
Abstract
Objective
The aim of this study was to compare and assess the pain perception, anxiety, and discomfort between two different rapid maxillary expansion (RME) protocols in patients with unilateral cleft lip and palate (UCLP).
Design
This is a prospective study.
Setting
The study was done in a comprehensive cleft care center.
Patien and Participants
The sample included 26 patients between ages 6 and 9 years with a history of repaired UCLP.
Interventions
The patients were randomly allotted into 2 groups—Group A and Group B. Group A received 1 RME activation per day and Group B received 2 activations per day. The participants after RME activation completed a self-report questionnaire and ranked the pain and anxiety levels using Faces pain scale and Hamilton anxiety scale, respectively. The evaluation was done every day for 1 week.
Main Outcome Measure
The Faces Pain Scale, Hamilton Anxiety Scale, and self-report questionnaires assessed the pain, anxiety, and discomfort experienced by the patients after 2 different types of RME activation protocols.
Results
Group B experienced significantly higher pain in the molars than Group A (P < .001). There was no significant difference between the 2 RME activation protocols regarding anxiety and jaw discomfort.
Conclusion
Patients who received 2 activations per day experienced significantly higher levels of pain in the molars compared to the patients who received a single activation per day. There were no significant differences between the 2 activation protocols in terms of pain in the palate, tongue, anxiety, and jaw discomfort.
Introduction
Cleft lip and palate (CLP) is considered to be one of the most common head and heck pathologies, which is caused by a multifactorial etiology (Trimetsuntorn et al., 2020). Patients with CLP develop growth disturbances of the midfacial region after primary surgery (Berkowitz, 2013). This is mainly due to scar tension. However, various factors affect the severity of abnormality such as the severity of cleft defect and the surgical techniques used. Maxillary deficiency, constricted upper arch, and cross-bite are common manifestations of patients with CLP. The technique of rapid maxillary expansion (RME) is commonly used to address the transverse discrepancy in patients with CLP (Pan et al., 2007). RME is generally performed during mixed dentition or early adolescent stage. Treatment during this period provides maximum skeletal expansion and reduces dental effects. RME is also done prior to facemask therapy to aid in adequate protraction of the maxilla by disarticulating the circumaxillary sutures (Halicioğlu et al., 2012).
Various intraoral appliances are used for RME. The Hyrax appliance is the most common appliance used for RME. It has an expansion screw and is usually activated either once or twice daily for about 2 to 4 weeks (Needleman et al., 2000). The expansion force varies depending on the activation protocol. A single activation of the screw produces approximately 3 to 10 pounds of force (Isaacson et al., 1964). Two-turn activation has an advantage of faster activation and shorter active treatment periods and chair side time as an advantage. Another advantage may be the shorter bonded appliance wear, which negatively affects oral hygiene (Ramoglu and Sari, 2010).A study by Ramoglu and Sari (2010) on noncleft patients found that both activation protocols have a similar effect on dentofacial structures in the transverse, vertical, and sagittal planes. However, 2-turn activation may produce much higher forces required for patients with CLP leading to pain and discomfort (Ekstörm et al., 1977).
Pain and discomfort are some of the most common side effects reported by the patients after RME screw activation (Needleman et al., 2000). A study concluded that the pain experienced during RME can be due to the inflammatory reaction during sutural opening and the compression of the periodontal ligament (Joviliano et al., 2008). Few studies have evaluated the pain and discomfort during RME. The studies concluded that most children undergoing RME report pain, which generally occurs during the initial phase and diminishes later (Needleman et al., 2000; Gecgelen et al., 2012; Halicioğlu et al., 2012). A study found that RME activation protocols with 2 turns per day produced greater pain levels than protocols with only 1 turn per day (Needleman et al., 2000; Baldini et al., 2015). Long duration of treatment, involvement of multiple specialists, and multiple surgeries make children with CLP and their parents more apprehensive than their non-CLP counterparts. Pain perceived during treatment can affect patient compliance and impede oral hygiene maintenance (Datana et al., 2020). The pain and discomfort experienced due to RME activation protocols could be the determining factor for compliance and adherence to treatment in patients in CLP. Although there are studies comparing the effect of RME activation protocols in patients without CLP, there is a shortage of literature that studies the pain perception and discomfort experienced by patients with cleft lip and palate during RME procedures and different activation protocols. Hence, the primary objective of the study is to compare and assess the amount of pain and anxiety of 2 different RME activation protocols in patients with cleft lip and palate for a period of 1 week. The secondary objective is to compare and assess the amount of discomfort experienced by the patient after 2 different RME activation protocols over a period of 1 week.
Methods
The study was approved by the Institutional Ethics Committee. Informed consent was obtained from the parents or legal guardians of the patients to be enrolled, before starting the study. Prospective enrollment of patients with 6–9 years of age was done, with a history of repaired unilateral cleft lip and palate (UCLP) and who required RME as a part of their routine treatment. All patients were enrolled from a single center.
The study was conducted in a comprehensive cleft care center. A total of 26 consecutive patients (11 males, 15 females) with repaired UCLP were recruited into the study. The sample size was estimated using G*Power software (Version 3.1) with an effect size of 1.1 and power of 0.80 based on a previous study by Figueiredo et al. (2016). The patients were randomly allotted into the study groups: Group A and Group B, with 13 patients in each group. Group A received a 1 RME activation per day, while Group B received 2 activations per day. The selection criteria include: age group of 6–9 years, patients with repaired UCLP, and patients with hypoplastic maxillae who required RME treatment before maxillary protraction. The exclusion criteria include: patients older than 10 years of age, bilateral cleft lip and palate, presence of periodontal disease, neurological disease, and/or genetic disease, clefts associated with craniofacial syndromes, patients with a history of previous orthodontic treatment, and patients who did not require RME as part of their treatment protocol.
All the subjects underwent RME with a bonded expander (Hyrax). The appliance extended from the molars to the primary canine. The bonded hyrax was fabricated with an acrylic splint (Figure 1). The appliances were designed and delivered to the patients by the same investigator. The bonded RME appliance was cemented to the maxillary arch and the patients were recalled after 1 week of cementation of the appliance. This was done to eliminate any anxiety and discomfort arising from the appliance per se. After 1 week, once the patients got accustomed to the appliance, the effect of the activation protocol on the patients was assessed. In Group A, the expansion screw was activated at 1/4 turn per day (1 activation, 0.25 mm per day), and in Group B, the expansion screw was activated at 2/4 turns per day (2 activations, 0.5 mm per day). In both groups, the expansion screw was activated until the desired palatal expansion was reached. Pain, anxiety, and discomfort assessment was done 10 min after the activation of the RME for a period of 1 week. First RME activation for all patients was done in the cleft center. Pain, anxiety, and discomfort assessment was done after 10 min of activation. Verbal instructions were given to the parents and the patients on correct assessment of pain, anxiety, and discomfort. The patients were asked to complete the proforma daily, after the activation of the expander for next 6 consecutive days.
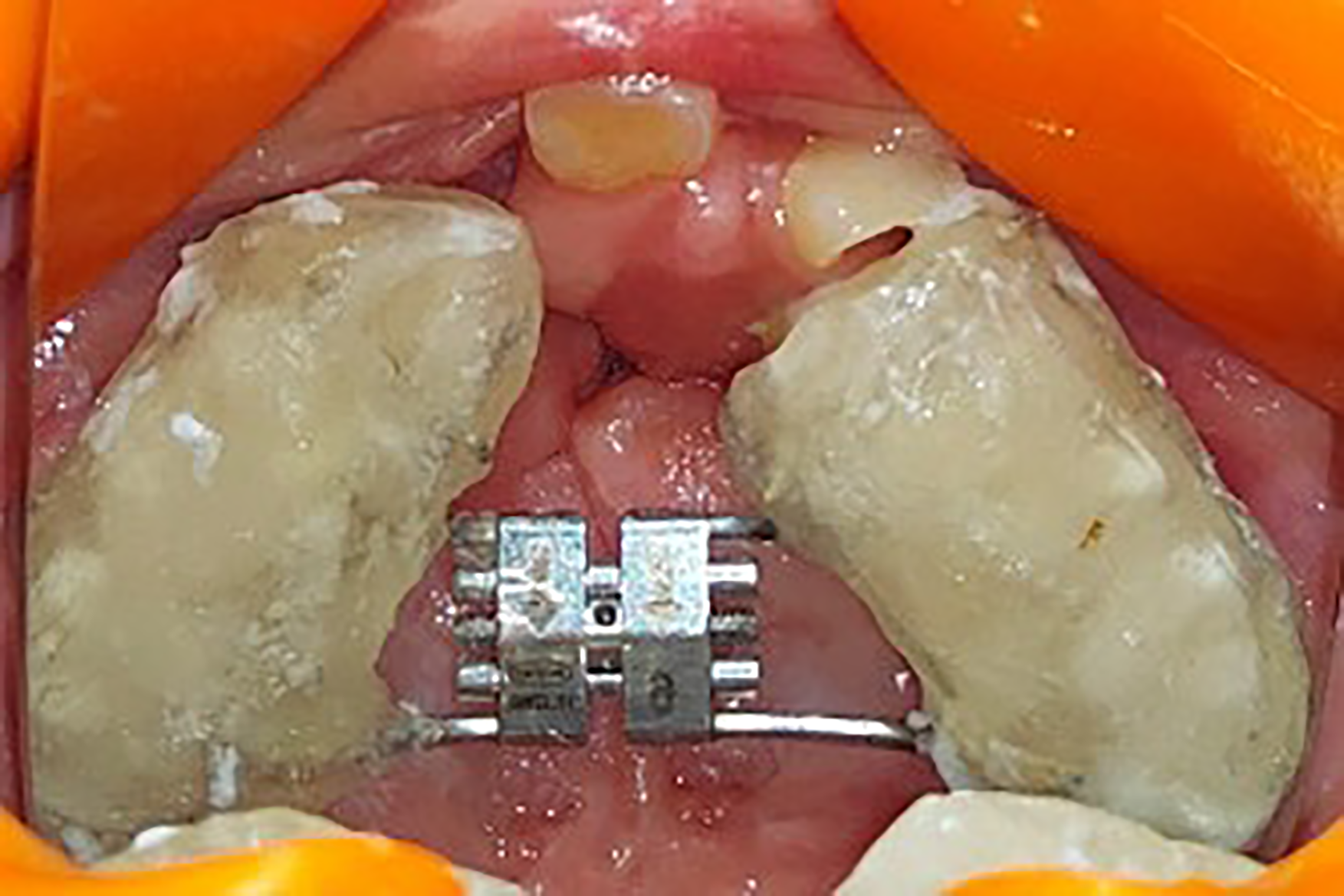
Bonded rapid maxillary expansion (RME) expander used in both groups. The RME appliance was fabricated using an acrylic splint over a metal framework and extended from the canines to the molars.
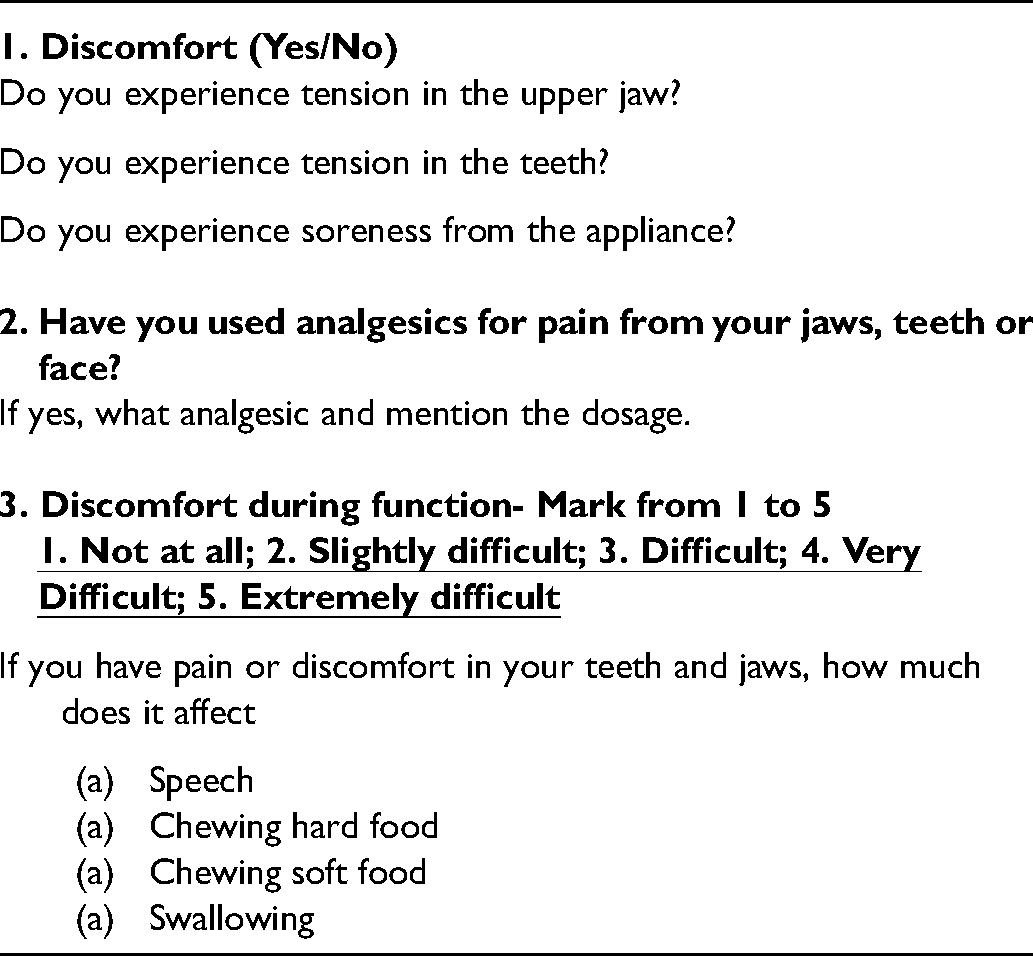
The anxiety level was assessed using the Hamilton Anxiety Rating Scale (HAM-A) (Hamilton, 1959). Based on the scores, the anxiety levels of the patients after RME activation were recorded as follows: 0, No anxiety; 1, Mild; 2, Moderate; 3 Severe; 4, Very severe. Wong–Baker Faces Pain Scale (FPS) was used to assess the pain (Garra et al., 2013). The scale consists of faces describing the level of pain from “No Hurt” to “Hurts Worst.” The patients were asked to select a face that best describes their pain perception. Pain assessment was done in relation to molars, incisors, palate, and tongue. The patients were advised to take any over-the-counter analgesics if required. Patients were also provided with a questionnaire consisting of self-report questions concerning discomfort, analgesic consumption, and jaw function after activation of RME. The questionnaires were based on 2 previous studies and are considered to have “acceptable” to “good” reliability and internal consistency (Stegenga et al., 1993; Feldmann et al., 2007; Feldmann and Bazargani, 2017) (Table 1).
Questionnaire to Assess Discomfort, Jaw Function, and Analgesic Consumption After Rapid Maxillary Expansion (RME) Activation for the First Week.
Data Analysis
Means and standard deviation (SD) were calculated for each variable. The Mann–Whitney test was used to compare the mean difficulty levels for speech; chewing hard and soft food; Faces scores for pain in relation to molars, incisors, palate, and tongue; Hamilton Anxiety Scale scores; and duration of treatment between groups at different time intervals. Friedman's test followed by Wilcoxon signed rank post hoc analysis was used to compare the mean difficulty levels for speech; chewing hard and soft food; Faces scores for pain in relation to molars, incisors, and palate between different time intervals in each study group. The χ2 test was used to compare the analgesic consumption between the 2 study groups. The level of significance (P-value) was set at P < .05. Considering the risk of Type I error when multiple comparisons are made between 2 groups, a Bonferroni correction was applied ie dividing the P-value by the number of comparisons made between 2 groups. Bonferroni's correction in the present study was 0.00625 to look for a true statistical significance between 2 groups for different variables. Applying this Bonferroni's correction to various P-value for intergroup comparisons done for different variables, the tables on comparison of mean Faces scores for pain in molar region between groups and mean number of days of treatment, remains unchanged, since all the P-values reported are <0.00625 (Bonferroni's correction value). The table on comparison of mean Faces scores of pain in the incisor region shows no significant change on day 3 and day 4, since the obtained P-values are higher than the Bonferroni's correction value (P = .00625). All analysis was performed using SPSS software version 22.0.
Results
Among the 26 patients, 24 patients completed the questionnaires. Two patients from Group A did not revert to the hospital. Consequently, Group A comprises 11 patients (4 males and 7 females) with a mean age of 6.8 years (SD 0.63 years). Group B comprises 13 patients (7 males and 6 females) with a mean age group of 7 years (SD 0.98 years). There were no significant differences in age and gender between the 2 groups (Table 2).
Age and Gender Distribution Among the Study Groups: Group A (1 Turn Activation) and Group B (2 Activations).
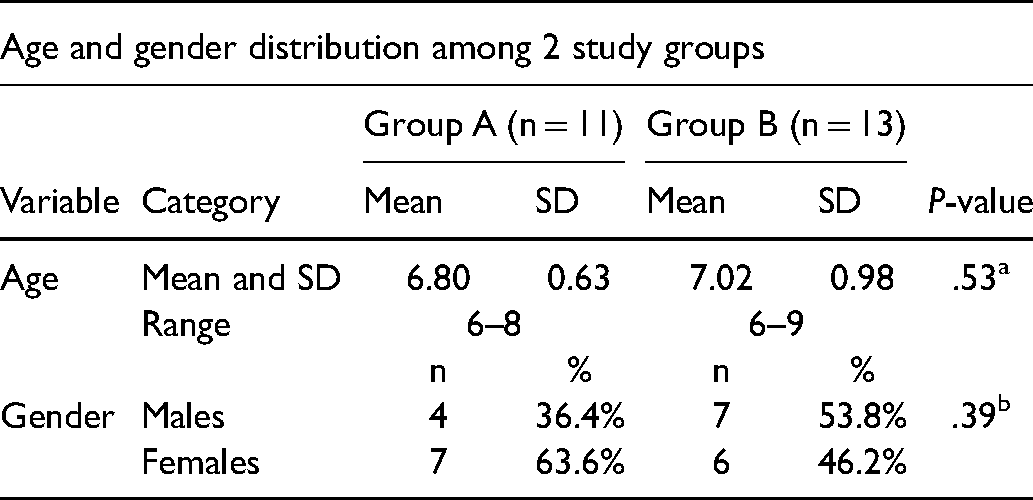
Table 3 describes the duration required for achieving optimal expansion in both Group A and Group B. Group A, which had 1 activation per day, required a longer treatment duration (mean 26 days) than Group B (mean 13.54 days), which had 2 activations per day. This difference in treatment duration was statistically significant (P < .001).
Mean Duration of Time Taken to Achieve the Required Expansion in Group A (1 RME Activation per Day) and Group B (2 RME Activations per Day).
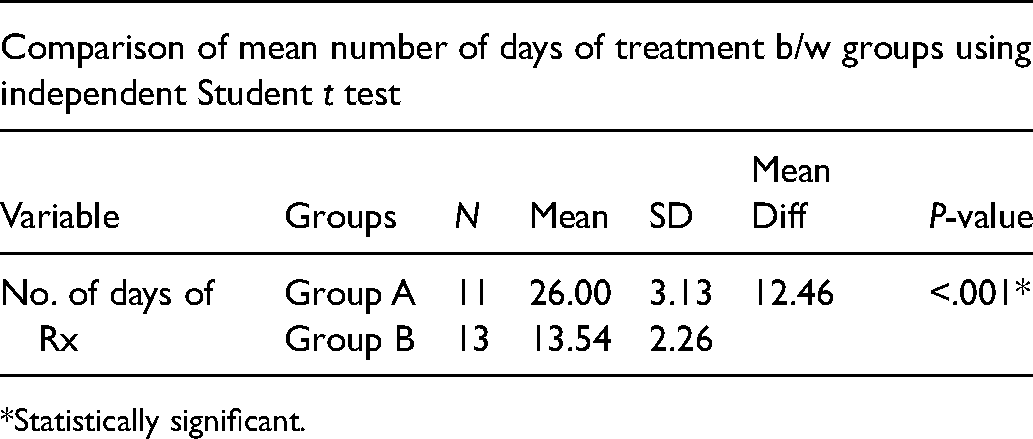
*Statistically significant.
Pain
Patients from both Group A and Group B experienced mild pain in the molars during the first week of activation. In Group A, the maximum pain was experienced on day 4, with a mean Faces score of 2.55 (SD 0.93). Even in Group B, the maximum pain was experienced on day 4 of activation, with a mean Faces score of 4.46 (SD 1.45). There was a statistically significant difference between the pain reported by the patients on day 4 compared to all other days in Group A. In Group B, there was a statistically significant difference between the pain reported on day 4 and day 5 compared to the first 3 days. Overall, the pain scores in the molars during 1 week of activation was significantly higher in Group B (P < .001) (Table 4).
Comparison of the Mean Faces Pain Scores in the Molars Between Groups at Different Time Intervals Using the Mann–Whitney Test.
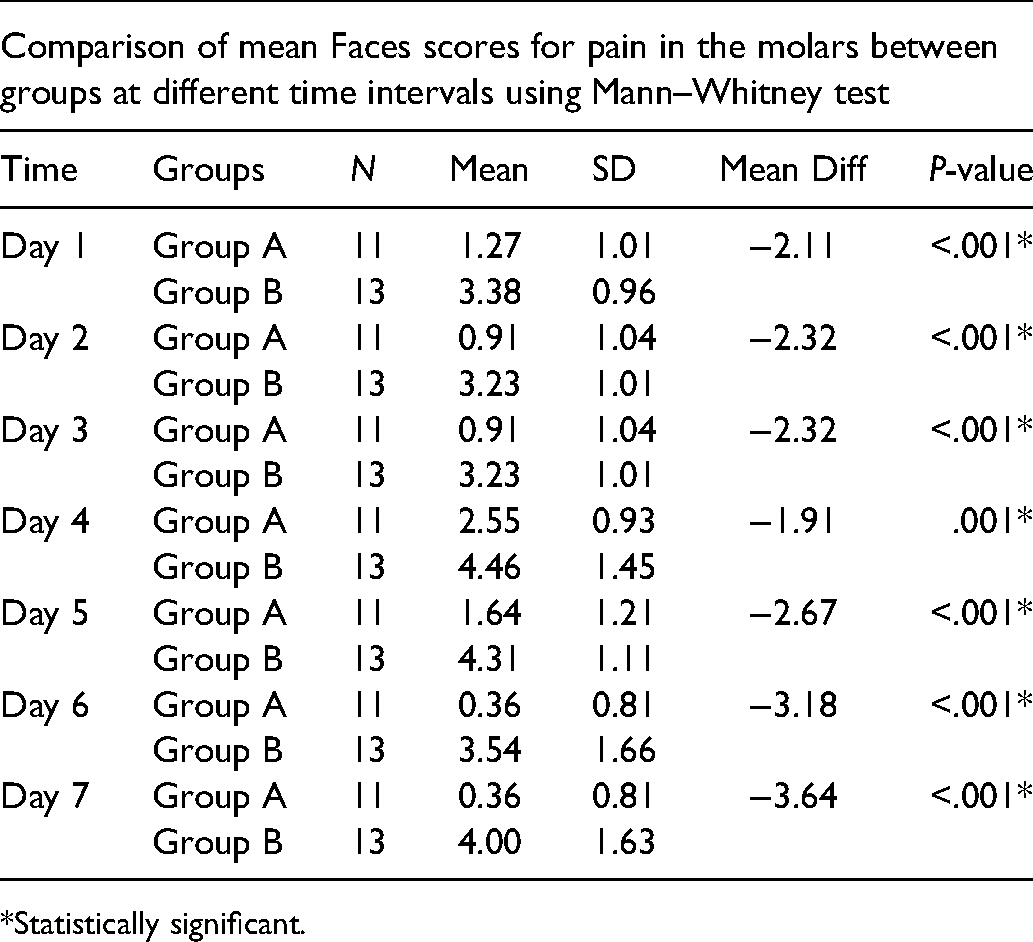
*Statistically significant.
On comparing the pain experienced in the incisors, Group B showed higher mean pain scores than Group A only on day 3 and day 4. This difference was statistically significant (day 3, P = .04; day 4, P = .02) (Table 5). The groups showed no significant differences between the pain experienced in the palate and tongue.
Comparison of Mean Faces Pain Scores in the Incisors Between Two Groups at Different Time Intervals Using the Mann–Whitney Test.
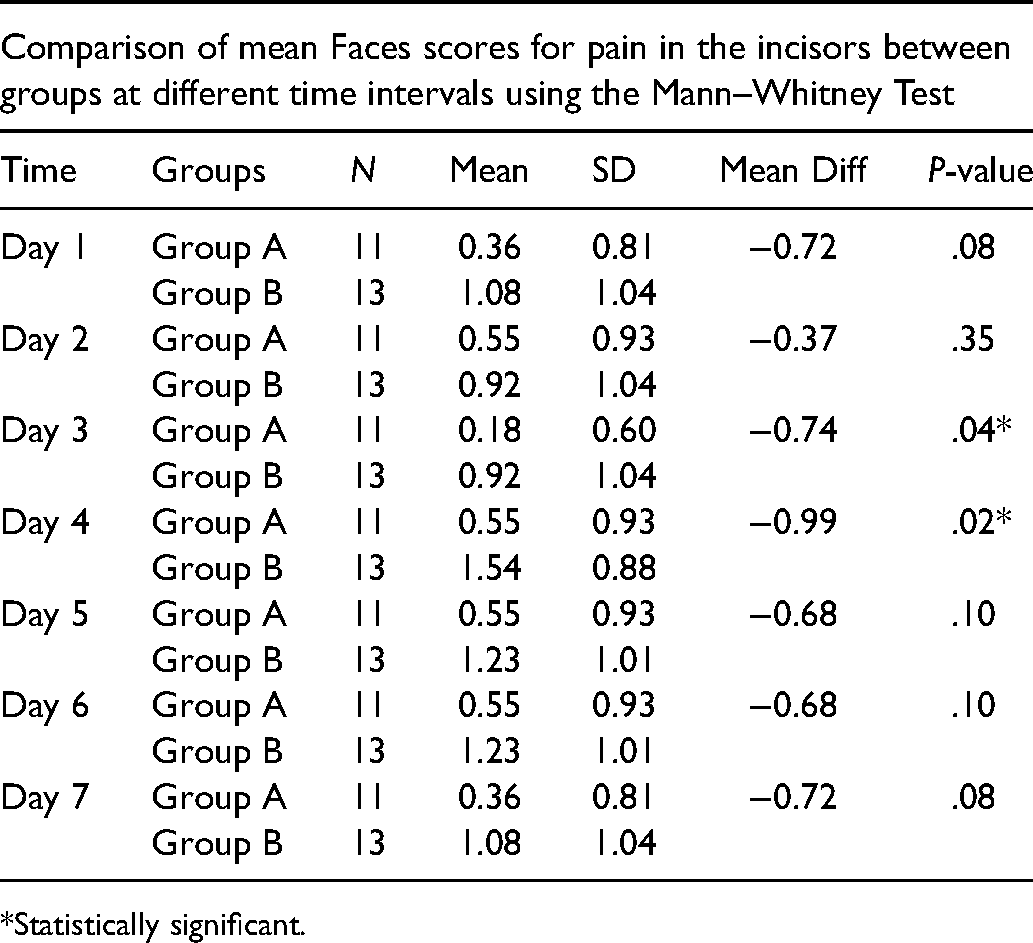
*Statistically significant.
Analgesic consumption was minimal and did not differ significantly between the groups. A total of 92.3% of patients did not take any analgesics for the pain. The most used analgesic was paracetamol.
Anxiety
The mean anxiety score of Group A was 1.36 (SD 1.12) and Group B was 1.31 (SD 0.48). There were no statistically significant differences between the anxiety experienced by Group A and Group B.
Discomfort During Function
The patients from both groups did not experience much discomfort during various jaw functions such as speech, swallowing, and chewing soft foods. However, patients from both groups had mild discomfort while chewing hard foods. However, the difference between the 2 groups was not statistically significant.
Discussion
RME is a widely used procedure during the treatment of malocclusions in patients with cleft lip and palate. The clinical monitoring of RME treatment often uses pain as a guide, and the correct interpretation of pain is of great importance (Timms, 1981). De Felippe et al. (2010) indicated that 93.9% of patients experienced pain and discomfort from palatal expanders (Hyrax, Haas, banded, and quad-helix). Although numerous studies have documented the pain, anxiety levels, and discomfort after RME procedures (Needleman et al., 2000; Gecgelen et al., 2012; Halicioğlu et al., 2012; Baldini et al., 2015; Feldmann and Bazargani, 2017), there are no studies that evaluate the pain and anxiety levels on patients with cleft lip and palate. Hence, the study compared and assessed the amount of pain and anxiety of 2 different RME activation protocols for a period of 1 week in a group of 26 patients with repaired UCLP.
Pain is a complex sensation that varies from 1 person to another; thus, objective quantification of pain can be difficult. The Visual Analog Scale (VAS) is one of the most used tools to assess pain intensity and has been shown to be a valid and reliable method of measuring discrete pain. It is also a sensitive, simple, reproducible, and universally accepted method of assessing pain. Moreover, VAS can assess the relative change in the magnitude of pain over time on a linear scale (Lee et al., 2008). However, there are studies showing the difficulty of using VAS for pain measurement in children under 7 years (Champion et al., 1998). Shields et al. (2003) demonstrated that only one-third of children between 5 and 14 years old understood the concept of the VAS for pain scoring. They also found that patients who were able to understand the concept of the VAS were older than those who did not understand. Hence, instead of VAS, facial expression scales can be used in young children. Face pain scales do not require the child to translate pain experience into a numerical value. They require a child to discriminate among different levels of pain depicted in pictures (Garra et al., 2010).
In the present study, Wong–Baker FPS, which is a FPS, was used to assess pain intensity in different regions like molars, incisors, palate, and tongue. The Wong–Baker FPS has been extensively studied and its reliability and validity has been confirmed in children between 3 and 18 years of age. Strong correlations have been reported between the Wong–Baker Scale scores and other faces scales (Stein, 1995; Bosenberg et al., 2003). The Wong–Baker Scale was preferred by children to the numeric rating scale, the graphic rating scale, and the Color Analog Scale (Wong and Baker, 1988; West et al., 1994; Keck et al., 1996; Chambers et al., 2005). Maunuksela et al. (1999) reported the validity of using the VAS and FPS in children to rate postoperative pain. Children ages 6 to 8 were able to rank a series of faces in order of increasing pain (Tyler et al., 1993). Agreement between the FPS and the standard VAS was previously documented (Bieri et al., 1990). The present study found that both groups experienced mild pain in the molars and incisors during the first week of RME activation. The maximum pain was experienced by both groups on day 4 after which the pain diminished. Gecgelen et al. (2012) in their study found that the maximum number of patients reporting pain was at day 3 and day 4. From day 5 onward, the percentage of patients reporting pain gradually reduced. Similarly, Needleman et al. (2000) showed the highest levels of pain were reported during the first 10 turns with the greatest intensity during the first 6 turns and a steadily decreasing amount of pain. Cleall et al. (1965) reported that the midpalatal suture widened soon after the application of pressure in the rhesus monkey. As expansion continued, less disruption of the midpalatal tissues occurred with each progressive turn of the screw. This may explain the decrease in reported pain during the later stages of the activation. The decreasing trend in reported pain may also be explained by the fact that patients may become more comfortable with the procedure, and thus the fear and anxiety of turning the appliance may be lessened with each turn.
There was a statistically significant difference between the pain reported by patients who received 2 activations per day (Group A) than 1 activation (Group B). The pain perceived in the molars was the highest and was statistically significant. This was because the appliances are connected to the molars and also the expansion pattern during RME results in dentoalveolar expansion (including dental tipping) being larger than skeletal expansion (Feldmann and Bazargani, 2017). Pain in the palate and tongue were not significant.
Needleman et al. (2000) compared and evaluated the pain arising from 2 different RME protocols. However, the main analysis of the study did not concentrate on how the pain varied between the 2 protocols. The study concluded that during the first 10 activating turns, children whose rate of expansion was 2 turns/day were more likely to report pain and take pain medication than children whose rate of expansion was 1 turn/day, and this finding agreed with the present study. In contrast to the results of the present study, Halicioğlu et al. (2012) concluded that different activation protocols did not appear to alter subjective symptoms encountered during RME. A study by Baldini et al. (2015) concluded that the choice of activation protocol influenced the perceived pain during RME. They found the overall pain perception was significantly higher in the group that received 2 activations per day, which correlated with the results of the present study. There were no significant differences in the analgesic consumption between the 2 groups. In the present study, paracetamol was the most used drug for pain management.
Anxiety levels of the groups during activation of RME was evaluated using HAM-A. It was one of the first rating scales developed to measure the severity of anxiety symptoms and is still widely used today in both clinical and research settings. The reported levels of interrater reliability for the scale appear to be acceptable (Hamilton, 1959). HAM-A has been used as a benchmark for more recently devised scales (Thompson, 2015). Maier et al. (1988) tested the scale's reliability and validity and concluded that the reliability and concurrent validity of the HAM-A and its subscales were sufficient and there is reasonable interrater reliability and good 1 week retest reliability. To eliminate anxiety that can occur due to the RME splint itself, the appliance was placed in the patient's mouth 1 week before the activation protocols were begun. There were no statistically significant differences between the anxiety levels experienced between the 2 different activation protocols.
Jaw function was assessed using a questionnaire. The differences in effect of the activation protocols on jaw function discomfort was not statistically significant.
There was a significant difference between the 2 groups in the treatment duration. The group with single activation protocol needed to be treated for a longer duration to achieve the required expansion. However, this may also depend on the amount of transverse discrepancy.
Based on the results of the present study, the RME activation in cleft patients can be maintained at 1 turn per day for initial activations, to reduce discomfort and can be increased after the fifth or sixth day to 2 activations until the desired expansion is achieved. Single turn activation may reduce the pain perceived in the molars and incisors during the initial phase of treatment and thereby increase patient comfort and compliance.
The strengths of the study include the use of a homogeneous age group for assessment of pain as this age group is representative of the most common age for RME in patients with CLP. The assessment methods and questionnaires have documented good reliability and validity.
The limitations of the study are the following: The correlation between gender and pain perception was not assessed. The data was collected based on subjective reports of the patients, which may not be reliable especially in children due to language skills, developmental factors, different attitudes toward pain, and prior pain experiences. A larger sample size may have been more beneficial to generalize the study to all patients with CLP.
Conclusion
Patients who received 2 activations per day experienced significantly higher levels of pain in the molars compared to the patients who received a 1 activation per day. On day 3 and day 4, there was a significant difference between the 2 groups regarding pain in the incisors.
There were no significant differences between the 2 activation protocols in terms of pain in the palate, tongue, anxiety, and jaw discomfort.
The 2-turn activation group had a significant reduction in the treatment duration than the 1-turn activation group.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.