
Abstract
Objectives:
To evaluate the effects of maxillary anterior segmental distraction osteogenesis (MASDO) in patients with cleft lip and palate (CLP) and to identify risk factors for increased relapse.
Design:
A retrospective study.
Patients:
Thirty-one Japanese patients with CLP who underwent MASDO were eligible for study inclusion.
Main Outcome Measures:
We evaluated lateral cephalograms obtained before (T1), at 3 months (T2), and at 1 year (T3) after MASDO, and measured changes from T1 to T2 (δT1T2), from T2 to T3 (δT2T3), and from T1 to T3 (δT1T3). We also evaluated the risk factors associated with an increased relapse.
Results:
Overall (δT1T3), MASDO improved retrusion of the maxilla. We measured a significant advancement (6.1 mm) of the anterior maxillary segment in δT1T2 (A-McNamara classification) and increases in the overjet and the SNA, ANB, and nasolabial angles. However, skeletal relapse was evident in δT2T3, and the median percentage of relapse was 10%. To explore the risk factors, we subdivided patients with a δT1T2 of >5 mm into 2 groups based on the percentage of relapse (>15% vs ≤15%). There were significant differences between these groups in the vertical positions of the anterior nasal spine and point A, and the angle formed by the SN and palatal planes (SNPP), suggestive of intraoperative counterclockwise rotation of the maxilla.
Conclusions:
MASDO is effective for correcting midfacial deficiencies, but counterclockwise rotation of the maxilla during surgery may cause relapse.
Introduction
The incidence of cleft lip and palate (CLP) in Japan is relatively higher than the global incidence, with 1 in 495 to 695 live births as compared with 1 in 1008 live births, respectively (Natsume et al., 2000; IPDTOC Working Group, 2011). Patients with CLP tend to have various degrees of deformities to the maxillary dental arch, including class III malocclusion and maxillary constriction with a collapsed arch form, caused by reduced maxillary growth in a transverse and anteroposterior direction as a result of scarring of the soft tissue (palatal mucosa and palate muscles) and the cleft itself (Wada and Miyazaki, 1976; Mars et al., 1987; Mars and Houston, 1990; Scolozzi, 2008; Paradowska-Stolarz and Kawala, 2014). Although patients with CLP usually receive treatment early with a class III protraction facemask, approximately 10% to 25% of patients with CLP require additional orthognathic surgery to correct anteroposterior skeletal issues after growth (Cohen et al., 1995; DeLuke et al., 1997; Schnitt et al., 2004). Previously, maxillary advancement was achieved through LeFort I osteotomy (Posnick and Dagys, 1994). However, in recent years, total maxillary distraction osteogenesis (total DO) has gained popularity for the correction of severe maxillary hypoplasia (Scolozzi, 2008), as it coordinates a controlled normal healing process between surgically osteotomized bone segments. Total DO uses LeFort I as a bone cutting line and leads to a gradual advancement of the whole maxilla. As such, total DO offers greater stability and fewer limitations in the amount and direction of advancement (Maegawa et al., 1998; Scolozzi, 2008).
One complication with the LeFort I osteotomy or total DO is that these techniques may pull the velum forward, potentially inducing velopharyngeal incompetence (VPI; Janulewicz et al., 2004), which can cause nasal resonance (hypernasality) and reduced speech intelligibility. To overcome the potential limitation in speech, our clinical team recently developed maxillary anterior segmental distraction osteogenesis (MASDO), a technique that facilitates the forward advancement of only the anterior maxillary segments without affecting the patient’s velopharyngeal function (Iida et al., 2007; Aikawa et al., 2010). This technique can also correct a flattened or collapsed arch (Aikawa et al., 2010; Hirata et al., 2016). Consequently, MASDO is a new alternative technique to conventional total DO or LeFort I osteotomy for use in CLP patients exhibiting suspected VPI after surgery and/or a flattened dental arch.
Previous studies have reported and discussed the effectiveness of MASDO in terms of its effect on speech (Iida et al., 2007; Aikawa et al., 2010); however, orthodontic considerations, such as surgical relapse with the need for overcorrection, have not been examined. Therefore, the objective of this study was to evaluate the long-term effects of MASDO in patients with CLP and identify risk factors for an increased percentage of relapse.
Materials and Methods
Patients and Surgical Intervention
We enrolled 31 consecutive Japanese patients with CLP (18 male and 13 female; mean age, 19.2 years; age range, 14-26 years) who underwent MASDO between 2005 and 2013 in our university dental hospital. The choice to use MASDO was decided by the surgeons and the orthodontists through a consensus, and it was performed in patients who presented with a class III malocclusion with potential VPI with or without collapsed arch form. The surgical procedure has been described previously (Iida et al., 2007; Aikawa et al., 2010).
The position of the distraction device was selected on the basis of the required movement of the transport segment. Linear advancement was achieved by activating the distractor positioned on the palate (Iida et al., 2007) (Figure 1A), whereas rotational movement of the segment was accomplished via asymmetric activation using 2 bilateral distractors (Aikawa et al., 2010; Hirata et al., 2016) (Figure 1B). After a 7-day latency period, the anterior segment of the maxilla was distracted forward by 0.5 mm twice a day (1.0 mm). To prevent unwanted upward movement of the segment because of soft-tissue tension, we supplemented orthodontic elastic protraction (250-350 g force) from the facemask in the transport segment during distraction. Where necessary, intermaxillary elastic traction was also used for minor corrections to the position of the segment. After distraction was completed, the anterior segment teeth were connected to the posterior segment of the molar with an orthodontic wire to fix the positions of the segments. During this procedure, the transport segment showed some mobility until new bone ossification was complete. Patient demographic characteristics (ie, sex, age, cleft type, and site of distraction device placement) are described in Table 1.
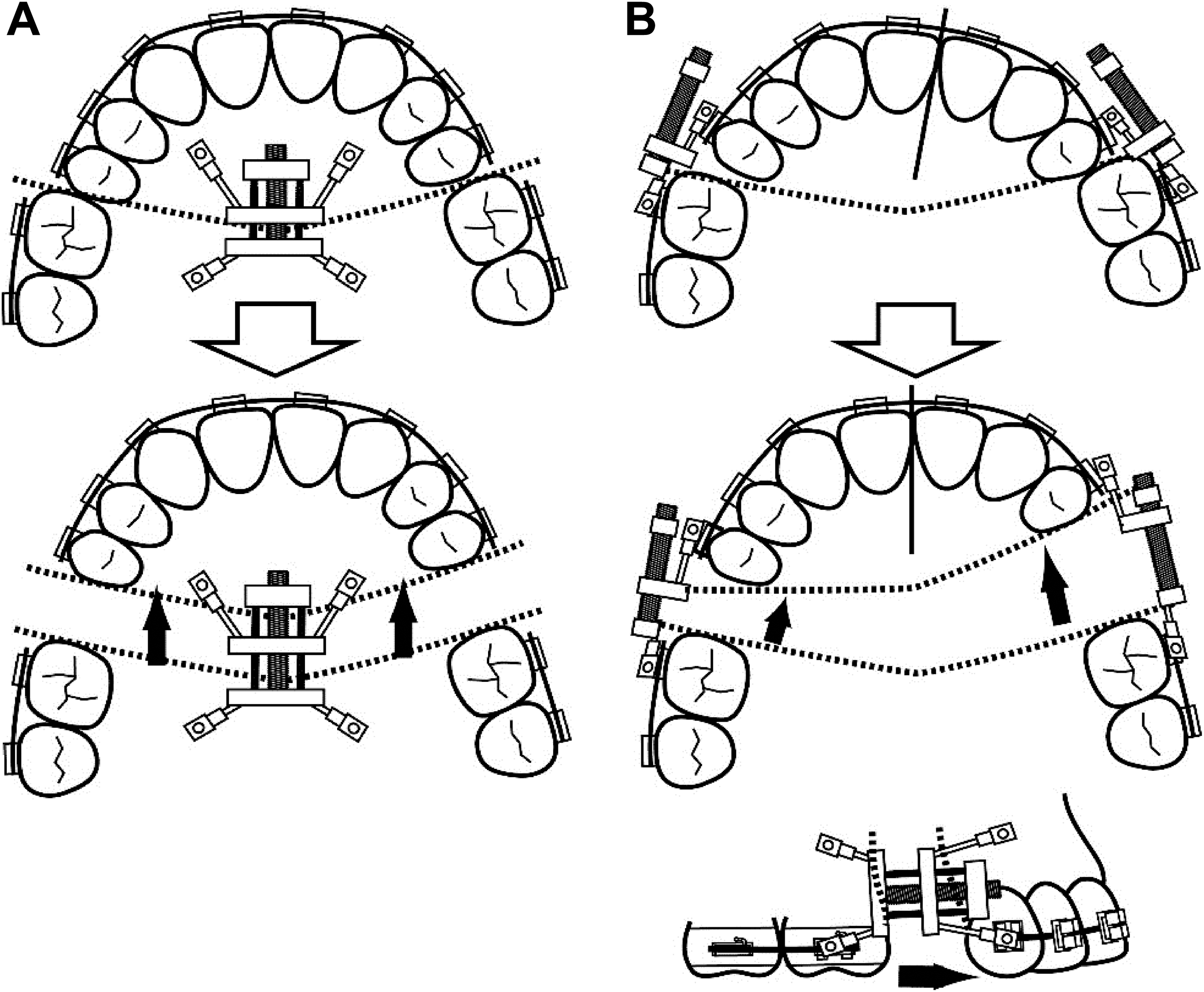
Palatal and buccal device for maxillary anterior segmental distraction osteogenesis (MASDO). (A) Linear advancement was achieved by activating the distractor positioned on the palate. (B) Rotational movement of the segment was obtained using 2 bilateral distractors via asymmetric activation.
Demographic Characteristics of the Patients With CLP Receiving MASDO and Those With Advancement of the Maxilla by ≤5 mm or >5 mm.
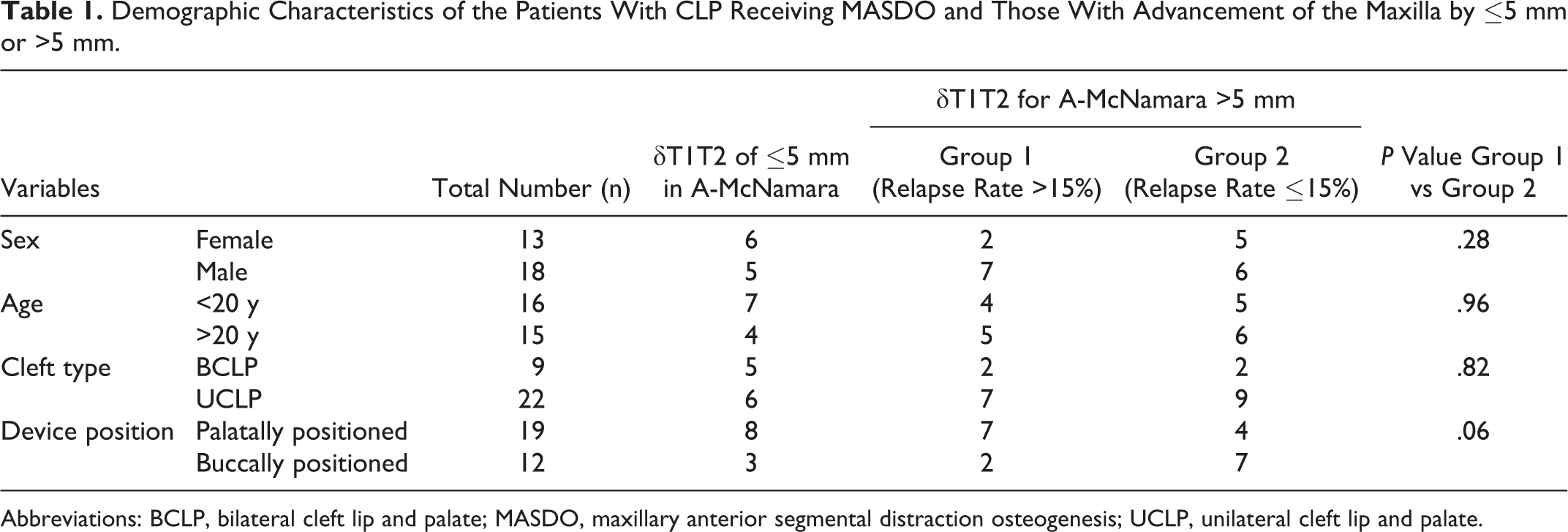
Abbreviations: BCLP, bilateral cleft lip and palate; MASDO, maxillary anterior segmental distraction osteogenesis; UCLP, unilateral cleft lip and palate.
Radiography, Data Collection, and Processing
Lateral cephalograms were obtained for each patient at a magnification ratio of 1:1.1, with the teeth in habitual maximum intercuspation and the lips in repose before (T1), at 3 (T2), and 12 months (T3) after MASDO.
Radiographs were overlaid with acetate paper and traced with a pencil. The consistency of tracings among T1, T2, and T3 was confirmed according to the methods of superimpositions advocated by the American Board of Orthodontics (Gu and McNamara, 2008). Fourteen anatomical landmarks (sella [S], nasion [N], orbitale [Or], porion [Po], anterior nasal spine [ANS], posterior nasal spine [PNS], point A [A], point B [B], menton [Me], gonion [Go], pterygomaxillary fissure [Ptm], pronasale [prn], subnasale [sn], and labiale superius [ls]) (Tanikawa et al., 2009) were visually identified, cross-marked by one of the authors (K.H.) and confirmed by another (C.T.). In the case of a disagreement in marking or landmark identification, the results were confirmed by a third author (T.Y.). Films with the traced papers were then digitized on a scanner (ES8500, EPSON, Tokyo, Japan) at a resolution of 300 dots per square inch to provide a traced image data set (2320 × 2960 pixels, 1 pixel = 0.085 mm). Using a computer mouse, one of the authors (K.H.) identified the anatomical landmarks for the traced image data on a computer monitor (24-inch pen tablet monitor, 1920 × 1200 dots, Cintiq 24HD; Wacom, Kazo, Japan). The images were analyzed at their actual size and then magnified to 150% of their original size. This process was repeated twice for all images, and the landmark coordinates from both digitization processes were averaged to provide the final landmark coordinates.
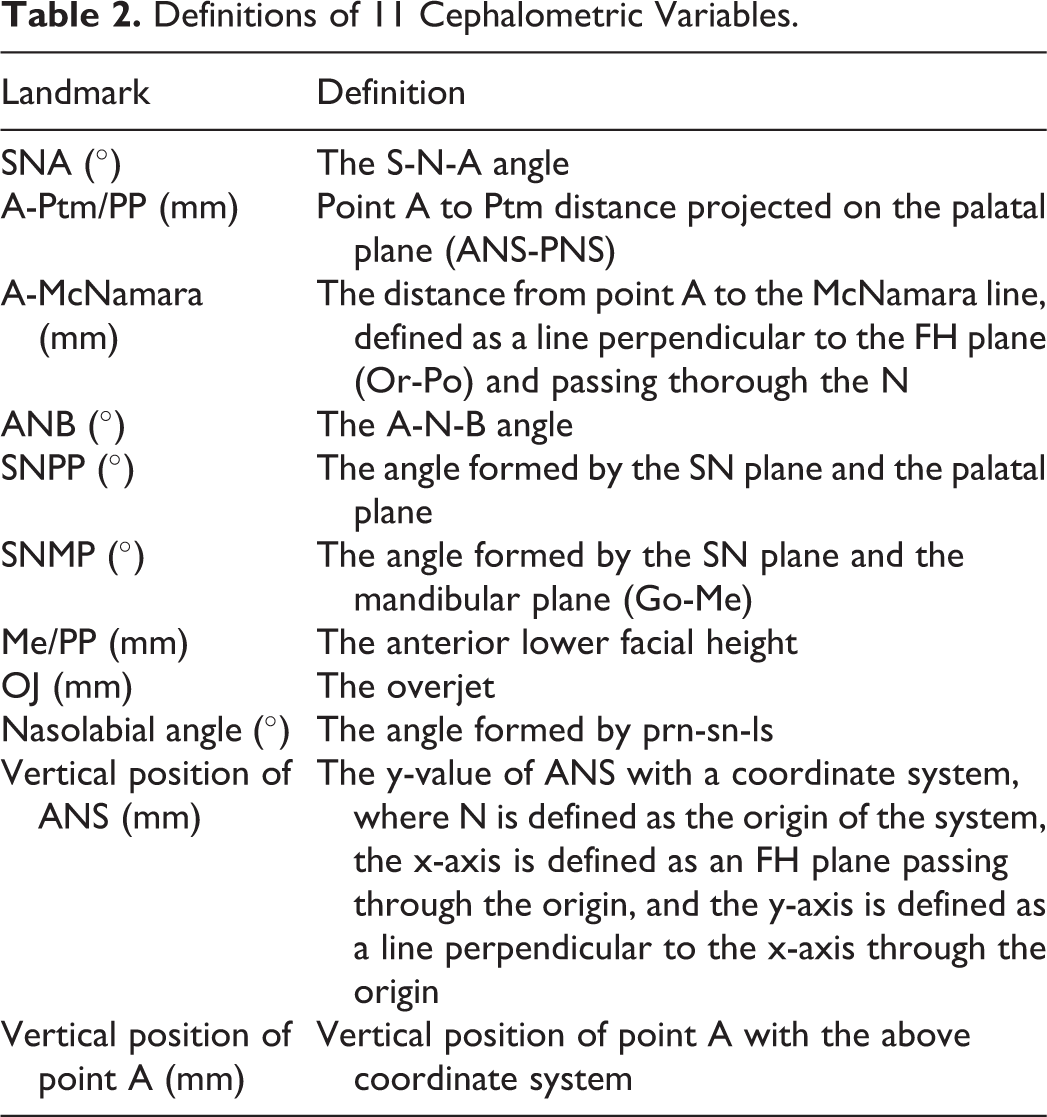
To determine the intraobserver reliability for landmark identification, traced pretreatment images of 6 participants were randomly selected and subjected to the digitization process 1 week later. On the basis of the landmark coordinates, 11 cephalometric variables (Table 2) were measured using a customized software program. All calculations were performed on a computer (MATLAB 7.12.0; MathWorks, MA).
Definitions of 11 Cephalometric Variables.
Soft-tissue profile changes after MASDO were also traced using a tablet pen (attached to the monitor, as described above), and the traced images provided a series of coordinates for the facial profiles (ie, semi-landmarks).
Statistics
A paired t test was used to calculate cephalometric changes from T1 to T2 (δT1T2), from T2 to T3 (δT2T3), and from T1 to T3 (δT1T3). The percentage of relapse was defined as the proportion of patients with a δT2T3/δT1T2 status according to the A-McNamara classification (McNamara, 1984), and the median percentage of relapse was calculated. To examine risk factors associated with an increased percentage of relapse, patients with a δT1T2 value of >5 mm in the A-McNamara classification were subdivided into 2 groups based on an arbitrarily defined threshold for relapse of >15% (group 1; greater relapse) and ≤15% (group 2; smaller relapse). The reason why we used patients with a δT1T2 value of >5 mm to examine relapse was that smaller relapse was estimated if the elongation distance was small; the threshold of 5 mm was chosen because the literature shows an average elongation of almost 10 mm by distraction (Figueroa et al., 2004; Harada et al., 2005; Wang et al., 2009; Daimaruya et al., 2010; ), and 5 mm is its 50% value. Further, the threshold value of 15% was chosen as it split the candidates into 2 groups of almost equal numbers. A 2-sample t test was performed for between-group comparisons for δT1T2, δT2T3, and δT1T3. A Kolmogorov-Smirnov test was used to confirm a normal distribution of the data. A P value of <.05 was considered statistically significant.
Demographic Factors Related to Relapse
To examine whether other demographic variables (ie, sex, age, cleft type, and distraction device position) were related to the incidence of relapse between the 2 groups, we used a test for equal or given proportions (P < .05) for each demographic variable (ie, male/female; age ≥20 years or <20 years; unilateral or bilateral cleft; buccally or palatally positioned distraction devices).
This study was approved by the ethics committee for medical research at Osaka University Dental Hospital (project ID: H28-E28).
Results
Intraobserver Reliability
The mean absolute landmark difference was 0.4 mm in both the x- and y-axes. These results are regarded as reliable to highly reliable (Aung et al., 1995).
Changes in Landmark Positioning
The average cephalometric landmark positions and soft-tissue profiles are shown in Figure 2A and are listed in Table 3.
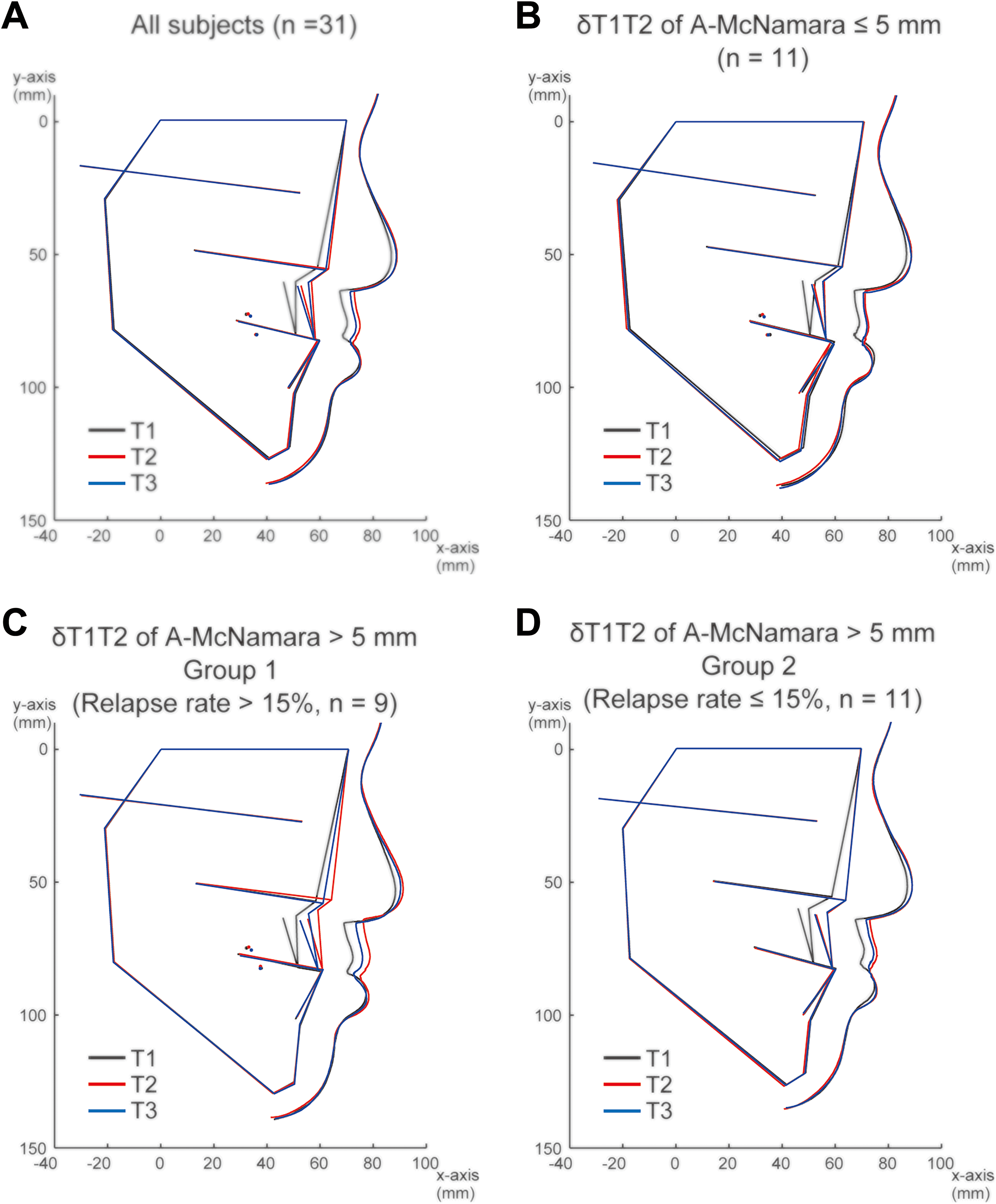
Mean configurations of the landmarks and soft-tissue profiles for all patients. (A) Patients with a δT1T2 value of ≤5 mm according to the A-McNamara classification. (B) Patients with a δT1T2 value of >5 mm according to the A-McNamara classification and relapse of >15% (group 1: C), and patients with a δT1T2 value of >5 mm according to the A-McNamara classification and relapse of ≤15% (group 2: D). The origin is denoted by N. The x-axis indicates the line parallel to the FH plane (Or-Po) passing through the origin; the y-axis is the line perpendicular to the x-axis through the origin. The black line denotes T1 (before surgery), the red line denotes T2 (at 3 months after surgery), and the blue line denotes T3 (at 1 year after surgery).
Mean and Standard Deviation (SD) for the Cephalometric Variables at Each Time Point and the Cephalometric Changes From T1 to T2 (δT1T2), T2 to T3 (δT2T3), and T1 to T3 (δT1T3).
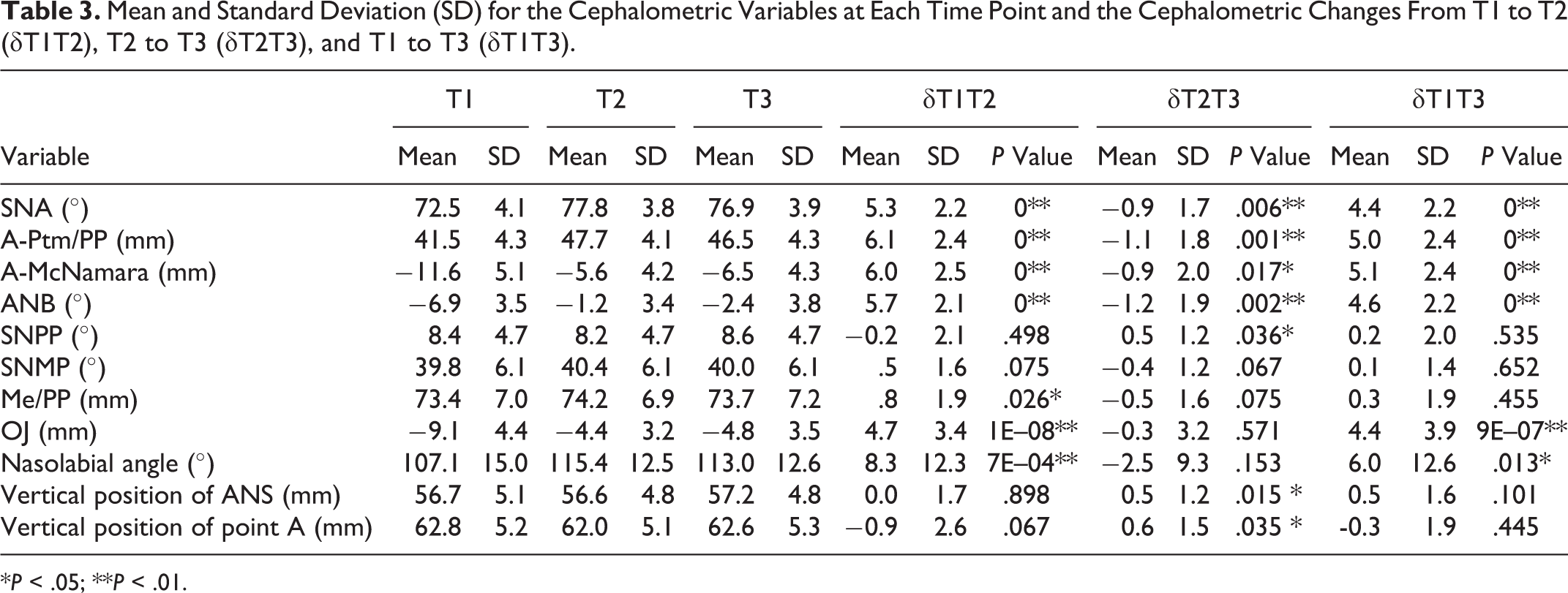
*P < .05; **P < .01.
From T1 to T2, we found that MASDO created a significant advancement in the anterior segment of the maxilla, with changes of 6.0 ± 2.5 mm (P < .01) and 6.1 ± 2.4 mm (P < .01) for A-Ptm/PP and A-McNamara, respectively. Statistical analyses also revealed increases in SNA, ANB, and OJ from the surgery over the first 3 months (P < .01). Qualitative evaluations of the soft-tissue profile changes indicated an improvement in the midfacial deficiencies, as determined by an elevated nasal tip and an increased nasolabial angle. We also found a significant increase in the nasolabial angle by 8.3° from T1 to T2 (Table 3).
However, skeletal relapse was evident, with reductions measured in A-Ptm/PP, A-McNamara, SNA, ANB, and OJ between T2 and T3. In addition, from T1 to T2, we observed a significant decrease in SNPP followed by the downward movement of the vertical positions of ANS and point A. This indicated a counterclockwise rotation of the maxilla after surgery, and this pointed to a possible cause of relapse.
Overall (δT1T3), MASDO improved retrusion of the maxilla in patients with midfacial deficiencies, with significant increases in measurements for SNA, A-Ptm/PP, A-McNamara, ANB, and OJ from T1 to T3 (P < .01).
Cephalometric Factors Related to Increased Percentage of Relapse
We next sought to evaluate the potential risk factors associated with this increased tendency for relapse. According to the A-McNamara classification, from T1 to T2, 11 patients showed advancement of the maxilla by <5 mm (Figure 2B), whereas 20 patients showed maxillary advancement >5 mm. We split these 20 patients into 2 groups based on the percentage of relapse, with 9 patients in group 1 (>15%, Figure 2C) and 11 in group 2 (≤15%, Figure 2D). The median percentage of relapse for the whole sample was 10% (interquartile range [IQR] = −6% to 27%), whereas those for groups 1 and 2 were 29% (IQR = 26% to 54%) and 2% (IQR = −7% to 10%), respectively.
To determine the possible predictors of relapse, we evaluated δT1T2 changes in the cephalometric values between the 2 groups (Table 4). We found a significant difference in the vertical positions of the ANS and point A, and the SNPP (P < .05) between groups 1 and 2, indicating that the counterclockwise rotation of the maxilla from T1 to T2 is related to an increased percentage of relapse from T2 to T3.
Mean and Standard Deviation (SD) for Risk Factors for Increased Relapse and the Cephalometric Changes From T1 to T2 in Groups 1 and 2.
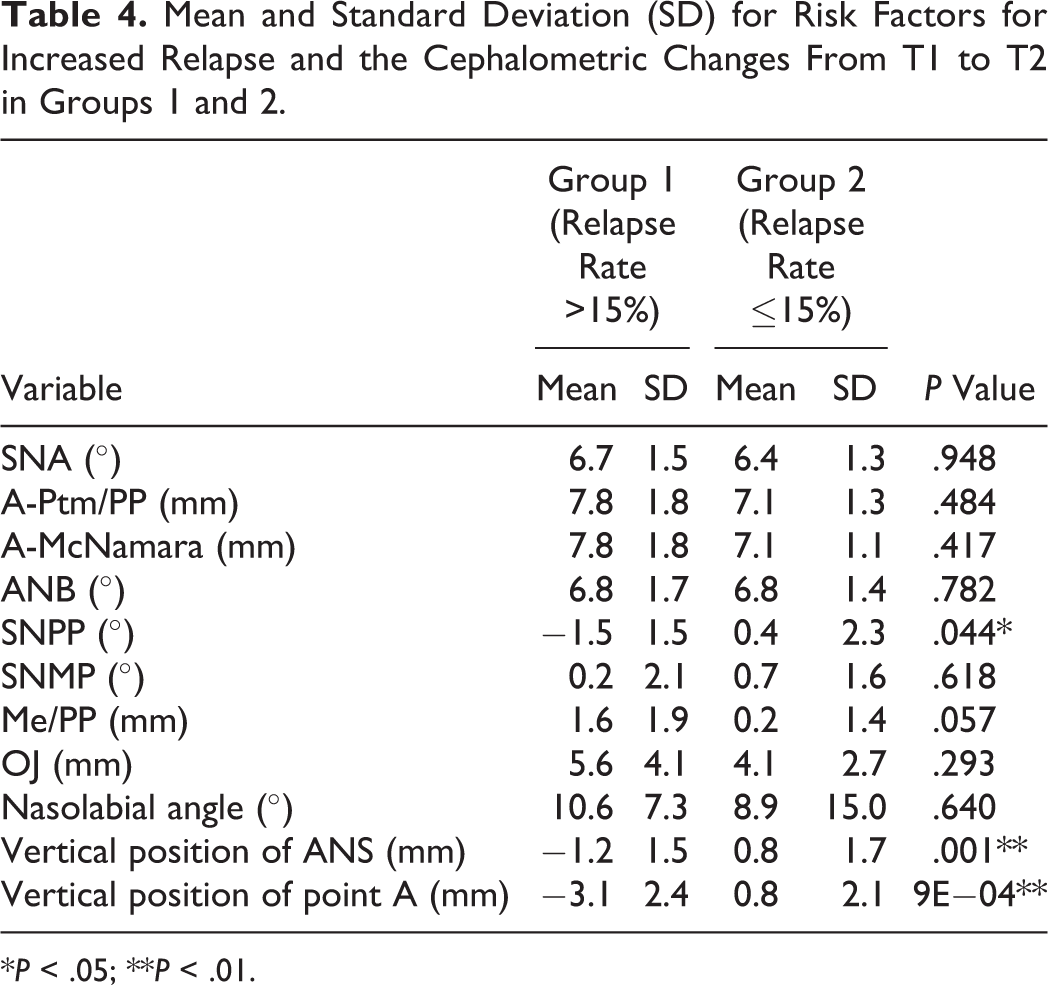
*P < .05; **P < .01.
Demographic Factors Related to Increased Percentage of Relapse
No significant demographic variables were related to the increased percentage of relapse (P > .05; Table 1). However, patients treated with palatally positioned distraction devices tended to show an increased percentage of relapse (P = .06; Table 1).
Discussion
Although our study had a limited sample size, this is the first report to statistically show that MASDO is effective for improving midfacial deficiencies in patients with CLP. Furthermore, we showed that the median percentage of relapse at 1 year after MASDO was 10% for the A-McNamara value, and this is comparable with or slightly less than the 13.7% relapse (SNA value) for patients treated with conventional total DO using a rigid external distractor (Sahoo et al., 2014). A review of patients treated with conventional Le Fort I osteotomy showed an average relapse of almost 30% (Saltaji et al., 2012). When we set an acceptable relapse limit of 30%, the proportion of patients within this limit in the present study was 84%. Thus, we may at least say that the relapse was smaller than that associated with conventional Le Fort I osteotomy. However, our relapse had a high IQR variation of −6% to 28%. To explore the reasons for this high variation, we stratified patients as having a smaller advancement (<5 mm), a greater advancement with an increased percentage of relapse (>5 mm, >15%), or a greater advancement with a decreased percentage of relapse (>5 mm, ≤15%). We found that the patients with increased relapse showed a significant intraoperative counterclockwise rotation of the maxilla compared with patients with smaller relapse (T1 to T2, P < .05). This result indicates that an increased percentage of relapse is related to counterclockwise rotation of the maxilla during surgery.
This counterclockwise rotation may be related to the position of the distraction device, that is, buccal or palatal (P = .06), during surgical intervention. At our hospital, MASDO is performed with either a single palatal distractor or 2 buccal distractors, and the position is chosen on the basis of the need for symmetrical or asymmetrical elongation: the use of 2 buccal distractors allows for asymmetrical elongation of the anterior segment of the maxilla by changing the elongation distance. Our results suggest that these differences in the position of the distractors may have led to the variation in relapse. Theoretically, we consider that the distractors—either 2 buccal distractors or a single palatal distractor—were placed below the center of resistance of the anterior segment of the maxilla, thereby generating the momentum required for vertical counterclockwise rotation. However, the use of 2 buccal distractors would make it more rigid and therefore better to resist vertical rotation. In other words, a total of 8 legs from the 2 buccal distractors placed approximately parallel to the plane perpendicular to the rotational axis of the anterior segment of the maxilla should be more rigid against the momentum as compared with a single palatal distractor placed parallel to a plane (Figure 1B).
To use buccally positioned distractors, patients must fulfill 2 requirements: that is, patients should have a large vestibular space and a large distance between the tooth roots for placing the distractors on both sides. If these 2 requirements can be fulfilled, we recommend that surgeons use buccally positioned distractors to avoid a greater relapse and the likelihood of counterclockwise rotation of the maxilla during elongation, even in patients with a symmetric maxilla.
We also suggest that surgeons check the degree of vertical rotation of the maxilla before removing the distractors. If counterclockwise rotation is observed, we recommend overcorrection of the elongation. Moreover, we suggest that orthodontists plan to move teeth in such a way that the overjet does not decrease in patients exhibiting such counterclockwise rotation. For this, the use of a temporary anchorage system would be effective.
Conclusions
The results of this study indicate that MASDO is effective for correcting midfacial deficiencies. The median percentage of relapse at 1 year after surgery is 10%, and this appears to be related to the counterclockwise rotation of the maxilla during surgery, possibly caused by placement of the distractors during surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.