful as a suitable instrument for researchers and mental health professionals to assess the presence of anxiety symptoms and their psychological and physiological impacts in vulnerable people with and without dysfunctional mourning for the death of a loved one by COVID-19. Anxiety symptoms are treatable, and effective intervention is just as important when they occur after bereavement as when they occur at any other time (Shear & Skritskaya, 2012). There is some evidence to suggest that the presence of treatments to reduce anxiety symptoms may be effective in improving grief management (Marques et al., 2013). However, little is known about the proper course and treatment of anxiety during bereavement (Horenstein & Charney, 2020). In this regard, investigators could use the four-item version of the CAS as an outcome measure within intervention studies. That is, the scale can be used in studies with pre-post test designs to assess the effectiveness of an intervention that reduces anxiety in people who have experienced the loss of a loved one.
On the other hand, little is known about the mechanisms or risk factors of anxiety during bereavement (Horenstein & Charney, 2020). Thus, the four-item version of the CAS could be used as a measure within a structural model that would allow information to be obtained to understand the underlying mechanisms of anxiety symptoms during grief. Knowing the risk factors for anxiety during bereavement would guide clinical care and contribute to developing more efficient specific interventions. In this way, from a theoretical perspective, the results would allow us to have a measurement tool that can be used in studies that examine how other individual factors can determine the experiences of bereavement due to COVID-19 (Breen et al., 2022; Lobos-Rivera et al., 2023) which add to the scientific literature on the antecedents and consequences of mourning the death of a loved one (Burke & Neimeyer, 2013; Lobb et al., 2010; Mason, Tofthagen & Buck, 2020). In addition, carrying out this study with people with and without dysfunctional grief due to the death of a loved one expands the scientific knowledge of CAS at an international level.
Conclusion
The findings allow us to conclude that the four-item version of the CAS is a unidimensional scale with adequate reliability. Likewise, this version of the CAS is invariant at the metric level, which would make it possible to directly compare the relationships between symptoms of anxiety due to COVID-19 and other variables between people with and without dysfunctional grief.
Footnotes
Author Contribution
MEL-R, WCM-C and TC-R, provided initial conception, organization, and main writing of the text. MEL-R and LWV analyzed the data and prepared all figures and tables. ShAL, JCTR, ANF-M, PDV, CC-L, JT and MR-B were involved in data collection and acted as consultants and contributors to research design, data analysis, and text writing. The first draft of the manuscript was written by MEL-R, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Code Availability
Does not apply.
Consent for Publication
Does not apply.
Data Availability Statement
The database is available with a request to the corresponding author.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Universidad Privada del Norte (Registration number: 20213002).
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.