
Abstract
Objective
To evaluate the influence of filling material and timing of surgery on radiograph outcomes of alveolar grafting with premaxillary osteotomy. The null hypothesis was that radiographic outcomes would be similar with both rhBMP-2 (rhBMP-2G) and cancellous bone from the iliac crest (IG), regardless of the timing of surgery.
Design
Cross-sectional study with consecutive sampling of 56 periapical or occlusal radiographs taken 12 months after surgery.
Setting
A single tertiary craniofacial center.
Patients/Participants
Twenty-eight patients with complete bilateral cleft lip and palate and mean age of 13 years. The individuals underwent bilateral alveolar grafting associated with premaxillary osteotomy (AG + PO) with rhBMP-2 or cancellous bone from the iliac crest.
Interventions
Experienced maxillofacial surgeons used the same surgical technique in both groups. AG + PO were assigned as success or failure by 3 blinded raters based on modified Bergland and SWAG scales.
Main Outcome Measures
The influence of filling materials and timing of surgery on radiographic outcomes was verified by Fisher's exact test and chi-square test (P < .05).
Results
There was no significance variation between the mean age of participants in the rhBMP-2G and IG (P = .471). Scales showed almost perfect reliability (agreement rate = 96.4%; K = 0.85). rhBMP-2G and IG had similar success rates with modified Bergland scale (85.7% and 82.1%) and SWAG scale (92.9% and 82.1%), respectively. However, only modified Bergland scale found influence of age on radiographic outcomes (P = .025).
Conclusions
AG + PO performed with rhBMP-2 and iliac crest bone showed similar radiographic success rates, regardless of the timing of surgery.
Keywords
Introduction
Patients with complete bilateral cleft lip and palate (BCLP) usually have a protruding and deviated premaxilla due to overgrowth at the premaxillary-vomerine suture. There may also be abnormal inferior position of the premaxilla and underdevelopment of the lateral maxillary segments.1–3 While sagittal excess is physiological in patients with BCLP during childhood, decreasing progressively and spontaneously until completion of the growth spurt, vertical excess does not spontaneously decrease with growth and, therefore, may and must be corrected. 4 Different protocols for protruding premaxillary management are cited in the literature, including secondary alveolar bone grafting with premaxillary osteotomy and early secondary alveolar bone grafting with premaxillary osteotomy.5,6 Orthodontic intrusion to treat premaxillary vertical excess according to patient age and defect severity has also been suggested. However, the protocol is not effective for vertical excesses greater than 7–8 mm.4,7,8
Bilateral alveolar bone grafting presents considerable challenges: severe bone and soft tissue deficiency, a protruded and often displaced premaxilla, premaxillary mobility, and a high prevalence of oronasal fistulae after primary surgeries. 9 Studies have shown that better outcomes are achieved when alveolar grafts are performed before eruption of the maxillary canines at the cleft site. Furthermore, dental development at the timing of surgery is probably the most important factor influencing the success rate of these surgical procedures.10,11 Alveolar bone grafting with premaxillary osteotomy (AG + PO) in patients with BCLP is still controversial. Generally, there are two main indications for surgical positioning. First, PO may be required to facilitate nasolabial soft tissue revision. Second, there is a need for premaxillary positioning in combination with alveolar bone grafting. This would have the advantage of aligning and leveling maxillary segments and the arguable advantage of facilitating closure of oronasal fistulae.5,8,12 More accurate nasal closures performed during AG + PO have been reported, although fistulae after AG + PO may be associated with both difficult closure of the various layers during surgery6,13 and with compromised blood supply.8,12,14 In addition, a study demonstrated a 90% reduction in the risk of fistula symptoms after performing alveolar bone grafting alone. This reduction was not influenced by the type of cleft and timing of surgery. 15
The gold standard for filling alveolar clefts is currently fresh autogenous cancellous bone grafting from the anterior iliac crest. It provides bone with highly osteogenic, osteoinductive, osteoconductive, and nonimmunogenic properties in abundant amounts and very good surgical outcomes; however, donor-site morbidity is present.16–19 Accordingly, there is a great interest in developing alternatives to patient-harvested bone for bone grafting. Growth factors, such as bone morphogenetic proteins (BMPs), have shown great promise in bone regeneration. 20 Several studies on the role of BMPs in bone formation have been carried out since the classic study by Marshal Urist, 21 with their role in inducing the bone morphogenesis cascade being discovered. Recombinant gene technology manufacturing and a suitable carrier have also been required for clinical application of BMPs.22–24
Recombinant human bone morphogenetic protein 2 (rhBMP-2) has become a viable alternative to iliac crest bone for performing AGs after previous studies have shown similar outcomes between them.25–30 However, concerns persist in the association of both the material and the premaxillary osteotomy and its surgical positioning with AG. Therefore, this study aimed to compare radiographic outcomes of alveolar grafting with premaxillary osteotomy in patients with BCLP performed with rhBMP-2 or with autogenous iliac crest bone. The influence of timing of surgery was also evaluated. The null hypothesis was that AG + PO outcomes would be similar with both types of filling material, regardless of the timing of surgery.
Materials and Methods
Patients
The cross-sectional study was approved by the Research Ethics Committee of the Hospital of Rehabilitation of Craniofacial Anomalies of University of São Paulo (process n. 2.334.63429874520.1.0000.5441) and was conducted in accordance with the Declaration of Helsinki. The sample consisted of 56 periapical and occlusal radiographs of individuals with BCLP who were consecutively submitted to AG + PO between 2004 and 2016. All surgeries were performed in a single craniofacial center in Brazil, by experienced maxillofacial surgeons using a standardized technique. Only periapical or occlusal radiographs taken from 12 months after osteotomy, surgical premaxillary positioning and bilateral alveolar grafting in single-stage (AG + PO) were included. Exclusion criteria were associated craniofacial syndromes and comorbidities.
Patients were divided into two groups according to the graft used: rhBMP-2 (rhBMP-2G) or cancellous bone from the anterior iliac crest (IG). rhBMP-2G comprised 14 patients (10 males, 4 females) with a mean age of 12.5 years (±4.8) operated between 2011 and 2016. IG consisted of 14 patients (9 males, 5 females) with a mean age of 13.4 years (±3.8) operated from 2004 to 2010. Groups were paired according to dental development. AG + POs performed before canine eruption were considered “optimal”. AG + POs performed after canine eruption were classified as “late”. All patients underwent preoperative orthodontic maxillary expansion to improve surgical access to the cleft site and enable premaxillary repositioning. Before AG + PO, patients who had not yet started comprehensive orthodontic treatment had orthodontic brackets and wires fixed on both maxillary posterior teeth and premaxillary teeth in order to maintain an acrylic occlusal splint in position postoperatively. These splints were pre-surgically fabricated during a mock surgery.
Surgical Procedure
On the buccal side, oblique incisions were made along the gingival border, extending from the cervical limits of the molar teeth to the depth of the mucolabial fold, providing sufficient mobility for these flaps. Cuts were also made in the periosteum at its base. Anteriorly, the incisions were extended along the gingival border to the central incisors and through vertical incisions along the cleft edges. Bilateral buccal mucoperiosteal flaps were raised, keeping the pedicled premaxilla on the labial mucosa. Vertical mucosal incisions on the premaxillary side of each cleft were carefully sited to maintain a wide mucosal attachment. The subperiosteal mucosal flaps outlined by these incisions were undermined and raised from the bone, separating the nasal and palatal sides, and exposing the maxillary-vomerine suture. The osteotomy of the maxillary-vomerine suture was then performed with a drill and a reciprocating saw. The nasal floor and palatal side were reconstructed using interrupted and everted mattress sutures, respectively. The premaxilla was repositioned. Either two sponges soaked in 4.2 mg of rhBMP-2 (INFUSE Bone Graft; Medtronic Sofamor Danek) per cleft or iliac crest bone were placed in the alveolar defect. Scaffolds or absorbable membranes other than absorbable collagen sponge from kit were not used in either group. The mucoperiosteal flaps were sutured with interrupted stitches. The acrylic occlusal splint attached to the fixed appliance was maintained for 60 days.
Assessment of Radiographic Outcomes
The success of AG + PO was determined using modified Bergland 31 and The Americleft Standardized Way to Assess Grafts (SWAG) 32 scales. The 56 radiographs were organized on the software PowerPoint, and the images were independently analyzed by 3 blinded raters, twice with a 30-day interval between evaluations. AG + PO outcomes were considered successful when categorized as “A” and “B” on the modified Bergland scale 11 or “5”and “6” on the SWAG scale (Figures 1 and 2). Primary outcomes were AG + PO radiographic success rates according to the material used to fill the bone defect and timing of surgery. Secondary outcomes included reliability and reproducibility between scales.
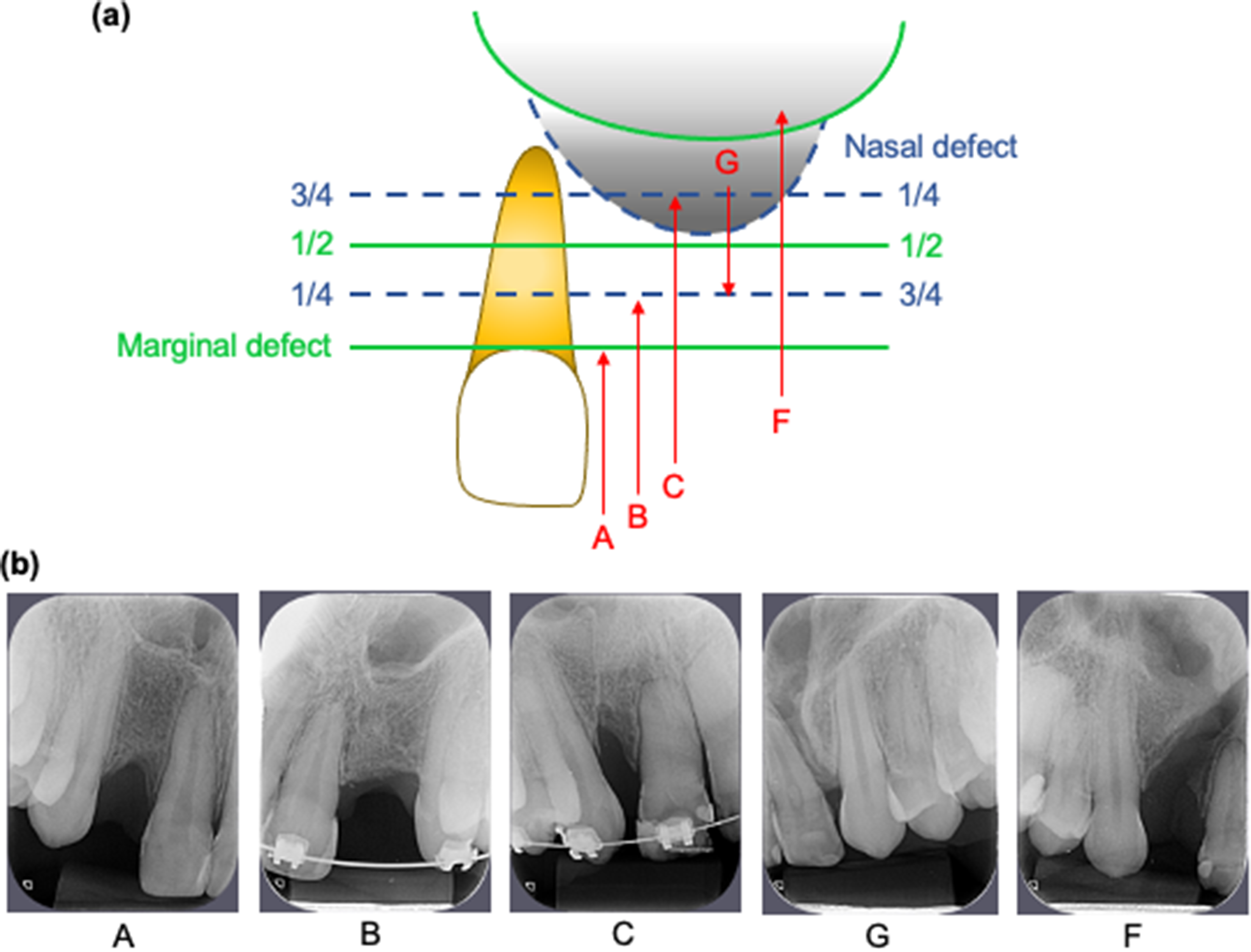
(a) the modified Bergland scale categorizes surgical outcomes according to cleft filling. A: 100% filled cleft; B: marginal defect of 25% of the tooth root; C: marginal defect of 75% of the tooth root; G: nasal defect of 75% of the tooth root; F: failure;31 (b) Corresponding radiographic images.
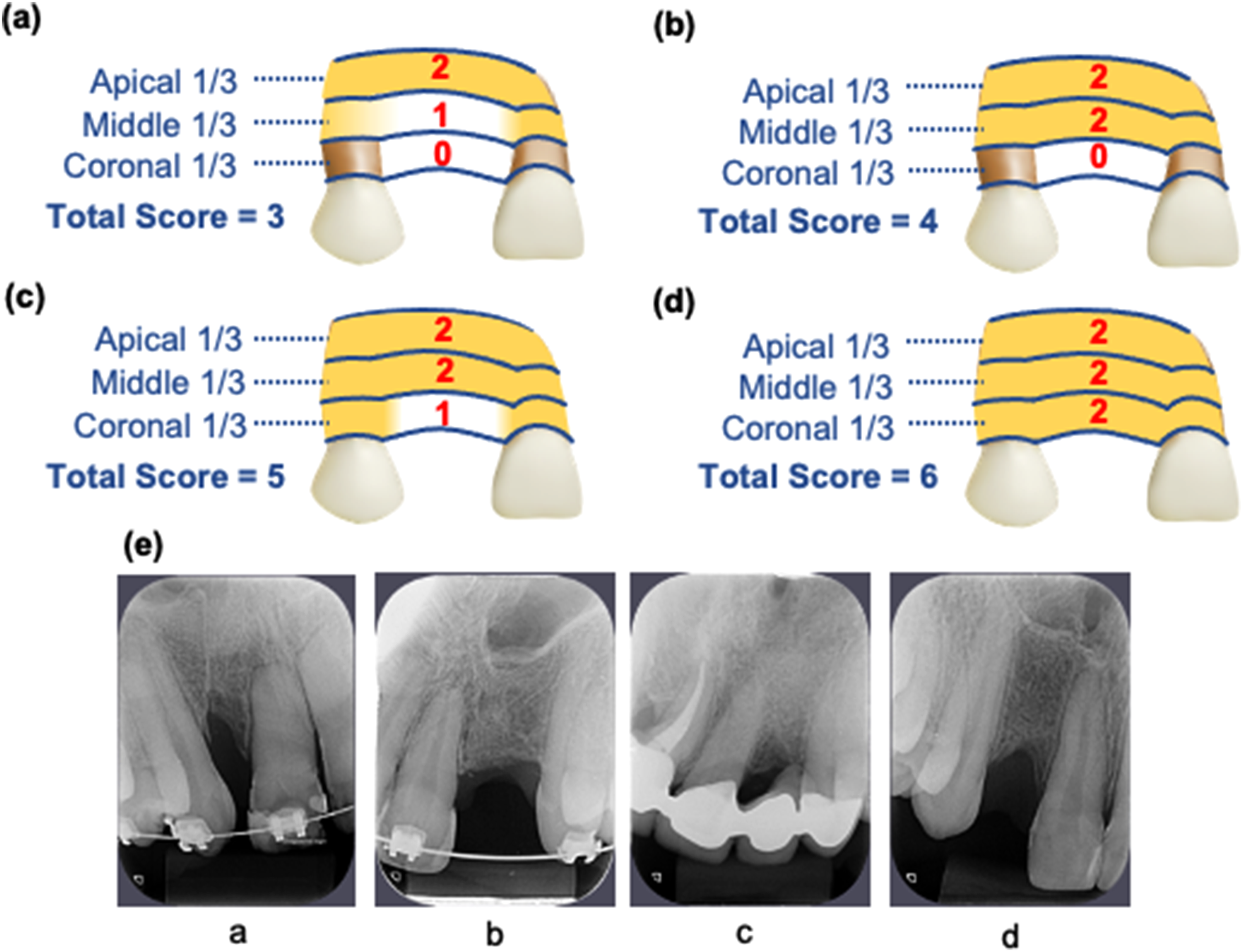
The standardized way of assessment grafts (SWAG) scale categorizes the apical, middle and cervical thirds according to bone formation - 0: no bone formation and root exposure; 1: covered roots with no bone formation; 2: bone bridge. The sum of ratings produces a final score from 0 to 6.32 (a) Example of final score 3; (b) example of final score 4; (c) example of final score 5; (d) example of final score 6.
Statistical Analysis
Statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) software. k statistics were applied to analyze intra- and inter-examiner reliability for radiographic outcomes and between scales. The influence of filling materials and timing of surgery on radiographic outcomes was analyzed using Fisher's exact test and qui-square test (P < .05).
Results
The mean and median age of patients were similar in both groups (P = .471). Intra- and inter-rater reliability ranged from moderate to excellent (0.51 to 0.94) (Table 1). Agreement between scales was also almost perfect (agreement rate = 96.4%; K = 0.85). rhBMP-2G and IG had similar radiographic success rates with the modified Bergland scale (85.7% and 82.1%) and SWAG scale (92.9% and 82.1%), respectively (Table 2). The graft materials also showed similar radiographic outcomes when the timing of surgery was considered (Table 3). However, only evaluations based on the modified Bergland scale found influence of the timing of surgery on radiographic outcomes (P = .025, Table 4), with a prevalence of failures 8 times higher in AG + PO performed late compared to AG + PO performed at the optimal time (95% CI =1.07–59.82, P = .043).
Intra- and Inter-Examiner Reliability (k Statistics).
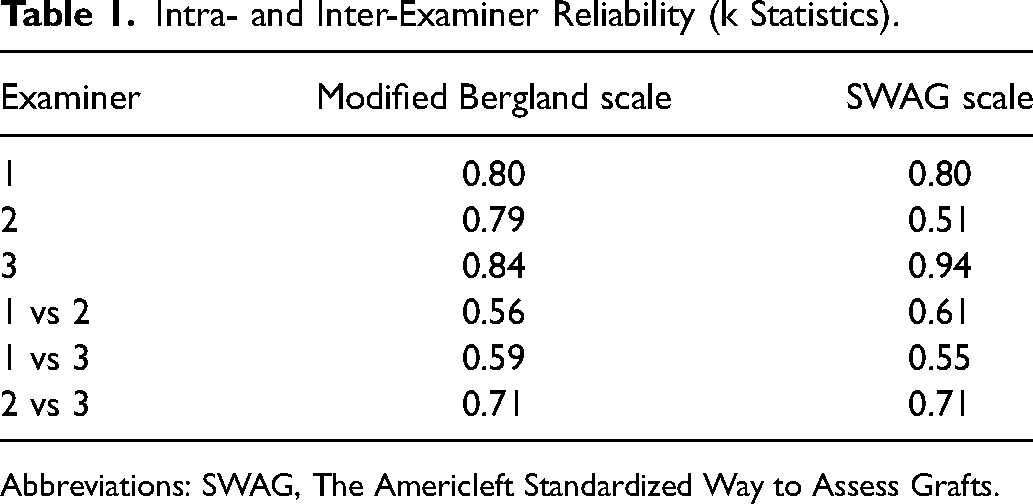
Abbreviations: SWAG, The Americleft Standardized Way to Assess Grafts.
Influence of Filling Materials on AG + PM Radiographic Outcomes (Fisher's Exact Test).
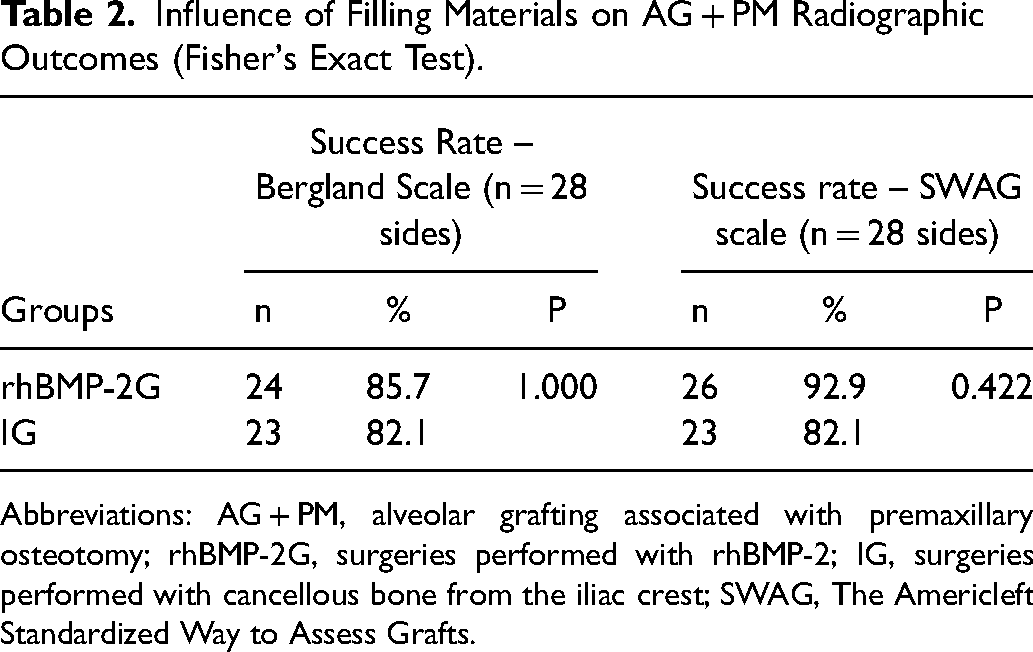
Abbreviations: AG + PM, alveolar grafting associated with premaxillary osteotomy; rhBMP-2G, surgeries performed with rhBMP-2; IG, surgeries performed with cancellous bone from the iliac crest; SWAG, The Americleft Standardized Way to Assess Grafts.
Influence of Filling Materials on AG + PM Radiographic Outcomes Considering the Timing of Surgery (Chi-Square Test).
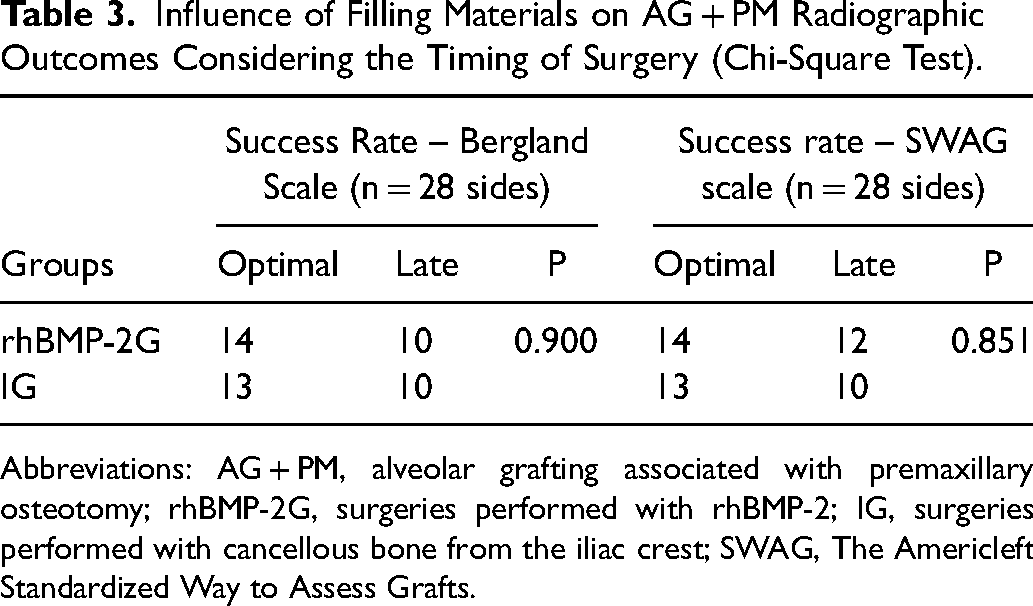
Abbreviations: AG + PM, alveolar grafting associated with premaxillary osteotomy; rhBMP-2G, surgeries performed with rhBMP-2; IG, surgeries performed with cancellous bone from the iliac crest; SWAG, The Americleft Standardized Way to Assess Grafts.
Influence of Timing of Surgery on AG + PM Radiographic Outcomes (Fisher's Exact Test).
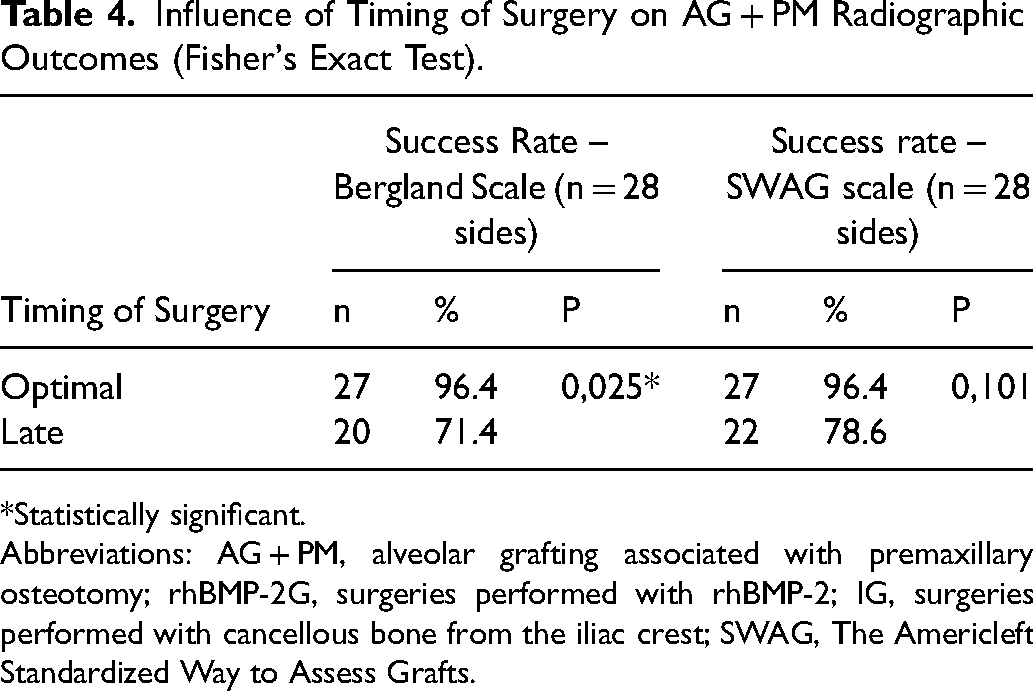
*Statistically significant.
Abbreviations: AG + PM, alveolar grafting associated with premaxillary osteotomy; rhBMP-2G, surgeries performed with rhBMP-2; IG, surgeries performed with cancellous bone from the iliac crest; SWAG, The Americleft Standardized Way to Assess Grafts.
Discussion
The current standard of care for an alveolar cleft defect is an autogenous bone graft from the iliac crest. However, limited supply and donor-site morbidity have increased interest in alternatives to replace traditional bone grafts. 20 Although dental development at the timing of alveolar grafting is considered the most important factor in its success rate,10,11 factors such as soft tissue scar, poor blood supply and type of graft can also lead to dehiscence, infection and bone resorption.9,14,33 This concern increases in bilateral alveolar grafts associated with premaxillary osteotomy due to greater complexity, tissue manipulation and risk of premaxillary devitalization.6,8,12,14 Accordingly, the present study evaluated AG + PO radiographic outcomes based on previously validated rating scales in order to prove that rhBMP-2 and iliac crest bone have similar success rates, both with better outcomes when surgeries are performed before canine eruption on the cleft side.
Method Reliability
Several methods have been used to determine AG + PO success rates; however, categorization of intraoral radiographs using rating scales is a frequently used method due to its accuracy, reliability and clinical application. Two previously validated scales31,32 were used and showed a total of 54 agreements (0.85). Inter-rater reliability ranged from moderate to excellent (0.51 to 0.94) and intra-rater agreement ranged from moderate to strong (0.55 to 0.71) 34 (Table 1). Although these results are in agreement with previous studies,11,35 non-standardized radiographs and the absence of categories for all types of bone bridges probably impaired the categorization.11,36
Filling Materials
Direct comparisons with the literature were difficult because studies used different systems to verify bone formation after AG + PO. A previous study using the Kindelan score demonstrated radiographic success rates of AG + PO similar to this study. 13 However, a study using the Bergland scale presented worse success rates. 6 These differences were probably due to the types of grafts employed. In the first study, 13 iliac crest bone was used; while in the second, 6 mostly mandibular symphysis bone. In the present study, rhBMP-2 therapy resulted in similar radiographic bone repair compared to traditional iliac crest bone grafting (Tables 2 and 3). These findings are in agreement with previous studies25–30 and suggest that the lack of donor-site morbidity makes rhBMP-2 a promising alternative for premaxillary surgical positioning.
Timing of Surgery
The timing of surgery is a relevant factor in AG success rates.10,11,16,33,35 Previous studies have shown that surgeries performed late were more associated with poor wound healing, graft exposure and recurrent fistula than those performed at the optimal time.13,37 Therefore, medians and means of age were calculated in order to verify the variation of intergroup ages, with no statistically significant difference. In comparisons considering both the timing of surgery and material, the intergroup outcomes of this study were similar (Table 3). However, a previous study observed better bone regeneration using rhBMP-2 for late AGs compared to traditional iliac bone. 37 Thereby, the use of rhBMP-2 should be advocated especially in situations that require a considerable increase in soft tissue healing. 38 When the influence of timing of surgery was analyzed without considering the material used, only assessment based on the modified Bergland scale corroborated the influence of age on radiographic outcomes10,11,16,33,35,37 (Table 4). This difference between scales was probably due to the sample size and the poor quality of some radiographs.
Strengths and Limitations
There were some limitations in this study that may have implicate its results. For example, carrying out a study with only patients operated on by the same surgeon was not possible due to the sample size. This would eliminate biases associated with possible individualities in performing the standardized surgical technique. All patients at the Hospital with BCLP who were available in the selected time period and who met the inclusion criteria were included. Many radiographs were unavailable or of poor quality. In addition, data from these patients were retrieved retrospectively through analysis of patient charts. A prospective study or with a larger sample would add important data on AG + PO outcomes. On the other hand, AG + PO is still a controversial procedure, 12 usually indicated only for severe abnormalities that cannot be treated orthodontically.4,7,8 Hence, this study was useful to show that rhBMP-2 is a viable alternative material also to perform AG + PO.
Conclusion
AG + PO performed with rhBMP-2 and iliac crest bone showed similar radiographic success rates, regardless of the timing of surgery.
Footnotes
Acknowledgements
We thank Dr. Flávia Neves Cintra for helping with the data analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.