
Abstract
This report describes a method to expand cleft segments of patients with cleft lip and palate prior to the secondary alveolar bone graft (ABG) using a reprogrammable nickel titanium expander. The expander can be reprogrammed with electric current to the desired width for each patient and delivers a gradual slow expansive spring force that expands and aligns the segments without further adjustments. Reprogramming the expander eliminates the need for multiple appliances and reduces chair time and patient appointments. The expander can be left in place during the ABG, because it does not interfere with a palatal flap. This alternative approach may be useful for patients who travel long distances to obtain cleft-related care.
Keywords
Introduction
Treatment of patients with a cleft lip and palate (CLP) requires a team approach with several dental and medical specialists (Pan et al., 2007; Yang et al., 2012; Raju et al., 2014). Orthodontic expansion as preparation for an alveolar bone graft (ABG) is an integral part of the treatment of patients with complete CLP. Most patients with CLP require differential expansion with more anterior than posterior expansion, as a result of the collapse of the cleft segments into the void of the alveolar cleft (Ross, 1970; Bardach, 1990; da Silva Filho et al., 1992; Aizenbud et al., 2012; Garib et al., 2014). The goal of the expansion is to regain the archform and coordinate the transverse dimension of the maxillary to the mandibular arch.
There is some debate over the optimal timing and type of appliance used for this orthodontic intervention. Traditional expansion appliances include various designs of the rapid palatal expander (RPE), the fan expander, and the quad-helix (QH) expander (Tindlund et al., 1993; Vasant et al., 2009; Aizenbud et al., 2012; Garib et al., 2014). Regardless of the appliance used, the displaced maxillary segments require a period of stabilization that usually consists of leaving the expander passively in place for 3 to 6 months in order to allow sutural reorganization and stabilization (Yang et al., 2012). This stabilization period is particularly important to prevent relapse in patients with CLP because the long-term stability may be affected by factors such as muscle strain, pressure of the surrounding musculature, palatal scar contraction, and rotation of bone segments (Isaacson and Murphy, 1964; Yang et al., 2012).
This report describes a NiTi expander (nickel–titanium expander; Ortho Organizers, Inc, San Marcos, California) that was reprogrammed with the Bender Soarer-X machine (Tomy Incor, Tokyo, Japan) by transmitting heat through electric current to customize the expansion to the individual needs of 2 patients with CLP. Different versions of the NiTi expander are on the market and have been used in patients with and without clefts around the world (Abdoney, 1995; Karaman, 2002; Ferrario et al., 2003; Donohue et al., 2004; CG et al., 2013; Raju et al., 2014). However, no previous author has reprogrammed the NiTi expander and individualized its expansion. The original reason for developing a programmable NiTi expander was to help a patient who lived far from our center to receive care by reducing the number of presurgical orthodontic visits needed to prepare the patient for an ABG. The programmable NiTi expander represented an attempt to problem-solve the particular needs of this family. This method for reprogramming the NiTi expander solved many of the drawbacks previously described with this technique as illustrated in this case series.
Case Description: Patient 1
Patient 1 is a 9-year and 5-month-old male born with complete unilateral cleft lip and palate (UCLP) who has been seen at the Children’s Hospital Los Angeles for all his medical and dental care. His past medical history included lip and palate repair in early infancy. Clinical examination revealed the presence of collapsed alveolar segments with a maxillary intercanine width of 23 mm, mandibular intercanine width of 26.5 mm, maxillary intermolar width of 38 mm, and mandibular intermolar width of 41 mm (Figure 1A–E and Figure 2A and B). The intermolar distance was measured at the maxillary palatal cusp and mandibular central grove, so the ideal measurements should be equal. The intercanine distance was measured at the center of the cusp tip and the desired upper distance should be 5 mm greater than the lower (Lindsten et al., 2002). It was decided that the patient needed 8.5 and 3 mm of orthodontic expansion in the canine and molar area, respectively, to regain the archform prior to the ABG surgery.

Patient 1 initial photos. A, Center view of the maxillary and mandibular arches in occlusion. B, Occlusal view of the maxillary arch. C, Occlusal view of the mandibular arch. D, Right lateral view of the dentition in occlusion. E, Left lateral view of the dentition in occlusion.
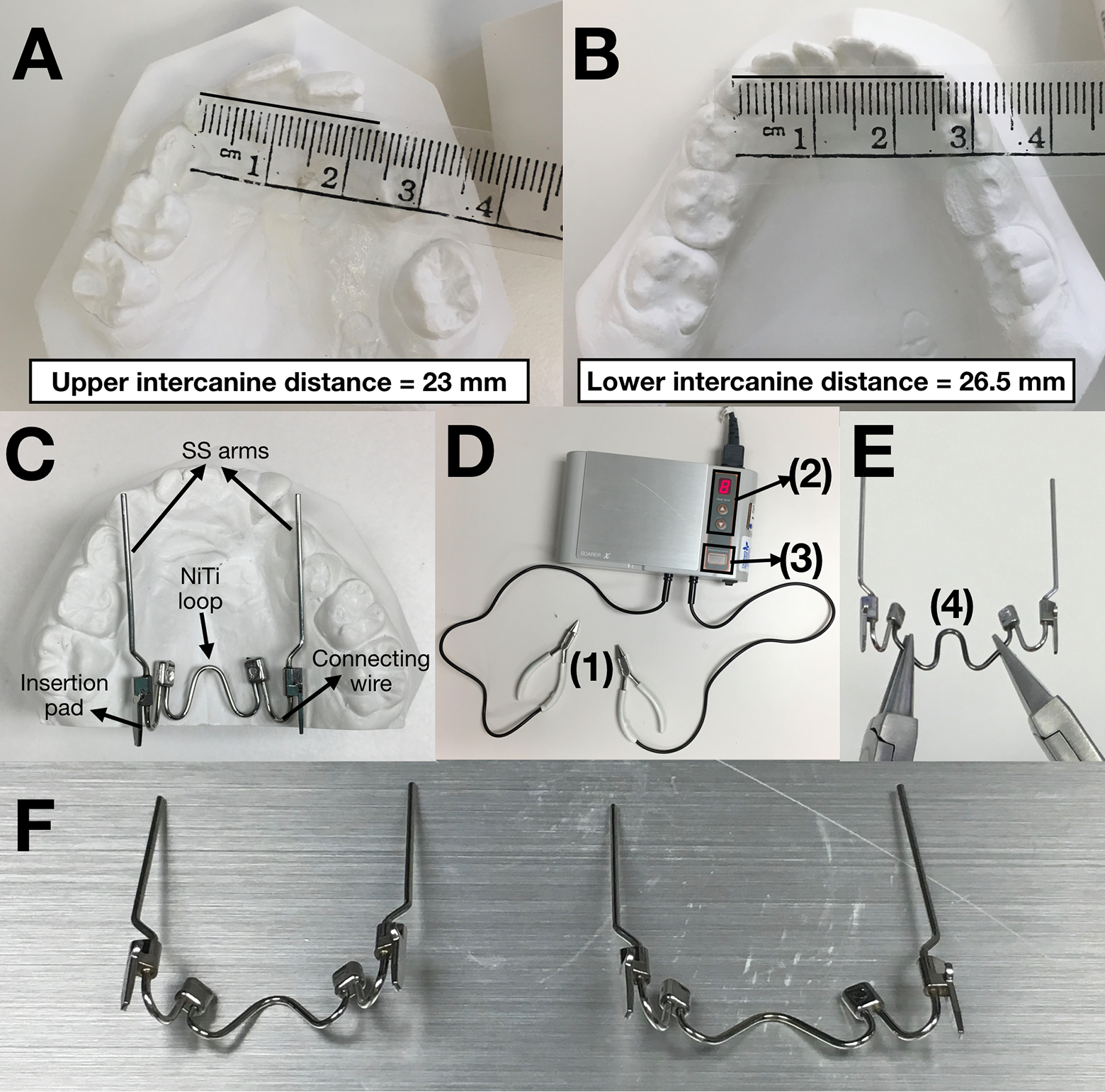
Reprogramming the nickel titanium (NiTi) expander. A and B, Measuring the models to determine amount of expansion needed. C, Small expander prior to being reprogrammed. Description of the expander: central 0.040″ nickel–titanium wire in form of a rounded W (NiTi loop) connected 0.036″ stainless steel (SS) wire arms that can be adapted to the dentition (Marzban and Nanda, 1999; Raju et al., 2014). The wire of the NiTi loop is curved up in the vertical plane as well, to follow the vault of the palate. Between the SS arms and the NiTi loop, there is an NiTi connecting wire that allows differential expansion. Where the SS arm and the connecting wire come together, there is a connecting pad with a hook and a rectangular blade that can be inserted in the lingual sheaths of the bands that the patient should have in the maxillary first molars. D, Bender Soarer-X equipment (Tomy Incor) with 2 pliers that transmit electric current (1), a panel to adjust the intensity of the current and heat level (2), and the infrared sensor that allows the current transmission (3). E, Pliers positioned in the NiTi section and ready to have the electric current transmitted to reprogram the expander. F, NiTi expander before and after being reprogrammed (left is before and right is after).
This patient illustrates the need for differential anterior expansion as the anterior part of the lesser segment collapsed into the void of the alveolar cleft. In this type of case, an RPE, which can only provide parallel expansion, could correct the intercanine distance but would overcorrect the molar position and result in overexpanded posterior segments (Holberg et al., 2007; Pan et al., 2007; Gautam et al., 2011; Aizenbud et al., 2012; Figueiredo et al., 2014; Ayub et al., 2016). Typically, a fan-type RPE, a spring-loaded expander, or QH appliance would be used to provide differential expansion. More recently, a twin-screw RPE was designed to provide differential expansion (Garib et al., 2014). However, all of these expanders require monitoring to determine whether the desired expansion was reached and they interfere with the surgical field. Therefore, we chose to use the reprogrammable NiTi expander (Figure 2C), as the appliance does not interfere with the surgical field and differential expansion can be programmed into it by reprogramming the expander with the Bender Soarer-X equipment (Figure 2D–F).
The process to reprogram and deliver the expander was as follows: after fitting bands, we welded lingual sheaths and cemented them on the first maxillary permanent molars. Selecting the size of the expander was not as critical as with the regular NiTi expander, since the dimensions would change once we reprogrammed it to the desired width. Using the models, the stainless steel (SS) arms were adapted to the lateral segments to follow the embrasures of the maxillary dentition. The expander was then reprogrammed with the Bender Soarer-X machine (Tomy Incor) to the desired final width individualized for this patient. To determine the desired arch width, we measured the maxillary intermolar and intercanine widths and compared them to the mandibular model for arch coordination (Figure 2A and B). When reprogramming the expander to the desired width, an additional overcorrection of 3 to 4 mm was added to compensate for relapse due to dental tipping as previously reported in the literature (Marzban and Nanda, 1999; Karaman, 2002; Donohue et al., 2004; Raju et al., 2014). To reprogram the appliance, the NiTi loop wire was held by 2 bird beak pliers in the corrected position and then the electric current was applied to the wire segment between the pliers. The Bender Soarer-X equipment transmitted heat to the NiTi wire loop through electric current (Figure 2D and E). The machine only transmits current to the appliance when the appliance is held by both pliers above the area of the infrared sensor (Figure 2D). The amount of current and applied heat level can be adjusted. We used setting number 8, which transmitted a current of 0.360 V and 0.4 µA, enough to reprogram the expander (Figure 2D).
Since the transverse discrepancy was smaller in the maxillary first molars, the expander had to be reprogrammed to provide more expansion in the area of the collapsed segments, without overexpanding the first molar area. This differential expansion was programmed by making a hinge-like rotation at the central NiTi loop and connecting NiTi wires while it was being reprogrammed. Because the lingual sheaths and the expander blades did not line up, the NiTi wires needed to be twisted to adjust for the inclination of the molars and allow a clearer path of insertion. Additionally, lingual crown torque was added to the insertion pads to counteract the buccal tipping of the molars and compensate for the expansion effect. The pads were twisted until they were parallel.
To deliver the expander, we inserted the pads into the lingual sheaths of the bands. Upon placing the expander, the appliance was active in the mouth. The appliance was reprogrammed and inserted in one visit. The expansion proceeded slowly and continuously until it reached the programmed limit at the final range of the expander. To determine whether the desired width had been achieved, the intercanine and intermolar distances were measured again clinically and compared to the goal measurements. The patient was seen 5 weeks after delivery to monitor the expansion and it was determined that the appliance was still active. The patient was seen again 5 weeks later (for a total of 10 weeks) and it was determined that the desired dimensions had been achieved. During this case, it was noted that unlike the QH appliance, the NiTi expansion was precise and self-limiting, eliminating the risk of overexpansion. Furthermore, there was no need for additional appointments to re-expand or adjust the alignment or expansion of the appliance. Also, the appliance was easier for patients to accept because there was no need for impressions as the bands were cemented first to ensure a good fit before the expansion component was added.
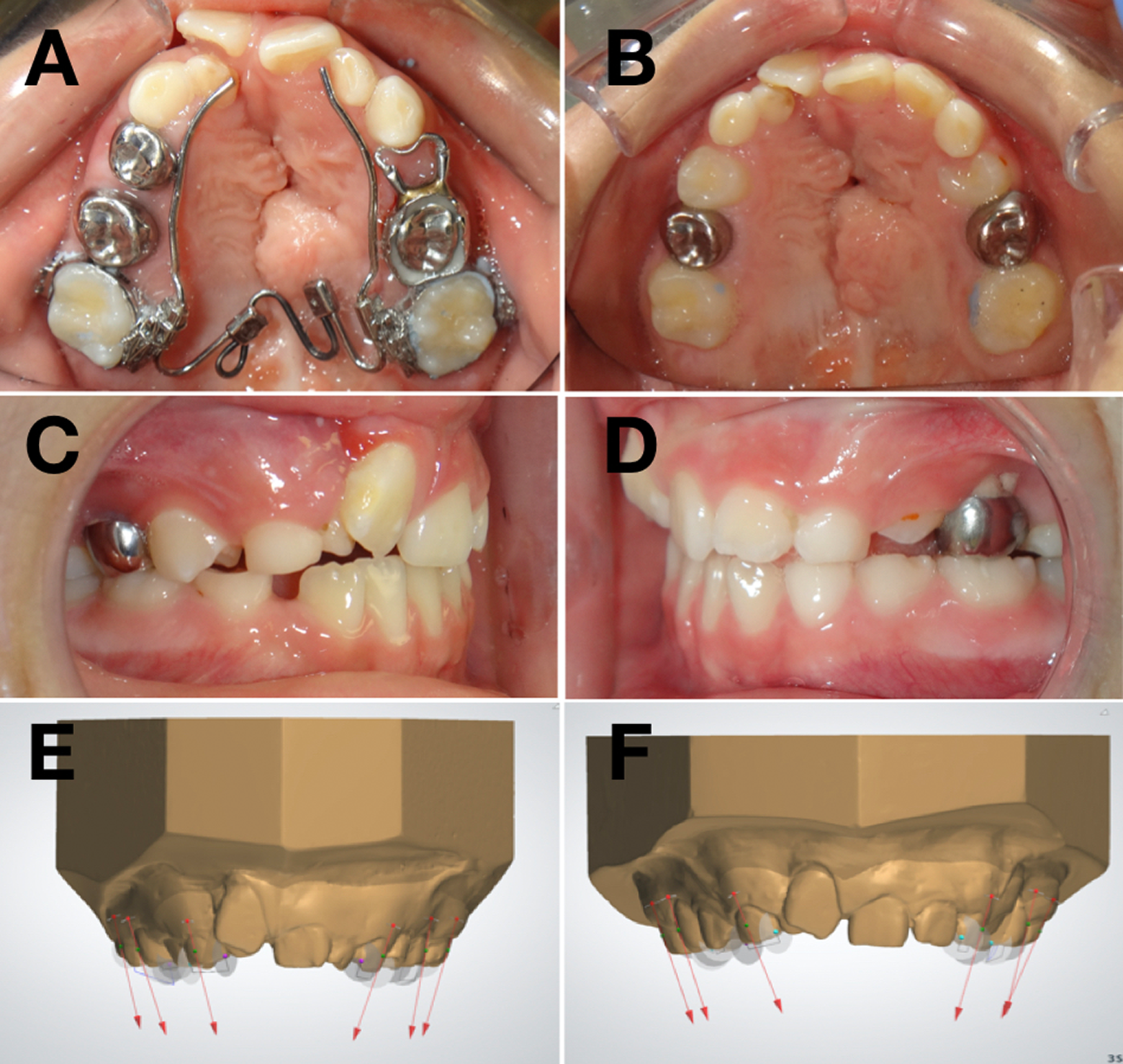
The patient was then referred to the oral surgeon for the ABG. Marzban and Nanda (1999) suggested a retention period lasting 50% to 100% of the expansion time. Because the NiTi expander does not interfere with the surgical field, removal of the appliance was not necessary prior to the ABG surgery, as it allows palatine flap access. This enabled a longer period of stabilization of the expansion without having to delay the surgery due to extra appliances or lack of palatine access. The expander remained in place during the ABG surgery and was removed 3 months after the surgery. Figure 3A shows the dentition the day of expander delivery and Figure 3B the day of expander removal. Note that the canine successfully erupted into the bone graft area. Figure 3C and D shows lateral views of the dentition the day of expander removal. Figure 3E and F shows the inclinations of the teeth to the occlusal plane before and after expansion. Note the inclination of the right first molar barely changed (from 78.93° to 77.50°), as the expander counteracted the buccal tipping effect of orthodontic expansion. The left first molar tipped lingually 14.08° (from 64.85° to 56.66° to the occlusal plane) thanks to the lingual crown torque added.
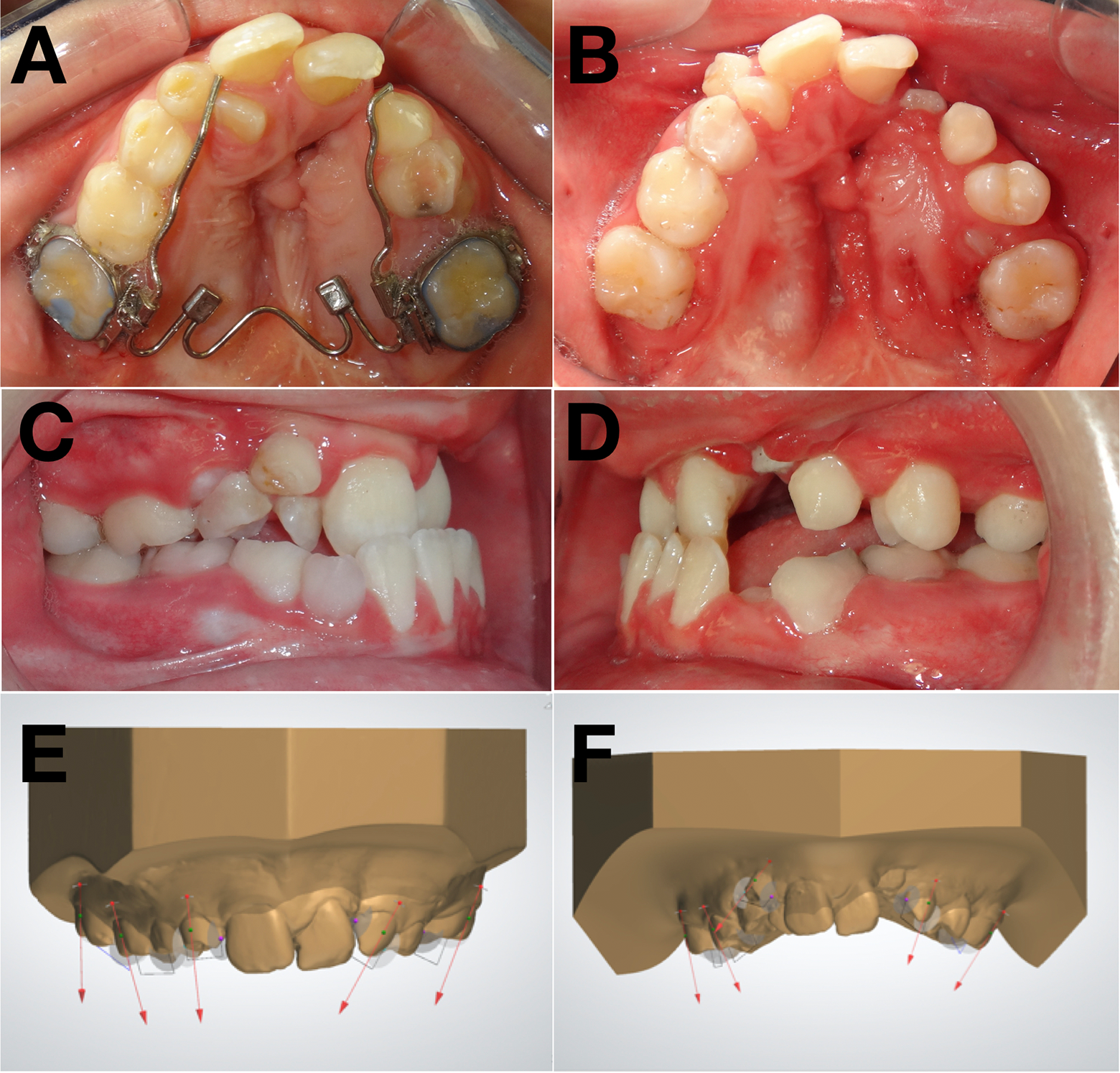
Patient 1. A, Occlusal picture at delivery of the programmed expander. B, Occlusal picture 3 months post alveolar bone graft (ABG) surgery, at expander removal. Note the maxillary left canine erupting into the bone graft area. C and D, Lateral views of the dentition in occlusion at expander removal. E, Digital models at initial showing the inclinations of the teeth. F, Digital models at expander removal showing the inclinations of the teeth.
Case Description: Patient 2
Patient 2 is an 8-year and 1-month old male born with complete UCLP and history of lip and palate repair in early infancy. Clinical examination revealed the presence of collapsed alveolar segments, with a maxillary intercanine width of 24 mm, mandibular intercanine width of 25 mm, maxillary intermolar width of 37 mm, and mandibular intermolar width of 39 mm (Figure 4A–E).
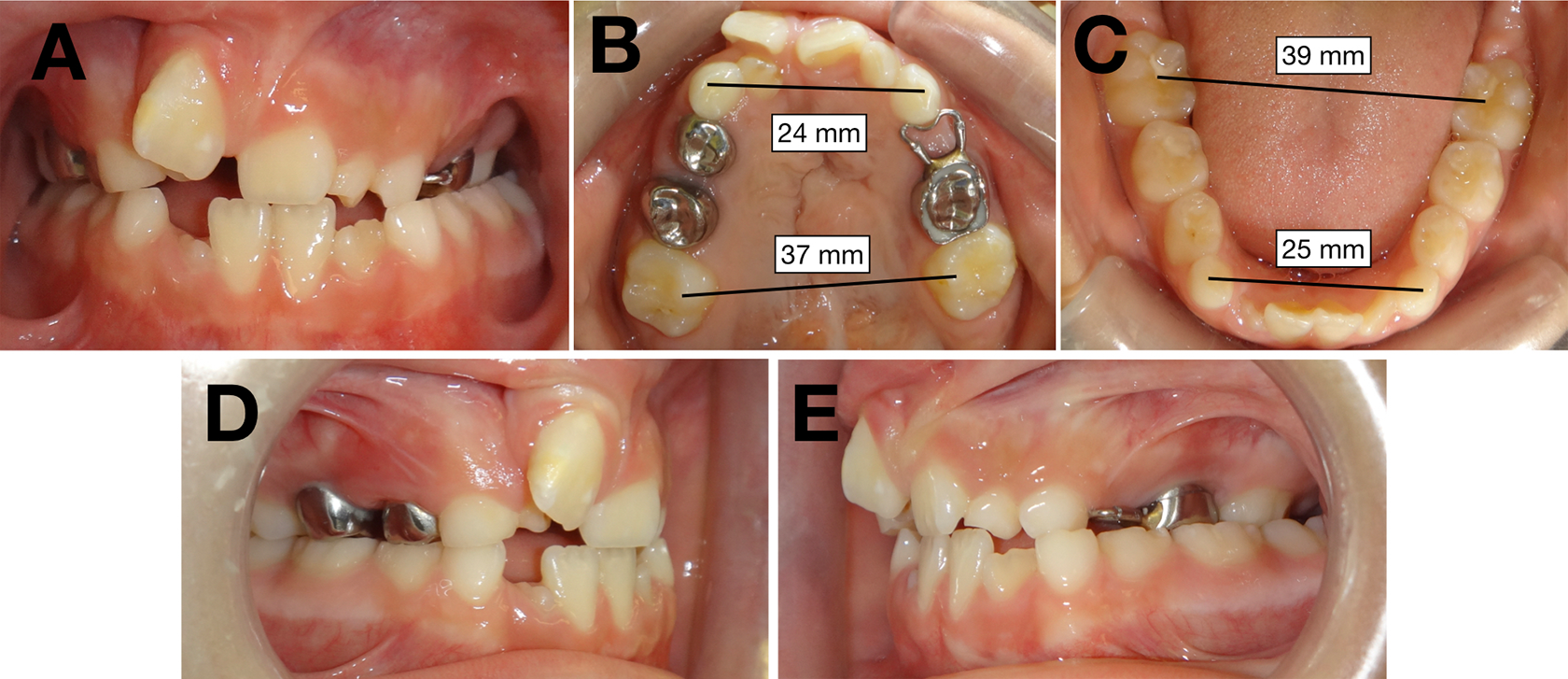
Patient 2 initial photos. A, Center view of the maxillary and mandibular arches in occlusion. B, Occlusal view of the maxillary arch. C, Occlusal view of the mandibular arch. D, Right lateral view of the dentition in occlusion. E, Left lateral view of the dentition in occlusion.
It was decided that the patient needed orthodontic expansion to regain the archform prior to the ABG surgery and the programmable NiTi expander was chosen for the same reasons as in the previous case. The expander was reprogrammed to the desired width of the dentition for this patient following the same method described for patient 1 and the total expansion time was 3 months. However, this patient had a flatter palatal vault, which resulted in a complication with impingement of the expander in the palatal tissue that was not observed in the previous patient (Figure 5A). The expander was therefore removed by cutting the transpalatal wire into curved segments that could be grasped with a plier and rotated out of the embedded tissue. The NiTi expander was replaced by a transpalatal arch (TPA) with steel arm extensions and the patient underwent the ABG surgery without incident.
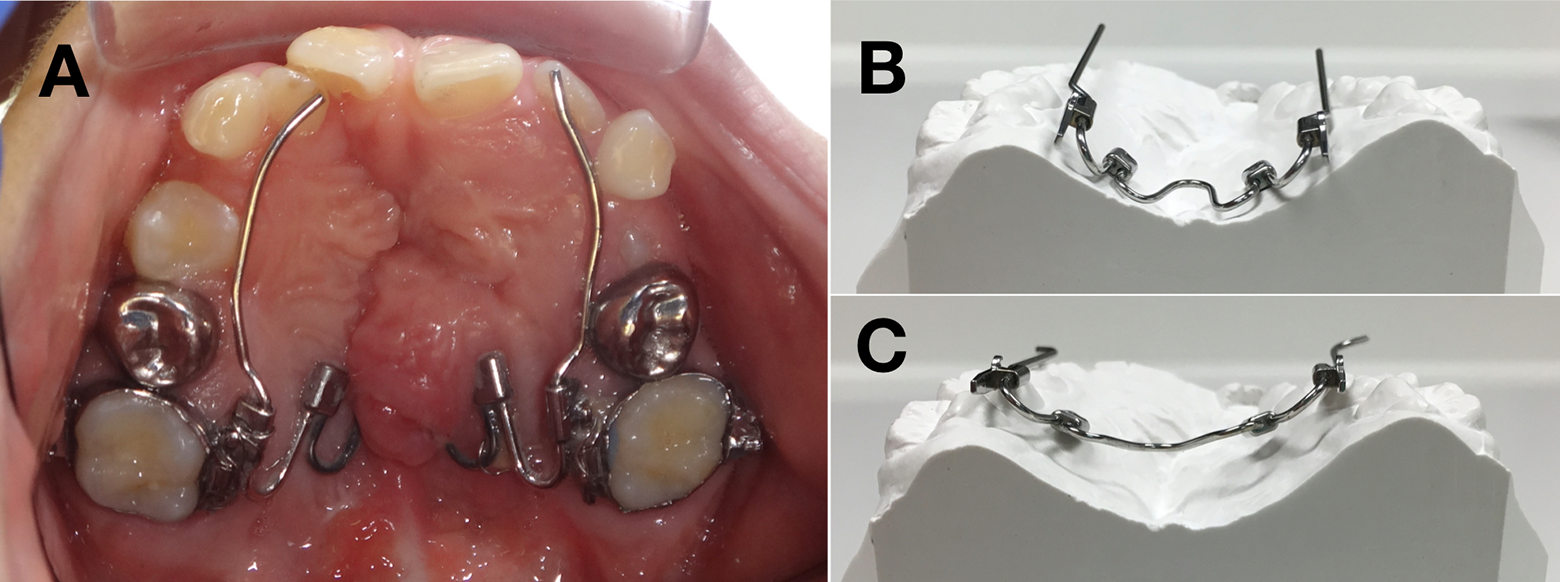
Patient 2. A, Complication: expander embedded in the palatal tissue. B and C, Posterior views from nickel titanium (NiTi) expander before and after being reprogrammed. Note the flatter configuration of the widened expander in image C.
Due to this complication, we learned that when selecting the size of the expander it is important to take into consideration the depth of the palate. Patients with CLP usually have a flatter palatal vault after palatal surgery, and therefore, an NiTi expander with a big activation can impinge the roof of the palate and embed in the palatal tissue. A considerably smaller size of the expander should be selected if the expander is going to be reprogrammed so that it will flatten as it is widened and impingement in the soft tissue of the palate can be avoided (Figure 5B and C). The smaller expander is reshaped in the outstretched position by reprogramming the NiTi wires with the Bender Soarer-X equipment (Figure 5B and C). Additionally, the expander should be checked at delivery for adequate initial clearance.
Figure 6 shows the dentition the day of expander delivery (A) and the day of removal of the TPA with arms (B-D). Figure 6E and F shows the inclinations of the teeth to the occlusal plane before and after expansion. Note that the right first molar only tipped 2.96° buccally (from 66.11° to 69.07° to the occlusal plane) as the expander counteracted the buccal tipping effect of orthodontic expansion. The left first molar tipped lingually 9.70° (from 73.30° to 63.60° to the occlusal plane) thanks to the lingual crown torque added.
Patient 2. A, Occlusal picture at delivery of the programmed expander. B, Occlusal picture 3 months post alveolar bone graft (ABG) surgery, at the removal of the transpalatal arch (TPA) with arms. C and D, Lateral views of the dentition in occlusion at removal of the TPA with arms. E, Digital models at initial showing the inclinations of the teeth. F, Digital models at removal of the TPA with arms showing the inclinations of the teeth.
Discussion
Currently, there is no agreement regarding which type of appliance should be used for the expansion prior to secondary ABG in patients with CLP. Some centers use RPE, while others prefer to use slow expansion, typically with a QH appliance (Tindlund et al., 1993; Vasant et al., 2009; Aizenbud et al., 2012). We chose not to use an RPE in these patients, because their constriction was mainly in the anterior area and expansion with an RPE would have resulted in overexpanded posterior segments. A fan expander would have been able to provide more anterior than posterior expansion, but we chose not to use it because of the interference with the surgical field. Lastly, a QH appliance would also have been able to provide differential expansion, but we chose not to use it because of the interference with the surgical field, the need of multiple appointments for its reactivation, and the inability to precisely predict the exact expansion effects. Furthermore, these expanders would require extra appointments to separate, band, take impressions, deliver an expansion device, monitor the expansion of the cleft segments, and make adjustments as required. Due to the shape memory of the NiTi alloy, the reprogrammed NiTi expander can be customized to the desired width and becomes passive once that dimension is achieved. On the contrary, the QH has its activation in the SS body of the appliance, and in order to be activated, it needs to be widened beyond the desired dimension. Thus, its expansion effect is not self-limiting, which can lead to overexpansion.
Reprogramming the NiTi expander simplified the procedure, reduced patient visits, moved the segments to the programmed position, and could be left in place during ABG, avoiding the delay of the surgery. Furthermore, contrary to a QH or RPE, this programmable NiTi expander does not need a dental laboratory for its fabrication, which would make this appliance a candidate for use on missions in developing countries, where dental laboratory support is not available. On the other hand, this expander also requires a wire shaper power supply unit such as the Bender Soarer-X (Tomy Incor) or the Memory Maker (Forestadent, Pforzheim, Germany), which are not standard pieces of orthodontic equipment. Nevertheless, this initial investment would be cost-efficient on the long run, since laboratory fees would be eliminated. The expander was useful in reducing the number of appointments and is based on a “band first add expander later” approach, which can be helpful in treating uncooperative young patients.
Most orthodontists will use the appliances that they are accustomed to using; hence, this appliance is unlikely to replace the QH and RPE in a regular clinical practice. However, if the equipment is available, the use of the programmable NiTi expander should be favored in some clinical situations, due to its advantages over RPE and QH.
Possible complications of the programmable NiTi expander include wire breakage if bent at the junction of the SS arms and the insertion pad (although contraindicated by the manufacturer to bend the arms there), disinsertion from the lingual sheath, nonactivation if the SS arms are considerably readapted after reprogramming the appliance, and wire embedment into palatal tissue if the expander size is too large.
Conclusions and Future Perspectives
The programmable NiTi expander can be used for pregraft orthodontic expansion in patients with CLP. The advantages of this expander include programmable differential expansion customizable to the patient’s needs, predictable expansion effects, no risk of overexpansion, ability to control molar torque, less chair time, fewer appointments, no laboratory needed for fabrication, noninterference with palatal flap surgical access, and therefore no need to be replaced with a TPA with arms prior to surgery.
For all of these reasons, the NiTi expander could be an alternative to conventional appliances to provide expansion in patients with CLP prior to ABG surgery, as it adapts to the specific needs of these patients. However, comparative studies are necessary to determine whether the results obtained are comparable to the ones from RPE and QH, the most commonly used appliances. Currently, we are studying how the programmable NiTi compares to these appliances in 71 patients with UCLP and hope to be able to report results soon.
Footnotes
Acknowledgments
The authors would like to acknowledge Proclinic for contributing in financing the postgraduate studies in Orthodontics of the first author with the Proclinic Scholarship.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.